
Abstract
Background
Cerebrospinal fluid (CSF) pTau181 is used to support Alzheimer's disease (AD) diagnosis but can also rise in amyloid-negative individuals. This CSF profile (Aβ−/pTau181+) lies outside the AD continuum and complicates real-world etiologic diagnosis of neurocognitive disorders.
Objective
To determine the prevalence and clinical phenotype associated with the Aβ−/pTau181+ CSF biomarker profile in a real-world memory clinic population.
Methods
We screened the Mount Sinai Hospital database (2015–2024) for patients who underwent ADmark CSF biomarker testing. An Aβ−/pTau181+ group was classified using assay cutoffs (Amyloid-Total-Tau Index>1.2, pTau181 > 54 pg/mL) and compared to an Aβ+ group (Amyloid-Total-Tau Index<0.8) matched for pTau181 and total-Tau. Clinical variables were extracted via chart review, limited to notes preceding CSF and blinded to CSF results.
Results
The Aβ−/pTau181+ group included 25 individuals (10.1% of the cohort) and had equally impaired cognition but fewer episodic memory complaints. Diagnosis was more often Lewy body or frontotemporal dementia. On neuroimaging, Aβ−/pTau181+ exhibited less white matter hyperintensity burden and temporoparietal atrophy.
Conclusions
CSF Aβ−/pTau181+ is frequent in real-world evaluations of cognitive impairment and presents with fewer AD phenotypic features. Further research is required to clarify Aβ−/pTau181+ underlying biology and clinical trajectory.
Keywords
Introduction
The interpretation of positive hyperphosphorylated tau fluid biomarkers has undergone substantial evolution over the past two decades, as reflected in successive National Institute on Aging and Alzheimer's Association (NIA-AA) diagnostic frameworks for Alzheimer's disease (AD).1–3 In the 2018 framework, cerebrospinal fluid (CSF) tau phosphorylated at threonine 181 (pTau181) was proposed as an early marker of neurofibrillary tangles (NFT), positioned upstream of neurodegenerative biomarkers. In the revised 2024 framework, pTau181 is considered upstream of cortical NFT formation and more closely associated with brain amyloid-β (Aβ). While both frameworks interpret pTau181 primarily in the context of Aβ positivity, it can rise above cut-off values in individuals with negative Aβ status based on CSF, amyloid PET and postmortem studies.4–10 This discordant CSF biomarker profile (Aβ−/pTau181+) lies outside the biological AD continuum yet is categorized within the AT(N) framework, making its clinical interpretation challenging in individuals with cognitive impairment.
Research on Aβ − /pTau181 + CSF profile to date has limited applicability to real-world clinical practice. This is because most studies are based on research cohorts of cognitively unimpaired individuals or studies that systematically exclude participants with non-AD syndromes, psychiatric disorders, parkinsonism or markers of cerebrovascular disease.11–13 This selection bias results in poor generalizability to memory clinic populations, where presentations are heterogeneous and biomarker testing is often prompted by atypical or mixed syndromes.
Our goal was to conduct a preliminary assessment of the prevalence and clinical phenotype of the Aβ−/pTau181+ profile in a real-world memory clinic population. To better understand this biomarker profile's features, we compared this group to individuals with Aβ positive CSF profiles. This approach was intended to highlight characteristics of individuals with positive pTau181 that occur independently of amyloid pathology.
Methods
Participants
This study was conducted at the Icahn School of Medicine at Mount Sinai. Data were pulled via the institutional data warehouse, a real-world clinical data repository integrating structured data from the electronic health record across the Mount Sinai Health System. Institutional Review Board approval was obtained, and all data access complied with institutional privacy and ethical standards. The data warehouse was queried to identify all patients who had undergone CSF testing for Aβ1−42, pTau181, and total tau (tTau) between 12/2015 and 12/2024.
Patients were evaluated on an outpatient basis within the Division of Cognitive Neurology, the Barbara and Maurice Deane Center for Wellness and Cognitive Health, a tertiary referral center for mild cognitive impairment (MCI) and dementia serving New York State and the broader tri-state area. A smaller subset was from other outpatient neurology subspecialty clinics, including movement disorders, vascular neurology, and general neurology.
Patients evaluated in the division routinely undergo comprehensive neurobehavioral phenotyping, including structured assessment of neurodegenerative symptoms, the Katz and Lawton-Brody instruments for measuring basic and instrumental activities of daily living (BADLs and IADLs),14,15 and bedside cognitive screening with the Montreal Cognitive Assessment (MoCA). Brain MRI is routinely performed as part of the standard diagnostic work-up.
CSF biomarker analysis
Samples were analyzed using the Alzheimer's Disease Evaluation panel by Athena Diagnostics (ADmark®), the sole panel used at the Mount Sinai Health System during the study period. This panel utilizes a standardized sandwich enzyme-linked immunosorbent assay (ELISA) platform to quantify core CSF AD biomarkers: Aβ1−42, pTau181, and tTau. These assays have previously shown high correlation with AD pathology at autopsy16–20 and amyloid PET imaging.21–24 All CSF samples were collected and processed according to ADmark standard procedures, including collection into polypropylene tubes and proper storage until analysis.
Defining subgroup of interest
Subgroups were defined using the ADmark Amyloid Tau Index (ATI, see Formula 1) and pTau181 values. The ATI incorporates CSF Aβ1−42 and tTau values to predict positive Aβ status, with restrictive cutoffs below 0.8 or above 1.2, indicative of Aβ-positive and Aβ-negative status, respectively.17,19 Participants with very low CSF tTau levels (<150 pg/mL) were excluded, as such values can artificially elevate ATI scores despite low (positive) CSF Aβ1−42. An Aβ − /pTau181 + group was then defined with ATI > 1.2 and pTau181 > 54 pg/mL, the recommended threshold indicative of neurofibrillary tangle pathology.18–20 A comparison Aβ+ group (ATI < 0.8) was generated via one-to-one unrestricted nearest-neighbor matching on both pTau181 and tTau values. Matching on tTau was necessary given its contribution to ATI values.
Both groups subsequently underwent retrospective chart review by two behavioral neurologists (O.K. and F.E.) blinded to biomarker status. Clinical notes reviewed were limited to those preceding CSF testing to minimize bias from knowledge of biomarker results. Brain MRI evaluation by reviewers was blinded to clinical notes and biomarker status.
Gray matter regional brain atrophy was assessed using visual atrophy scores for six brain regions,25–27 consisting of an ordinal scale with higher scores representing worse atrophy.27,28 Regions assessed included anterior and medial temporal regions (scores range 0-5), orbitofrontal cortex, anterior cingulate cortex, fronto-insular and posterior parietal lobes (scores range 0–4). Scores for each region were summed for each of the hemispheres. Cerebrovascular disease burden was evaluated using a visual rating scale that included white matter hyperintensities (WMH, aka Fazekas), lacunar infarcts and cerebral microbleeds. 29 Raters had formal training in applying scores with high inter-rater agreement.
Annotated chart data and neuroimaging findings were used to re-evaluate each patient's clinical diagnosis. Diagnosis was conducted in consensus between the two reviewers and in accordance with established dementia diagnostic criteria.30–36
Analysis
Comparisons of Aβ+ and Aβ − /pTau181 + groups included CSF, demographics, clinical, cognitive, and imaging variables. Continuous variables were analyzed using two-tailed independent-samples t-tests when assumptions of normality were met. For ordinal and non-normally distributed variables, group comparisons were conducted using the Mann–Whitney U test, and values were reported as medians with interquartile ranges (IQR). Categorical variables were analyzed using Fisher's exact test; exact p-values were estimated via a Monte Carlo procedure with 1,000,000 permutations when expected counts in any cell were <5. Statistical significance was defined as α = 0.05 for all comparisons. All analyses and visualizations were conducted in R (version 2025.05.1, Build 513).
Results
Prevalence of Aβ − /pTau181 +
During the study period, 247 individuals underwent CSF testing for AD biomarkers and had a complete set of core biomarkers available for analysis (see Figure 1 for the participant flowchart). The distribution of ATI and pTau181 values across the cohort is shown in Figure 2. Twenty-five individuals (10.1%) met criteria for an Aβ − /pTau181 + CSF profile. Individuals in this group were matched on pTau181 and tTau values with 25 individuals with Aβ positive status indicated by ATI < 0.8.

Flow diagram of participant selection and CSF biomarker classification (STROBE guidelines).

Distribution and comparison of CSF biomarker values across Aβ−/pTau181+ and Aβ+/pTau181+ profiles.
Comparison of Aβ−/pTau181+ and Aβ+/pTau181+
As expected, based on study design, the groups diverged on CSF biomarkers and biomarker combinations that indicate Aβ status. The Aβ − /pTau181 + had higher concentrations of CSF Aβ1−42 (1214 ± 190 versus 477 ± 106, p < 10−18, Figure 2), higher ATI (1.75 ± 0.37 versus 0.63 ± 0.14, p < 10−14), lower pTau181 to Aβ1−42 ratio (0.06 ± 0.01 versus 0.17 ± 0.06, p < 10−10) and tTau to Aβ1−42 ratios (0.33 ± 0.09 versus 0.98 ± 0.37, p < 10−10).
Post-matching comparisons of groups indicated no appreciable differences with regards to demographics, dementia risk factors or time from onset to evaluation (Table 1). Non-significant trends included younger symptom onset (62.91 ± 10.68 versus 67.86 ± 8.33 years, p = 0.08) and more men (16 versus 9, p = 0.09) in the Aβ−/pTau181 + group. Importantly, groups were equally impaired on baseline scores of cognitive testing, functional independence and MCI diagnosis.
Demographic, clinical, and CSF biomarker comparisons between Aβ−/pTau181+ and Aβ+/pTau181+ groups.
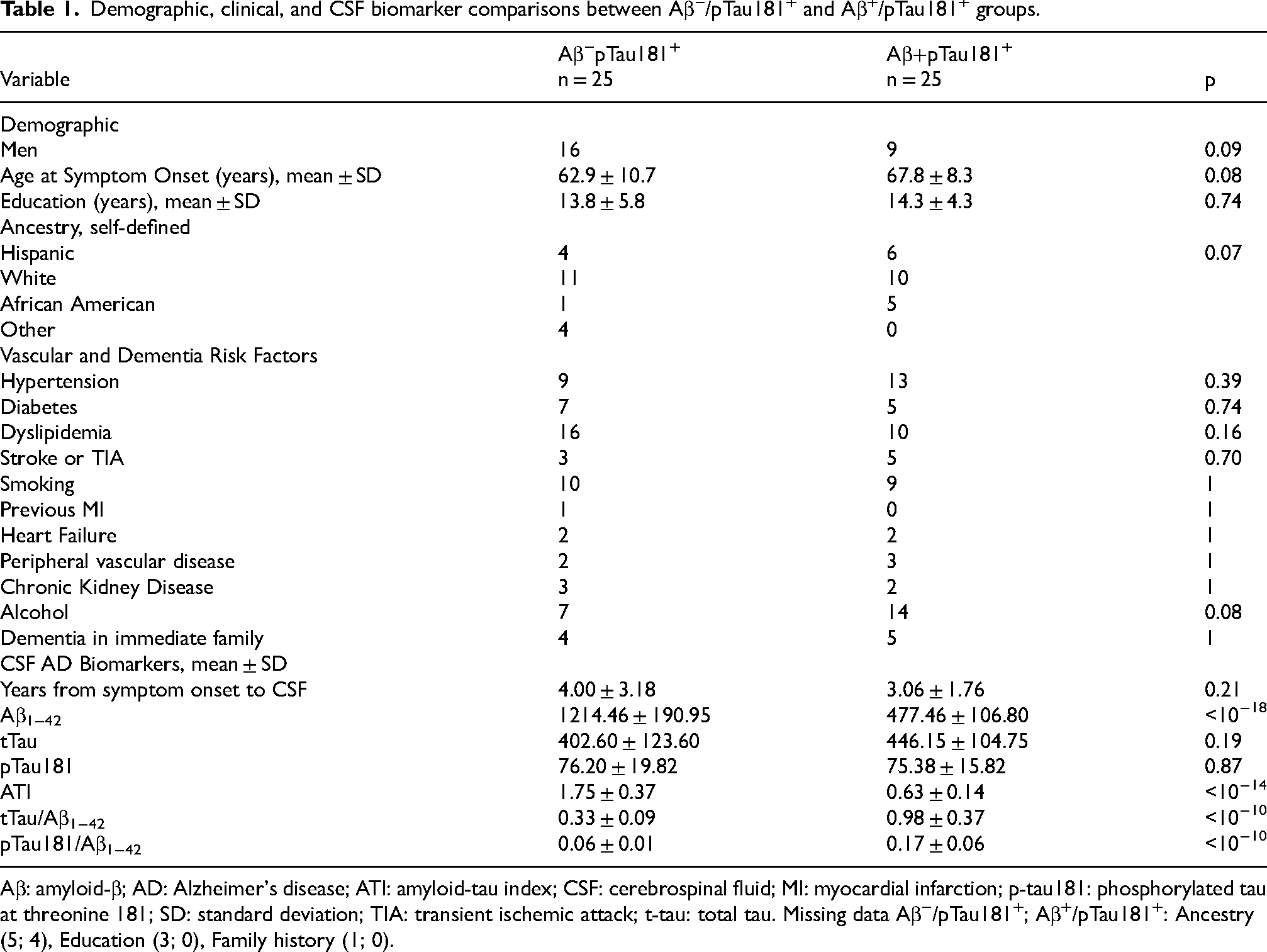
Aβ: amyloid-β; AD: Alzheimer's disease; ATI: amyloid-tau index; CSF: cerebrospinal fluid; MI: myocardial infarction; p-tau181: phosphorylated tau at threonine 181; SD: standard deviation; TIA: transient ischemic attack; t-tau: total tau. Missing data Aβ−/pTau181+; Aβ+/pTau181+: Ancestry (5; 4), Education (3; 0), Family history (1; 0).
The Aβ − /pTau181 + group presented with less episodic memory-related complaints (7 versus 15, p = 0.046), whereas no differences were identified in the frequency of other symptoms or in neurological examination findings (Table 2). The Aβ − /pTau181 + group exhibited a heterogeneous distribution of clinical diagnoses (p = 0.004), in particular much less clinical AD (2 versus 13). Interestingly, the Aβ−/pTau181+ group included four uncommon causes for cognitive impairment: antiphospholipid antibody syndrome, progressive cerebellar ataxia, idiopathic normal pressure hydrocephalus and late-life progressive mitochondrial encephalopathy. Two Aβ−/pTau181+ patients were classified as subjective memory complaints via serial neuropsychological testing spanning more than 3 years after CSF testing.
Cognitive, clinical, and neuroimaging comparisons between Aβ−/pTau181+ and Aβ+/pTau181+ groups.
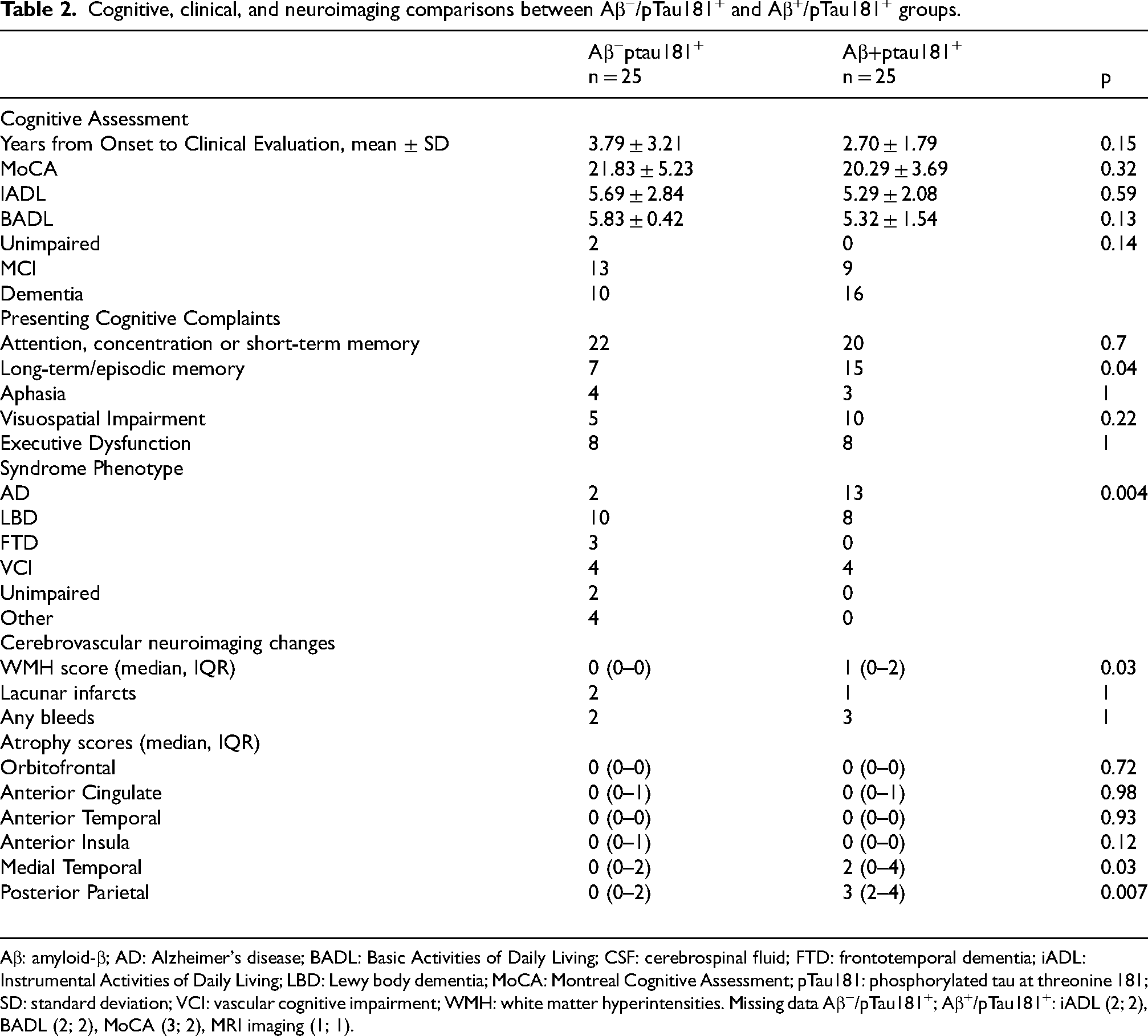
Aβ: amyloid-β; AD: Alzheimer's disease; BADL: Basic Activities of Daily Living; CSF: cerebrospinal fluid; FTD: frontotemporal dementia; iADL: Instrumental Activities of Daily Living; LBD: Lewy body dementia; MoCA: Montreal Cognitive Assessment; pTau181: phosphorylated tau at threonine 181; SD: standard deviation; VCI: vascular cognitive impairment; WMH: white matter hyperintensities. Missing data Aβ−/pTau181+; Aβ+/pTau181+: iADL (2; 2), BADL (2; 2), MoCA (3; 2), MRI imaging (1; 1).
On MRI, the Aβ−/pTau181+ group had on average lower atrophy scores in medial temporal regions (median (IQR) 0(0-2) versus 2(0-4), p = 0.03) and posterior parietal (0(0-2) versus 3 (2-4), p = 0.0007) regions. Average WMH score was also lower in Aβ−/pTau181+ group (median (IQR) 0(0-2) versus 1(0-2), p = 0.03).
Discussion
In this real-world memory clinic study, 10% of individuals undergoing CSF analyses for AD biomarkers had an Aβ−/pTau181+ profile. Compared to Aβ+ individuals, the Aβ−/pTau181+ group was, on average, less likely to report symptoms of decline in episodic memory and less frequently diagnosed with a clinical AD syndrome. Review of neuroimaging demonstrated Aβ−/pTau181+ had less temporoparietal atrophy and lower burden of WMH. Despite these differences, both groups exhibited comparable levels of cognitive impairment and functional decline. Our findings underscore the importance of studying AD biomarker profiles outside of research cohorts and in real-world clinical settings, particularly for subgroups that do not follow expected sequences of biomarker positivity. 1
Our observation of a non-AD pattern of cognitive impairment in Aβ−/pTau181+ profile aligns with the broader construct of SNAP (suspected non-Alzheimer's pathophysiology). 4 SNAP is a biomarker construct developed within the AT(N) framework to account for individuals with negative Aβ but evidence of neurodegeneration, defined by elevated CSF pTau181, increased tTau, or medial temporal atrophy. Individuals meeting SNAP criteria and cognitive impairment present with non-amnestic MCI and are about three times more likely to develop non-AD syndromes.5,37 More recent work, however, emphasizes that SNAP represents a heterogeneous group of Aβ negative pathologies. 38 Among these, SNAP with medial temporal atrophy has been associated with Limbic-predominant age-related TDP-43 encephalopathy (LATE-NC). 39 Because LATE-NC occurs predominantly in advanced age, typically after 80 years, it is less likely to explain cases in younger cohorts such as ours.
Studies focusing specifically on the Aβ−/pTau181+ profile, however, remain sparse. One memory clinic study in France reported this biomarker profile with a frequency of ∼4%, with most individuals exhibiting an FTD or another non-AD clinical phenotype. 40 In contrast, analyses from the ADNI and WISC research cohorts suggested that Aβ−/pTau181+ confers a relatively benign prognosis, similar to biomarker-negative cases. 6 Our results are more consistent with the results from memory clinic cohort, indicating that the Aβ−/pTau181+ profile can be observed in individuals evaluated for cognitive impairment in routine clinical practice. This discrepancy likely reflects the more symptomatic and diagnostically heterogeneous nature of real-world clinical populations compared to biomarker-focused research cohorts in unimpaired individuals. However, in the absence of a cognitively unimpaired comparison group, we could not assess whether this biomarker profile is enriched in impaired individuals relative to the general population. Previous postmortem studies of non-AD neuropathology documented elevated CSF pTau181 and even an Aβ−/pTau181+ profile. Although the Aβ−/pTau181+ biomarker profile is uncommon within any single non-AD pathology, its cumulative frequency may become relevant in real-world populations. The Aβ−/pTau181+ profile has been reported in up to 10% of autopsy-confirmed Lewy body disease cases.8,10,41,42 Elevated CSF pTau181 is found in roughly 20% of FTLD-tau and much less frequently in FTLD-TDP-43.8,10 It has also been described in Creutzfeldt–Jakob disease. 9 There are currently no published CSF studies of pTau181 in Primary Age-Related Tauopathy (PART). Data from confirmed LATE-NC are similarly sparse, as most studies have relied on antemortem amyloid PET rather than CSF biomarkers.5,38,43
We interpret the existence of an Aβ−/pTau181+ CSF profile in two ways: misclassified amyloid status (i.e., an error in Aβ measurement) or as a reflection of non-AD neuropathology. Support for the latter comes from recent multimodal biomarker studies of clinically defined Aβ−/pTau181+ cases, which demonstrated both low rates of amyloid PET positivity and minimal tau PET uptake. 6 These findings align more closely with alternative, non-AD neurobiology than with misclassification of AD. We therefore suspect that, in the absence of brain Aβ, elevated CSF pTau181 reflects tau phosphorylation arising in other neuropathologies8,41,42,44–46 (e.g., vascular, Lewy body disease, FTLD-tau). In our study, the WMH burden was slightly greater in the Aβ-positive group. Prior studies show that WMH are common in Alzheimer's disease and may reflect Wallerian degeneration, cerebral amyloid angiopathy, or mixed cerebrovascular processes rather than purely ischemic small vessel disease. 47 Key strengths of this study include the use of clinically acquired CSF and imaging data, rigorous phenotyping through chart review by expert behavioral neurologists, and a focus on a diagnostically diverse, real-world patient population, underscoring the relevance and generalizability of our findings. The use of tau-based matching further enabled clearer attribution of group differences to positive Aβ status.
Several limitations must be acknowledged. The relatively small sample size limits the power to detect subtle effect sizes. Our real-world cohort lacks advanced biomarker and pathological validation (e.g., quantitative neuroimaging, tau PET, biomarkers for α-synuclein, or autopsy). These tests could better define the primary pathologies of relevance to Aβ−/pTau181+ but are not obtained in routine clinical care. Secondary measures of Aβ status, such as amyloid PET or plasma pTau217, could have supported group classification beyond CSF alone. The CSF AD biomarkers were analyzed via ADmark® ELISA in a clinical lab, and thus with potentially higher variability than automated electrochemiluminescence assays currently used in international quality control initiatives. 48 This may have led to misclassification of amyloid or tau status in some individuals. Nevertheless, individual-level measurement variability was mitigated using biomarker composite measures (i.e., ATI) and individual matching.
In conclusion, our findings suggest that the Aβ−/pTau181 + CSF profile is not uncommon in memory clinic populations and reflects a clinically heterogeneous group. While plasma pTau217 becomes increasingly integrated into the diagnostic workflow for cognitive complaints, CSF remains one of the gold-standard confirmatory tests, particularly in atypical cases of MCI and dementia. 49 Our findings suggest that, in the absence of amyloid positivity, CSF pTau181 elevation should be interpreted cautiously. Clinical history, examination, and imaging should be reviewed to ensure appropriate context for subsequent biomarker testing and interpretation. The findings underscore the need for combined biomarker- and neuroimaging- informed phenotyping of phosphorylated tau elevation in the absence of amyloid pathology, and expansion of biomarker panels to better capture etiological molecular drivers of neurodegeneration.
Footnotes
Acknowledgements
The authors acknowledge with appreciation the patients and families of the Mount Sinai Memory Clinic for their invaluable contributions to clinical research. This work was supported in part through the Mount Sinai Data Warehouse (MSDW) resources and staff expertise provided by Scientific Computing and Data at the Icahn School of Medicine at Mount Sinai.
Ethical considerations
This retrospective chart-review study was approved by the Institutional Review Board of the Icahn School of Medicine at Mount Sinai.
Consent to participate
The requirement for informed consent was waived owing to minimal risk and the use of existing clinical data collected during routine care.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: FME's research is supported by the National Institute on Aging and Department of Veterans Affairs IK2CX002180 and Mount Sinai ADRC P30AG066514, Chan Zuckerberg Initiative, Rainwater Charitable Foundation, DataPhilanthropy, Rockefeller Philanthropy Advisors fund. SG's research is supported Cure Alzheimer's Fund grant and Mount Sinai ADRC grant P30AG066514.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available from the corresponding author upon reasonable request.