
Abstract
Background
Alzheimer's disease and related dementias (ADRD) were the sixth leading cause of death among people aged 65 + in 2022 and are currently the leading cause of disability and morbidity in older adults. In 2025, an estimated 7.2 million Americans aged 65 years and older were living with Alzheimer's disease (AD), with prevalence projected to rise.
Objective
We describe 1) the trends in the adoption of ADRD policies that were implemented in the U.S. from 2008–2020, as well as 2) the trends in ADRD mortality during 1999–2022.
Methods
We presented mortality data for the age-adjusted rate of ADRD mortality per 100,000 people in 1999–2022 from the Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research (CDC WONDER). We also collected policy data from state websites from 2008–2020.
Results
Policies were implemented for all 50 states, starting in 2008 and ending in 2020. ADRD mortality steadily rose during 1999–2022. The first states to implement ADRD in 2008 were Iowa and Kentucky. The largest number of states added policies in 2013. South Dakota, Wyoming, Ohio, and Kansas were the last states to implement policies.
Conclusions
Our study documented that all the states in the United States implemented a policy to reduce ADRD cases. We also observed that ADRD mortality steadily rose between 1999 and 2022. This rise may reflect increased reporting of ADRD as a cause of death, or policies needing more time to meet national reduction goals.
Introduction
Alzheimer's disease and related dementias (ADRD) were the sixth leading cause of death among people aged 65 and older in 2022 and are currently the leading cause of disability and morbidity in older adults. 1 According to the World Health Organization (WHO), ADRD was the third and fourth leading cause of death for women and men respectively in 2021. 2 In 2022, there were at least 6.5 million Americans, 65 years and older, living with Alzheimer's disease (AD) and this prevalence rose to 7.2 million by 2025.1,3 In the U.S., 10.9% of people aged 65 and older, including 5% of people 65–74, 13.2% of people 75–84, and 33.4% of people 85 and older have AD. 1 These prevalence estimates need to be lowered to reach federal National Alzheimer's Project Act (NAPA) goals. However, federal NAPA goals may not be achievable without the support of state policies, as state-level policies more directly influence day-to-day care. 4
The prevalence of dementia varies by state with Alaska having the lowest percentage at 8.8% and Maryland having the highest at 12.9%. 1 The 10 counties with the highest dementia prevalence are from Texas, California, South Carolina, Georgia, Louisiana, Mississippi, Maryland, New York, Maryland, and Florida in increasing order. 1 This alludes to potential geographical disparities for dementia. In addition to substantial prevalence, dementia is deadly for older populations, solidifying the importance of effective interventions. Among Americans aged 70 and older, 61% of those with dementia are expected to die before they turn 80 compared to 30% of people without dementia. 1 The mortality rate due to dementia in each state in the U.S. greatly varies; from 18.1 in New York to 57.4 per 100,000 individuals in Mississippi. This estimate has increased 141% from 2000 to 2021 (17.6 to 36 per 100,000 people). The high prevalence and mortality of dementia are reasons why policies that aim to prevent ADRD by focusing on risk factors are crucial.
In an effort to reduce the burden of ADRD in the United States, individual states have adopted specific strategic plans addressing the burden of ADRD. This was accelerated by the National Alzheimer's Project Act (NAPA) which was signed in 2011 and which focused on research and improved care/services for individuals living with ADRD.5,6 NAPA stated six subgoals to achieve its overall goal of improving the lives of those with this disease: 1) prevent and effectively treat ADRD by 2025; 2) enhance quality and effectiveness of care; 3) expand support for people with AD/ADRD and their families; 4) enhance public awareness and engagement of ADRD; 5) improve data so it is easier to track progress and 6) promote healthy aging by accelerating action and reduce risk factors for ADRD.5,6 As each state strives to achieve these goals, documenting and describing state ADRD policies and ADRD outcomes becomes essential.
This study's aims are twofold: 1) describe trends in the adoption of ADRD policies that were implemented in the U.S. from 2008–2020, 2) describe trends in ADRD mortality during 1999–2022.
Methods
Data sources
We focused on all 50 states adopting their own state's ADRD policies in 2008–2020. We also described the mortality trends for the age-adjusted rate of ADRD mortality per 100,000 individuals. Information on ADRD policies came from state policy and state aging websites (Supplemental Table 1). Mortality data came from the Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research (CDC WONDER). 7 Causes of death were classified using ICD-10 codes. 7
Variables and measures
ADRD policies
The ADRD policies included those that aimed to reduce ADRD cases or mortality from ADRD. The identified policies were state policy plans and are described in more detail in the supplementary materials. Policy implementation was defined as a state initiating a published state ADRD plan or roadmap where all plans were non-funded legislation. The target populations for all 50 collected policies were persons living with ADRDs and family caregivers and 23 policies also added the target population of healthcare and/or social service providers (Supplemental Table 1). The overarching goal for these states’ policies focused on supporting individuals with ADRD, supporting family caregivers, addressing growing cases or financial costs, increasing research and/or data collection, and supporting healthcare providers (Supplemental Table 1).
ADRD mortality
ADRD mortality was the age-adjusted rate of mortality for people who die from ADRD per 100,000 individuals. These data came from CDC WONDER for 1999 to 2022.
Results
Figure 1 shows the data structure for policy implementation ordered by the state which first implemented the policy (hence the longest) to the state that implemented it last (hence the shortest). Iowa and Kentucky were the first states to implement ADRD policies in 2008. Several states followed in 2009 including: Louisiana, Michigan, North Dakota, Oklahoma, South Carolina, Tennessee, and Vermont. In 2010, Colorado, Missouri, and Texas implemented their ADRD state policies. Another six states added policies in 2011 and four in 2012. The largest number of states added policies in 2013 with 10 states implementing their ADRD policies. Georgia, Illinois, Pennsylvania, Rhode Island and Wisconsin were added to the list in 2014 and two added in 2015. Seven states implemented policies in 2016. The last states to add policies in 2018–2020 were South Dakota, Wyoming, Ohio, and Kansas.

Implementation of ADRD policies for each state in the U.S. (2008–2020).
Figure 2 illustrates an increase in age-adjusted ADRD mortality rate from 1999 to 2010, with slower growth from 2012 to 2022. In 2020, the rate seems to plateau, but more data are necessary to observe if this is a true plateau or still results in an increase a few years later. However, the standard errors become larger in the years 2012–2022, indicating the rate may be less precise in the most recent decade.
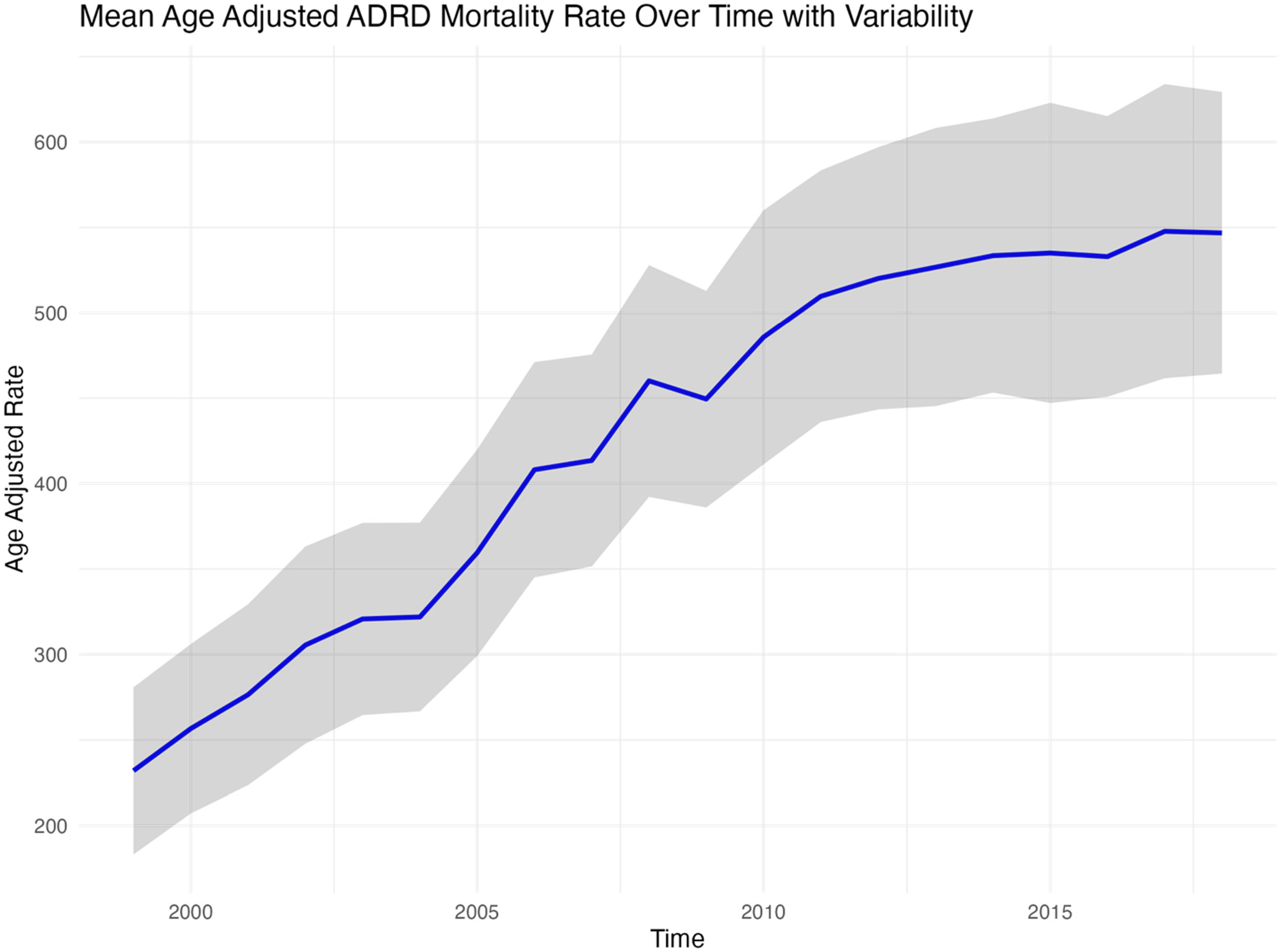
Mean age adjusted ADRD mortality rate in U.S. for 1999–2022.
Discussion
The purpose of this study was to describe trends in the adoption of ADRD policies implemented in the U.S. from 2008–2020 as well as trends in ADRD mortality during the same period. The increase in mortality before any decrease is common in research as the implemented policy can facilitate increased ADRD diagnoses as awareness increases.8,9 Data for actual observed ADRD prevalence across the years and states during the same policy periods were not available but would be expected to increase due to 1) an increase detection of ADRD and 2) an increase in ADRD risk factors which include common vascular factors such as diabetes and hypertension. 10
Although ADRD policies were implemented, there was still a rise in mortality. This can be partially explained by increases in life expectancies because age is one of the greatest risk factors for ADRD. 1 As the population ages, the number of individuals at highest risk for developing ADRD is expected to increase. In the absence of a cure, this demographic shift will also lead to an increase in ADRD-related mortality. Another reason for the consistent increase in ADRD mortality is the persistent disparities that remain due to the unaddressed social determinants of health. Having a lower socioeconomic status and living in a rural environment are two risk factors that may remain unaddressed by policy changes and could allow for persistent ADRD deaths.1,11 When a policy is first implemented, it is usual to find an increase in prevalence to occur due to increased primary prevention methods such as testing, screening, and diagnostic capacity. 12 If there are prevention measures implemented in the policy, then the incidence is expected to decrease. 13 Although our study did not assess ADRD prevalence or incidence, mortality may still be affected by policy changes. Given the variety of times the policies were implemented and the long prodromal period of ADRD, it is unsurprising that the policies implemented did not change the mortality rates due to the longer time required to see changes in ADRD outcomes. Policies that draw attention to a specific disease can increase clinical recognition and diagnostic awareness, which in turn may lead to more frequent reporting of ADRD on death certificates. Diagnostic coding practices differ across all U.S. states due to access to resources and state priorities. In most cases, dementia diagnoses remain non-specific due to limited access to specialists. 14 This increase in ADRD reporting includes upcoding and diagnostic ambiguity which can decrease the reliability of claims data. 14
The contents of these state ADRD policies varied from state to state. The first states to implement policies, Iowa and Kentucky, were both focused on the individuals living with ADRD and their caregivers. Iowa's goal was to address the current needs of the state and prepare for future needs associated with projected increase in individuals diagnosed with ADRDs whereas Kentucky aimed to mitigate the impact on families, the healthcare system, communities, public safety, and long-term care resources (Supplemental Table 1). Even though these states both implemented plans in 2008, the broad goal of Iowa's plan compared to the details of Kentucky's plan reflect some of the differences between state policies. Many states focused their policies on broad goals for supporting the healthcare systems, meeting needs for individuals with ADRD, and increasing ADRD research but a state that stood apart in its policy's goals was California. California targeted a range of topics of focus including eliminating stigma, ensuring access to high quality and coordinated care in an individual's setting of choice while establishing more comprehensive support for family caregivers, developing an “Alzheimer's proficient, culturally competent workforce”, expanding ADRD-related research, and creating coordinated state care delivery infrastructure (Supplemental Table 1). This number of goals outlining all aspects of ADRD care surpassed other state's policies with their general goals to lessen disease burden for the state. The content of the policies implemented could have an effect on the state level ADRD outcomes. Unlike general state plans that focus on affected populations without addressing root causes of disparities and poor public health outcomes, comprehensive state plans directly target the underlying mechanisms for ADRD development, public health outcomes, and treatment. As a result, comprehensive plans are better positioned to achieve federal NAPA goals.
Legislation on ADRD is frequently being suggested and implemented into state policies. More recently, states have been targeting issues regarding long-term care facilities, disease mitigation, research, and other factors that emerge when examining the difficulties of ADRD. For instance, Kentucky enhanced security protocols and training of staff working in assisted living facilities and Tennessee created a program to provide home- and community-based services. 15 In 2015, Alabama created recommendations focusing on single source of information, education, and referral for families and caregivers and promoting adult day care services especially extending Medicaid to cover these services. 16 In 2021–2022, Pennsylvania passed a bill to help healthcare providers with early detection and diagnosis of ADRD and West Virginia passed a bill requiring training be developed for law enforcement to promote appropriate interactions with individuals with ADRD. 15 Similarly, in 2024, Governor Newson signed policies for law enforcement in California to have; training on preventing and responding to wandering by persons with ADRD, continuing education for healthcare providers who provide care to elderly populations, and improve delivery of local aging services. 17
There are regional disparities that exist in ADRD risk and mortality.18–23 Place of residence and environment in critical life periods have been found to be associated with ADRD mortality rates.20–23 The environmental exposures one faces throughout their life has a major impact on their risk of ADRD mortality such as access to reliable education in early life and state-specific health policies in mid and late-life.21,23 Access to proper health care is crucial in the prevention of death from ADRD and other chronic diseases.
Individuals with dementia have a higher risk of mortality. 24 This appears to be because people with dementia are more likely to suffer from other comorbidities such as somatic and psychiatric diseases. 24 Also, dementia disorders have been found to increase mortality due to frailty, comorbidities and insufficient or inappropriate treatment for other diseases among persons living with ADRD.25–28
Implementation of policy is dependent on multiple factors such as the state's political will, financial availability, state priorities, and state-specific needs. 6 For example, states that had larger increases in ADRD cases may choose to prioritize ADRD prevention more than states that had smaller increases in ADRD cases. The Assistant Secretary for Planning and Evaluation (ASPE) presented a National Plan to Address Alzheimer's Disease with the following goals: prevent and effectively treat AD by 2025, enhance care quality and efficiency, expand supports for people with AD and their families, enhance public awareness and engagement, and improve data to track progress. 6 Some noteworthy suggestions to accomplish these goals include expanding research to identify risk and protective factors, molecular and cellular mechanisms, educate health care providers, strengthen workforces for direct care and aging, and increase clinical trial enrollment. Different states will have different resources and representatives that have different opinions about how important ADRD is to their state.
In addition to these state specific policies, the U.S. targeted some major goals focusing on ADRD. Given the unrealized promise of disease-modifying medications on ADRD outcomes, policies targeting modifiable risk factors such as less education, hearing loss, hypertension, diabetes still have the potential to reduce the risk of developing ADRD. 29 The U.S. has several policies for action including a national dementia plan with a focus on early action; public health initiatives that promote risk reduction, mitigation, and early detection; and research efforts on enabling these public health initiatives. 30
Every state in the U.S. has implemented a state ADRD policy to decrease incidence and mortality and improve care of people with ADRD, but the impact of these policies remains unknown. The type of analysis to uncover the impact of such policies would include strong analytical methods such as quasi-experimental design, for instance interrupted time series designs. 31 The impact of these policies may take decades to recognize given that ADRD can remain dormant in individuals for several decades before symptoms occur.
This study was not without limitations. First, there could be misclassification in the ADRD mortality data. ADRD is usually diagnosed postmortem but there are other diseases that could have caused death in a person with ADRD, pneumonia being the most common.32,33 Note that inter-regional differences in filling out death certificates does not appear to account for significant differences in mortality. 19 Second, the polices implemented varied from state to state. It is possible that some policies could have had more impact than others if implemented in a specific state such as being given more funds or targeting specific populations of the dementia care triad during implementation. There was a slight increase in cases in 2020–2021, likely due to the increases in ADRD mortality contributing cause of death during the pandemic. 34 Compared to pre-2020 trends, the plateau between 2020–2022 may be partially explained by a harvesting effect, in which frail, high-risk individuals with ADRD died from COVID-19 or its complications rather than from ADRD itself. 35 Furthermore, our study did not evaluate the impact of ADRD policies on ADRD mortality. Future studies should utilize appropriate methods such as quasi-experimental designs to assess the relative impact of state ADRD policies on ADRD outcomes over time.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261453609 - Supplemental material for Alzheimer's disease and related dementias state policies and mortality in the United States: A descriptive study
Supplemental material, sj-docx-1-alz-10.1177_13872877261453609 for Alzheimer's disease and related dementias state policies and mortality in the United States: A descriptive study by Nicola Churchill, Thuy-Tien Le and Roch A. Nianogo in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
All ethical guidelines for research were followed. This study used publicly available de-identified data and as such did not qualify as human subject research; therefore, institutional review board approval was not required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NC and RAN were partially supported by the Alzheimer's Association (AARGD-NTF-22-924312). The funders had no role in the preparation, review, or approval of this manuscript, or the decision to submit the manuscript for the publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.