
Abstract
Background
Early Alzheimer's disease (AD)-related cognitive vulnerability is characterized by subtle disruptions in attentional and executive processing that may precede overt declines in global cognitive scores. Identifying process-sensitive behavioral markers capable of capturing these early alterations remains a major challenge in psychogeriatric assessment.
Objective
To examine whether eye-movement–derived process-level measures, particularly fixation-shift dynamics, are associated with early cognitive vulnerability in older adults and whether they provide incremental value beyond conventional cognitive screening scores in an AD-related context.
Methods
This cross-sectional study enrolled 109 adults aged ≥65 years, categorized as cognitively normal (CN, n = 33), mild cognitive impairment (MCI, n = 35), and dementia due to AD (ADD, n = 41). Participants completed a standardized online interactive cognitive task while eye movements were recorded using a non–head-fixed, desktop-based eye-tracking system. Cognitive-only, eye-movement–only, and combined multimodal models were compared using receiver operating characteristic (ROC) analysis and area under the curve (AUC).
Results
The combined multimodal model consistently outperformed single-modality approaches. Discriminative performance was high for CN versus ADD (AUC = 0.925) and for CN versus cognitively impaired participants overall (AUC = 0.897). Fixation-shift dynamics emerged as a robust process-level marker, demonstrating particular sensitivity in distinguishing CN individuals from those with MCI.
Conclusions
Fixation-shift eye-movement dynamics capture early AD-related cognitive vulnerability beyond conventional total cognitive scores. This multimodal framework may support psychogeriatric screening and clinical triage by detecting subtle cognitive inefficiencies that precede measurable declines on standard cognitive tests.
Keywords
Introduction
Dementia represents a major public health challenge driven by global population aging. According to the World Health Organization, more than 55 million people worldwide currently live with dementia, a number projected to increase to 78 million by 2030 and 139 million by 2050. 1 In Taiwan, epidemiological surveys report a dementia prevalence of 7.99% among adults aged 65 years and older, while an additional 17.99%, over 730,000 individuals, meet criteria for mild cognitive impairment (MCI), a transitional stage associated with increased risk of dementia, including Alzheimer's disease (AD).2,3 AD accounts for approximately 60%–70% of dementia cases, with prevalence rising sharply with advancing age. Together, these trends underscore the need for scalable and clinically meaningful approaches to identify early cognitive vulnerability in aging populations before irreversible functional decline occurs.4,5
Early identification of MCI and AD-related cognitive impairment commonly relies on brief cognitive instruments such as the Mini-Mental State Examination (MMSE), the Clinical Dementia Rating (CDR), and the Montreal Cognitive Assessment (MoCA). Among these, the MoCA has demonstrated improved sensitivity for distinguishing MCI from normal cognitive aging. 6 Nevertheless, important limitations persist. Global cognitive scores provide relatively coarse summaries of working memory, visuospatial processing, and executive control, and test performance may be influenced by educational background, language proficiency, and cultural context.7,8 Consequently, subtle disease-related alterations in cognitive processing efficiency, particularly those affecting attentional and executive control rather than overt task accuracy, may precede measurable declines in total scores and remain undetected by conventional screening approaches.
Eye-tracking technology offers a noninvasive and objective means of quantifying oculomotor behavior associated with attention, memory, and visuospatial–executive processing. Core eye-movement measures, including fixations, saccades, and smooth pursuit, reflect underlying cognitive processes that are vulnerable in the earliest stages of neurodegeneration. Prior studies have shown that eye-movement features can differentiate individuals with MCI or early AD from cognitively normal older adults, reveal subtle impairments not captured by conventional neuropsychological assessments, and exhibit relative independence from language and educational confounders.9–11 These characteristics suggest that eye-movement metrics may provide complementary insight into early cognitive vulnerability in older adults.
Despite these promising findings, it remains unclear whether eye-movement–derived process-level measures provide incremental value when assessed within a standardized cognitive task context, particularly during transitional stages such as MCI. Conventional approaches relying on end-point cognitive scores may lack sensitivity to early inefficiencies in cognitive processing, reflecting a broader measurement gap between observable task performance and underlying disease-related cognitive dynamics.
Disruptions in fixation-shift dynamics, which index the efficiency and flexibility of visual attention allocation, may reflect early dysfunction of frontoparietal attentional and executive networks implicated in prodromal AD. Such process-level inefficiencies may emerge prior to overt performance failure on conventional cognitive tests, thereby providing a window into early AD-related cognitive vulnerability.
Accordingly, the present study examined whether eye-movement–derived process-level measures, particularly fixation-shift dynamics, are associated with early cognitive vulnerability in older adults across cognitively normal individuals, those with MCI, and those with dementia. By evaluating the incremental value of these behavioral markers beyond conventional cognitive screening scores, we aimed to clarify their potential relevance for psychogeriatric assessment, early risk stratification, and clinical monitoring in outpatient and community-based settings.
Methods
Setting/study population
A total of 112 individuals were purposively recruited from neurology and geriatric outpatient clinics, community senior centers, and adult day care facilities in northern and central Taiwan between May and September 2025. Three participants were excluded due to incomplete assessments or withdrawal, resulting in a final analytic sample of 109 participants (cognitively normal [CN], n = 33; mild cognitive impairment [MCI], n = 35; dementia due to AD [ADD], n = 41).
Eligible participants were aged 65 years or older, provided informed consent, and met CDR criteria for their respective cognitive groups: CN (CDR = 0), MCI (CDR = 0.5 with preserved activities of daily living or clinician-confirmed MCI), and ADD (CDR ≥ 0.5 with a physician-confirmed diagnosis). Exclusion criteria included acute medical or psychiatric illness, major psychiatric disorders, significant visual impairment, severe ocular disease, or inability to complete the computerized cognitive or eye-tracking assessments. Participants were allowed to wear their habitual corrective lenses (e.g., glasses) during the assessment to ensure adequate visual performance. Individuals with severe dementia were not included, as they were unable to reliably complete the computerized and eye-tracking tasks.
The mean age of participants was 74.8 ± 7.6 years (range 65–96), with CN participants younger (70.5 ± 7.0) than MCI (76.7 ± 8.2) and dementia (76.6 ± 6.2) groups. Women comprised 64.2% of the sample. Regarding education, 59.6% had completed junior high school or higher, with higher proportions in CN (78.8%) and MCI (65.7%) groups, whereas most dementia participants (61.0%) had elementary school education or below. The dementia group included 41 participants able to follow test instructions, with 13 (31.7%) having a CDR of 0.5 and 28 (68.3%) a CDR of 1. Participant characteristics are summarized in Table 1.
Demographic and clinical characteristics of cognitively normal, MCI, and dementia participants.
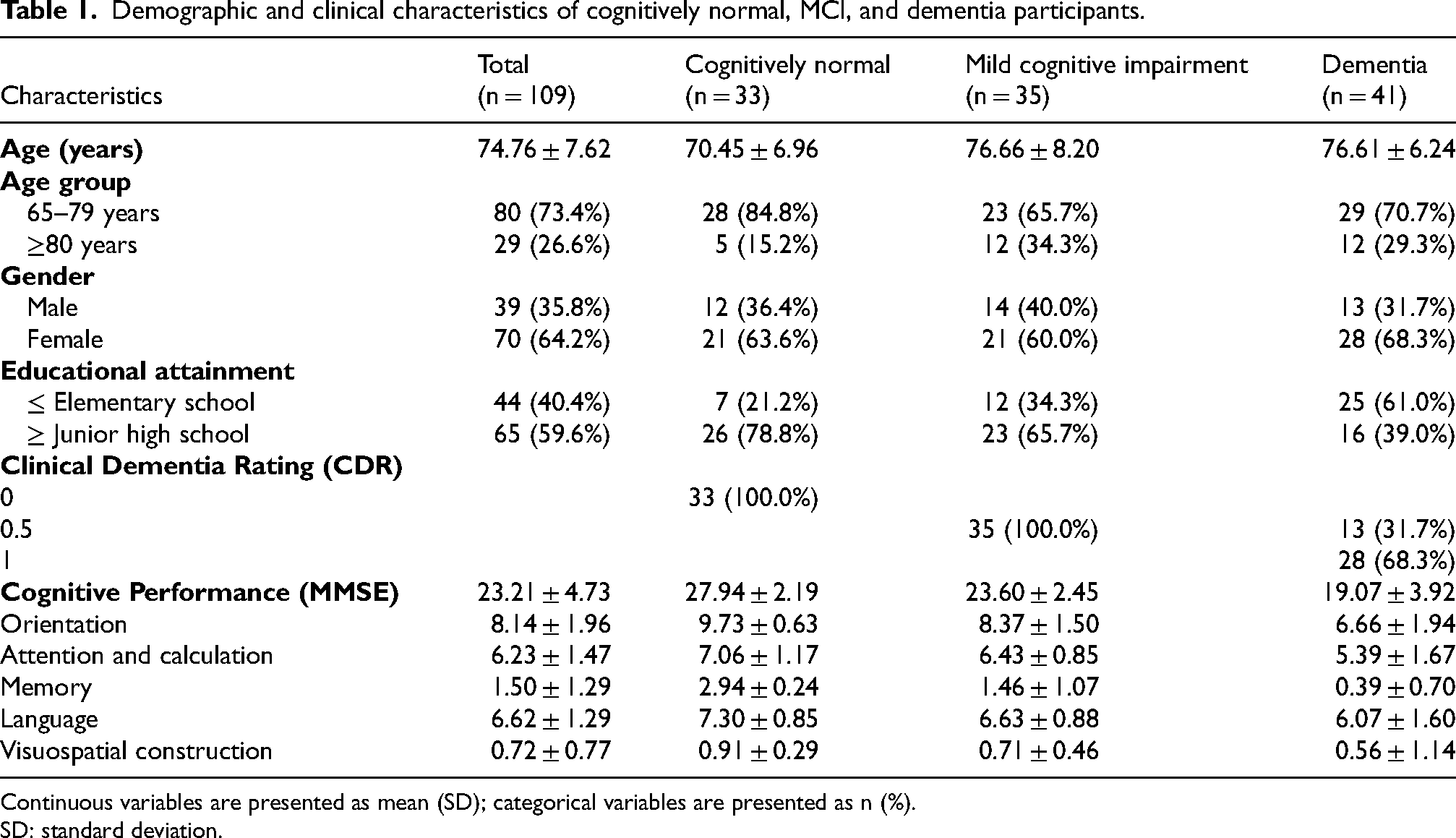
Continuous variables are presented as mean (SD); categorical variables are presented as n (%).
SD: standard deviation.
Instruments/device
Demographic and clinical data
Demographic and clinical data were obtained from participants’ electronic medical records and documentation provided by hospital or adult day care centers. Collected variables included age, sex, and education level. Cognitive status and dementia severity were assessed using the CDR scale and the MMSE.
The CDR is a semi-structured, interview-based instrument administered to participants and their informants to assess cognitive and functional performance across six domains: memory, orientation, judgment and problem solving, community affairs, home and hobbies, and personal care. 12 Based on the global CDR score, participants were classified into five levels of cognitive impairment, ranging from no dementia to severe dementia (0, 0.5, 1, 2, and 3). The MMSE is a brief cognitive screening tool consisting of 11 items that assess orientation, attention and calculation, memory, language, and visuospatial construction. 13 Total MMSE scores range from 0 to 30, with lower scores indicating greater cognitive impairment; scores of 21–26 indicate mild impairment, 10–20 moderate impairment, and <10 severe impairment.
Customized online interactive cognitive screening tool
This study employed a customized online interactive cognitive screening tool developed by the research team. Task selection and targeted cognitive domains were informed by the cognitive constructs assessed in the MoCA, a widely used screening instrument with established reliability and validity.14,15 Rather than replicating or replacing the MoCA, the tool was designed as a standardized digital adaptation to approximate key cognitive domains while providing a controlled task context for capturing process-level behavioral dynamics during task execution. Design principles from prior work on interactive computer-based paradigms for early detection of AD guided both the response processes and the user interface. 16
To enhance feasibility in an online setting, the assessment excluded tasks requiring paper-and-pencil drawing or verbal responses. All items were administered using mouse-click responses, including multiple-choice formats and interactive selection mechanisms. The final version comprised 13 items with a maximum total score of 17 points, covering major cognitive domains typically evaluated by the MoCA, with the exception of language-related items. This design aimed to preserve broad cognitive coverage while ensuring compatibility with online, self-paced administration. Detailed descriptions of individual item formats and their corresponding cognitive domains are provided in the Supplemental Material.
Because this instrument represents a customized online adaptation rather than the original MoCA, established MoCA cutoff scores and total-score interpretations were not applied. Classification performance and optimal cutoff values were instead determined empirically using receiver operating characteristic (ROC) analyses, sensitivity, and specificity, consistent with its intended use as a screening and research tool rather than a diagnostic substitute.
For analytic purposes, test items were further categorized into three task types based on their cognitive and visual processing demands. Search tasks required participants to visually locate and identify a target stimulus prior to response selection. Memory tasks emphasized immediate encoding and delayed retrieval processes. Cognitive processing tasks involved rule-based judgment or decision-making prior to response execution. The mapping of individual items to cognitive domains and task categories is detailed in the Supplemental Material.
Although certain MoCA subdomains, such as clock drawing, language, and abstract reasoning, were not administered in their original formats, the underlying cognitive processes associated with these domains were engaged through the interactive task structure. Specifically, visuospatial planning, semantic discrimination, and rule-based abstraction were elicited by tasks requiring visual search, decision-making, or response selection (e.g., search and cognitive processing tasks). Eye-movement measures were applied only to tasks involving visual exploration, capturing the efficiency and organization of cognitive processing at the level of task execution rather than overt verbal or motor output. Tasks primarily assessing orientation or memory without explicit visual exploration demands were included in the cognitive score analyses but were not used for eye-movement feature extraction.
During testing, all items were presented sequentially on the computer screen, and participants completed the assessment using mouse-click responses. This design allowed for both standard cognitive scoring and selective integration of eye-movement metrics for process-level analyses.
Eye-tracking device
Eye movements were recorded using the Gazepoint GP3 eye tracker (Gazepoint Research Inc.), a desktop-based, infrared eye-tracking system that operates without wearable sensors or head stabilization. The system was configured in a non–head-fixed setup designed to approximate natural computer use, with participants seated comfortably in front of a laptop computer under standard ambient lighting conditions. Participants were instructed to maintain a viewing distance of approximately 55–65 cm, consistent with the manufacturer's recommended operating range (Figure 1).
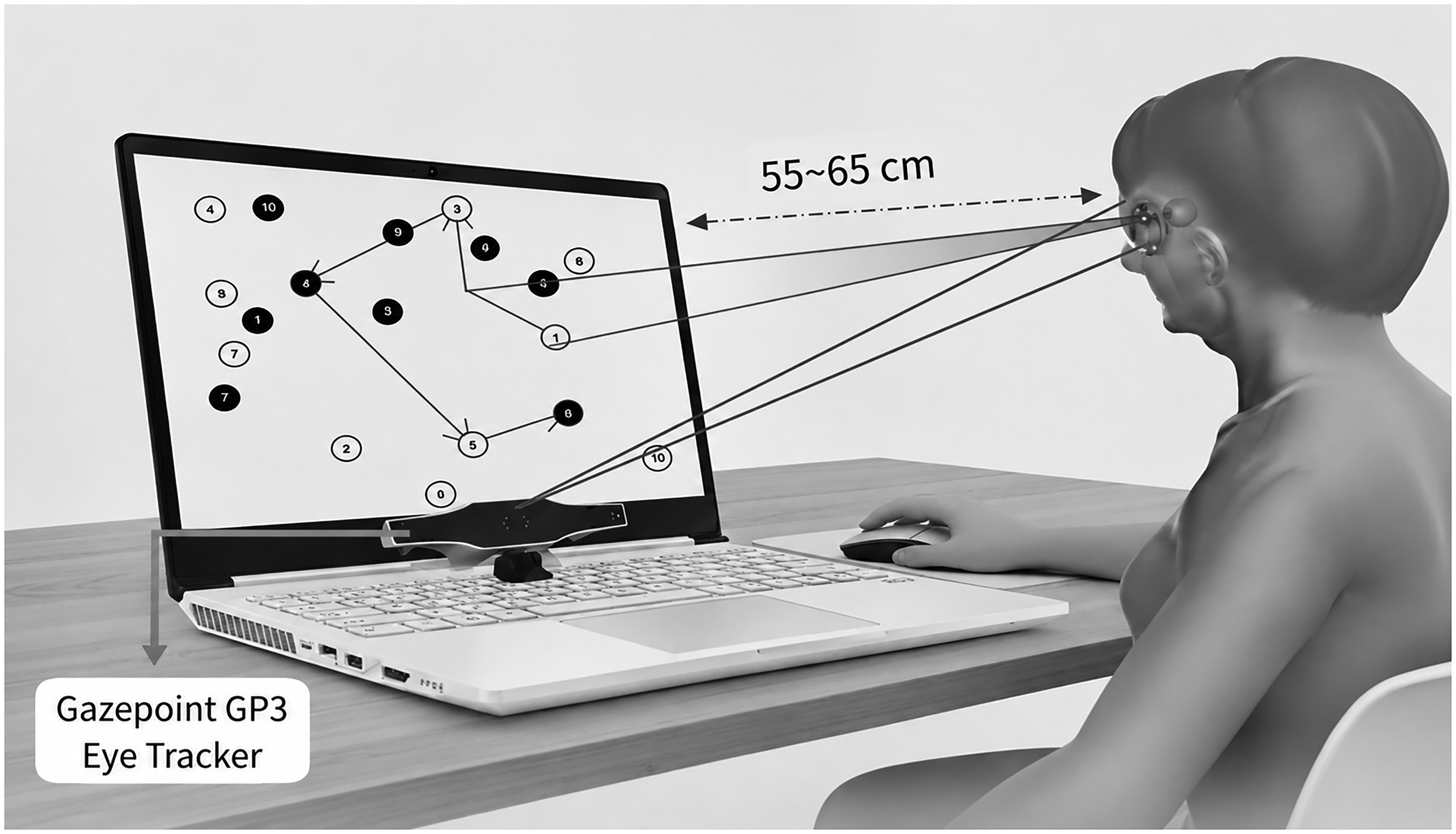
Schematic illustration of the test setup. Participants were instructed to maintain a viewing distance of approximately 55–65 cm.
Prior to task initiation, a standard calibration procedure was performed for each participant to establish gaze–screen correspondence. Calibration was repeated if initial calibration quality did not meet the manufacturer's acceptance criteria. Eye-tracking data were collected at a sampling rate of 60 Hz while participants completed the customized online interactive cognitive screening tasks. The test interface was displayed on a laptop computer with a screen resolution of 1920 × 1080 pixels and a display area of approximately 34.4 × 19.4 cm. All device placement, calibration, and data acquisition procedures adhered to the manufacturer's guidelines. 17
During task performance, the Gazepoint GP3 continuously captured multiple eye-movement parameters using infrared pupil-tracking technology, including fixation shifts, fixation error, target fixation position, and cursor position. To enhance robustness under non–head-fixed conditions, subsequent analyses focused on relative and aggregate eye-movement metrics rather than absolute gaze coordinates. Fixation shifts were defined as transitions between successive fixation points and were used to characterize patterns of visual attention allocation and information-processing efficiency. 18 Fixation error was defined as the spatial discrepancy between the estimated fixation location and the target stimulus and was used as an index of visual localization accuracy and oculomotor control.16,19
Basic data quality control procedures were applied prior to analysis. Eye-tracking segments exhibiting evident tracking loss, such as prolonged absence of valid gaze samples or unstable pupil detection, were excluded. Participants with insufficient usable eye-tracking data across tasks were not included in eye-movement analyses. These procedures were implemented to reduce the influence of signal noise while preserving ecological validity in a non–head-fixed testing environment. Only eye-movement features directly related to visual search and spatial localization, specifically fixation shifts and fixation error, were retained for inclusion in the analytic models.
Procedure
After obtaining written informed consent, participants’ medical records and demographic data were reviewed, including CDR and MMSE scores. Eligibility criteria were reconfirmed prior to testing. Participants subsequently completed a series of online interactive cognitive screening tasks in a quiet, well-lit environment. During task performance, eye movements were continuously recorded using a Gazepoint GP3 infrared eye tracker positioned below the laptop screen, with a viewing distance maintained between 55 and 65 cm. The tasks were administered sequentially, and participants provided responses via mouse clicks.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Taoyuan General Hospital, Ministry of Health and Welfare, Taiwan (IRB No. TYGH113107). The study was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from all participants or their legally authorized representatives prior to participation, and participants with dementia provided assent whenever possible. All data were anonymized and handled confidentially in accordance with institutional regulations.
Statistical analysis
All analyses were performed using SPSS (version 26.0). Descriptive statistics were used to summarize participant characteristics, cognitive screening scores, and eye-tracking measures. Continuous variables are presented as means ± standard deviations, and categorical variables as frequencies and percentages. Three predictive models were constructed to assess the discriminative performance of an online interactive cognitive screening tool and eye-tracking measures: (1) a scale-only model based on the total screening score, (2) an eye-tracking–only model using gaze features, and (3) a combined model incorporating both measures. Four binary classification tasks were evaluated: CN versus cognitively impaired (MCI + dementia), CN versus MCI, CN versus dementia, and MCI versus dementia.
Model performance was evaluated using ROC curve analysis, with the area under the curve (AUC) as the primary measure of discriminative validity. The optimal cutoff score for the screening test was determined using Youden's Index to maximize the balance between sensitivity and specificity. 20 AUCs were compared across models to examine the incremental diagnostic value of eye-tracking measures. All statistical tests were two-tailed, with statistical significance set at p < 0.05.
Results
Discriminative performance of the online interactive cognitive test
ROC curve analysis showed that the total score of the online interactive cognitive test was able to discriminate cognitively normal older adults from cognitively impaired individuals (including MCI and dementia), with an area under the curve (AUC) of 0.877 (p < 0.001). The optimal cutoff score was 14 points (threshold = 14.5), corresponding to a sensitivity of 75.0% and a specificity of 84.8%.
In the comparison between cognitively normal older adults and individuals with MCI, the AUC was 0.834 (p < 0.001). The optimal cutoff score was 15 points (threshold = 15.5), yielding a sensitivity of 88.6% and a specificity of 66.7%. For the comparison between cognitively normal older adults and individuals with dementia, the test demonstrated an AUC of 0.914 (p < 0.001). Using the same cutoff score of 14 points (threshold = 14.5), sensitivity and specificity were 92.7% and 66.7%, respectively.
In the comparison between individuals with MCI and those with dementia, the AUC was 0.672 (p = 0.010). The optimal cutoff score of 14 points (threshold = 14.5) resulted in a sensitivity of 82.9% and a specificity of 65.7% (Table 2).
Discriminative performance of the online interactive cognitive test (ROC analysis).
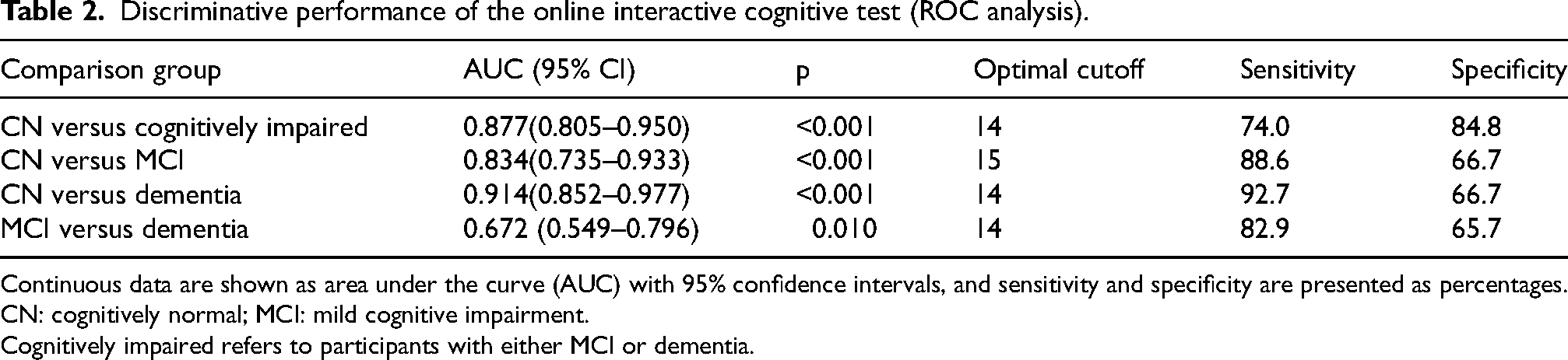
Continuous data are shown as area under the curve (AUC) with 95% confidence intervals, and sensitivity and specificity are presented as percentages.
CN: cognitively normal; MCI: mild cognitive impairment.
Cognitively impaired refers to participants with either MCI or dementia.
Discriminative performance of eye-movement features
Overall task
In the overall task condition, fixation shifts demonstrated discriminative ability in distinguishing cognitively normal older adults from cognitively impaired individuals (including MCI and dementia), with an area under the curve (AUC) of 0.797 (p < 0.001). The highest discriminative performance was observed in the comparison between cognitively normal individuals and those with MCI (AUC = 0.825), with a sensitivity of 88.6% and a specificity of 69.7% (Table 3).
Discriminative validity of fixation shifts and fixation error in the overall task (ROC analysis).
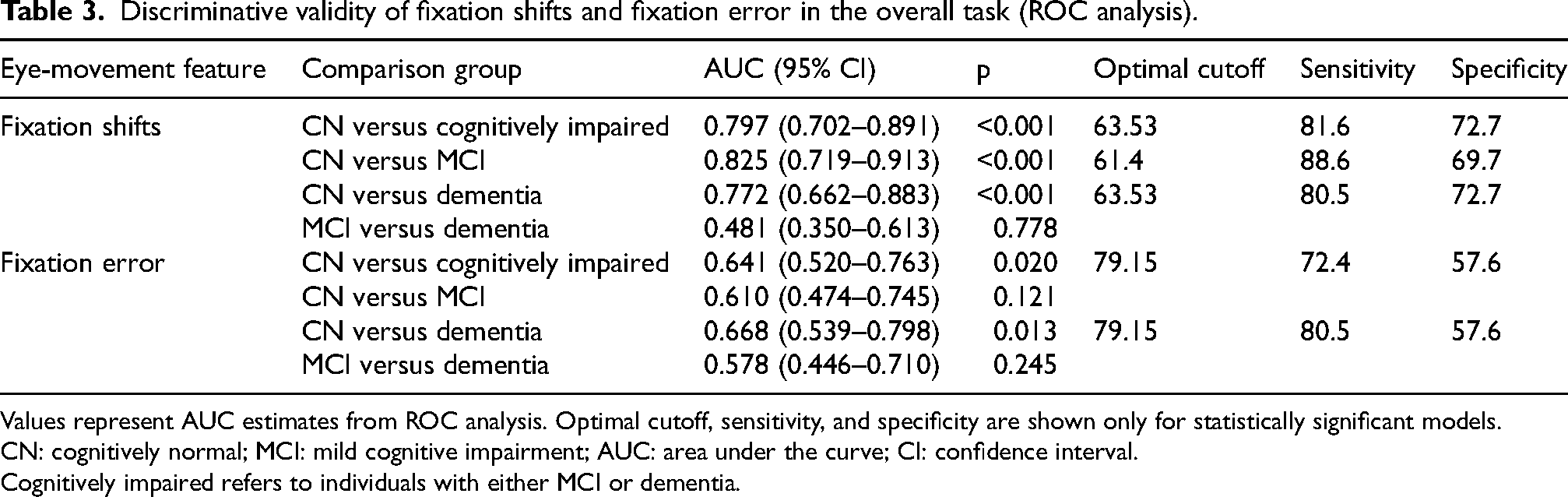
Values represent AUC estimates from ROC analysis. Optimal cutoff, sensitivity, and specificity are shown only for statistically significant models.
CN: cognitively normal; MCI: mild cognitive impairment; AUC: area under the curve; CI: confidence interval.
Cognitively impaired refers to individuals with either MCI or dementia.
Search task
In the search task, fixation shifts continued to discriminate cognitively normal individuals from those with MCI, yielding an AUC of 0.814 (p < 0.001). In addition, gaze deviation showed discriminative ability in distinguishing cognitively normal individuals from cognitively impaired participants, with an AUC of 0.704 (p = 0.001) (Table 4).
Discriminative validity of fixation shifts and fixation error in the search task (ROC analysis).
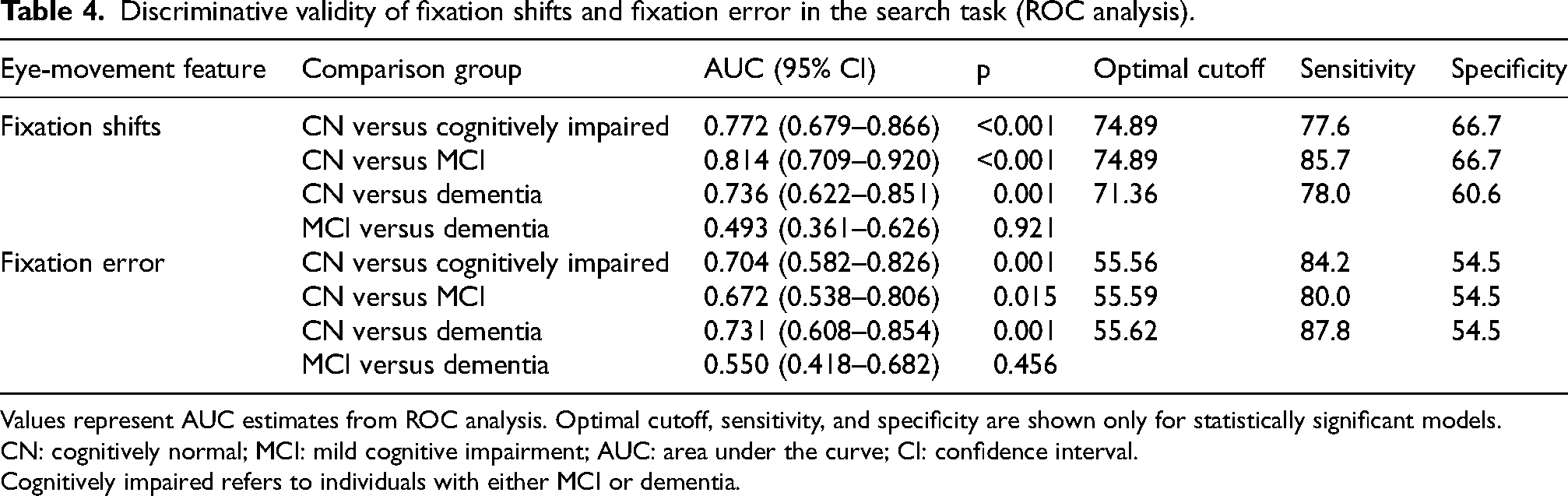
Values represent AUC estimates from ROC analysis. Optimal cutoff, sensitivity, and specificity are shown only for statistically significant models.
CN: cognitively normal; MCI: mild cognitive impairment; AUC: area under the curve; CI: confidence interval.
Cognitively impaired refers to individuals with either MCI or dementia.
Memory task
In the memory task, fixation shifts demonstrated discriminative validity in differentiating cognitively normal individuals from those with MCI, with an AUC of 0.733 (p = 0.001) (Table 5).
Discriminative validity of fixation shifts in the memory task (ROC analysis).

Values represent AUC estimates from ROC analysis.
CN: cognitively normal; MCI: mild cognitive impairment; AUC: area under the curve; CI: confidence interval.
Cognitive processing task
In the cognitive processing task, fixation shifts also differentiated cognitively normal individuals from those with MCI, yielding an AUC of 0.791 (p < 0.001) (Table 6).
Discriminative validity of fixation shifts in the cognitive processing task (ROC analysis).
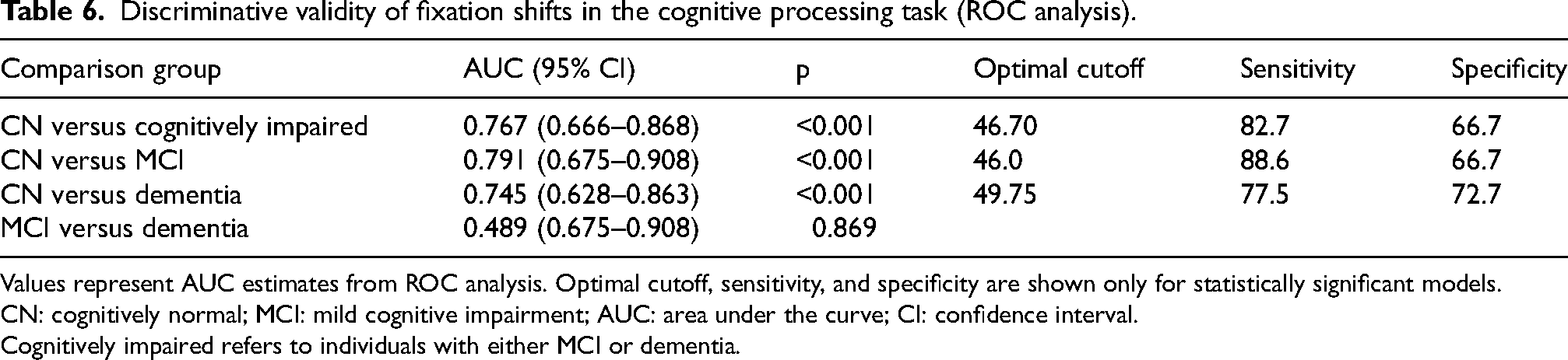
Values represent AUC estimates from ROC analysis. Optimal cutoff, sensitivity, and specificity are shown only for statistically significant models.
CN: cognitively normal; MCI: mild cognitive impairment; AUC: area under the curve; CI: confidence interval.
Cognitively impaired refers to individuals with either MCI or dementia.
Discriminative performance of the combined model integrating the online cognitive test and eye-movement features
The screening performance of the combined model integrating the online interactive cognitive test with eye-movement features across cognitive-status comparisons is presented in Table 7.
Classification performance of the combined online interactive test and eye-movement features across cognitive status groups.
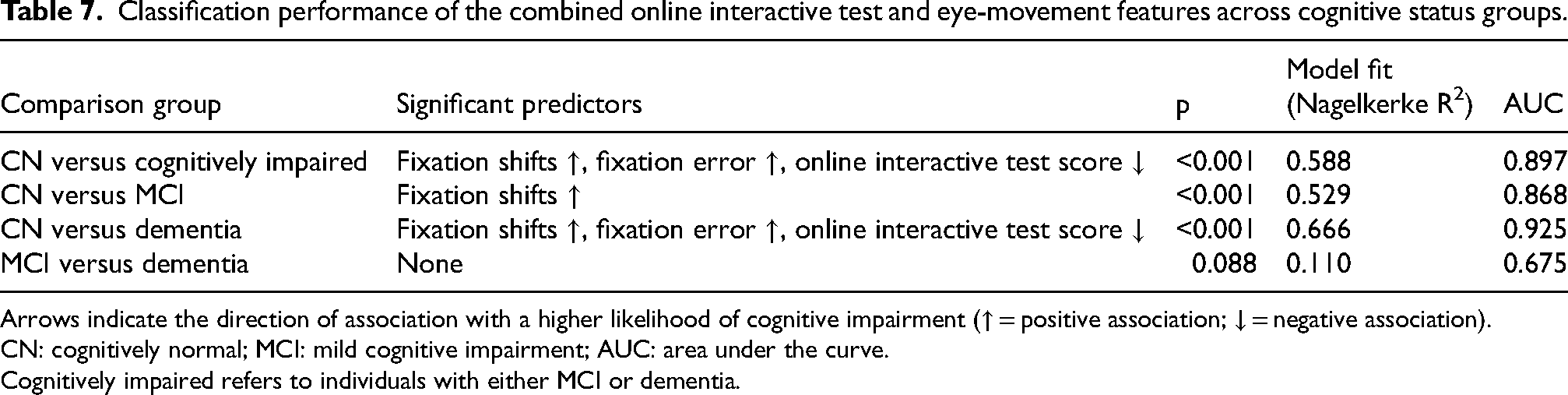
Arrows indicate the direction of association with a higher likelihood of cognitive impairment (↑ = positive association; ↓ = negative association).
CN: cognitively normal; MCI: mild cognitive impairment; AUC: area under the curve.
Cognitively impaired refers to individuals with either MCI or dementia.
Cognitively normal versus cognitively impaired
The overall model was statistically significant (p < 0.001). In logistic regression, fixation shifts (overall task) and gaze deviation (search task) were positively associated with cognitive impairment, whereas higher cognitive test scores were negatively associated. ROC analysis showed AUCs of 0.867, 0.877, and 0.897 for the cognitive-test–only, eye-movement–only, and combined models, respectively.
Cognitively normal versus mild cognitive impairment
This model was statistically significant (p < 0.001). Fixation shifts in the overall task were significantly associated with cognitive status (p = 0.006). AUCs were 0.834 for the cognitive-test–only model, 0.862 for the eye-tracking–only model, and 0.868 for the combined model.
Cognitively normal versus dementia
The model reached significance (p < 0.001). The cognitive test score was negatively associated with cognitive status (p = 0.002). AUCs were 0.914 (cognitive test), 0.864 (eye tracking), and 0.925 (combined).
Mild cognitive impairment versus dementia
This comparison did not reach statistical significance (p = 0.088). AUCs were 0.672, 0.597, and 0.675 for the cognitive-test–only, eye-tracking–only, and combined models, respectively.
Discussion
In this study, we demonstrated that integrating eye-movement measures with an online interactive cognitive task improves sensitivity to early cognitive vulnerability in older adults. The combined multimodal model outperformed single-modality approaches, underscoring the value of complementing conventional outcome-based cognitive performance with process-level eye-movement markers. These findings suggest that eye-movement–derived measures capture subtle alterations in cognitive processing that may not be fully reflected by end-point test scores alone. Importantly, this approach is intended to support psychogeriatric cognitive screening and clinical triage by providing complementary process-level information, rather than to replace comprehensive neuropsychological evaluation or biomarker-based diagnostic procedures.
The online interactive cognitive task alone effectively distinguished cognitively normal older adults from those with cognitive impairment, consistent with prior evidence supporting the utility of computerized cognitive assessments for early cognitive evaluation. 21 However, its reduced discriminative performance in differentiating MCI from dementia suggests that reliance on a single global performance score may be insufficient to capture the heterogeneity and continuum of cognitive impairment in older adults. This finding highlights the limited sensitivity of end-point performance measures to underlying process-level cognitive inefficiencies, particularly during transitional stages of impairment. 22 Importantly, this pattern is likely to be clinically meaningful rather than purely methodological. As cognitive impairment progresses beyond the prodromal stage, overlapping neurodegenerative changes may attenuate the ability of both performance-based scores and process-level markers to further differentiate disease severity. Furthermore, the modest specificity observed here reflects the inherent trade-off in screening tools, which prioritize high sensitivity to minimize the risk of missing early-stage decline. While inter-individual variability in education level or sensory factors may also influence performance, these process-level markers remain highly sensitive to initial cognitive shifts. Accordingly, eye-movement–derived measures appear most informative for early-stage characterization, particularly in distinguishing cognitively normal aging from MCI.
Eye-movement analyses focused on tasks requiring visual search and decision-making, thereby capturing process-level cognitive engagement relevant to attentional control and executive functioning. Among the examined parameters, fixation-shift dynamics emerged as the most sensitive and stable indicator of early cognitive vulnerability, reflecting subtle disruptions in the efficiency and organization of visual exploration during task performance. These alterations likely reflect reduced flexibility in visual–attentional sampling and executive control, cognitive processes supported by frontoparietal networks that have been implicated in prior neuroimaging studies and are known to be vulnerable during early cognitive decline in aging.
In contrast, fixation error appeared to be more strongly influenced by task demands and cognitive load, potentially reflecting later-stage impairments in attentional control and spatial targeting under increased processing demands.23–25 Although fixation error demonstrated discriminative ability in visually demanding search tasks, its performance was less consistent across task types, suggesting greater susceptibility to task demands and cognitive load rather than stable early-stage cognitive vulnerability. Tasks that did not involve explicit visual exploration were therefore excluded to ensure that eye-movement metrics captured meaningful process-level cognitive behavior rather than task-specific or motor-related artifacts.
Importantly, integrating cognitive performance with eye-movement features improved discriminative performance beyond either modality alone, particularly in distinguishing cognitively normal individuals from those with MCI and from cognitively impaired participants overall.26–28 This complementarity highlights the value of combining outcome-based cognitive performance with process-level behavioral indicators to improve sensitivity to early cognitive vulnerability, which may not be fully reflected by end-point test scores alone.
From a clinical perspective, eye-movement–derived process markers offer several advantages. These measures are noninvasive, objective, and relatively independent of language and educational background, addressing key limitations of traditional cognitive assessments. While not intended to replace established instruments, integrating standardized cognitive tasks with concurrent eye-movement recording may augment existing approaches by supporting psychogeriatric assessment, clinical characterization, early risk stratification, and monitoring in outpatient and community-based settings.16,19,29
Future research should prioritize longitudinal validation to determine whether eye-movement–derived process-level measures are associated with cognitive trajectories or predict progression from MCI to dementia. Further optimization of task design and analytic strategies may enhance robustness, interpretability, and scalability in real-world psychogeriatric clinical and research settings. By bridging outcome-based cognitive performance with process-level behavioral assessment, this approach aligns with emerging calls to move beyond total scores toward more mechanistic markers of early AD-related cognitive vulnerability.
Limitations
Several limitations warrant consideration. First, certain components of the online cognitive screening task may have limited sensitivity to the earliest stages of cognitive decline. For example, the naming task primarily employed highly familiar stimuli (e.g., common animals), which may allow individuals with MCI to maintain high accuracy, thereby limiting sensitivity to subtle impairments in early semantic retrieval. In addition, the fixed structure of the visual search paradigm may have constrained variability in eye-movement behavior, potentially reducing sensitivity to subtle process-level inefficiencies. This design may have limited participants’ visual exploration strategies and may partially explain why some eye-movement parameters did not show significant group differences. Future studies may improve sensitivity by incorporating adaptive and difficulty-adjusted task designs. Task complexity could be systematically manipulated—for example, by introducing concurrent working memory demands during visual search, increasing target uncertainty, adding distractors, or implementing multi-target search conditions. Such modifications may enhance variability in eye-movement patterns and improve the detection of early cognitive vulnerability. These limitations are particularly relevant in early-stage conditions, where performance accuracy may remain preserved despite underlying process-level inefficiencies.
Second, cognitively normal participants were younger and more highly educated than those with MCI or dementia. Although eye-movement measures are generally less influenced by educational background than conventional cognitive scores, residual confounding by age and education cannot be fully excluded and should be addressed through age-matched designs or statistical adjustment in future work. Age and education were not included as covariates in the primary ROC analyses, which focused on overall discriminative performance rather than etiologic inference. Future studies incorporating age-matched samples or covariate-adjusted models are warranted to further clarify the independent contribution of eye-movement measures.
Third, participants with severe dementia were not included, limiting generalizability to later disease stages. Finally, the cross-sectional design precludes inference regarding cognitive trajectories or disease progression.
These factors, together with the inherent overlap in cognitive and neurodegenerative processes across early disease stages, particularly between cognitively normal aging and MCI, may contribute to the relatively lower specificity observed in some classification tasks, which is consistent with the intended role of the model as a screening and triage tool that prioritizes sensitivity to early-stage cognitive vulnerability.
Despite these limitations, the present findings provide clinically meaningful proof-of-concept evidence that integrating eye-movement measures into interactive cognitive screening improves sensitivity to early cognitive vulnerability in older adults beyond conventional performance-based scores. This multimodal approach may be particularly relevant for psychogeriatric screening and triage, where subtle alterations in cognitive processing may precede measurable declines in total scores. With further longitudinal validation, such frameworks may support scalable screening, early risk stratification, and monitoring in outpatient and community-based settings, including primary care contexts.
Conclusion
In conclusion, fixation-shift–derived eye-movement metrics, when integrated with computerized cognitive assessment, improve sensitivity to early cognitive vulnerability in older adults by bridging outcome-based performance with process-level behavioral assessment. This complementary approach provides objective insight into cognitive processes that may not be captured by total scores alone. While not intended to replace established instruments, it may augment existing assessment strategies by supporting psychogeriatric screening, early risk stratification, and monitoring in clinical and community-based settings, particularly where access to biomarker-based assessment is limited.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261457344 - Supplemental material for Process-level eye-movement dynamics enhance sensitivity to early Alzheimer's disease-related cognitive vulnerability
Supplemental material, sj-docx-1-alz-10.1177_13872877261457344 for Process-level eye-movement dynamics enhance sensitivity to early Alzheimer's disease-related cognitive vulnerability by Ping-Yu Chen, Wann-Yun Shieh, Li-Cheng Weng, Hsiu-Hsin Tsai, Wei-Xiang Wang and Chia-Yih Liu in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We thank all participants and their families for their time and cooperation. We also acknowledge the assistance of the staff at participating regional hospitals with neurology or geriatric outpatient services, as well as community-based settings providing older adult day care or community support services for their support in participant recruitment and data collection.
Ethical considerations
This study was approved by the Institutional Review Board of Taoyuan General Hospital, Ministry of Health and Welfare, Taiwan (IRB No. TYGH113107).
Consent to participate
The study was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from all participants or their legally authorized representatives prior to participation, and participants with dementia provided assent whenever possible. All data were anonymized and handled confidentially in accordance with institutional regulations.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Science and Technology Council (grant number NSTC 113-2314-B-182-035-MY3) and the Chang Gung Memorial Hospital (grant number BMRP849).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are not publicly available due to ethical and privacy restrictions but are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.