
Abstract
Background
Glymphatic system dysfunction is linked to cognitive decline in dementia continuum. Diffusion magnetic resonance imaging markers like the Diffusion Tensor Image Analysis Along the Perivascular Space (DTI-ALPS) index and whole-brain free water (FW) fraction allow non-invasive evaluation of glymphatic activity.
Objective
This study assessed whether DTI-ALPS and FW fraction are associated with cognitive performance and examined the influence of factors such as education on these relationships across dementia stages.
Methods
Cognitively normal, mild cognitive impairment, and dementia participants were recruited from both the community and the memory clinic at Chang Gung Memorial Hospital, Keelung. Brain MRI and neuropsychological assessments were performed.
Results
A total of 127 individuals (Clinical Dementia Rating 0, 0.5, 1–3; N = 75, 43, 6) completed the study. Both DTI-ALPS index and FW fraction differed among groups (p < 0.001) and correlated with cognitive performance (DTI-ALPS: β = 0.35; FW: β = −0.50; both p < 0.001). Mediation analysis showed that DTI-ALPS was positively associated with Montreal Cognitive Assessment (total effect b = 21.94, p < 0.001), largely mediated by FW fraction (indirect β = 0.22, 95% CI [0.14–0.33]). After adjusting for age, sex, and education, the total effect remained significant (b = 10.93, p = 0.018), while the direct effect was not (b = 8.15, p = 0.080), and the indirect effect via FW persisted (β = 0.05, 95% CI [0.01–0.13]). Education moderated these associations (DTI-ALPS x education: b = −2.07, p = 0.033; FW x education: b = 5.59, p = 0.034). In addition, sleep-medication use interacted with FW fraction in relation to cognitive performance (FW x sleep-medication: b = −58.87, p = 0.044).
Conclusions
DTI-ALPS index and FW fraction provided complementary insights into glymphatic dysfunction linked to cognitive decline. Higher DTI-ALPS values were associated with better cognition, mediated by lower whole-brain FW, but with attenuated effects in individuals with higher education.
Keywords
Introduction
Dementia progresses along a continuum rather than as discrete categories. The pathology of Alzheimer's disease (AD) emerges prior to the onset of detectable clinical symptoms and advances in a continuous manner. Its phenotypic presentation comprises a spectrum of neuropsychiatric disorders, rather than occurring through abrupt stages of decline.1–3 Despite this understanding, the mechanistic pathways that connect dementia risk factors and continuous biological and clinical progression remain incompletely understood.
The glymphatic system regulates waste clearance and interstitial fluid dynamics. It operates brain water metabolism through a directed fluid pathway, moving from arterial perivascular space, interstitial spaces, toward venous perivascular space. This process depends on the active transport of water via aquaporin 4 (AQP4) channels located at the astrocytic end-feet. The glymphatic system works in conjunction with the cervical lymphatic system to accomplish a complete water circulation of the brain.4,5 Aging and AD pathology reduce glymphatic efficiency, with AQP4 polarity loss and reduced amyloid and tau clearance.4,6 Diffusion Tensor Image Analysis Along the Perivascular Space (DTI-ALPS) index is a non-invasive surrogate marker from diffusion MRI for glymphatic activity, emerging as a clinically feasible imaging marker of glymphatic transport efficiency. 7 Reduced DTI-ALPS values have been linked to aging8,9 and AD.4,7 The DTI-ALPS index also serves as a mediator, as demonstrated in a multimodal neuroimaging study combining amyloid PET, tau PET, and diffusion MRI. 10 Therefore, the DTI-ALPS index is a clinically feasible surrogate marker of glymphatic dysfunction in dementia continuum.
The free water (FW) fraction of the brain is a diffusion MRI-based marker that measures the proportion of water molecules within a voxel exhibiting isotropic diffusion. FW serves as an indicator of extracellular fluid dysregulation and stagnation, considered a biologically plausible mediator linking glymphatic dysfunction to cognitive decline in AD. Previous research identified an association of memory performance and hippocampal FW, alongside relationships involving hippocampal volume and hippocampal fractional anisotropy after FW correction. 11 Additionally, hippocampal FW distinguished cognitively normal, early, and late mild cognitive impairment (MCI), and AD. 12 FW represents a sensitive imaging marker of early neurodegenerative changes along the dementia continuum and may capture glymphatic-related pathological processes contributing to cognitive impairment.
Although accumulating evidence suggests a connection between glymphatic dysfunction and cognitive impairment, the mechanistic pathway linking glymphatic system activity, tissue water homeostasis, susceptibility to aging, cognitive reserve factors such as educational attainment, and cognitive performance across the dementia spectrum remains unresolved. We propose that glymphatic dysfunction exerts an indirect effect on cognition mediated by brain tissue water stagnation, as well as by factors associated with aging and cognitive reserve. This study investigated the roles of DTI-ALPS index and FW fraction in dementia continuum.
Methods
Participant enrollment
Participants were recruited from two sources to cover the dementia continuum: community-dwelling healthy older adults and cognitively impaired patients from the memory clinic. First, community residents aged between 60 and 80 years old were enrolled from the Northeastern Taiwan Community Medicine Research Cohort (NTCMRC; ClinicalTrials.gov identifier NCT04839796) in collaboration with the Community Medicine Research Center of the Keelung Chang Gung Memorial Hospital. The community-dwelling healthy participants were free from dementia, major organ failure, inherited or acquired brain disorders, cranial surgery, or active psychiatric disorders. Also, patients of the Department of Neurology at Keelung Chang Gung Memorial Hospital with a clinical diagnosis of MCI and dementia of varying severity were enrolled.
Brain MRI image processing
MRI scans were conducted using a Siemens 3 T Skyra MR scanner with a 20-channel head and neck coil at Chang Gung Memorial Hospital, located in Keelung, Taiwan. MRI scans and cognitive testing were performed during routine daytime clinical hours (9am to 4pm). All participants underwent the same pulse sequences. This included a high-resolution T1-weighted image obtained through a 3D Magnetization-Prepared Rapid Gradient Echo sequence (TR/TE = 2200/2.45 ms, TI = 900 ms, field-of-view (FOV) = 256 mm × 256 mm, flip angle = 8°, matrix size = 256 × 256, with 176 sagittal slices and a slice thickness of 1 mm, no gap). Diffusion-weighted images were also captured using single-shot spin-echo echo-planar imaging (TR/TE = 8500/99 ms, matrix size = 108 × 108, 50 contiguous slices, voxel size = 2.37 × 2.37 × 2.4 mm), including two b-values of 1500 s/mm2 (30 diffusion directions) and 3000 s/mm2 (64 diffusion directions), along with two b = 0 images in a posterior-to-anterior phase encoding direction. To address susceptibility distortions, an additional b = 0 image was acquired in an anterior-to-posterior phase encoding direction. After acquiring the diffusion-weighted and T1-weighted images, we utilize the iDIO pipeline for image preprocessing. 13 Next, the co-registration of T1-weighted and diffusion-weighted images utilized a boundary-based registration method.14,15 Diffusion-weighted images with b-values less than 1500 s/mm2 were utilized for diffusion tensor modeling. 16
The DTI-ALPS index quantitatively assessed glymphatic flow along the medullary veins adjacent to the left lateral ventricle. The calculation of the DTI-ALPS index utilized the ICBM-DTI-81 atlas to align each subject's fractional anisotropy data.17,18 Voxels with a fraction anisotropy greater than 0.2 were masked to avoid including space with cerebrospinal fluid. The projection fibers (superior and posterior corona radiata) and association fibers (superior longitudinal fasciculus) were identified on the atlas. The DTI-ALPS estimated diffusivity along the x-axis in the limited space between the y- and z-axis fibers by calculating the ratio of the mean x-axis diffusivity of projection fibers (Dxproj) to that of association fibers (Dxassoc), and subsequently dividing this value by the mean y-axis diffusivity of projection fibers (Dyproj) to that of the z-axis diffusivity of association fibers (Dzassoc). 7
Free-water mapping was performed to quantify interstitial fluid stagnation using a bi-tensor diffusion model, 19 implemented with the Diffusion Imaging in Python (DIPY) software package (https://dipy.org). 20 Following Pasternak's free-water elimination framework, diffusion tensors were expressed in the canonical 6-dimensional representation, and a Euclidean metric was applied to separate the isotropic free-water compartment. 21 A white matter mask was defined by thresholding fractional anisotropy (FA > 0.2). The whole-brain FW fraction was calculated as the mean FW value across all voxels within this mask. This procedure generated a voxel-wise FW fraction map (scalar range 0–1), as well as FW-corrected diffusion tensor metrics, including fractional anisotropy, mean diffusivity, axial diffusivity, and radial diffusivity. 20
Cognitive assessments
Cognitive performance has been objectively assessed using global cognitive tests and individual cognitive tasks to evaluate different domains. The Montreal Cognitive Assessment (MoCA), 22 the Mini-Mental State Examination (MMSE), 23 and the cognitive subscale of the Alzheimer's Disease Assessment Scale (ADAS-cog)24,25 are global assessments of cognition. The facial Memory Test (FMT), Digit Symbol Substitution Test (DSST), Digit Span Test forward (DST-f) and backward (DST-b), Letter Number Sequencing (LNS), 26 and Category Fluency (CF) 27 are individual tasks spanning diverse cognitive domains. Subjective cognitive complaints were evaluated by the AD8 and the twelve-item short form of the Everyday Cognition scales (ECog-12). 28 The AD8 scale used eight questions to assess subjective cognition with answers provided by family caregiver 29 or the participants. 30
Psychiatric assessments
Depression and anxiety tendencies were assessed by the Hospital Anxiety and Depression Scale (HADS); it was a 14-item self-report questionnaire to assess levels of anxiety and depression in both hospital and community settings, with separate subscales for each condition.31,32 In addition, the Geriatric Depression Scale (GDS) was a 15-item instrument specifically designed to assess depressive symptoms commonly observed in older adults. 33 Loneliness was assessed by the UCLA Loneliness Scale-8 (UCLA-LS), a brief, self-report instrument for efficiently assessing subjective feelings of loneliness; it consisted of 8 items rated on a 4-point Likert scale, with higher scores indicating greater perceived loneliness.34,35 The Apathy Evaluation Scale (AES) consists of 18 items that evaluate the behavioral, cognitive, and emotional aspects of apathy.36,37
Sleep, physical activity, and fatigue assessments
Assessment of sleep quality utilized the Pittsburgh Sleep Quality Index (PSQI). 38 Daytime sleepiness was evaluated by the Epworth Sleepiness Scale (ESS). 39 Physical activity profiling used the International Physical Activity Questionnaire-Short Form (IPAQ-SF), which calculates the equivalent quantity of energy consumption from daily physical activity in metabolic equivalent (MET in minutes per week) and ordinal grading (IPAQ-SF category) as low, moderate, and high physical activity. 40 The SARCF questionnaire was a five-component screening tool for sarcopenia, ranging from 0 to 10; a score of 4 or greater indicates a higher likelihood of sarcopenia. 41 The Pittsburgh Fatigability Scale (PFS) which was a 10-item, self-administered questionnaire designed to assess perceived physical and mental fatigability in older adults by querying fatigue levels to specific activities of fixed intensity and duration. It provided separate scores for physical and mental fatigue, each ranging from 0 to 50, with higher scores indicating greater fatigue.42,43
Statistical analysis
Variables were compared across the Clinical Dementia Rating (CDR) groups (0, 0.5, and ≥1) by one-way analysis of variance (ANOVA). Homogeneity of variances was assessed using Levene's test. If the assumption of equal variances was met, standard ANOVA was performed, followed by Tukey's Honestly Significant Difference (HSD) post hoc analysis. If Levene's test indicated heteroscedasticity, Welch's ANOVA with Games-Howell post hoc comparisons was used to ensure robust results. Categorical and ordinal variables were compared across groups using Pearson's chi-square test.
The primary analysis used PROCESS macro in SPSS (Model 4) to test mediation of independent variable (X), mediator (M), and dependent variable (Y), estimating the direct (X→Y), indirect (X→M→Y), and total effects. Indirect effects were evaluated using bootstrapped 5000 resamples to derive 95% confidence intervals, with and without adjusting for age, sex, and education.44,45 As a sensitivity analysis, moderation was tested by adding an interaction term (X*W) to assess whether the effect of the independent variable (X) on the dependent variable (Y) varied by the moderator (W) using PROCESS (Model 1).
A sensitivity analysis was conducted to account for potential confounding by sleep medication use. Sleep medication use was assessed based on the relevant item of the PSQI and coded as variables, utilizing responses to the question: “During the past month, how often have you taken medication to help you sleep, including prescribed or over-the-counter drugs?” Responses were scored using both a binary metric (0 versus >0) and an ordered scale (0 = not during the past month, 1 = less than once a week, 2 = once or twice a week, 3 = three or more times a week). These variables were incorporated as the moderator in moderation analyses (PROCESS Model 1).
Statistical significance was defined as p < 0.05, and all estimates were reported with 95% confidence intervals. The statistical analysis was conducted using SPSS version 23 from IBM Corporation, USA.
Results
Participants
The study enrolled 127 participants (female-to-male ratio 1.19, age 68.60 ± 6.52 years old, education 9.36 ± 4.45 years), including 97 healthy elderly from the communities and 30 cognitively impaired patients from the memory clinic of Keelung Chang Gung Memorial Hospital (Figure 1). Using CDR for laddered grading, the participants were classified into normal (CDR = 0; N = 78), MCI (CDR = 0.5; N = 43), and dementia (CDR 1–3; N = 6).
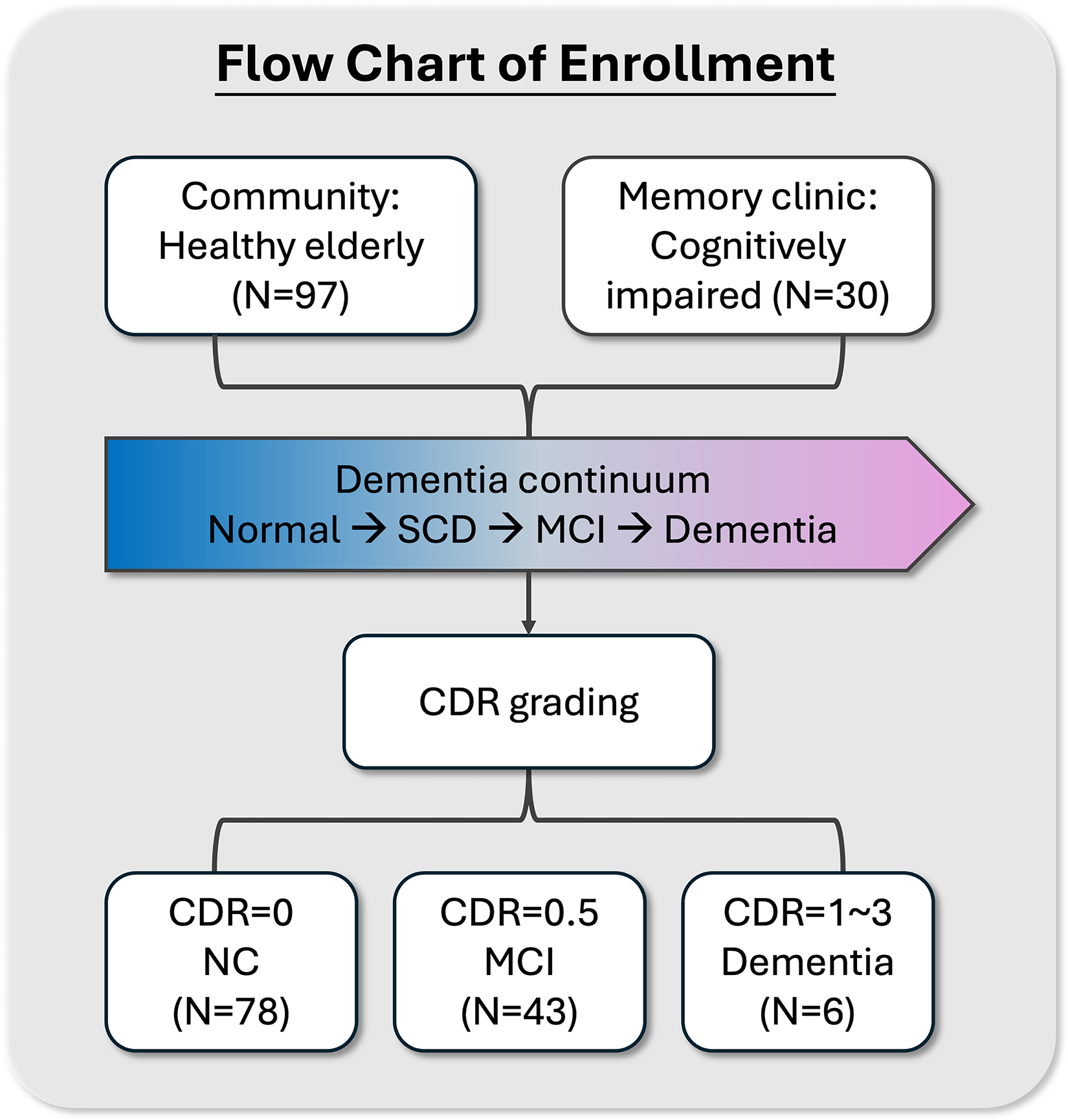
Participant enrollment. Participants were enrolled from community and memory clinic and covered the dementia continuum from normal subjects, SCD, MCI to dementia. They were grouped according to CDR ladders for further analysis. CDR: Clinical Dementia Rating; SCD: subjective cognitive decline; MCI: mild cognitive impairment; NC: normal control.
Neuropsychiatric and image features of CDR ladders
Figure 2 showed the multidomain assessments in CDR ladders. Age increased while education levels decreased with dementia severity. Sex did not differ (female ratio in CDR 0, 0.5, and 1–3 were 53.8%, 51.2%, and 83.3%; p = 0.330; not in the Table) between groups. Additionally, the cognitively impaired participants (N = 30) underwent APOE genotype examination [APOE4 non-carrier (N = 18), heterozygous (N = 9), and homozygous (N = 3)], which revealed a significantly higher rate of dementia associated with the APOE4 allele in CDR 0.5: 66.7%, 29.2%, 4.2% and CDR 1–3: 33.3%, 33.3%, 33.3% (p = 0.045).

Neuropsychiatric and image features of the CDR ladders. The sex (female) ratio of CDR = 0, 0.5, 1-3 were 53.8, 51.2, and 83.3%, respectively (p = 0.330). The DTI indices was based on FW-corrected DTI analysis. DTI-ALPS: Diffusion Tensor Image Analysis Along the Perivascular Space; FW: free water; DTI: diffusion tensor imaging; FA: fraction anisotropy; MD: mean diffusivity; RD: radial diffusivity; AD: axial diffusivity; Ecog-12: twelve-item short form of the Everyday Cognition scales; MoCA: Montreal Cognitive Assessment; MMSE: Mini-Mental State Examination; ADAS-cog: cognitive subscale of the Alzheimer's Disease Assessment Scale; HADS-A: anxiety subscale of the Hospital Anxiety and Depression Scale; HADS-D: depression subscale of the Hospital Anxiety and Depression Scale; GDS: Geriatric Depression Scale; UCLA-LS: UCLA Loneliness Scale-8; AES: Apathy Evaluation Scale; PSQI: Pittsburgh Sleep Quality Index; ESS: Epworth Sleepiness Scale; PFS: Pittsburgh Fatigability Scale; IPAQSF-MET: International Physical Activity Questionnaire Short Form—metabolic equivalent.
The glymphatic imaging markers, DTI-ALPS and FW fraction, showed significant differences among the three groups (p < 0.001 and p < 0.001 in ANOVA with Tukey HSD). However, the FW-corrected DTI metrics were not different between the groups. Subjective cognitive complaints, reflected by the AD8 score, increased with CDR levels (p < 0.001 in ANOVA with Tukey HSD); conversely, objective cognitive performance, demonstrated by MoCA, MMSE, and ADAS-cog scores, declined (p < 0.001, < 0.001, and < 0.001 in Welch's ANOVA with Games-Howell).
In multidomain assessments, loneliness (UCLA-LS score) was lower with CDR progression (p < 0.001); the apathy score (AES) was higher in CDR 0.5 but not in the other groups (p < 0.001). These results may reflect modern social isolation rather than neuropsychiatric symptoms from dementia progression. Additionally, physical inactivity (IPAQSF-MET, p < 0.001) and increased sarcopenia risk (SARCF, p = 0.006) were observed with higher CDR levels. GDS showed higher depressive tendency in MCI than NC (p = 0.003). Otherwise, the self-reported anxiety and depression in HADS, physical and mental fatigue, and sleep quality showed no differences among the groups.
Distributions of the glymphatic image markers
The distribution patterns of the DTI-ALPS index and FW fraction across CDR stages indicated a decline in DTI-ALPS values and an elevation in FW fraction as dementia severity increased. Among cognitively impaired participants who underwent APOE genotyping, neither the DTI-ALPS index (1.123, 1.126, 1.037; p = 0.232) nor the FW fraction (0.568, 0.576, 0.597; p = 0.455 by one-way ANOVA) differed significantly among APOE4 non-carriers (N = 18), heterozygotes (N = 9), and homozygotes (N = 3). However, statistical power may have been limited due to small sample sizes, as shown in Figure 3.
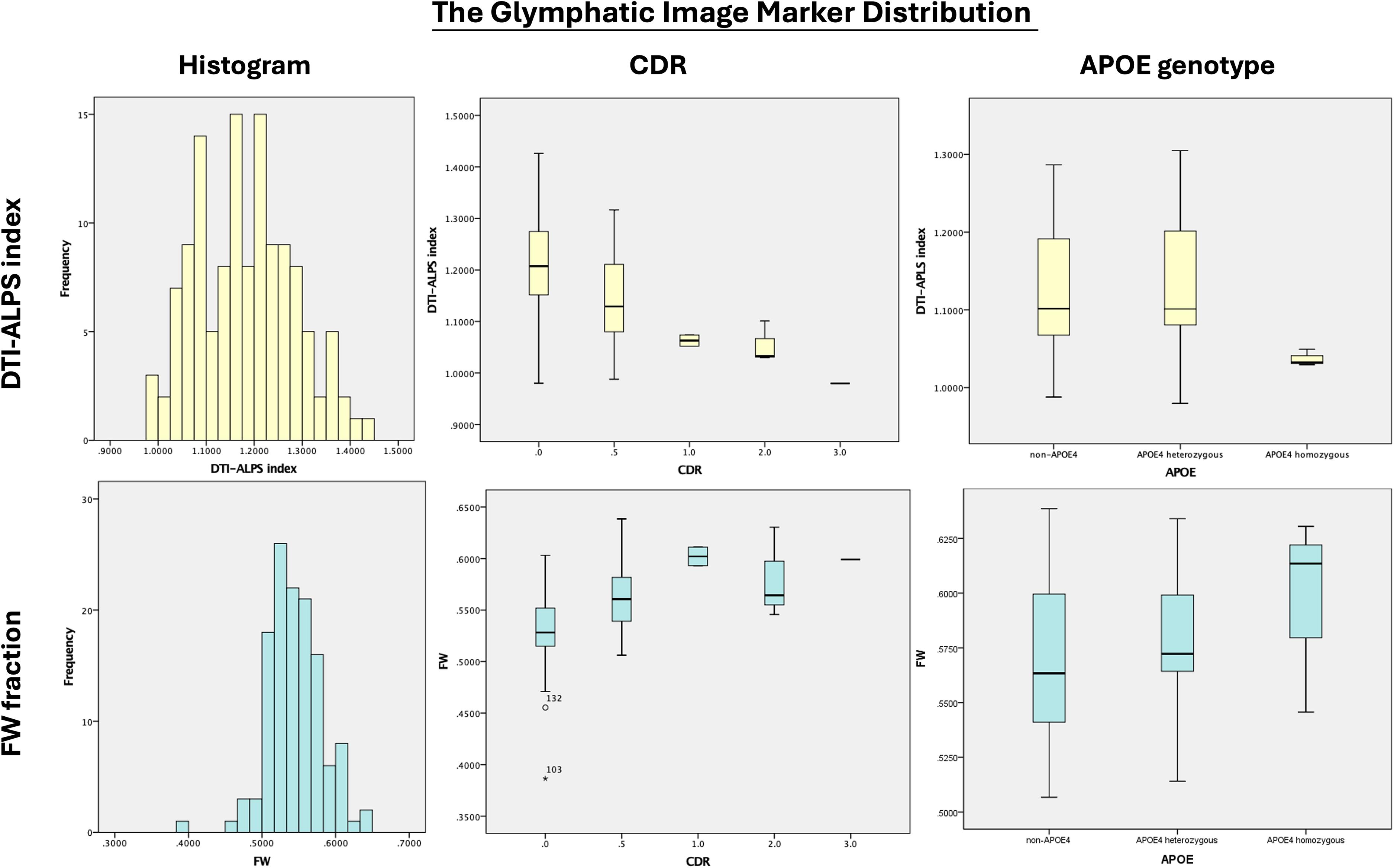
Distribution of DTI-ALPS index and FW fraction. The distribution of the DTI-ALPS index and whole-brain FW fraction was estimated to follow a normal distribution. Variations across different CDR stages demonstrated a progressive change: as glymphatic activity declined, there was increased interstitial fluid stasis, with decreasing DTI-ALPS and rising FW fraction corresponding to greater CDR severity. Among 30 cognitively impaired patients who underwent APOE genotyping, homozygotes (N = 3) exhibited a trend toward lower DTI-ALPS values and higher FW fraction compared to others; however, statistical power was limited due to the small sample size.
Associations between the glymphatic image markers and multidomain indices
The DTI-ALPS index and FW fraction correlated significantly in linear regression (standardized coefficient β = −0.51, p < 0.001). Additionally, DTI-ALPS index (β = 0.35, p < 0.001) and FW fraction (β = −0.50, p < 0.001) were significantly associated with cognitive performance as measured by the MoCA. In Figure 4, scatter plots with lines of linear regression showed the glymphatic image marker distribution associated with age, cognition (MoCA, MMSE, ADAS-cog, and the individual cognitive tests), anxiety (HADS-A), loneliness (UCLA-LS), apathy (AES), physical activity (IPAQSF-MET), and risk of sarcopenia (SARCF), which suggested glymphatic dysfunction might be a factor of multiple presentations in the dementia continuum.
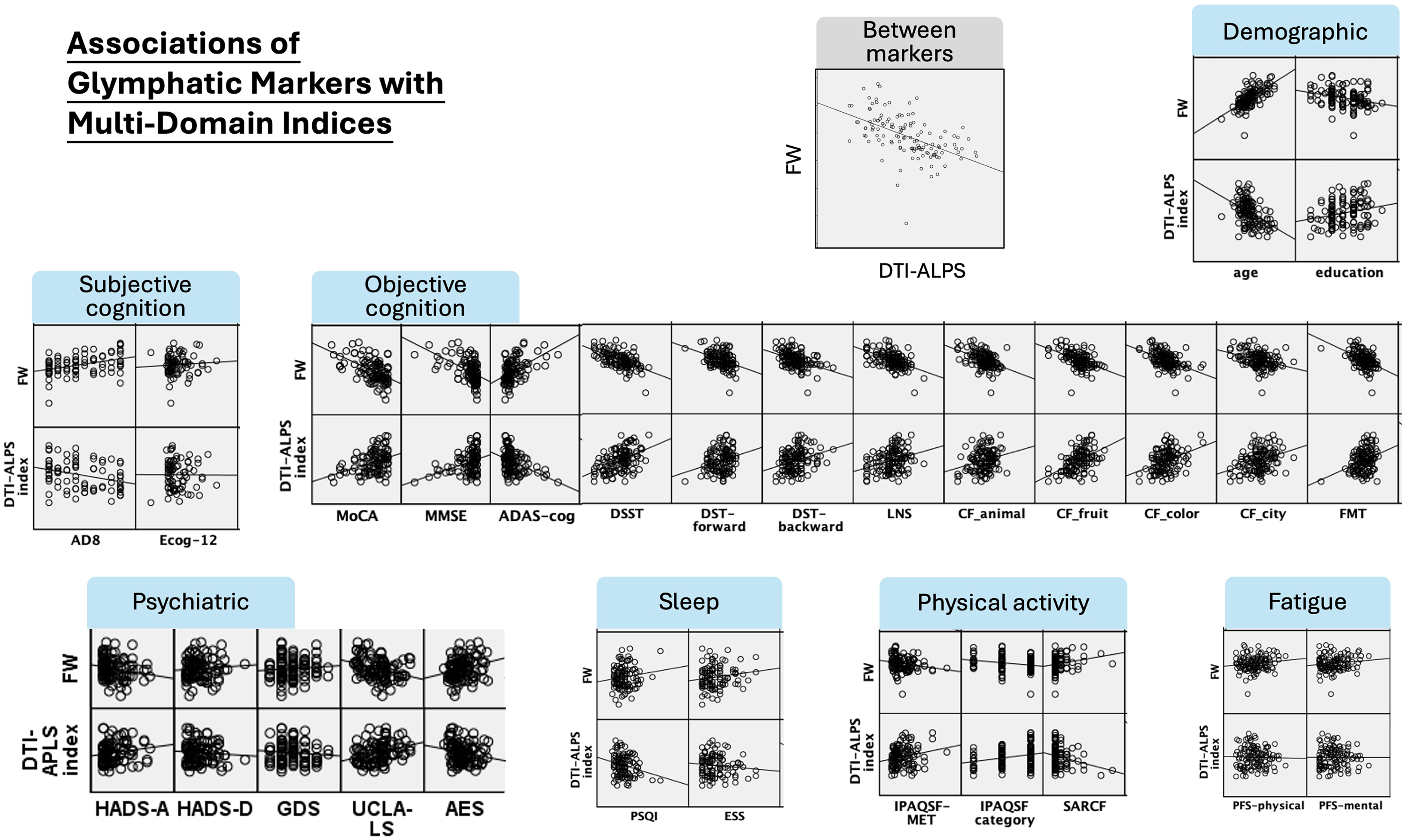
Association of DTI-ALPS index and FW fraction with clinical indices. The scatter plots of DTI-ALPS index and FW fraction with multiple clinical indices. The lines in the plot indicated linear regression lines. Ecog-12: twelve-item short form of the Everyday Cognition scales; MoCA: Montreal Cognitive Assessment; MMSE: Mini-Mental State Examination; ADAS-cog: cognitive subscale of the Alzheimer's Disease Assessment Scale; DSST: digit symbol substitution test; DST: digit span test; LNS: letter number sequence; CF: category fluency; FMT: facial memory test; HADS-A: anxiety subscale of the Hospital Anxiety and Depression Scale; HADS-D: depression subscale of the Hospital Anxiety and Depression Scale; GDS: geriatric depression scale; UCLA-LS: UCLA Loneliness Scale-8; AES, the Apathy Evaluation Scale; PSQI: Pittsburgh Sleep Quality Index; ESS: Epworth Sleepiness Scale; IPAQSF: International Physical Activity Questionnaire Short Form; MET: metabolic equivalent; PFS: Pittsburgh Fatigability Scale.
Glymphatic dysfunction as a mediator in cognitive decline
The study hypothesized that glymphatic activity influences interstitial water retention within the brain, in which the water stagnation in the brain as the whole brain FW fraction (M) mediated between the glymphatic clearance DTI-ALPS index (X) and cognitive MoCA score (Y). In mediation analysis (PROCESS Model 4), DTI-ALPS index showed a significant total positive association with MoCA (b = 21.94, SE = 4.88, t = 4.50, p < 0.001, 95% CI [12.28, 31.59]). DTI-ALPS index was significantly associated with FW fraction (b = −0.20, SE = 0.03, t = −6.97, p < 0.001, R2 = 0.28), and higher FW was strongly associated with lower MoCA scores when adjusting for DTI-ALPS (b = −67.37, SE = 14.41, t = −4.67, p < 0.001), whereas the direct effect of DTI-ALPS on MoCA controlling for FW fraction was attenuated and not statistically significant (b = 8.76, SE = 5.32, t = 1.65, p = 0.10). The indirect effect of DTI-ALPS on MoCA via FW fraction was significant (b = 13.17, bootstrap SE = 3.41, bootstrap 95% CI [7.45, 20.66]), with a significant completely standardized indirect effect (β

Mediation analysis of DTI-ALPS index, FW fraction, and cognition. (A) Mediation analysis revealed that the total effect of DTI-ALPS index on MoCA was significant, while the direct effect was not after accounting for the mediator (FW fraction). (B) The significant indirect effect and non-significant direct effect indicated that FW fraction fully mediated the association between DTI-ALPS and cognitive performance after adjusting for age, sex, and education.
Demographics were associated with the glymphatic markers and cognition. Age significantly correlated with DTI-ALPS (Pearson's correlation coefficient r = −0.447, p < 0.001), FW fraction (r = 0.655, p < 0.001), and MoCA score (r = −0.635, p < 0.001). Education (years of school attainment) was also associated with the DTI-ALPS (r = 0.237, p = 0.007), FW fraction (r = −0.281, p = 0.001), and MoCA score (r = 0.545, p < 0.001). Additionally, males and females differed significantly in the DTI-ALPS index (1.142 ± 0.090 versus 1.213 ± 0.101, p < 0.001) and FW fraction (0.555 ± 0.039 versus 0.535 ± 0.034, p = 0.002) but did not differ in MoCA scores (p > 0.05). Because of the potential influence of demographics on the glymphatic system and cognition, the mediation analysis was adjusted for age, sex, and education. The DTI-ALPS remained significantly associated with MoCA at the total-effect level (b = 10.93, SE = 4.55, t = 2.40, p = 0.018, 95% CI [1.93, 19.92], completely standardized coefficient β = 0.19). When FW was included as a mediator in the model, the direct effect of DTI-ALPS on MoCA was attenuated and was no longer statistically significant (b = 8.15, SE = 4.62, t = 1.77, p = 0.080, 95% CI [−0.99, 17.30], completely standardized coefficient β = 0.14). The indirect effect of DTI-ALPS on MoCA via FW remained statistically significant (b = 2.77, bootstrap SE = 1.85, 95% bootstrap CI [0.38, 7.44]), with a significant completely standardized indirect effect (β = 0.05, bootstrap SE = 0.03, 95% bootstrap CI [0.01, 0.13]), indicating that FW continued to mediate a modest but significant proportion of the association between DTI-ALPS and cognition even after controlling for age, sex, and education (Figure 5B).
The secondary analysis considered education level as a moderator between glymphatic dysfunction and cognition. In a secondary analysis using PROCESS Model 1, education significantly moderated the associations of both DTI-ALPS and FW fraction with cognition. In the model including DTI-ALPS and years of education, the overall regression was significant (R2 = 0.38, F = 25.50, p < 0.001). The DTI-ALPS x education interaction was significant (b = −2.07, SE = 0.96, t = −2.16, ΔR2 = 0.02, F = 4.65, p = 0.033), indicating that the positive association between DTI-ALPS and MoCA was weaker at higher education levels and stronger at lower education levels (Figure 6A). In the model including FW and education, the overall regression was also significant (R2 = 0.45, F = 33.55, p < 0.001). The FW × education interaction was significant (b = 5.59, SE = 2.60, t = 2.15, ΔR2 = 0.02, F = 4.62, p = 0.034), suggesting that the adverse association between higher FW fraction in white matter and cognitive performance was more pronounced among individuals with lower education and attenuated among those with higher educational attainment (Figure 6B).
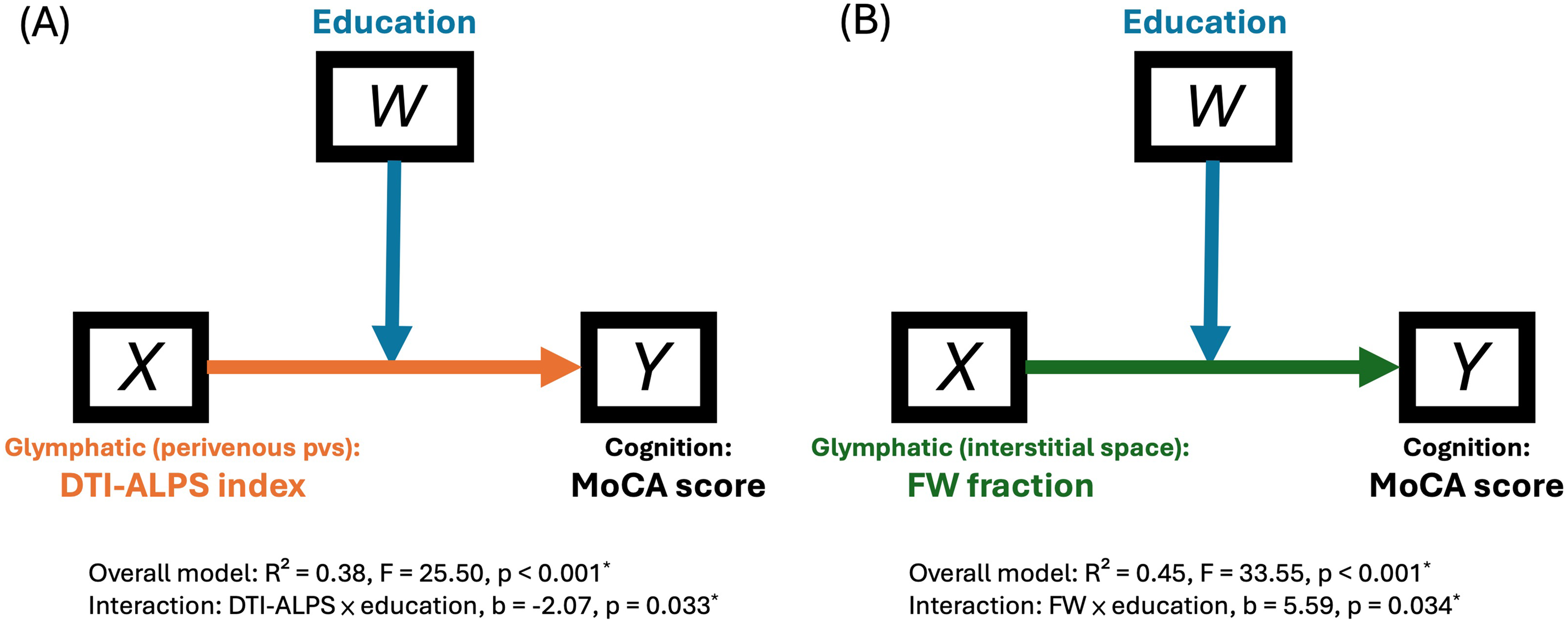
Interaction of education on the associations between glymphatic imaging markers and cognitive performance. Education years correlated with DTI-ALPS (r = 0.237, p = 0.007), FW fraction (r = −0.281, p = 0.001), and MoCA (r = 0.545, p < 0.001). Furthermore, moderating effects of education on associations between the glymphatic image markers and cognition were found. (A) The positive association between DTI-ALPS index and MoCA score was weaker at higher education levels and stronger at lower education levels (DTI-ALPS × education interaction: b = –2.07, SE = 0.96, t = –2.16, ΔR2 = 0.02, F = 4.65, p = 0.033; overall model: R2 = 0.38, F = 25.50, p < 0.001). (B) The adverse association between FW fraction and MoCA was more pronounced in individuals with lower education and attenuated in those with higher education (FW × education interaction: b = 5.59, SE = 2.60, t = 2.15, ΔR2 = 0.02, F = 4.62, p = 0.034; overall model: R2 = 0.45, F = 33.55, p < 0.001).
In sensitivity analyses, we tested whether sleep-medication use moderated the associations between glymphatic markers and cognitive performance. Both the binary indicator of sleep-medication use (Figure 7A) and the ordinal measure of sleep-medication dependence (Figure 7B) significantly moderated the relationship between FW fraction and MoCA score (p = 0.044 and p = 0.034, respectively). In contrast, there was no significant interaction between sleep-medication use and the DTI-ALPS index in relation to MoCA performance (p > 0.05).
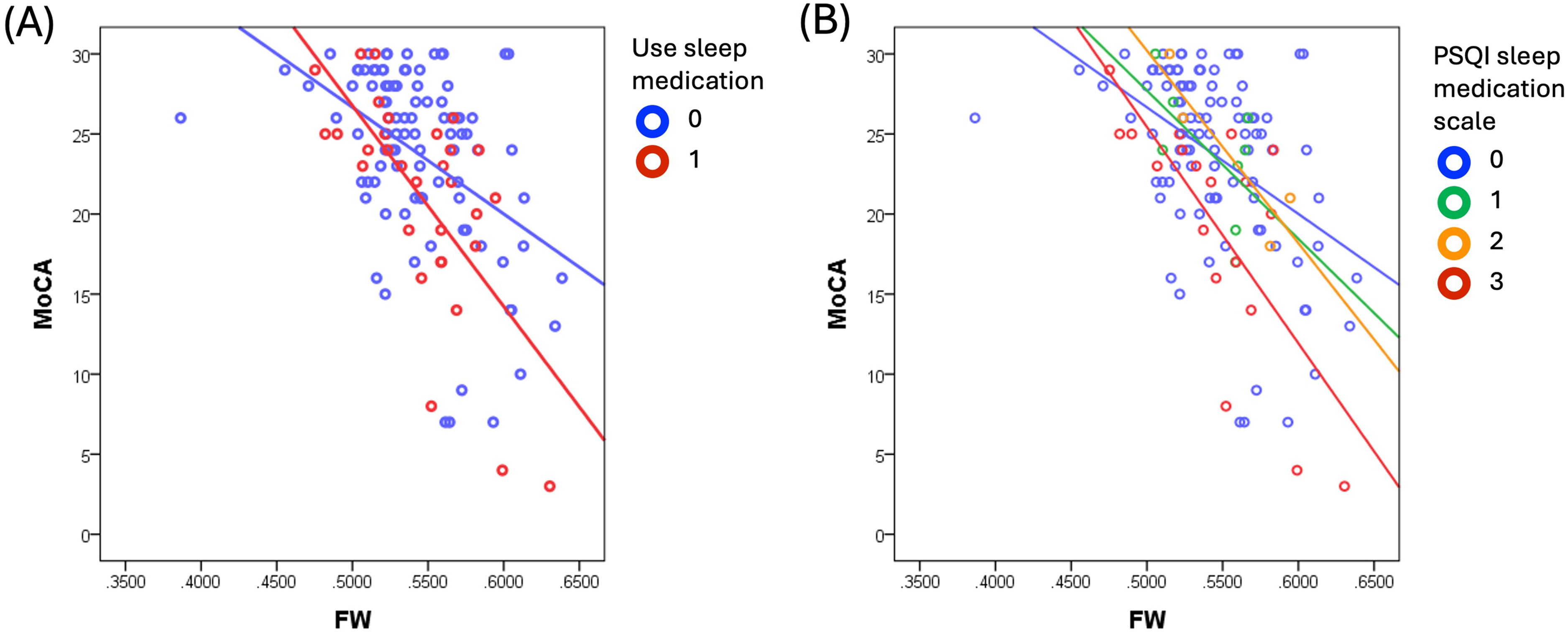
Interaction between FW fraction and sleep medicine use in predicting MoCA. (A) Predicted MoCA scores (y-axis) were plotted as a function of FW (x-axis) separately for using/not using sleep medication, with a steeper negative FW-MoCA slope when the participants were sleep medicine users, indicating that the cognitive impairment associated with the increase of FW fraction was worsen when medication to help sleeping was needed (binary variable, interaction of FW x sleep medication was significant (b = −58.87, SE = 28.94, t = −2.03, p = 0.044, 95% CI [−116.16, −1.59]). (B) The FW-cognition interaction moderated by sleep-medication dependence persisted when analyzing the full scale of sleep-medication use (b = −22.39, SE = 10.42, t = −2.15, p = 0.034, 95% CI [−43.02, −1.76]).
Discussion
Glymphatic dysfunction and image markers for dementia continuum
The DTI-ALPS index and FW fraction are promising non-invasive biomarkers for early dementia detection and monitoring, providing complementary perspectives for characterizing the glymphatic system through distinct measurement mechanisms. However, more comprehensive consideration with decreased glymphatic activity and interstitial fluid stasis, as well as effects of aging and role of education in maintaining cognitive reserve is necessary for understanding cognitive decline in the development of dementia. 46 This study, examining 127 participants across the dementia continuum, provides evidence that glymphatic system alterations, as indexed by the DTI-ALPS and FW fraction, are associated with cognitive decline and may represent a potential pathway of interest. These two glymphatic markers are associated with demographic, cognitive, psychiatric, sleep quality, and physical decline.
While the DTI-ALPS index and FW fraction show considerable promise as non-invasive biomarkers, their widespread clinical adoption requires harmonization of imaging protocols and robust longitudinal validation. 47 Current evidence indicates that monitoring preclinical changes in DTI-ALPS index can predict the conversion from MCI to dementia, 48 as well as long-term cognitive decline in small vessel disease. 49 Additionally, integrating these glymphatic imaging markers with other neuroimaging 10 and biochemical indicators 9 offers a promising strategy to evaluate whether DTI-ALPS and FW fraction can serve as universal biomarkers for glymphatic system efficiency.50,51
Insights of glymphatic-related cognitive impairment
The main findings of mediation analysis highlight the critical role of extracellular water homeostasis as a biological bridge between glymphatic dysfunction and cognitive decline. The mediation effects of the whole-brain FW fraction are significant between the DTI-ALPS index and the MoCA score, even after adjusting for age, sex, and education. Increased FW fraction is thought to reflect extracellular fluid accumulation related to microstructural degeneration, neuroinflammation, or vascular leakage.21,52 Prior work has shown that reduced glymphatic clearance efficiency leads to the accumulation of neurotoxic metabolites, impaired waste removal, and altered interstitial fluid dynamics.4,53 Our findings suggest that such glymphatic inefficiency may manifest in microstructural indices captured by FW, thereby linking glymphatic system disruptions to cognitive outcomes through tissue-level changes rather than direct functional impairment in the continuum of normal aging to dementia. This finding is compatible with the recent study of the middle to aged cohort at risk of cerebral small vessel disease, showing the mediation role of FW fraction on the relationship between DTI-ALPS index and executive function. 54
Besides, demographics are glymphatic influencers. Aging is a well-established determinant of glymphatic decline, driven in part by astrocytic AQP4 depolarization and vascular plasticity changes. 55 Female-male difference of the glymphatic activity has been documented.9,56 Additionally, educational attainment, indexed as a proxy for cognitive reserve, 46 further modulates the relationship between biological changes and cognitive performance. Both early 57 and late life 58 education level determines the lifelong cognitive trajectories. In this study, DTI-ALPS positively and FW fraction negatively correlated with education level.Furthermore, the interactions of education and these two glymphatic imaging markers modulate the glymphatic-cognitive relationship (Figure 6). The findings are compatible with the cognitive reserve hypothesis that individuals with higher educational backgrounds may better compensate for glymphatic dysfunction-associated neural inefficiencies through alternative cognitive strategies or neural network reorganization. 59 Building on accumulating evidence that astrocytes play key roles in memory and learning60–62 and are essential for maintaining glymphatic function, 63 these findings collectively support the hypothesis that educational attainment constitutes a modifiable background factor and a compensatory mechanism that may mitigate glymphatic dysfunction-related cognitive decline in dementia. 64 Overall, our findings provide mechanistic insight into how glymphatic dysfunction contributes to cognitive impairment and highlight the needs of considering both biological and socio-cognitive determinants when evaluating dementia risk and designing preventive strategies.
Limitations, methodological considerations, and future directions
The challenges in recruiting participants with advanced dementia, reflected in the uneven CDR stage distribution (78 normal, 43 MCI, 6 dementia), underscore practical limitations in this research. Recruiting individuals with advanced dementia presents practical difficulties when conducting dementia studies. This recruitment bias toward earlier disease stages may limit the generalizability of findings to more advanced dementia populations. Future studies should employ strategies to enhance participation recruitment and consider longitudinal follow-up to observe the transition from MCI to dementia and track dementia progression.
The use of DTI-ALPS as an indirect measure of glymphatic function represents both a strength and a limitation of the current approach. While DTI-ALPS provides a non-invasive assessment method suitable for clinical populations, it measures water diffusion along perivascular spaces rather than direct glymphatic flow. 51 Recent methodological discussions have emphasized that the DTI-ALPS index should be interpreted as a surrogate marker that measures diffusion characteristics rather than definitively representing glymphatic function. Strategies of incorporating multiple assessment methods, including dynamic contrast-enhanced imaging65,66 and other non-contrast imaging techniques 47 such as perivascular space, 67 arterial spin labeling, 68 and intravoxel incoherent motion,69,70 to provide more comprehensive glymphatic evaluation.
In addition, the precise timing of MRI scans was not systematically documented, and potential circadian influences on glymphatic activity might represent a confounding factor. Nevertheless, all scans were performed during standardized daytime clinical hours (9 am–3 pm), which may have introduced minor variability related to circadian-dependent glymphatic activity.
The mediation analysis framework employed in this study provides a valuable approach for understanding complex biological relationships. However, the cross-sectional design limits conclusions about whether glymphatic dysfunction precedes cognitive decline or represents a consequence of neurodegeneration. Longitudinal studies tracking glymphatic markers and cognitive function over time will provide stronger evidence of temporal sequence and causal relationships and enhance the predictive utility of these biomarkers.
Conclusion
The results of this study suggest that glymphatic system alterations, as indexed by the DTI-ALPS measure and FW fraction, may be involved in cognitive decline across dementia stages, particularly from normal cognition to MCI, which should be examined in future longitudinal and mechanistic work. The progressive impairment of glymphatic markers with increasing CDR severity, combined with their strong associations with cognitive performance, supports the clinical utility of DTI-ALPS as a biomarker for dementia progression. The mediation pathways involving glymphatic activity (DTI-ALPS) and brain tissue water content (FW fraction) underscore the importance of jointly considering these complementary imaging markers to better understand glymphatic dysfunction in cognitive decline. Furthermore, the observed interactions between education and glymphatic markers highlight the modulatory role of education in shaping the relationship between glymphatic function and cognition. These findings suggest that diffusion-based glymphatic markers are associated with cognitive performance and may serve as promising candidates for further longitudinal and mechanistic investigation.
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
The study protocol followed the Helsinki Declaration and received approval from the Institute Board Review Committee of Chang Gung Memorial Hospital (Approval numbers 202301485B0, 202201884A3, 201600580B0, 201901352B0C602, 202201527B0).
Consent to participate
Every participant comprehended the objectives of the research project and the process of participation. Written informed consent was secured from the participants or from their designated representatives when the participants had dementia and were unable to provide consent.
Consent for publication
Not applicable
Author contribution(s)
Funding
This study was financially supported by grants from the National Science and Technology Council (grant number NSTC 112-2628-B-182-007-MY3 and NSTC 112-2628-B-182A-009-MY3) and the Chang Gung Memorial Hospital Research Fund (grant numbers CRRPG2K0031, CORPG2P0091, CMRPG2N0212).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.