
Abstract
Background
In clinical settings, the head turning sign (HTS) occurs when patients with cognitive complaints turn their head toward the accompanying person seeking assistance. Due to its nature, and unlike other non-canonical neurological signs of cognitive impairment, the HTS is likely to occur in ecological, daily-life scenarios too. However, this hypothesis has not been tested yet.
Objective
To assess the prevalence and clinical correlates of the “ecological HTS” (eHTS) in MCI and dementia due to chronic-degenerative etiologies.
Methods
This retrospective cohort included 112 patients with MCI/dementia due to Alzheimer's disease (AD; N = 71), frontotemporal lobar degeneration (N = 6), Lewy body disease (N = 6), chronic cerebrovascular diseases (CVD; N = 11), mixed (i.e., AD + CVD; N = 15) unspecified non-AD neurodegenerative etiologies (N = 3). We recorded the number of HTSs displayed by patients during the MMSE and inquired accompanying persons whether the HTS occurred in daily life too.
Results
The overall prevalence of the eHTS in the cohort was 50%; its distribution was independent of demographics, disease severity (i.e., MCI versus dementia), and etiology. Within multiple logistic models, the presence of the eHTS + proved to be predicted both by lower scores on the Spatial Orientation subtest of the MMSE and by a higher number of HTSs during the execution of the MMSE. Moreover, a trend towards longer disease duration and the occurrence of the eHTS was found.
Conclusions
In MCI and dementia, the HTS is an ecologically valid non-canonical sign, frequently occurs in daily life too, associated with longer disease duration and spatial disorientation.
Keywords
Introduction
Several non-canonical neurological signs suggestive of cognitive impairment have been described, such as the “attended with” sign (AWS; i.e., a patient coming along with an accompanying person when seeking neurological consultation), the applause sign (AS; i.e., a patient clapping his/her hands more times than those that the examiner instructed him/her to due to inhibition deficits) and the head turning sign (HTS; i.e., a patient, when asked to provide answers or to perform cognitive tasks that exceed their capacity, turning his/her head towards the accompanying person seeking assistance or confirmation).1–3
Among them, the HTS is arguably one of the most extensively investigated, showing promising features as a marker of cognitive dysfunction in patients with brain disorders.2,4–10 In fact, previous studies have consistently associated the HTS with poorer cognitive performances.3–10 Moreover, whilst some reports linked the HTS to Alzheimer's disease (AD),6,8,9 including evidence from cerebrospinal fluid biomarkers,8,9 evidence also suggests that this sign may operate as a robust marker of cognitive impairment across different etiologies. 10
Interestingly, and unlike other non-canonical signs that can only be elicited and thus recorded within clinical settings (such as the AWS and the AS), it is reasonable to hypothesize that, due to its being a “help-seeking behavior”, 10 the HTS also occurs in ecological, everyday-life scenarios. In fact, in clinical settings, patients have been reported to display the HTS when they feel challenged by either an inquiry that they find it difficult to reply to (e.g., the reasons why they are seeking neurological consultation) or by a cognitive task exceeding their level of ability.2,4–10 It thus follows that such a sign is likely to be detected in ecological settings too, when patients with cognitive disorders might seek help from their caregivers when facing challenges elicited by demanding situations.
With that being said, no study to date has focused on determining whether the HTS manifests in daily life. Such an investigation would nevertheless be of clinical relevance, as possibly supporting the ecological validity of a sign whose value has not been explored “beyond the clinic walls”.
Given the above premises, the aim of the present study was to examine whether, in patients with mild cognitive impairment (MCI) and dementia due to neurodegenerative, chronic cerebrovascular or mixed etiologies, the HTS occurs in daily life as well. Specifically, we aimed to 1) assess the prevalence of the “ecological HTS” (eHTS), 2) investigate its clinical, demographic, and cognitive correlates and 3) determine whether the occurrence of the sign in a clinical setting predicted its manifestations in daily life.
Methods
Participants
We retrospectively retrieved data on N = 112 patients attending the Center for Cognitive Disorders and Dementias (CDCD) of IRCCS Istituto Auxologico Italiano (Milan, Italy) between June 2024 and June 2025. Patients were excluded if: 1) attending without an accompanying person; 2) did not present with a diagnosis of interest (i.e., MCI/dementia due to neurodegenerative, chronic cerebrovascular, or mixed etiology) and/or had a positive history of further, potentially confounding brain disorders (e.g., acute stroke/major focal lesions; brain neoplasms; epilepsy); 3) were diagnosed with MCI/dementia of undefined etiologies (due to unavailable/inconclusive instrumental or biomarker findings); 4) were unable to complete the Mini-Mental State Examination (MMSE), as HTS occurrences were recorded during its administration and incomplete testing would have provided fewer opportunities to observe the sign.
The cohort included patients with MCI or dementia due to possible/probable 1) Alzheimer's disease (AD; MCI: N = 19; dementia: N = 52), 2) frontotemporal lobar degeneration (FTLD; MCI: N = 1; dementia: N = 5), 3) Lewy body disease (LBD; dementia: N = 6), 4) chronic cerebrovascular disease (MCI: N = 8; dementia: N = 3), 5) mixed etiologies (AD and chronic cerebrovascular disease; MCI: N = 3; dementia: N = 12). A further group was that of Aβ-negative patients with CT- and/or MRI-detected atrophy that could not be otherwise classified under any of the abovementioned AD-unrelated category (non-AD degenerative, NADD; MCI: N = 2; dementia: N = 1).
Diagnoses were pursuant to current nosographic systems and supported at neurological, neuropsychological and neuroradiological (i.e., MRI/CT and, occasionally, 18FFDG-PET) levels, being at times also availed by CSF A/T/N biomarkers/amyloid-PET and genetic testing. The distinction between MCI and dementia relied on proxy-reported information on functional independence. Detailed information on the diagnostic work-up has been described elsewhere. 3 Supplemental Table 1 shows in-depth information on patients’ phenotypes across etiologies and MCI/dementia status.
Patients provided informed consent and the study was approved by the local Ethics Committee.
Materials
The HTS was recorded by a single neurologist with expertise in dementing conditions (F.V.) during the administration of the MMSE. 11 In accordance with Aiello et al., 10 for an HTS to be scored as positive, the patient had to turn his/her head to an angle of at least 45° towards the accompanying person(s) in search of assistance when instructed to perform a given task. The number of HTSs displayed across the entire administration of the MMSE was recorded. If at least one HTS occurred during the screening session, the neurologist asked the accompanying person(s) if he/she/they have ever witnessed the patient displaying this behavior in daily life, especially during challenging situations. Conversely, if the patient did not show the HTS during the administration of the MMSE, the physician asked the accompanying person(s) whether the patient, in daily situations, would turn his/her head toward a reference person in search for help when facing challenging circumstances (eHTS). The eHTS was ultimately classified as positive (eHTS+) or negative (eHTS-) if the accompanying persons confirmed or not its occurrence in patients’ daily life, respectively.
Demographic (sex, age and education in years), clinical (disease duration in months, disease severity, i.e., MCI versus dementia, and etiology, i.e., AD versus FTLD versus LBD versus vascular versus mixed versus NADD) and MMSE measures were also retrieved. MMSE items were grouped as previously described: Temporal Orientation (range=0–5); Spatial Orientation (range=0–5); Short-Term Memory (i.e., Immediate Recall items; range=0–3); Long-Term Memory (i.e., Delayed Recall items; range=0–3); Attention (range=0–5); Language (i.e., Naming, Repetition, Comprehension, Reading and Writing tasks; range=0–8); Constructional Praxis (range=0–1).3,10 MMSE total scores were classified as impaired versus unimpaired based on current Italian norms. 11
Statistics
We first computed the frequency of eHTS + and eHTS- patients. Then, eHTS + and eHTS- patients were compared on demographics (i.e., age, sex, and education), disease duration (in months), severity, and etiology, as well as total and subscale-/item-level MMSE scores via appropriate univariable analyses, i.e., χ2-tests for categorical outcomes and independent-sample t-tests or Mann-Whitney's U-tests for Normally distributed and non-Normally distributed continuous outcomes. To check for the assumption of Normality, we descriptively assessed skewness values (i.e., judged as abnormal if >|1|) and visually inspected histograms and Q-Q plots.
Subsequently, those variables that significantly differed between the two groups were entered as predictors into a multivariable logistic model (Model 1) addressing, as the outcome, the presence versus absence of the eHTS. With specific regard to MMSE measures, in order not to incur in an inflation of type-I error rates, the selection of those to be entered within the logistic model relied on Bonferroni's correction (i.e., α=0.05/k, with k = 7, corresponding to the MMSE grouping categories described above).
Moreover, in order to verify whether the number of HTSs exhibited during the MMSE was predictive of the presence of the eHTS, another logistic model (Model 2) was run with the number of HTSs as the predictor and, as the outcome, the presence versus absence of the eHTS. In this last model, those demographic and clinical variables entered into Model 1 were likewise accounted for as covariates. The same logistic model (Model 3) was also run by nevertheless addressing, as the predictor, the presence of at least one HTS during the MMSE instead of the number of HTSs displayed during its administration.
Analyses were run via jamovi 2.3 (the jamovi project, 2022). Missing data were excluded pairwise.
Results
Table 1 shows eHTS + and eHTS- patients’ demographic and clinical features. According to caregiver reports, the eHTS was exhibited in daily life by 56 patients out of the whole cohort (50%). During the administration of the MMSE, 67.86% of patients (i.e., 72 out of 112) displayed at least one HTS. Consistently, eHTS + patients were by far more represented among those displaying at least one HTS during the MMSE when compared to those who did not display it within the cognitive screening session (χ2 (1) = 13.26; p < 0.001) (Figure 1).
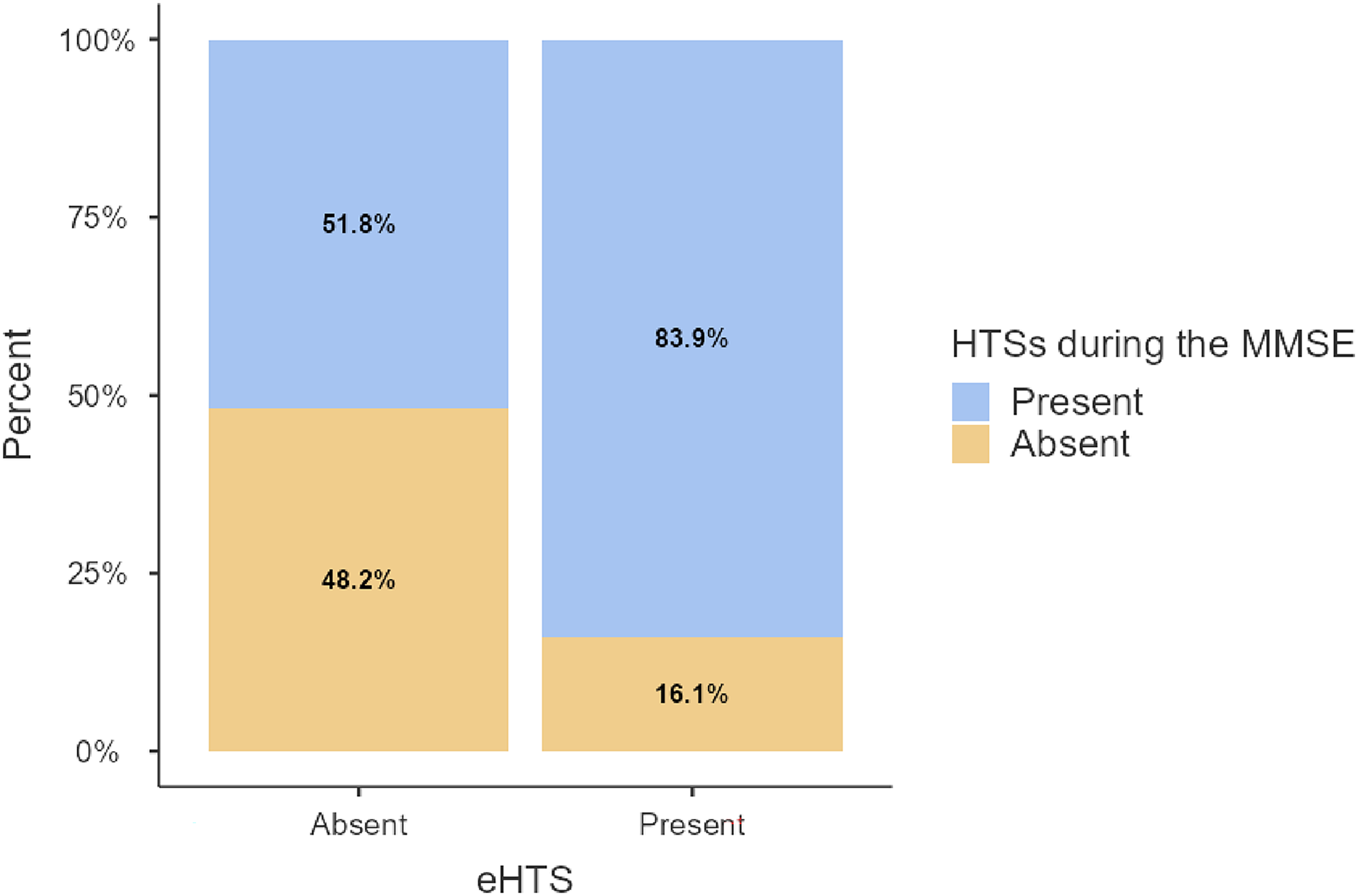
Stacked bar chart representing the prevalence of displaying or not at least one HTS during the MMSE in patients showing or not the eHTS.
Patients’ demographic and clinical features.

AD: Alzheimer's disease; FTLD: frontotemporal lobar degeneration; HTS: head turning sign; eHTS: ecological HTS; eHTS-: patients not showing the eHTS; eHTS+: patients showing the eHTS; LBD: Lewy body disease; MCI: mild cognitive impairment; MMSE: Mini-Mental State Examination; NADD: non-AD degenerative. adata missing for N = 1 eHTS + patient; bdata missing for N = 3 eHTS- patients and for N = 4 eHTS + patients; cdata missing for N = 2 eHTS- patients and for N = 1 eHTS + patient; dt-statistic; eχ2-statistic; fMann-Whitney's U-statistic; *Foderaro et al.'s normative dataset. Continuous outcomes are reported as M ± SD (range); categorical measures are reported as either frequencies or percentages.
HTS: head turning sign; MMSE: Mini-Mental State Examination; eHTS: ecological HTS.
HTS: head turning sign; MMSE: Mini-Mental State Examination; SO: Spatial Orientation; eHTS: ecological HTS.
HTS: head turning sign; MMSE: Mini-Mental State Examination; eHTS: ecological HTS.
The two groups were matched for sex, age and education. As to clinical variables, eHTS + patients had a longer disease duration (U = 968, p = 0.009) than the eHTS- group; however, no discrepancies in the distribution of the eHTS were found either among different etiologies (χ2 (5) = 3.11, p = 0.683) or based on MCI versus dementia status (χ2 (1) = 2.11; p = 0.147).
eHTS- patients outperformed the eHTS + group on the MMSE—this being true for both raw (t(110) = 3.48, p < 0.001) and demographically adjusted scores (U = 1024, p = 0.002). However, the percentage of patients whose scores fell below the established cut-off was not significantly different between the two groups (χ2(1) = 3.45, p = 0.063).
When looking at individual MMSE subtests/items, eHTS + patients performed worse than eHTS- on Language, Long-Term Memory, and Constructional Praxis measures (p ≤ 0.017). However, among these comparisons, only the one on Spatial Orientation survived Bonferroni's correction.
Thus, Model 1 tested the effect of disease duration and Spatial Orientation in predicting the occurrence of the eHTS. Spatial Orientation was a predictor of the presence of eHTS (b = −0.63; OR = 0.52, 95% CI [0.33, 0.75]; z = −3.20; p = 0.001), with post-hoc analyses showing that patients with lower Spatial Orientation scores (M-1*SD) had an estimated probability of exhibiting the eHTS of 0.72, while patients with average scores (M) had a probability of 0.51, and those with higher score (M + 1*SD) had a probability of 0.30 (Figure 2). However, only a trend towards significance was found as far as the effect of disease duration was concerned (b = 0.01; OR = 1.01, 95% CI [1.00, 1.03]; z = −1.77; p = 0.078).
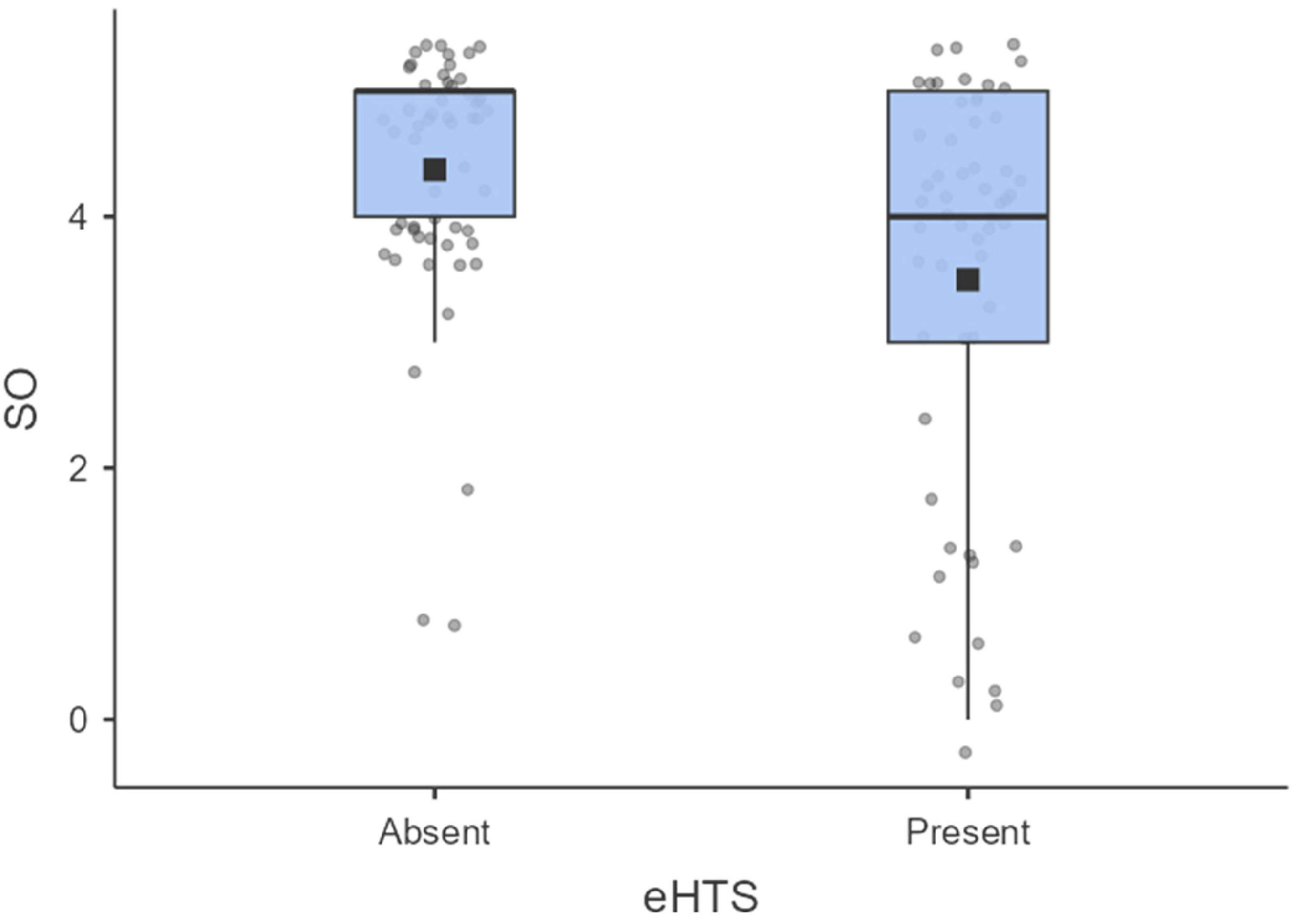
Box-plot representing Spatial Orientation scores from the MMSE (y-axis) in patients displaying (right) or not (left) the eHTS.
Moreover, Model 2 showed that, net of a marginally significant effect of disease duration (b = 0.01; OR = 1.01, 95% CI [1.00, 1.03]; z = −1.71; p = 0.085), a higher number of HTSs exhibited during the MMSE proved to be predictive of the presence of eHTS (OR = 1.41, 95% CI [1.19, 1.71]; z = 3.72, p < 0.001], with the post-hoc decomposition of this effect showing that patients who manifested a lower number of HTSs during the test (M-1*SD) had an estimated probability of exhibiting the eHTS of 0.26, while patients who manifested an average number of HTSs (M) had a probability of 0.52 and those who manifested a higher number of HTSs (M + 1*SD) had a probability of 0.77 (Figure 3). Similar results were detected as to Model 3, with the detection of at least one HTS during the administration of the MMSE predicting (b = −2.14; OR = 0.12, 95% CI [0.04, 0.33]; z = −3.86; p < 0.001) a higher probability of a patient falling under the eHTS + category (0.64) then the eHTS- one (0.17). Interestingly, in this last model, disease duration did reach significance (b = 0.02; OR = 1.02, 95% CI [1.00, 1.03]; z = 2.37; p = 0.018), with the post-hoc analysis showing that patients with a longer disease duration (M + 1*SD) had a higher probability of being classified as eHTS + then those having an average (M) or shorter (M-1*SD) disease duration (0.53 versus 0.38 versus 0.24, respectively).
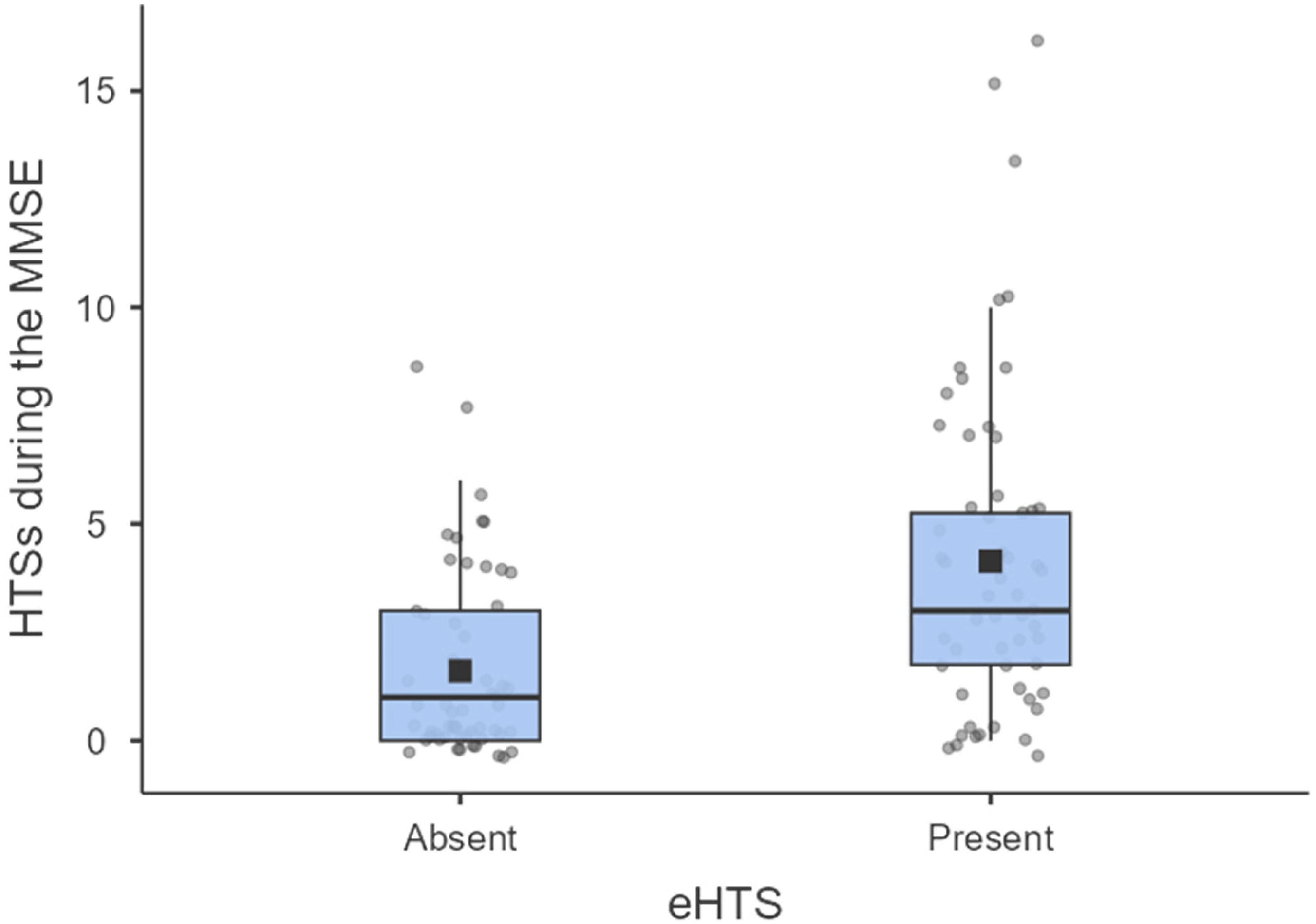
Box-plot representing the number of HTSs during the MMSE (y-axis) in patients displaying (right) or not (left) the eHTS.
Discussion
The present study explored the prevalence and correlates of the HTS displayed in daily life (i.e., the eHTS) in a fairly large (N = 112), retrospective cohort of patients with MCI and dementia due to chronic-degenerative etiologies. Moreover, we aimed at determining whether the detection of this sign within a clinical setting predicts its occurrence “beyond the clinic walls”.
A first, relevant finding lies in the fact that the eHTS was reported in half of the cohort—this suggesting that the behavior observed within cognitive screening sessions is relatively common in patients’ daily living as well. Such a stance also appears to be supported by the fact that the frequency of the eHTS reported here aligns with the vast majority of previous prevalence estimates of the sign in clinical settings.2,4–9
With regard to the correlates of the eHTS, the most consistent finding stemming from this study lies in the association between the presence of the eHTS and spatial disorientation. This partially aligns with a previous report from our research group, 10 where the occurrence of HTS during the administration of the MMSE was found to be associated with lower scores on its Temporal and Spatial Orientation subtests. 10 Taken together, these observations suggest that, in everyday life, the sign might be addressed as a compensatory or help-seeking behavior triggered by disorientation and/or confusion: in these terms, turning towards a reference person might represent an adaptive strategy to cope with a reduction in the ability to frame the situation at hand by relying on spatial (and possibly temporal) information.
As far as clinical variables are concerned, we found that longer disease duration was associated with a higher probability of showing the eHTS, although this effect not always reached full statistical significance. This suggests that, in everyday life, the eHTS might become more frequent in everyday life as cognitive impairment advances, possibly as a result of an increased reliance on external support over time. Another potential explanation lies in the fact that caregivers of patients with a longer disease duration might have had a higher chance of observing the sign in daily life due to more numerous opportunities for interaction with the patient throughout the disease course.
At variance, and in alignment with what has been reported in clinical settings, 10 the occurrence of eHTS in our cohort did not differ as a function of disease severity (i.e., MCI versus dementia status) or etiology. Thus, the present study appears to support previous findings as to its transdiagnostic value across different levels of cognitive involvement. 10
However, in respect to demographic features, and contrarily to previous findings, we found no significant differences in the prevalence of the eHTS based on sex or age. In fact, prior studies often reported, in clinical settings, a higher frequency of the HTS among older individuals and females.7,10,12 One possible interpretation is that, in real-life contexts, the HTS reflects a consolidated behavioral response primarily driven by cognitive determinants, with demographic factors such as sex and age playing a secondary role that may become evident in performance-based testing situations only.
A key contribution of the present work is the demonstration that the HTS observed during the administration of the MMSE predicts its occurrence in daily life, providing empirical support for its ecological validity, and, more specifically, for its veridicality (i.e., the degree to which a given measure collected within a clinical setting is related to daily-life functioning). 13 Interestingly, this was true when addressing both the number of HTSs displayed during the MMSE and the presence versus absence of the HTS itself within the screening session. Overall, these findings suggest that the HTS should not be addressed as a momentary reaction to testing conditions in clinical settings, but rather as a relatively stable and generalized behavioral pattern that can be traced in everyday-life scenarios as well. As a consequence, it might be useful for clinicians to inquire about the presence of this sign in everyday life during history taking from the accompanying person.
Some limitations of the present study should be acknowledged. First, the cohort was unbalanced across etiological subgroups, with AD being the most frequent one among them. This disproportion, which mirrors previous investigations7,10 and aligns with the epidemiology of cognitive disorders due to chronic-degenerative conditions, 14 might have prevented us from detecting meaningful discrepancies in the prevalence of the eHTS across diagnostic categories. Future studies should thus include patient cohorts with a greater representation of non-AD etiologies. Another issue concerns the assessment of the cognitive correlates of the sign. Although MMSE subtest- and item-level scores allowed for the exploration of domain-/function-level associations, the MMSE is, as a screening tool, far from comprehensively and exhaustively assessing specific cognitive facets. Additionally, the exclusion of patients unable to complete the MMSE may have introduced a selection bias by underrepresenting more severely impaired individuals, potentially leading to an underestimation of eHTS prevalence. Hence, to better clarify the cognitive correlates of the eHTS and capture performance across the full spectrum of impairment, future research should employ second-level cognitive tests and assessment strategies suitable for more severely impaired patients. Furthermore, the eHTS was assessed through caregiver reports rather than direct behavioral observation, which may be subject to recall and interpretation bias. In this regard, it should be noted that a caregiver who has just observed the HTS during the MMSE might more easily remember the occurrence of this sign in daily life (“prompted recall”) compared to a caregiver who has not observed it; this tendency could determine an overestimation of the association between the HTS during the MMSE and the eHTS. Finally, we did not examine the association between the eHTS and measures of behavioral changes and functional independence. Moreover, individual differences in personality traits (e.g., help-seeking behavior, dependency, or anxiety), as well as the nature of the relationship between patients and their caregivers, may influence the occurrence of the HTS in daily life independently of cognitive or clinical variables. Further research is warranted to better characterize the eHTS.
In conclusion, the present study suggests that, in patients with MCI and dementia due to chronic-degenerative etiologies, the HTS frequently occurs in daily life, associated with spatial disorientation. In addition, the present report hints at the fact that the number of HTSs displayed during cognitive screening sessions predicts its presence in daily life, thus supporting the ecological validity of this sign.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261452271 - Supplemental material for The head turning sign “outside the clinic walls” in patients with mild cognitive impairment and dementia
Supplemental material, sj-docx-1-alz-10.1177_13872877261452271 for The head turning sign “outside the clinic walls” in patients with mild cognitive impairment and dementia by Edoardo Nicolò Aiello, Francesco Cazzini, Arianna Moreschi, Beatrice Curti, Giulia De Luca, Francesca Frisco, Selene Saba, Valerio Patisso, Alessio Maranzano, Vincenzo Silani, Nicola Ticozzi, Federico Verde and Barbara Poletti in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors are thankful to patients and their caregivers. The authors thank Prof. Sara Mondini for her support. The authors acknowledge the support of the Italian Ministry of Health – Ricerca Corrente/Ricerca Finalizzata; Hub Life Science—Diagnostica Avanzata (HLS-DA), PNC-E3-2022-23683266, funded by the Italian Ministry of Health within the Complementary National Plan Innovative Health Ecosystem – and of the Italian Ministry of Education and Research (“Dipartimenti di Eccellenza” Program 2023–2027—Department of Pathophysiology and Transplantation, Università degli Studi di Milano).
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of IRCCS Auxologico (I.D.: 2021_05_18_04).
Consent to participate
All participants provided written informed consent.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Italian Ministry of Health—Ricerca Corrente.
Italian Ministry of Health - Ricerca Corrente, (grant number NA).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.P. is Associate Editor for Frontiers in Neuroscience; she received compensation for consulting services and/or speaking activities from Liquidweb S.r.l. V.S. received compensation for consulting services and/or speaking activities from AveXis, Cytokinetics, Italfarmaco, Liquidweb S.r.l., Novartis Pharma AG, Amylyx Pharmaceuticals, Biogen, and Zambon Biotech SA; he receives or has received research supports from the Italian Ministry of Health, AriSLA, and E-Rare Joint Transnational Call; he is in the Editorial Board of Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration, European Neurology, American Journal of Neurodegenerative Disease, Frontiers in Neurology, and Exploration of Neuroprotective Therapy. E.N.A. serves as an Editorial Board Member for BMC Neurology. E.N.A. and F.V. are Editorial Board Members of this journal but were not involved in the peer-review process of this article nor had access to any information regarding its peer-review. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Datasets associated with the present study cannot be made publicly available on ethical-legal grounds but have been stored on an online repository (https://doi.org/10.5281/zenodo.20133986) and can be made available upon reasonable request of interested researchers to the Corresponding Author(s), who will forward a request for a data transfer agreement to the relevant Ethical Committee(s).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.