
Abstract
Background
Active euthanasia by physicians involves administering a substance that directly causes a patient's death. In Alzheimer's disease, progressive cognitive decline and increasing dependence raise complex ethical and emotional dilemmas. Although legalized in some countries, active euthanasia remains controversial, with public attitudes shaped by multiple factors, particularly in advanced disease stages.
Objective
This study examined older adults’ attitudes toward active euthanasia in advanced Alzheimer's disease from three perspectives: toward themselves, a family member, and an unknown individual. It also explored associations between sociodemographic and psychosocial variables and these attitudes.
Methods
A quantitative study was conducted with 501 individuals aged 75+, recruited through day centers and snowball sampling. Attitudes were measured using hypothetical cases involving euthanasia decisions for oneself, a family member, and an unknown individual. Variables included self-efficacy, will to live, desire to prolong life, life satisfaction, fear of death, social support, and sociodemographic characteristics. Analyses employed mean comparisons and hierarchical linear regression models.
Results
Participants reported the most favorable attitudes toward euthanasia when considering themselves (M = 3.61), followed by a family member (M = 3.22), with the least favorable attitudes expressed toward an unknown individual (M = 2.86). Lower desire to prolong life and higher self-efficacy predicted more positive attitudes across all cases, while lower will to live was positively associated only in personal and familial contexts. Female gender, higher education, and lower religiosity were linked to more favorable attitudes across all contexts.
Conclusions
Sociodemographic and personality characteristics should be considered when developing strategies aimed at increasing public awareness of active euthanasia, especially among older adults.
Introduction
End-of-life decisions in the case of Alzheimer's disease
Alzheimer's disease (AD) is the most common form of dementia, a neurological disorder characterized by memory loss, cognitive impairment, and difficulties with language and problem-solving that affect a person's ability to perform everyday activities1,2 The number of people with AD is expected to rise significantly worldwide, from 57.4 million cases in 2019 to 152.8 million cases in 2050. 3 The prevalence of AD sharply increases with age, which is the most significant risk factor: 5% of individuals aged 65 to 74, 13.2% of those aged 75 to 84, and 33.4% of those aged 85 or older are affected by AD. 4
At advanced stages of AD, patients lose the ability to make decisions for themselves; consequently, family caregivers must oversee such decision-making, which is challenging and stressful. These decisions usually include treatments at the end of life such as feeding, being connected to life-sustaining treatments, and requesting euthanasia5–8
Euthanasia in the case of Alzheimer's disease
Euthanasia, which originates from a Greek term whose translation is “good death”, is a conscious decision to terminate life with the aim of relieving severe and intolerable suffering. Euthanasia remains a contentious topic and has ignited widespread debate across the globe in recent years. 9 Euthanasia was defined by the World Medical Association as “knowingly and intentionally performing an act that is clearly intended to end another person's life and that includes the following elements: the subject is a competent, informed person with an incurable illness who has voluntarily asked for his or her life to be ended; the agent knows about the person's condition and desire to die, and commits the act with the primary intention of ending the life of that person; and the act is undertaken with compassion and without personal gain” (page 59). 10 There are different “types” of euthanasia: active euthanasia occurs when medical professionals, or another person, deliberately do something that causes the patient to die, whereas passive euthanasia occurs when the patient dies because medical professionals either don’t do something necessary to keep the patient alive, or when they stop doing something that is keeping the patient alive. 11
Although euthanasia is legal in some countries such as Canada, New Zealand, and the Netherlands, the ethics of conducting euthanasia, especially for individuals living with AD, is very complex and can cause disputes among professionals, family caregivers, and the public12–15.
In Israel, where euthanasia is prohibited, “The Dying Patient Act” was enacted in 2005 with the aim of promoting autonomous decision-making in medical care. The law allows individuals to specify, in advance the types of treatments they would like to receive or refuse at the end-of-life16,17
Attitudes toward euthanasia in Alzheimer's disease among healthcare professionals, family members, and the public
Healthcare professionals often find themselves navigating the ethical dilemmas and emotional burdens associated with euthanasia requests from individuals with dementia and their family caregivers. 18 In a study conducted in Belgium, where the law prohibits euthanasia at the end stage of dementia, 308 general practitioners were found to have a progressive perspective on euthanasia for individuals living with dementia. Namely, as the severity of dementia increased, there was a growing inclination to consider euthanasia. 19
By contrast, a systematic review showed that healthcare professionals tended to have more conservative attitudes toward assisted dying (a term that refers to voluntary euthanasia and physician-assisted suicide) than did the public, patients, and caregivers, and these views seemed less influenced by cultural backgrounds. Public acceptance of euthanasia and physician-assisted suicide has been found to be highest in cases of severe dementia if requested while the individual still has mental capacity, particularly in countries where assisted dying is legal. However, individuals with dementia and their carers prefer physician-assisted suicide during the early stages rather than euthanasia in advanced stages, whereas most physicians and nurses oppose assisted dying at any stage of dementia. Nonetheless, there is greater support for physician-assisted suicide in mild dementia and for euthanasia when an advance euthanasia directive is present, suggesting that health professionals may be more open to assisted dying when it is legal and capacity issues are clearer. 20
Family caregivers and patients themselves have exhibited varied understandings and attitudes towards euthanasia, with knowledge gaps and differing opinions on its suitability for individuals with dementia underscoring the need for enhanced educational efforts and dialogue. 21
Factors associated with attitudes toward euthanasia in Alzheimer's disease
Attitudes toward euthanasia have been found to be related to sociodemographic variables, although the findings have not been consistent. An American study conducted among 1711 adults to assess public opinion on advance request euthanasia and/or assisted suicide (AR-EAS) for dementia found that more than half of the participants (54.4%) agreed with AR-EAS legalization. Agreement was associated with lower dementia quality-of-life rating, younger age, not being religious, and being politically liberal. That said, the complex ethical and practical issues surrounding AR-EAS may make it challenging to elicit well-considered public opinions on the topic. 22
A longitudinal study was conducted in 62 countries to identify attitudes toward euthanasia and to examine how economic, religious, and health-related factors influenced these attitudes. On the one hand, it was found that euthanasia was more accepted in high-income countries, with higher life expectancy and lower infant mortality. On the other hand, the greater the importance placed on religion, the lower respondents’ acceptance of euthanasia. The research also revealed that cultural context had a main impact on attitudes toward euthanasia. 23
Studies have revealed that religion and religiosity seem to be important factors associated with attitudes toward euthanasia. A study conducted among the Israeli public found that the public was polarized on end-of-life issues, particularly regarding patient autonomy and medically-assisted dying, with significant differences based on religiosity. 24 Similarly, a Finish study conducted among nurses and the public toward euthanasia for individuals with dementia and cognitive impairment found that religiosity was the main predictor of participants’ attitudes. 25
The present study
The literature review above revealed complex attitudes toward euthanasia for individuals with advanced AD among professionals, family caregivers, and the general public. As demonstrated, attitudes toward euthanasia vary depending on whether it is considered for oneself or for another individual, as well as on the specific circumstances involved. Moreover, these attitudes have been shown to be associated with various socioeconomic factors, cultural norms, and social values.
In the current study, we chose to focus on older adults, as AD is one of the most prevalent diseases in later life and affects millions of individuals and their family caregivers worldwide. Nevertheless, studies examining older adults’ attitudes toward euthanasia in the context of AD remain limited.
Therefore, the research questions were:
Methods
Participants and research context
A cross-sectional study was conducted among 501 older adults. Eligibility criteria included being aged 75 years or older, proficiency in Hebrew, and the ability to comprehend and respond to the study questionnaire. Participants were recruited using convenience sampling from seven adult day centers (four located in urban areas and three in rural areas), as well as from community centers nationwide, supplemented by snowball sampling. The adult day and community centers are attended by individuals who are cognitively intact but vary in their levels of physical functioning.
Prior to participation, all individuals were informed about the study's objectives and assured that participation was voluntary and anonymous. Written informed consent was obtained from all participants, who signed a consent form before being interviewed by trained interviewers. The questionnaires were administered by experienced interviewers who were graduate students in the medical and social sciences and who received extensive training from the research team. Interviewers followed a standardized interview protocol and ensured that participants responded only to the questions posed, without introducing additional topics. Interviews were conducted in private locations selected by the interviewers.
Ethical considerations
The study was approved by the Ethics committee of the Faculty of Health Sciences, Ben-Gurion University of the Negev (13-2017) in compliance with the Helsinki Declaration.
Measurements
Attitudes toward active euthanasia
Participants’ attitudes toward active euthanasia were measured via the following three cases:
Case A (unknown individual): An 80-year-old man diagnosed with AD. The patient has difficulty performing instrumental activities, recognizing family members, and suffers from delusions, increasing confusion, and disorientation. Due to his condition, he requires full-time care and supervision.
Case B (oneself): You are the 80-year-old man with AD described in Case A.
Case C (first-degree family member): The 80-year-old man with AD described in Case A is a first-degree relative of yours.
In all three cases, the patient had left a signed legal document requesting assistance in ending his life if he would no longer be able to make such a request himself due to his medical condition. For Case A, respondents were asked to rate their consent with the sentence: “The physician needs to inject the patient with a lethal dose of medication in order to terminate his life.” For Case B, respondents were asked to rate their consent with the sentence: “I would want the physician to inject me with a lethal dose of medication in order to terminate my life.” For Case C, respondents were asked to rate their consent with the sentence: “I would want the physician to inject my family member with a lethal dose of medication in order to terminate their life.” All three situations were rated on a six-point Likert scale: 1 (definitely disagree) 2 (disagree) 3 (somewhat disagree) 4 (somewhat agree) 5 (agree) 6 (definitely agree). The final score was computed as the average of participants’ ratings for each situation. The higher the score, the more positive the attitude toward active euthanasia. The cases were developed by the researchers, who consulted a psycho-geriatrician and social science professionals to ensure the face validity of the vignettes.
Sociodemographic variables
The sociodemographic variables included in the study were: age, gender, marital status, education and religiosity.
Psychosocial variables
This study is part of a larger research project, and the questionnaire containing these items was also used in a study conducted by Lifshitz et al. (2024). 31 Notably, whereas the present study focuses on AD, the previous study refers to a comparison between cancer and Parkinson's disease.
Analytic strategy
Means and standard deviations were computed using descriptive statistics. Associations between background and study variables were examined using Pearson, Spearman, or a chi-square correlation coefficient, according to the variables’ structures. Differences between group means were examined using t-tests conducted as two-tailed tests. Internal reliability was measured using Cronbach's alpha. Repeated measures analysis of variance (ANOVA) tests were performed to examine differences between the dependent variables. A series of linear regressions was conducted to explore the factors associated with attitudes in the three cases. Variables found to significantly correlate with at least one of the dependent variables in univariate analyses were included in the regression models. Only participants who provided complete responses to all items within the relevant step were included in the statistical analysis. Cases with missing data on any item in this step were excluded to ensure the consistency and validity of the statistical analyses. The significance level was set at p < 0.05 for all analyses. Data were analyzed using SPSS statistical software, PC version 28.0.
Results
The sample's sociodemographic characteristics are presented in Tables 1 and 2. Participants ranged from 75 to 94 years of age (M = 80.96, SD = 4.52), with the majority being women, married, and having a tertiary education. They rated their health condition as good and their economic status as average or higher.
Sociodemographic characteristics of the study participants (N = 501).
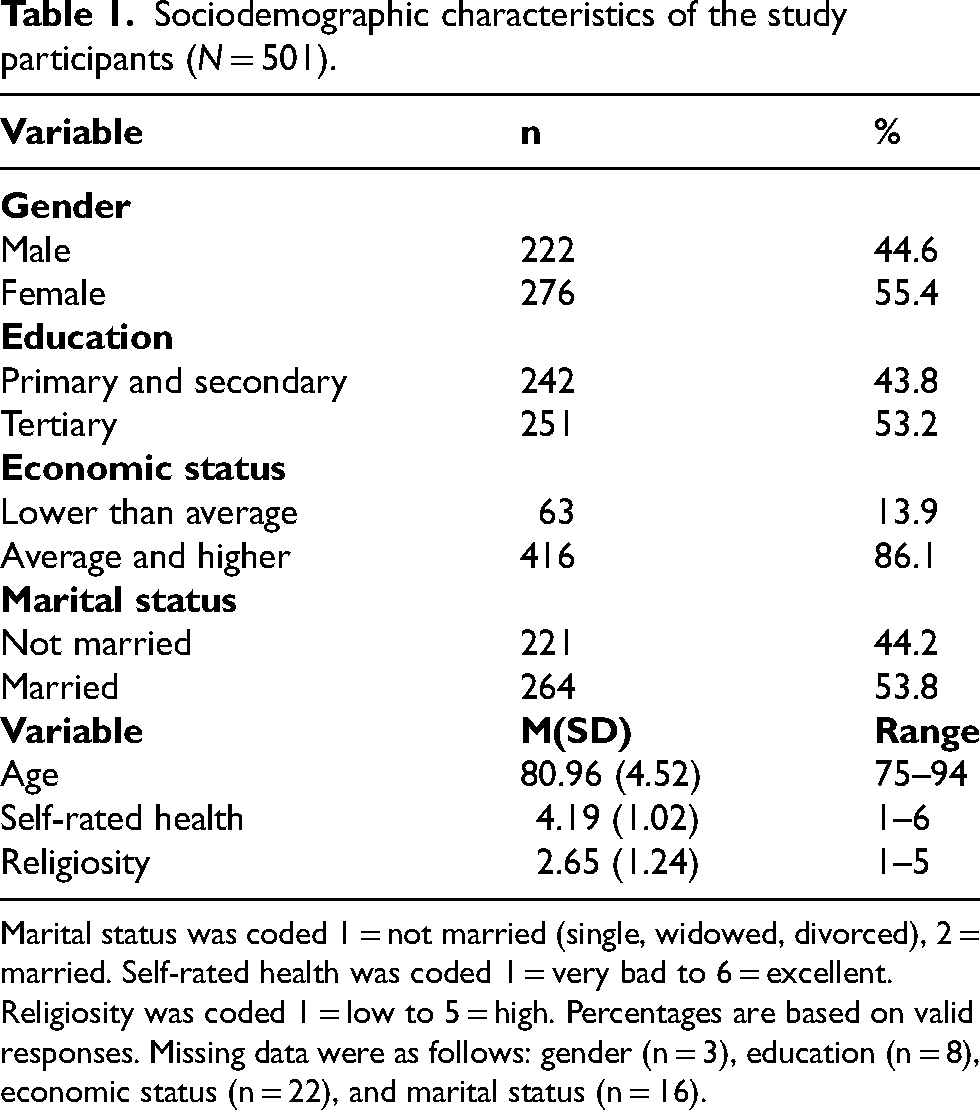
Marital status was coded 1 = not married (single, widowed, divorced), 2 = married. Self-rated health was coded 1 = very bad to 6 = excellent. Religiosity was coded 1 = low to 5 = high. Percentages are based on valid responses. Missing data were as follows: gender (n = 3), education (n = 8), economic status (n = 22), and marital status (n = 16).
Associations between the sample's sociodemographic characteristics, psychosocial variables, and attitudes toward active euthanasia (EUT) in the three cases (N = 495).
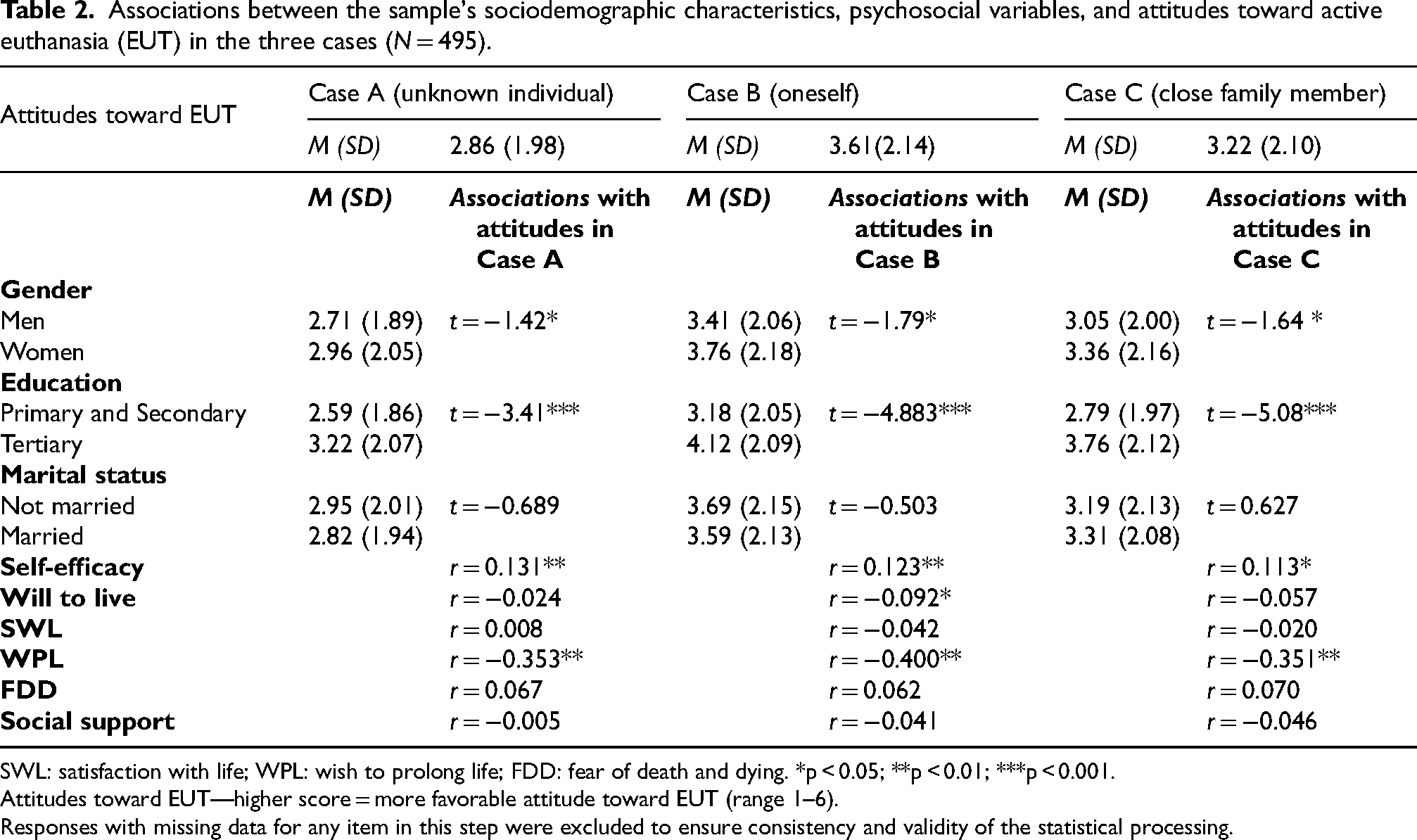
SWL: satisfaction with life; WPL: wish to prolong life; FDD: fear of death and dying. *p < 0.05; **p < 0.01; ***p < 0.001.
Attitudes toward EUT—higher score = more favorable attitude toward EUT (range 1–6).
Responses with missing data for any item in this step were excluded to ensure consistency and validity of the statistical processing.
Factors explaining attitudes toward euthanasia (EUT) for the three cases (N = 495).
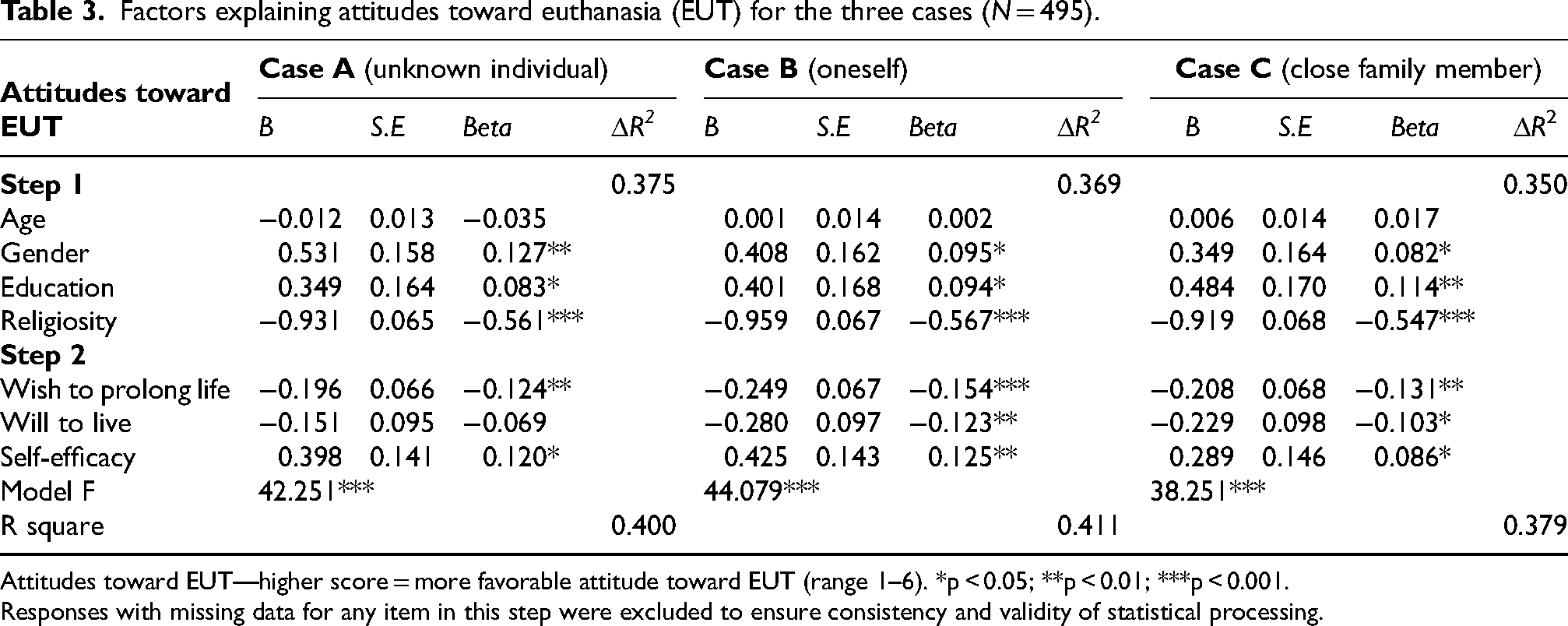
Attitudes toward EUT—higher score = more favorable attitude toward EUT (range 1–6). *p < 0.05; **p < 0.01; ***p < 0.001.
Responses with missing data for any item in this step were excluded to ensure consistency and validity of statistical processing.
Comparison of attitudes toward euthanasia among the three cases (RQ1)
The highest average score for positive attitudes toward active euthanasia was found in the case of oneself (Case B) (M = 3.61, SD = 2.14), followed by attitudes toward a family member (Case C) (M = 3.23, SD = 2.10) with the least favorable attitudes expressed toward an unknown individual (M = 2.86, SD = 1.98).
A one-way repeated-measures analysis of variance (ANOVA) was conducted to examine differences across the three vignettes. The analysis revealed a significant main effect of vignette, F(2, 980) = 60.44, p < 0.001, ηp2 = 0.11. Follow-up pairwise comparisons using the Least Significant Difference (LSD) method indicated that Case B elicited significantly higher scores than both Case C and Case A. Additionally, Case C elicited significantly higher scores than Case A (all ps < 0.001).
Descriptive statistics of study variables and their associations with attitudes toward euthanasia (RQ2)
The associations between attitudes toward euthanasia in the three cases and the study variables are presented in Table 2. Significant negative correlations between age and attitudes toward euthanasia were found in all three cases: Case A (r = −0.159) Case B (r = −0.129) Case C (r = −0.110), as well as negative correlations between religiosity levels and attitudes toward euthanasia in all cases (r = −0.594, r = −0.603, r = −0.579, respectively). Young and secular participants manifested more positive attitudes toward euthanasia in Cases B and C than did other participants (full matrix available from second author upon request).
Differences in attitudes toward euthanasia regarding dichotomous variables—gender, marital status, and education level—were tested using an independent t-test (shown in Table 2). Significant differences were found between men and women in all cases (Case A t(493) = −1.42, p = 0.021; Case B t(493) = −1.79, p = 0.036; Case C t(490) = −1.64, p = 0.050). Women reported more positive attitudes toward euthanasia in all conditions (M = 2.96, SD = 2.05; M = 3.76, SD = 2.18; M = 3.36, SD = 2.16, respectively) than did men (M = 2.71, SD = 1.89; M = 3.41, SD = 2.06; M = 3.05, SD = 2.00, respectively). Also, significant differences were found between participants with different levels of education in all three cases: in Case A t(468) = − 3.41, p < 0.001, in Case B t(469) = −4.88, p < 0.001, and in Case C t(466) = −5.08, p < 0.001. Participants with a tertiary education reported more positive attitudes toward euthanasia in all three cases (M = 3.22, SD = 2.07; M = 4.12, SD = 2.09; M = 3.76, SD = 2.12, respectively) than did participants with a primary or secondary education (M = 2.59, SD = 1.86; M = 3.18, SD = 2.05; M = 2.79, SD = 1.97, respectively). No significant differences were found between the cases in terms of marital status.
Two psychosocial variables were found to be significantly associated with attitudes toward euthanasia in all three cases: self-efficacy and the wish to prolong life. In all three cases, positive attitudes toward euthanasia positively correlated with self-efficacy and negatively with the wish to prolong life. Additionally, in Case B, positive attitudes toward euthanasia were negatively associated with the will to live (see Table 2).
A correlation matrix between all the psychosocial variables themselves was conducted. The associations were found to be in the range of r = 0.093 (between social support and the wish to prolong life) to r = 0.568 (between self-efficacy and satisfaction from life). (The full correlation matrix is available from the second author upon request).
Regression analyses of variables explaining attitudes toward euthanasia in each of the three cases (RQ2)
Three hierarchal regressions were applied separately to explain attitudes toward euthanasia in the three cases: A (unknown individual), B (oneself), and C (close family member) Table 3. The two steps were identical for all three regressions. In the first step, sociodemographic characteristics were entered, including age, gender, education, and religiosity level. The second step included three psychosocial variables: the wish to prolong life, the will to live, and self-efficacy. In Case A, more positive attitudes toward euthanasia were found among women, with higher education, lower religiosity, lower wish to prolong life and higher self-efficacy F(7, 443) = 42.251, p < 0.001. In Case B, more positive attitudes were found among women, with higher education, lower religiosity, lower wish to prolong life, lower will to live, and higher self-efficacy, F(7, 449) = 44.079, p < 0.001. In Case C, more positive attitudes were found among women, with higher education, lower religiosity, lower wish to prolong life, lower will to live, and higher self-efficacy, F(7, 446) = 38.251, p < 0.001. As for the models explained variance, the model for oneself explained 41% of the observed variance, followed by the model for an unknown individual (40%) and by the model for close family member (38%).
Discussion
The aim of the current study was to examine differences in older adults’ attitudes toward active euthanasia in advanced AD in three different cases: for themselves, for family members, and for an unknown individual. Additionally, we explored the associations between sociodemographic characteristics, psychosocial factors, and attitudes toward active euthanasia in these three cases.
The findings indicated that attitudes toward active euthanasia were highest when considering oneself, followed by a family member, and lowest when considering an unknown individual. These observed gradients in attitudes toward active euthanasia may be understood in light of differences in psychological proximity, perceived autonomy, and moral responsibility across the three scenarios. When respondents considered themselves, support for active euthanasia was highest, likely reflecting a strong emphasis on personal autonomy, self-determination, and certainty regarding one's own preferences at the end of life-concerns that become particularly salient in later life as individuals anticipate functional decline and loss of independence.33,34 In contrast, attitudes were less favorable when the subject was a family member, a context that introduces heightened emotional involvement, caregiving roles, and moral responsibility, all of which are especially pronounced in gerontological contexts. These factors may generate ambivalence, even when euthanasia is perceived as a means of alleviating suffering, particularly in the presence of uncertainty about the older family member's true wishes. 35 Attitudes were least favorable toward an unknown individual, consistent with Construal Level Theory, which posits that greater social distance leads to more abstract and normatively constrained moral judgments. 36 In older populations, this distance may also activate concerns about age-related vulnerability and the potential for misuse, contributing to greater ethical caution and lower endorsement of active euthanasia. 37
Another explanation for differences in attitudes toward active euthanasia may relate to the stigma associated with AD. AD is a highly stigmatized condition, and individuals living with AD, as well as their family caregivers, are often exposed to negative stereotypes, prejudice, and discrimination, which are associated with increased shame, social isolation, and psychological distress.38,39 This stigma may shape attitudes toward AD both at the personal and familial levels, reinforcing fears surrounding the diagnosis and its anticipated consequences.40,41
In particular, self-stigma, the internalization of negative societal beliefs, has been shown to adversely affect the emotional well-being of older adults with AD, contributing to feelings of shame, anxiety, depression, and social withdrawal, as well as delays in help-seeking.40,42,43 Fear of living with a stigmatized condition such as AD may therefore increase the desire to avoid prolonged life with the disease, helping to explain why participants expressed more favorable attitudes toward active euthanasia for themselves than for family members or an unknown individual.
Relatively favorable attitudes toward active euthanasia in the case of family members may further be understood through the concept of stigma by association. Family members and caregivers of individuals with AD often experience “spillover” stigma, including social judgment and marginalization due to their association with the person with the illness.44,45 This shared stigmatizing experience may increase caregivers’ empathy for the anticipated suffering associated with AD, thereby contributing to more supportive attitudes toward active euthanasia for a family member than for an unknown individual.
A third possible explanation relates to expectations of experiencing a “good death” if one were to develop AD. The concept of a good death emphasizes dying in a planned, peaceful, and dignified manner, ideally at home and in the presence of loved ones. 46 Individuals may endorse active euthanasia for themselves as a means to achieve such a death. Support decreases for family members and unknown individuals because people may feel less certain about the preferences of others and less able to ensure that the death would meet these ideals, reflecting the influence of relational closeness and knowledge of the person's wishes. This perspective highlights that the gradient in attitudes, from oneself to a family member, to an unknown individual, may reflect both the desire to secure a good death and the confidence in one's ability to honor it.
The findings of the current study also demonstrated correlations between sociodemographic factors and attitudes toward active euthanasia. Significant negative correlations between age and attitude
Another significant finding of this study was the negative correlation between religiosity and attitudes toward active euthanasia in all three cases described in the vignettes. In the current study, religiosity was a main factor that influenced the attitudes of older adults toward active euthanasia, a finding that is consistent with previous studies. A study conducted in the Netherlands revealed that 60% of the public agreed that people with advanced dementia should be eligible for euthanasia, whereas religion was associated with a lower acceptance of euthanasia. 50 An additional study conducted among older Dutch adults aged 79–100 found that attitudes toward euthanasia varied on the basis of religiosity, with more religious individuals being less supportive of euthanasia. 51
Psychosocial characteristics (in addition to sociodemographic factors) were also associated with attitudes toward active euthanasia. Our study revealed that self-efficacy was positively correlated with attitudes toward active euthanasia in all three cases described in the vignettes. A recent study that compared attitudes toward active euthanasia in Parkinson's disease and cancer found that higher self-efficacy contributed to more favorable attitudes toward euthanasia in both end-of-life conditions. 31 In a study conducted in Belgium among 196 nurses it was found that nurses’ involvement in advance care planning practices was primarily linked to their self-efficacy. 52 It may be that when people believe they are able to successfully perform an activity (in this case active euthanasia), they hold more positive attitudes toward it.
Finally, and unsurprisingly, the wish to prolong life was negatively correlated with attitudes toward active euthanasia in all three cases. Similarly, in a study conducted among 195 family caregivers of people with dementia examine their willingness to undertake advance care planning for themselves, it was found that the wish to prolong life was negatively related to their attitudes toward advance care planning. 53 Similar correlations have been found in previous studies as well.29,54
Limitations and future research
The current study has few limitations. First, its cross-sectional design does not allow for tracking changes in attitudes or making causal interpretations, thereby it constrains internal validity. Second, we did not use a counterbalanced design in the study, which could have affected the findings. Third, the sample comprised older Jewish adults who were highly educated and had a relatively high economic status. Given these limitations and the use of a convenience sampling method, the sample is probably not representative of the broader Israeli older population, limiting the external validity. Moreover, because the vignettes focused specifically on AD, the findings may not be generalizable to the broader spectrum of dementias or to more detailed clinical contexts. Additionally, a significant portion of the recruitment occurred during the COVID-19 pandemic, which may have influenced unforeseen ways the participants’ attitudes toward active euthanasia.
Going forward, researchers should explore attitudes toward active euthanasia among broader populations, including family caregivers, healthcare professionals, and the public. In addition, future studies should incorporate the perspectives of diverse cultural and ethnic groups to better understand how cultural background influences experiences and decision-making related to end-of-life care, both for oneself and for significant others.
Conclusion
Attitudes toward active euthanasia were highest for oneself, followed by a family member, and lowest for an unknown individual. This pattern reflects three factors: psychological proximity and autonomy, with stronger support when personal preferences are clear; stigma related to AD, where self-stigma and stigma by association increase concern about suffering; and expectations of a “good death,” with support decreasing as relational distance grows due to uncertainty about others’ preferences and ability to ensure dignity. These findings underscore the need to reduce AD-related stigma and raise public awareness to promote informed and compassionate end-of-life decision-making.
Our findings also indicate that attitudes toward active euthanasia are correlated with various sociodemographic and psychosocial characteristics. Older age, being female, having higher education level, lower levels of religiosity, greater self-efficacy and lower wish to prolong life were the main factors explaining attitudes toward active euthanasia in advanced AD. These characteristics should be considered when developing strategies to raise public awareness about active euthanasia, particularly among older adults. Expanding the dialogue on active euthanasia in AD among the public, family caregivers, and healthcare professionals may support more informed, values-based decision-making that respects individual preferences and promotes autonomy at the end of life.
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
The study was approved by the Faculty of Health Sciences at Ben-Gurion University of the Negev, Beer-Sheva, Israel.
Consent to participate
The participants provided their written informed consent for participation in this study.
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Israel National Institute for Health Policy Research (No. 204/2018).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.