
Abstract
Background
Young-onset dementia (YOD) causes major life disruptions and emotional strain for both persons living with YOD and their informal caregivers. Non-pharmaceutical interventions may help to improve quality of life and reduce stress.
Objective
We aimed at investigating the effects of non-pharmaceutical interventions for persons living with YOD and their informal caregivers and to explore the intervention characteristics.
Methods
We conducted a systematic review including randomized and non-randomized controlled trials (PROSPERO: CRD42025645744). We searched major bibliographic databases and performed citation and web searches. Two reviewers independently screened titles, abstracts, and full texts. For data extraction, we used Elicit, an artificial intelligent research assistant; with extractions confirmed by a human reviewer. The methodological quality was assessed using the Mixed Methods Appraisal Tool (MMAT). We performed a narrative synthesis based on a harvest plot. When appropriate, we performed meta-analyses.
Results
We found 9 trials assessing interventions on education and information or skills building interventions that were published between 1990 and 2024 (median sample size: 58). Meta-analyses revealed no statistically significant impact on behavioral outcomes, activities of daily living, and quality of life of persons living with YOD and no statistically significant impact on burden, depression and anxiety, and quality of life of informal caregivers.
Conclusions
Evidence on the effectiveness of non-pharmaceutical interventions for persons living with YOD and their informal caregivers is limited and inconsistent. Further, larger, and multiple randomized controlled trials assessing the impact of non-pharmaceutical interventions with comparable outcomes, standardized measurements, and longer follow-ups are needed.
Keywords
Introduction
Young-onset dementia (YOD) refers to any dementia diagnosed before the age of 65. 1 With an estimated prevalence of 119 per 100’000, YOD accounts for about five percent of all dementia cases. 2 Common symptoms in persons living with YOD are memory complaints, depression, behavioral issues, and physical symptoms such as gait disturbance, seizures, peripheral neuropathy, and visual impairment. Frontotemporal dementia (FTD) is a specific form of YOD that is characterized by progressive deficits in behavior, executive function, or language. 3
Being diagnosed with YOD can lead to significant consequences for a younger person, including early retirement, financial implications, and the psychological challenge of coping with cognitive decline. 4 Also family members of persons living with YOD experience emotional and psychological challenges and unmet needs pre and post diagnosis,4,5 characterized by worries about dependency, anxiety, and increased depression. 6
Despite these challenges, current interventions do not meet the personal and psychological needs of persons living with YOD and their informal caregivers, 7 as there exist YOD-specific barriers including ineligibility, unaffordability, lack of security and lack of childcare. Therefore, post-diagnostic care for persons living with YOD should be tailored, flexible, affordable and provide meaningful engagement. 8 From a qualitative systematic review, Zhang et al. (2025) derived three themes of supportive care needs of persons living with YOD: empowerment through knowledge and planning, promotion of physical and psychosocial well-being, and the need for a strong support network. 9
Various interventions aim to support activities of daily living, reduce neuropsychiatric symptoms, slow cognitive decline and improve social engagement for both persons living with YOD and their informal caregivers. 10 There can be benefits in improving quality of life in persons living with YOD and their informal caregivers through these non-pharmaceutical interventions, e.g., in reducing care burden and psychological stress, improved self-esteem and sense of purpose.10,11 A systematic assessment of the benefits and harms of non-pharmacological interventions for persons living with YOD and their informal caregivers is currently lacking. The objective of this study was therefore to investigate the effects of non-pharmaceutical interventions for persons living with YOD and their informal caregivers and to explore the intervention characteristics.
Methods
We performed a systematic review following our pre-specified methods as registered on the international prospective register of systematic reviews (PROSPERO, CRD42025645744). 12 We followed the “Preferred Reporting Items for Systematic reviews and Meta-Analyses” (PRISMA) 2020 statement to structure this report.
Eligibility criteria
We included primary studies with a comparative interventional design (i.e., participants allocated to one of two or more groups, e.g., individual or cluster randomized controlled trial, non-randomized controlled trial, stepped-wedge design) in any phase (e.g., pilot, feasibility, evaluation) with the following characteristics:
− Population: Persons living with YOD, FTD, and/or their informal caregivers. YOD is typically being defined as onset of dementia until the age of 65. However, we do not solely consider an age-related cut-off age (i.e., 65 as mean age of study participants) but also relied on the terminology as used by study authors (e.g., early-onset or young-onset dementia population). Studies including persons living with YOD, FTD, and/or their informal caregivers as a subgroup among other types of dementia were included if they presented information on a separate analysis for our target population in the abstract. − Intervention and comparison: Any post-diagnostic non-pharmaceutical intervention (e.g., care, nursing, medical, therapeutical, rehabilitative, supportive, behavioral, environmental, social, and system intervention) with any comparison (e.g., active, sham, usual care). Drug interventions, dietary supplements, and diagnostic interventions were not considered. − Outcome: Any clinical outcome measured in persons living with YOD or informal caregivers. We did not consider process evaluation outcomes (e.g., satisfaction with the intervention, feasibility of the intervention, other implementation issues), biomarkers (except from digital biomarkers), and surrogate outcomes (e.g., vital signs, labor measures, imaging measures, electrocardiogram, or ultrasound). − Setting: Any country, context, or setting.
We considered journal articles following an Introduction-Methods-Results-and-Discussion (IMRaD) structure published in English or German for inclusion with no restrictions to the publication year.
Evidence syntheses and study protocols were excluded but kept as seed reference for citation searching (see below for details).
Information sources and search strategy
We searched the following databases on February 7, 2025: MEDLINE/Ovid, Embase/Ovid, CINAHL/EbscoHost, CENTRAL/Cochrane Library, and PsycInfo/Ovid. The database search strategy was developed by two reviewers (MV and JH) with consultation of a medical information specialist (CAH); informed by population-related search terms identified in relevant evidence syntheses (e.g., young-onset, early onset, younger onset, or frontotemporal combined with dementia or Alzheimer) combined with search filters for study design (i.e., clinical trials using Canadian Agency for Drugs and Technologies in Health (CADTH) “All Clinical Trials” filters; except for CENTRAL) and publication type (i.e., full publication of study findings, only for Embase and CENTRAL) and a NOT-component (aiming at excluding biomedical and basic research). The search strategy was drafted for the search in MEDLINE and translated to the remaining databases with the support of Polyglot Search 13 (Supplemental Material 1). Deduplication was performed using Citavi. 14
Using the new web application Co*Citation Network (https://CoCitationNetwork.github.io), we performed citation searches 15 on March 13, 2025 using eligible study reports,16–28 pertinent evidence syntheses,7,10,11,29 and study protocols20,30,31 as retrieved by the database search as seed references. Specifically, we conducted unranked direct citation searching (UDCS; for cited and citing references) and ranked (in)direct citation searching (RICS; for top-ranking cited, citing, co-cited and co-citing references) as described in detail elsewhere. 32 One iteration of citation searching was performed. Deduplication (against references retrieved by database searching and within but not between citation searching methods [RICS and UDCS]) was performed using a method that is largely identical to the Bramer method and has been documented in an online video tutorial (https://osf.io/jaeu5).
After finishing the search and screening of references retrieved by database and citation searching, we searched Google Scholar using specific search terms (e.g., early-onset, young-onset, frontotemporal dementia, non-pharmaceutical intervention) and considered the first 20 search hits. We also made use of artificial intelligent search engines on April 29, 2025 (undermind.ai [free version] and Elicit.com [Plus version]) by prompting our review question (i.e., “What are the effects of non-pharmaceutical interventions for persons living with young-onset or frontotemporal dementia and their caregivers?”) and screening the first eight hits each.
Finally, one reviewer (MV) checked the reference lists of reviews33–38 that were retrieved from citation searching for additional eligible studies.
Study selection
Two reviewers (MV and NH) independently screened titles, abstracts, and full texts using the Rayyan web-app. 39 Any conflicts were discussed between the two reviewers, or with consultation of a third reviewer (JH). Results retrieved by searches on Google Scholar and from artificial intelligent search engines were screened by one reviewer (MV), with consultation of a second reviewer (JH) in any unclear case.
Data extraction
We used Elicit, an artificial intelligent (AI) research assistant, 40 to extract data from eligible studies. All extractions were verified or complemented by a human reviewer (MV). Extracted outcome and results data were in addition verified by a second human reviewer (NH or JH). We extracted the following information:
general study characteristics (corresponding author, protocol link, registry number, publication date, DOI), study design, design characteristics (number of study arms, number study centers, allocation type), study objective, population (type of participants, sample size, age and sex of participants, type of dementia), country of conduct, study setting, intervention (type and name of intervention(s) and comparator(s), duration, facilitator, frequency, content, delivery and location), outcome (name/type, participant group, measurement, measurement type and direction, timepoint(s) of measurement, maximum length of follow-op), and results (type, group differences, total number of experimental and control group, mean and SD of groups, latest follow-up for all intervention groups per outcome, narrative and numeric results of intervention effects).
Assessment of the methodological quality
One reviewer (MV) assessed the risk of bias using the Mixed Methods Appraisal Tool (MMAT) Version 201841,42 (relevant categories of study: quantitative randomized controlled trials and quantitative non-randomized) with consultation of a second reviewer (JH) in any unclear cases. Signaling questions were answered with yes, no, or can’t tell. Can’t tell meant that there was insufficient information to answer with yes or no. The appraisals were double-checked by a second reviewer (NH). We did not assess the certainty of evidence.
Data analysis and synthesis
To describe the study and intervention characteristics, we performed a narrative summary report based on tabulated data extractions using numbers and percentages. This was based on meaningful groupings of study characteristics, i.e., interventions, and outcomes; based on clinical and methodological expertise of three reviewers (MV, LA, and JH). 43
To provide an overview of the effects of non-pharmaceutical interventions for persons living with YOD and their informal caregivers, we designed a harvest plot showing effect directions of all study outcomes and results and we narratively summarized its content. Harvest plots provide an overview of evidence from studies with multiple designs reporting heterogenous interventions, outcomes, and other clinical characteristics with differential intervention effects. 44 Interventions and outcomes for the harvest plot and narrative synthesis were inductively categorized by two reviewers (JH, MV). To synthesize findings across interventions, we categorized the studies according to the primary target population (persons living with YOD or informal caregivers) and the mode of intervention delivery, i.e., intended pathway of knowledge or skills acquisition; two categories emerged from the data: (1) “education and information” and (2) “skills building interventions”. As education and information interventions, we classified those interventions that primarily provided conceptual frameworks, structured guidance, planning tools, or informational content aimed at increasing the knowledge, understanding, and decision-making of those receiving the intervention. Education and information interventions aimed at supporting informed coping or care but did not focus on structured training in psychological or behavioral skills. As skills building interventions, we classified those interventions that primarily and explicitly contained training of psychological or behavioral skills as a central component of the intervention. These programs required active participant engagement in learning, applying, and refining strategies that were designed to modify cognitive, emotional, or behavioral responses.
Three authors (MV, LA, and JH) explored clinical heterogeneity and thus the fundamental potential for statistical meta-analyses, based on discussion on the similarity and differences in study characteristics (i.e., population, intervention, comparison, and outcome). This assessment informed the meaningfulness of potential statistical meta-analyses. Statistical heterogeneity was explored based on visual results of forest plots to consider the direction and magnitude of effects and the degree of overlap between confidence intervals. In addition, we based our interpretation on the I2 statistics. 45 As a result from these clinical and statistical explorations and assessments, we performed pre-specified explorative meta-analyses with outcome results for persons living with dementia (behavior outcomes, activities of daily living, and quality of life) and informal caregivers (burden, depression, and quality of life), calculated by the free web-based tool MetaAnalysisOnline.com. 46 We used a random effects model, the inverse variance method, hedges’ g for estimating SMD, and restricted maximum likelihood for estimating between study heterogeneity. We pooled the intervention effects of the experimental group versus the control group on different outcomes with the standardized mean difference (SMD) using 95% confidence intervals (CI) based on mean, standard deviation (SD), and number of participants. 45 Where the SD was not available, we calculated it from the reported CI using RevMan Web. 47 For SMD calculation and to ensure that all the scales point in the same direction (i.e., lower values indicate a more positive impact) and to increase the readability of the forest plots, mean values of study groups that were measured by scales where higher values indicate a more positive impact have been reversed (i.e., multiplied by −1). 48 Cluster-randomized trials were combined with individually randomized controlled trials in the same meta-analyses. 49 We did not perform author requests for additional or missing data. For all outcome results, we considered the latest follow-up that was reported.
Results
Our search retrieved a total of 3391 hits. Ninety-three full text articles were screened against the inclusion criteria. We excluded 80 reports after full text screening (Figure 1; Supplemental Material 2) and included 9 studies.16,17,19,21,23–27 For 3 studies,16,23,24 we included additional study reports.18,20,22,28 In the following, we no longer refer to these additional reports. Except from two reports that we identified via citation searching methods,18,26 we retrieved all reports from database searching. Detailed results for UDCS and RICS will be published elsewhere, citing this report.
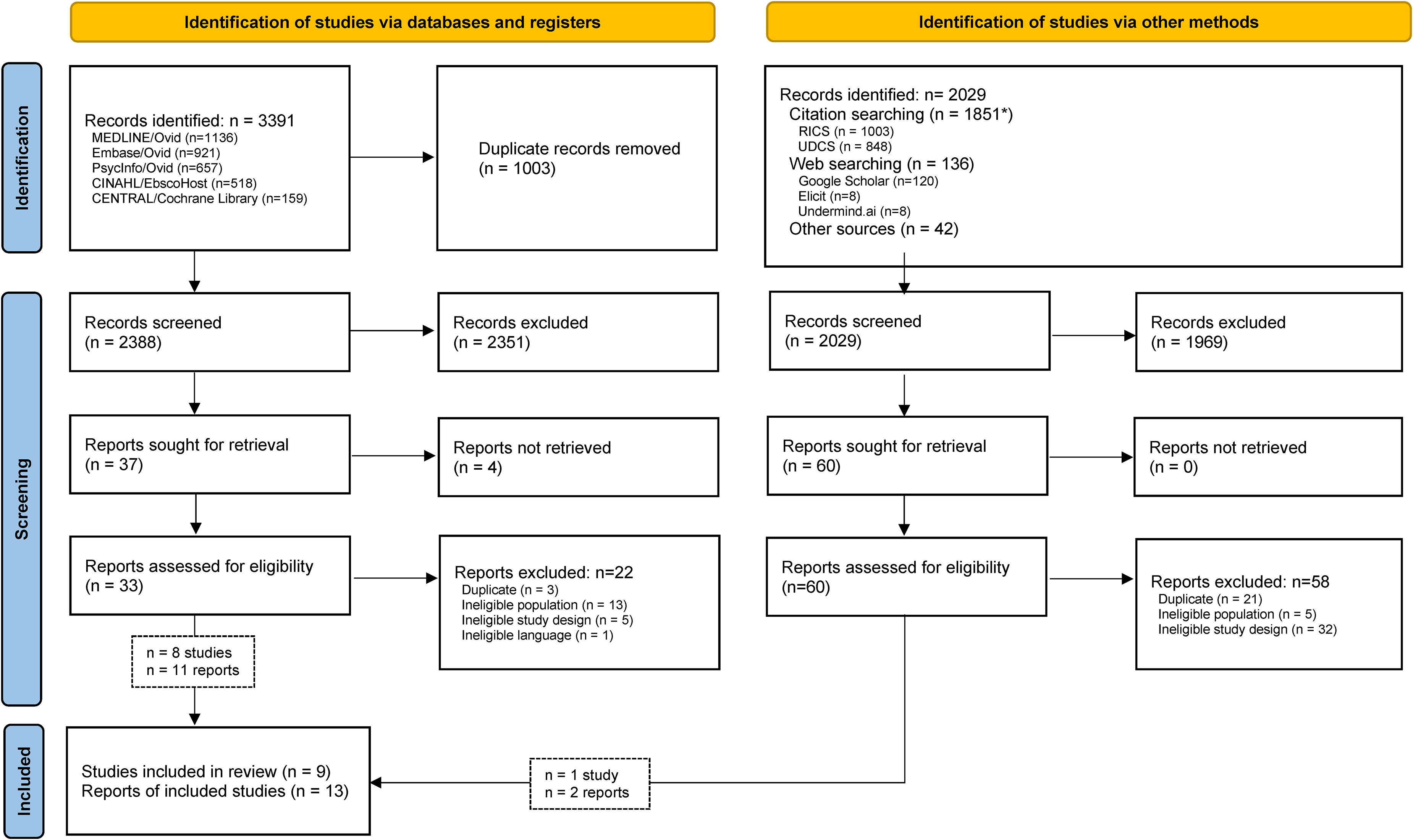
Literature search and selection process. *Deduplicated number of results; deduplicated against the search hits identified from databases, and within but not between RICS and UDCS. n: number; RICS: ranked indirect citation searching; UDCS: unranked direct citation searching.
Characteristics of the included studies
The studies were published between 1990 and 2024 with a median publication year of 2019 (Table 1). Three studies were conducted in the United States (33%),19,21,26 2 in the Netherlands (22%),16,17 2 in Australia (22%),24,25 1 in Italy (11%), 27 and 1 in the United Kingdom (11%). 23 Except from 1 study that was a non-randomized study of intervention (NRIS) (11%), 24 all were randomized controlled trials (RCT) (n = 8; 89%).16,17,19,21,23,25–27 In 1 study (11%), 16 participants were persons living with YOD, 6 studies (67%) included their informal caregivers,19,21,23,24,26,27 and 2 studies included dyads (22%).17,25 The number of participants ranged between 12 and 274 (median: 58, overall 524). The participants mean age varied between 53 and 64. The type of dementia was characterized as FTD (n = 5 studies; 56%)19,21,23–25 or YOD (n = 4 studies; 44%; Table 1; Table 2; Supplemental Material 3).16,17,26,27
Characteristics of the included studies (n = 9).
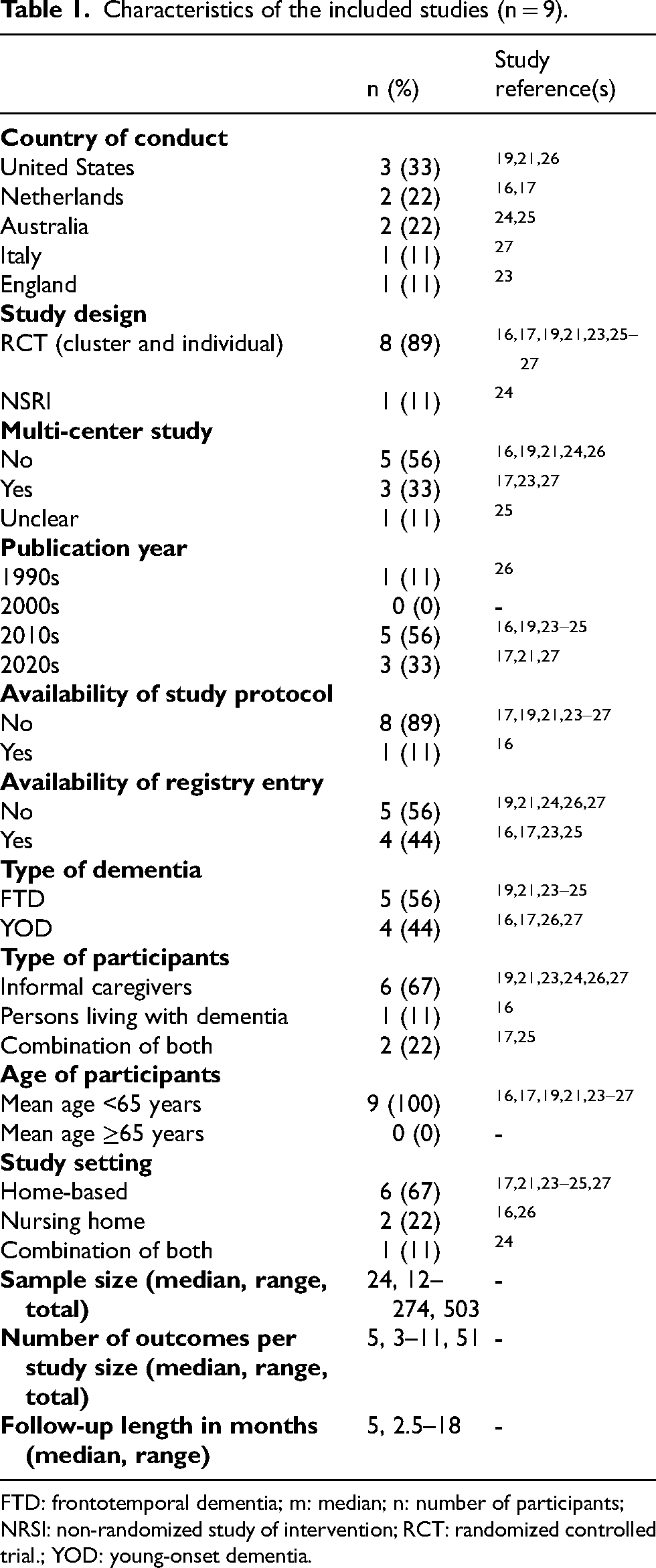
FTD: frontotemporal dementia; m: median; n: number of participants; NRSI: non-randomized study of intervention; RCT: randomized controlled trial.; YOD: young-onset dementia.
Study and intervention characteristics (n = 9).
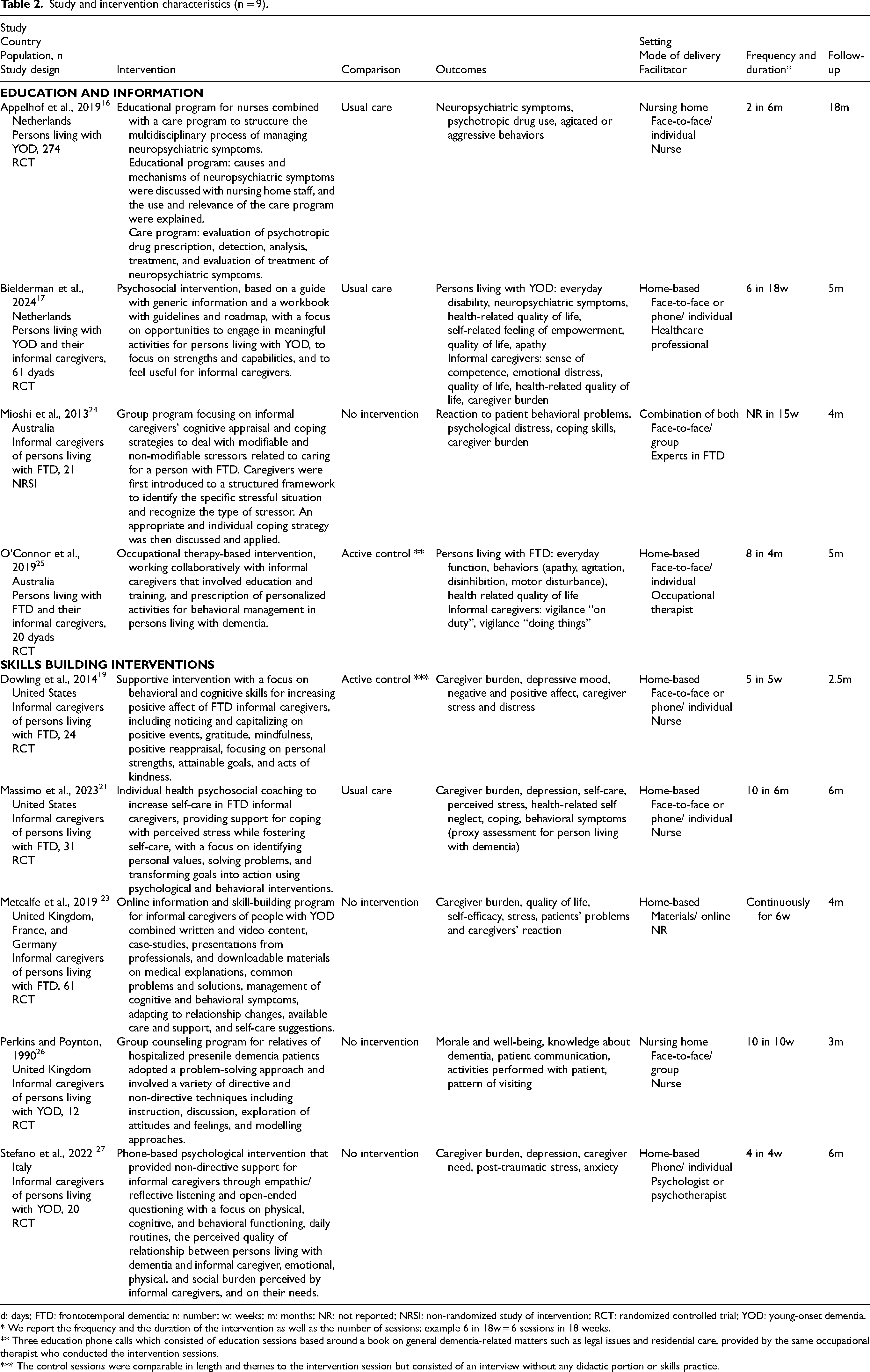
d: days; FTD: frontotemporal dementia; n: number; w: weeks; m: months; NR: not reported; NRSI: non-randomized study of intervention; RCT: randomized controlled trial; YOD: young-onset dementia.
* We report the frequency and the duration of the intervention as well as the number of sessions; example 6 in 18w = 6 sessions in 18 weeks.
** Three education phone calls which consisted of education sessions based around a book on general dementia-related matters such as legal issues and residential care, provided by the same occupational therapist who conducted the intervention sessions.
*** The control sessions were comparable in length and themes to the intervention session but consisted of an interview without any didactic portion or skills practice.
Characteristics of the study interventions
The included nine studies assessed education and information interventions (n = 4 studies, 44%)16,17,24,25 and skills building interventions (n = 5 studies, 56%).19,21,23,26,27 Intervention comparisons were made to usual care (n = 3 studies, 33%),16,17,21 wait list or no intervention (n = 4 studies, 44%)23,24,26,27 or active control (n = 2 studies, 22%).19,25 Six interventions (67%) were delivered individually, either face-to-face (n = 2 studies, 22%),16,25 phone based (n = 1 study, 11%) 27 or combined (n = 3 studies, 33%).17,19,21 The other interventions were delivered face-to-face in a group (n = 2 studies, 22%)24,26 or with online material (n = 1 study, 11%). 23 The interventions were conducted home-based (n = 6 studies, 67%),17,21,23–25,27 in nursing homes (n = 2 studies, 22%)16,26 or in both of them (n = 1 study, 11%). 24 In 4 studies (44%), the intervention was facilitated by nurses,16,19,21,26 in 2 studies (22%) by health professionals or experts in dementia care,17,24 in 1 study (11%) by occupational therapists, 25 in 1 study (11%) by psychologists or psychotherapists, 27 and 1 study (11%) did not report who facilitated the intervention. 23 The intervention period ranged from 1 month to 6 months. The frequency of the intervention delivery varied between 2 sessions in 6 months to weekly sessions throughout 2.5 months; one study offered the intervention online continuously for 6 weeks (study-specific details in Table 2). The length of follow up ranged from 2.5 to 18 months (Table 2; Supplemental Material 3).
Methodological quality of included studies
Randomized controlled trials (n = 8)
Randomization was appropriately performed in 4 out of 8 studies (50%). Groups were comparable at baseline in 7 out of 8 studies (88%). Outcome data were completed in 6 out of 8 studies (75%). In 5 out of 8 studies (67%), it was unclear if the outcome assessors were blinded to the intervention provided. In 6 out of 8 studies (75%), it was unclear if the participants did adhere to the assigned intervention (Table 3; Supplemental Material 3).
Methodological quality of the included studies (n = 9).
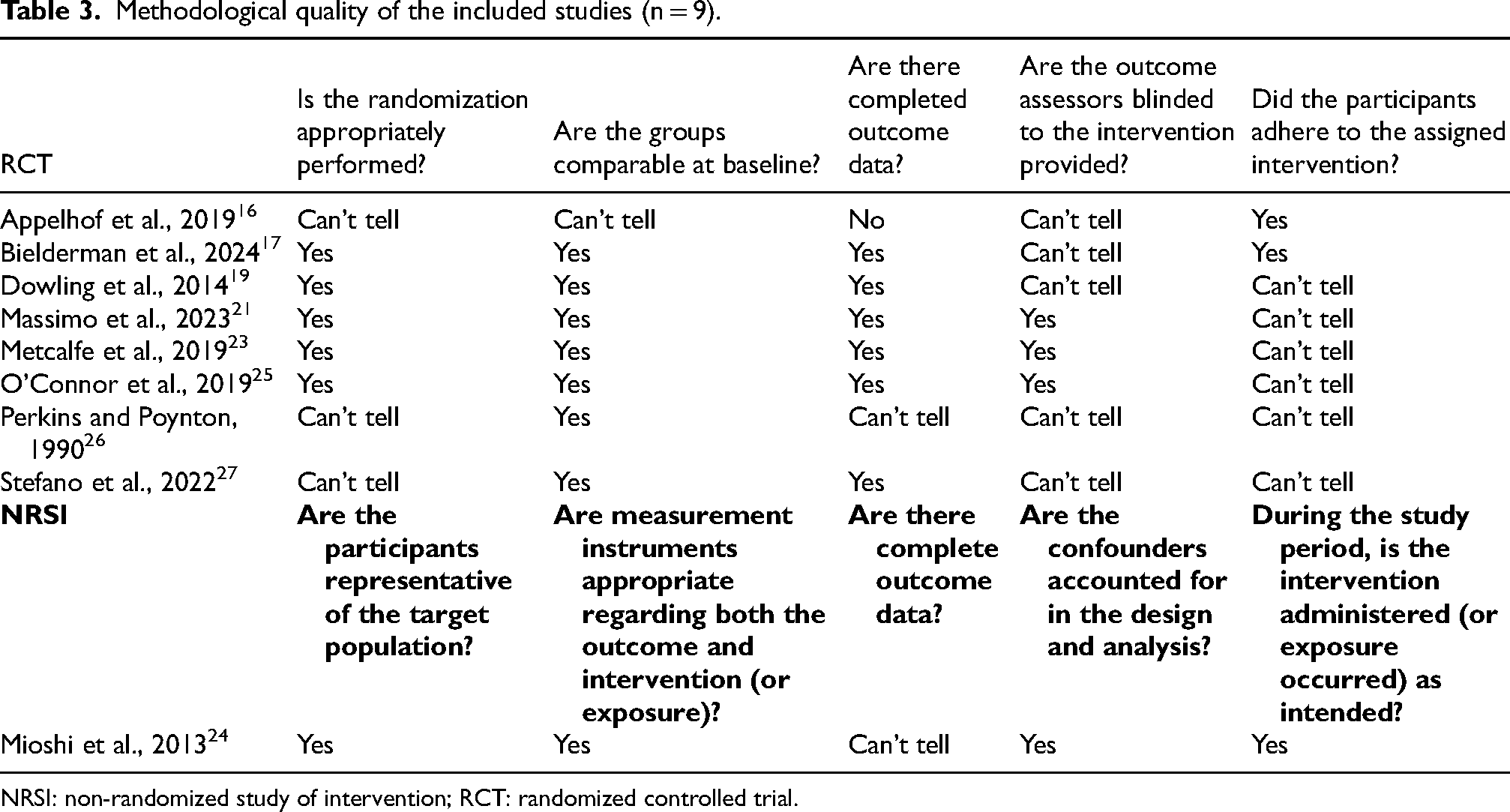
NRSI: non-randomized study of intervention; RCT: randomized controlled trial.
Non-randomized studies of intervention (n = 1)
In this single study, participants were assessed as being representative of the target population. Measurement instruments were appropriate regarding both outcome and intervention. It is unclear if there were complete outcome data due to insufficient reporting. Confounders were accounted for the design and analysis. The intervention was administered as intended during the study period (Table 3; Supplemental Material 3).
Qualitative synthesis of results
Eight studies that assessed the effects on 10 outcomes were considered for qualitative/narrative synthesis as shown in the harvest plot (n = 8 studies; follow-up range between 1 and 18 months, median = 14 months; Figure 2) and summarized below.

Harvest plot with effect directions of study outcomes and results. Each bar corresponds to a study outcome result (with multiple outcomes assessed per study), stratified by interventions in columns (i.e., education and information; skills building interventions), and stratified by population (i.e., persons living with YOD; informal caregiver) and outcomes in rows. The height of the bar represents the maximum length of follow-up measured for an outcome, clustered in 3-months steps: 1–3 months (minimum) to 16–18 months (maximum). The width of the bar has no meaning. The numbers and abbreviations below the bars indicate the number of participants (n) and the reference. The color of the bar indicates the type of dementia (dark grey = FTD, light grey = YOD). Benefit (left side of the dashed vertical line): studies with a statistically significant impact that favors the experimental intervention for the population; no/uncertain benefit (right side of the vertical line): studies with a uncertain statistically significant impact for the population or with a statistically significant impact that favors the control intervention for the population. One study was not included in the harvest plot because comparative results between groups were not reported. 24
Education and information for persons living with YOD
No statistically significant beneficial impact on behavioral outcomes (i.e., neuropsychiatric symptoms or single behavioral symptoms including apathy, agitation, aggression, disinhibition, motor disturbance; Supplemental Material 3),16,17,25 activities of daily living,17,25 quality of life,17,25 drug use 16 or empowerment. 16
Skills building interventions for persons living with YOD
Skills building interventions proved to have a statistically significant positive impact on behavioral outcomes. 21
Education and information for informal caregivers
No statistically significant beneficial impact on burden, 17 stress, 17 quality of life, 17 and other outcomes (self-care, self-efficacy, coping, needs, vigilance, knowledge and competence).17,25
For one study in which comparative results between groups were not reported, within group results indicated a statistically significant decrease in the level of informal caregiver burden and reaction of behaviors in the intervention group immediately after the intervention compared to baseline values (with no statistically significant changes on depression, anxiety, and stress; and no statistically significant within group changes on any outcome in the control group). 24
Skills building interventions for informal caregivers
No statistically significant beneficial impact on depression and anxiety.19,21,27 For burden and stress, one study reported significant benefits, 19 while others found no statistically significant effect.19,21,23,27 For quality of life, one study each showed a beneficial 26 and no beneficial 23 statistically significant impact. Two studies showed significant positive impact on interaction with persons living with YOD,23,26 though one also showed no statistically significant benefit in other domains in this category. 26 Other outcomes (self-care, self-efficacy, coping, needs, vigilance, knowledge and competence) showed both statistically significant 21 and insignificant beneficial impact.21,23,26,27
Quantitative synthesis of results
Eight studies that assessed the effects on 6 outcomes were considered for quantitative/statistical analysis (Figure 3; Figure 4) and summarized below.
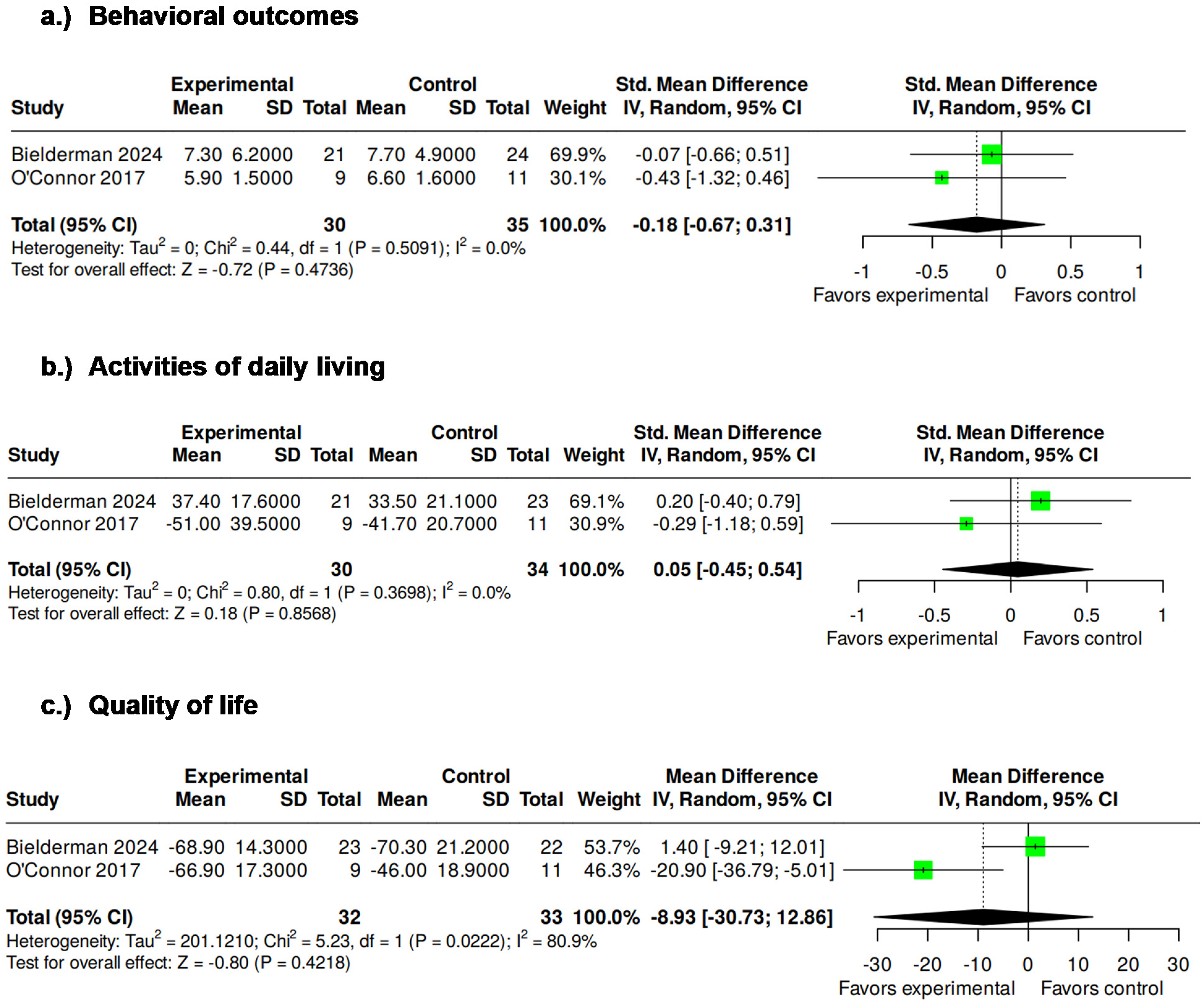
Forest plot on education and information interventions for persons living with YOD.
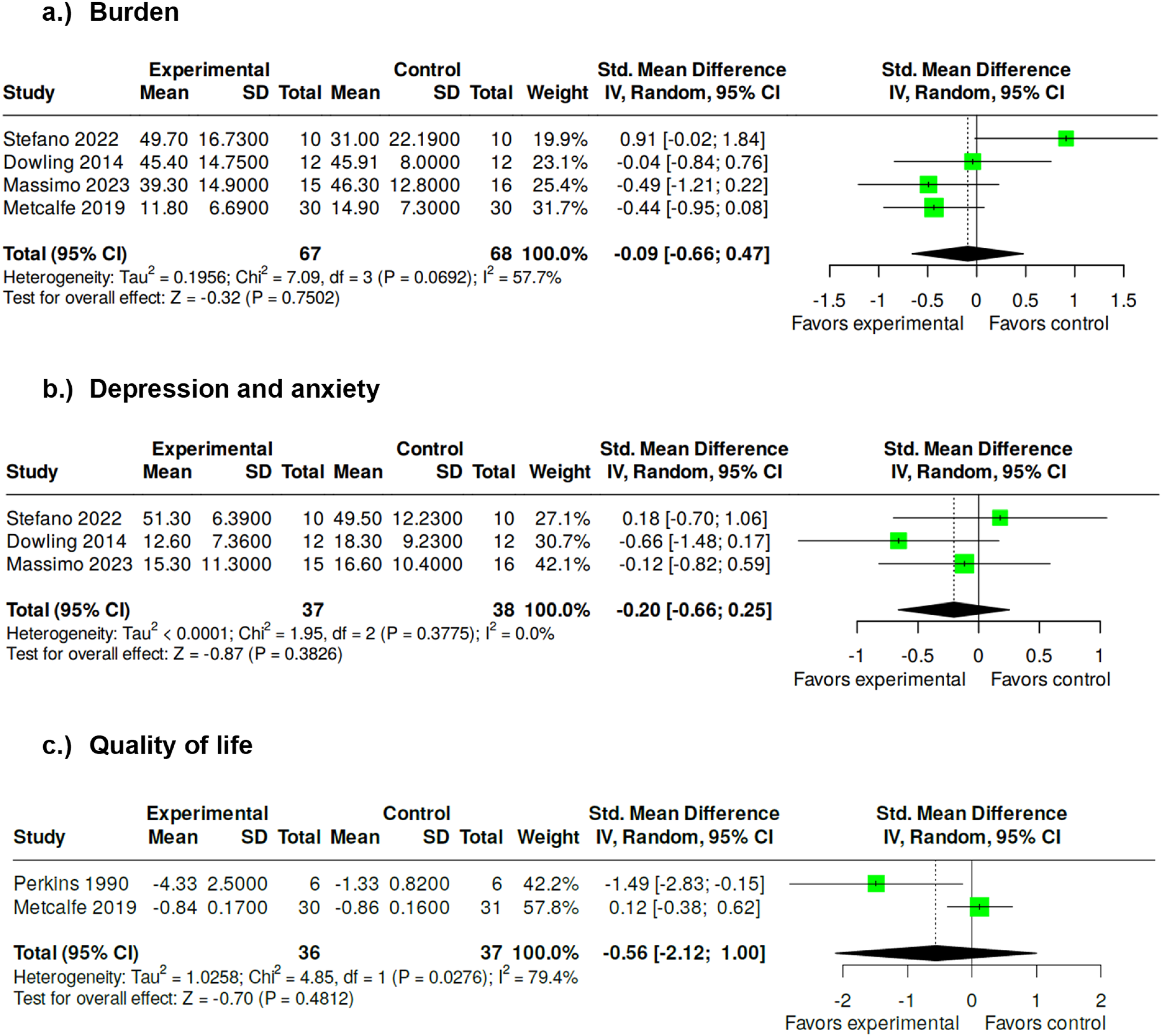
Forest plot on skills building interventions for informal caregivers.
Education and information for persons living with YOD
There were no statistical group differences on behavioral outcomes (SMD −0.18, 95% CI −0.67; 0.31),17,25 activities of daily living (SMD 0.05, 95% CI −0.45; 0.54),17,25 and quality of life (MD −8.93, 95% CI −30.73; 12.86).17,25
Skills building interventions for informal caregivers
There were no statistical group differences on burden (SMD −0.09, 95% CI −0.66; 0.47),19,21,23,27 depression and anxiety (SMD −0.20, 95% CI −0.66; 0.25),19,21,27 and quality of life (SMD −0.56, 95% CI −2.12; 1.00).23,26
Discussion
We included eight studies assessing the impact of non-pharmaceutical interventions for persons living with YOD and their informal caregivers. Educational and informational interventions for persons living with YOD had no statistically significant impact on behavioral outcomes, daily activities, quality of life, drug use, or empowerment. Skills building interventions showed a positive effect on behavioral outcomes in one study. For informal caregivers, education and information had no statistically significant effects, while skills building interventions showed mixed results, with some benefits in burden, quality of life, and interaction. The statistical synthesis widely confirmed the narrative findings. No statistically significant differences were observed between intervention and control groups for persons living with YOD in behavior, activities of daily living, or quality of life. Similarly, among informal caregivers, there were no statistically significant effects of skills building interventions on burden, depression and anxiety, or quality of life.
Impact of interventions for persons living with YOD
There was a statistically significant beneficial effect on behavioral symptoms in persons living with FTD in one small study with 31 participants in which informal caregivers of persons living with FTD received individual health psychosocial coaching. 21 A narrative review identified interventions that also aimed to assist informal caregivers in learning strategies to positively impact behavioral outcomes, e.g., by teaching how to respond and modify the behavioral response of the person with FTD over time, meeting unmet needs of the individuals or focusing on the role that their own and environmental status can play as triggers for behavioral symptoms. Thus, these interventions may reduce behavioral symptoms, such as agitation and aggression in dementia populations. 37
Education and information interventions showed no statistically beneficial impact on behavioral outcomes, activities of daily living, quality of life, drug use and empowerment.16,17,25 Even if information is known as an unmet need of people with YOD 7 and qualitative studies that evaluated psycho-educational interventions showed that participants generally expressed positive satisfaction with the interventions, 7 the results of our review suggest that education and information interventions might not have a positive impact. Non-pharmaceutical interventions such as cognitive rehabilitations, physical and social activities, psychosocial interventions, and environmental support showed partial improvements for persons living with YOD and positive satisfaction with the interventions. These findings, however, were derived from both controlled and non-controlled designs, unlike our review, which included only controlled trials. 7 Even if interventions included in our review did not show statistically beneficial impact on most outcomes, considering qualitative results, non-pharmaceutical interventions were experienced positively as they provided persons living with YOD a sense of purpose, enhanced their happiness, improved their ability to engage in independent activities, establish goals, and uplifted their mood. 10
Impact of interventions for informal caregivers of persons living with YOD
There were no statistically significant beneficial impacts when assessing education and information interventions.17,25 Our qualitative synthesis showed mixed benefits of skills building interventions on burden, stress, quality of life, interaction and others (e.g., knowledge, self-care) and no benefit on depression and anxiety.19,21,23,26,27 Meta-analyses showed no statistically significant benefits on burden, quality of life, and depression and anxiety.19,21,23,26,27
Taken together, these findings suggest that while skills building approaches may offer some benefits, their effects remain inconsistent across studies and outcomes. This variability has prompted growing interest in alternative modes of delivery, particularly technology-based interventions.36,50 In our review, we included one technology-based intervention, which provided informal caregivers of people with FTD with an online information and skill-building program. The program combined written and video content, case studies, and presentations from professionals. It also offered downloadable materials on medical explanations, common problems and solutions, the management of cognitive and behavioral symptoms, adapting to relationship changes, available care and support, and suggestions for self-care. 23 Based on 12 qualitative and quantitative (of which 3 RCTs) studies conducted in Europe and Canada, Moyle et al. (2025) identified technologies that support informal caregivers of persons living with YOD. These technologies included online support interventions with information and skill-building programs, virtual psychotherapy, telephone-based psychological intervention, assistive technologies such as sensor and location devices, automated timers, mobile phone, automatic calendar, talking wristwatch, a medicine dispenser, a TV remote control, and telehealth. The interventions showed a positive impact on self-efficacy, satisfaction, knowledge, well-being, perceived burden and stress, depression and anxiety, except for one study which did not find any significant differences in measured outcomes. In addition, informal caregivers rated the program overall positively, demonstrating high satisfaction and acceptability. 35 Another scoping review identified web-based and face-to-face intervention studies that supported informal caregivers of persons living with YOD in managing the changes brought about by the disease showed significant but also no or unclear significant benefits of these interventions. However, qualitative findings indicated positive changes, including improved well-being, confidence in coping with challenges, and transition process but challenges were also identified in the scoping review, including technological difficulties. 10 The positive effects of technological interventions could be attributed to their ease of integration into daily life and the relative anonymity they offer, which facilitates the expression of true feelings and experiences. They also save logistical workforce resources compared to traditional face-to-face interventions. 10
Characteristics of interventions and quality of the evidence
The included studies showed clinical and methodological heterogeneity, particularly regarding intervention type, content, format, setting, and duration. Interventions were delivered individually or in a group, face-to-face, phone-based or online in nursing homes or home-based. The facilitators were health professionals, most of them nurses. The duration varied widely. Some interventions focused solely on providing information, whereas others combined information with counselling or skills training. Importantly, interventions that relied on information and education alone appeared insufficient to produce significant benefits, suggesting that information may need to be embedded within broader frameworks. This heterogeneity precluded meaningful quantitative synthesis and was a key reason for presenting findings using a harvest plot approach rather than relying solely on pooled effect estimates. In their scoping review, Cui et al. (2024) focused on non-pharmaceutical interventions for persons living with YOD and/or their informal caregivers and also identified a variety of interventions in terms of duration, frequency, content, and delivery. The interventions were delivered by different health professionals and were offered individually or group-based in different settings, such as remote, nursing-homes, home-based or in zoos, gardens, or football clubs. The authors argued that information alone often fall short in achieving meaningful impact, and should be combined with other components like skills training or psychological support. 10 Also Kim et al. (2024) emphasized the need for combined approaches, rather than single-focus interventions, as being more aligned with the complex needs of persons living with YOD and their informal caregivers. 7 The reporting of intervention adherence and fidelity was limited across the included studies. Although aspects of fidelity and adherence were considered by our critical study appraisal, the lack of detailed reporting made it difficult to determine whether non-significant effects reflect limited intervention efficacy or challenges, for example, in implementation, adherence, or study design.
Our review is based on nine studies with a total sample size of 503 participants with a median of 24 and a median follow-up of 5 months. Most included studies were therefore characterized by small sample sizes and relatively short follow-up periods, limiting the statistical power and the ability to draw conclusions about the sustainability of intervention effects. Other reviews on the topic also reported small numbers of studies participants with mostly short lengths of follow-up.7,10,11,35,36 Additionally, our review includes only two studies with dyads of persons living with YOD and their informal caregivers, indicating a need for intervention studies that address the entire family of a person living with YOD. It is necessary that interventions understand and tailor on the care context of persons living with YOD and their informal caregivers to consider their needs and enhance quality of life.7,36 To do so, persons living with YOD and their informal caregivers can be included in the design of support groups or the project steering group or committee. 36
Limitations
The strength of this review is a comprehensive search strategy considering databases, direct and indirect citation searching, and web- and AI-based searches. Study selection by two independent reviewers with clinical and methodological expertise and verification of data extraction and synthesis served to ensure high data quality. Although we did not plan to contact study authors for missing outcome data, we were able to run all meaningful meta-analyses. Our review also has some limitations, which should be acknowledged, as they affect interpretation of the findings. First, our search missed the term “familial Alzheimer disease” and “presenile dementia”. However, we explored the related search hits on PubMed and do not believe that we missed eligible study reports. Second, we did not perform a robust risk of bias assessment of the study results. This, in combination with a certainty assessment of the evidence, should be considered in future assessments when aiming to derive clinical implications of the evidence; which was not the aim of our review. Third, the identification and analysis of theoretical frameworks underpinning the intervention methods were not pre-specified in our review protocol. Consequently, data on theoretical frameworks were not systematically extracted from the included studies and analyzed. This represents an important area for future research and could/should be addressed in dedicated reviews or primary studies focusing specifically on theory-driven intervention development. Finally, we did not perform a detailed assessment of the study intervention. Applying assessments such as the “Template for Intervention Description and Replication” (TIDieR) checklist, 51 the updated “Criteria for Reporting the Development and Evaluation of Complex Interventions” (CReDECI-2) guideline, 52 or the more recent “Guidance for reporting intervention development studies in health research” (GUIDED) 53 may help to understand the interventions’ mechanisms and plan future interventions for persons living with YOD and their informal caregivers.
Conclusions
Evidence on the effectiveness of non-pharmaceutical interventions for persons living with YOD and their informal caregivers is limited and inconsistent, highlighting that most of the studies are very small with short follow-ups, heterogenous interventions and outcomes, and that there is a lack of studies on interventions targeting both persons living with YOD and their informal caregivers through dyadic interventions. The non-pharmacological interventions studied were primarily educational, informational, and supportive or consulting in nature, with few focusing on active skills-building. Educational and informational interventions showed no significant impact, while skills building interventions yielded mixed results. Statistical analyses confirmed the absence of robust effects. To increase the quality and certainty of evidence on non-pharmaceutical interventions for persons living with YOD and their informal caregivers, further, larger, and multiple randomized controlled trials assessing the impact of specific non-pharmaceutical interventions with comparable outcomes, standardized measurements, and longer follow-ups are needed. Furthermore, new trials addressing the effectiveness of active skills-building are warranted.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261429998 - Supplemental material for Non-pharmaceutical interventions for persons living with young-onset dementia and their informal caregivers: A systematic review with meta-analysis
Supplemental material, sj-docx-1-alz-10.1177_13872877261429998 for Non-pharmaceutical interventions for persons living with young-onset dementia and their informal caregivers: A systematic review with meta-analysis by Magdalena Vogt, Nicole Helfenberger, Christian Appenzeller-Herzog, Laura Adlbrecht and Julian Hirt in Journal of Alzheimer's Disease
Supplemental Material
sj-xlsx-2-alz-10.1177_13872877261429998 - Supplemental material for Non-pharmaceutical interventions for persons living with young-onset dementia and their informal caregivers: A systematic review with meta-analysis
Supplemental material, sj-xlsx-2-alz-10.1177_13872877261429998 for Non-pharmaceutical interventions for persons living with young-onset dementia and their informal caregivers: A systematic review with meta-analysis by Magdalena Vogt, Nicole Helfenberger, Christian Appenzeller-Herzog, Laura Adlbrecht and Julian Hirt in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We thank Cristina De Biasio and Linda Premerlani (both mosa!k StGallen and PortoFaro project team members) for contributing to the design of this review (i.e., review questions and eligibility criteria). This review is part of the PortoFaro project which has been planned in close collaboration with patient and public representatives (![]() ).
).
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was part of an overarching project focusing on persons living with young-onset dementia aiming at developing a concept to accompany and support persons living with young-onset and frontotemporal dementia and their families, funded by Gesundheitsförderung Schweiz (PortoFaro; ![]() ). The funder had no influence on the design, conduct, and reporting of this review.
). The funder had no influence on the design, conduct, and reporting of this review.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated and analyzed in this study is part of the publication and Supplemental Material.
Detailed results for the unranked direct citation search and ranked indirect citation search will be published elsewhere, citing this report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.