
Abstract
Background
Interleukin-8 (IL-8) exhibits dual roles in Alzheimer's disease (AD), yet how the metabolic milieu of type 2 diabetes mellitus (T2DM) influences its impact in mild cognitive impairment (MCI) remains unclear.
Objective
This study aimed to investigate how T2DM status moderates the longitudinal association between baseline plasma IL-8 levels and AD-related outcomes, including cognitive decline, amyloid-β (Aβ) deposition, and neurodegeneration.
Methods
Data from 373 MCI participants (Alzheimer's Disease Neuroimaging Initiative cohort) were analyzed. Moderation analyses examined the IL-8 × T2DM interaction on cognitive trajectories, amyloid-β (Aβ) accumulation, and regional atrophy, adjusting for key covariates.
Results
In the T2DM group, higher baseline IL-8 was significantly associated with a slower longitudinal increase in Clinical Dementia Rating-Sum of Boxes (p = 0.005), indicating preserved clinical function. Furthermore, elevated IL-8 in the T2DM cohort correlated with lower hippocampal Aβ burden (p = 0.041) and attenuated atrophy rates in the parahippocampal cortex (p = 0.044). In contrast, no significant associations between IL-8 and any AD biomarkers or cognitive trajectories were observed in the non-T2DM group.
Conclusions
This research demonstrates that the role of IL-8 in MCI is “context-dependent,” contingent upon the patient's metabolic state. The author suggests that under chronic metabolic stress, IL-8 may reflect an adaptive immune response that mitigates amyloid pathology and slows neurodegeneration. These results emphasize the necessity of integrating metabolic profiles into the interpretation of neuroinflammatory biomarkers to facilitate personalized therapeutic strategies for AD.
This is a visual representation of the abstract.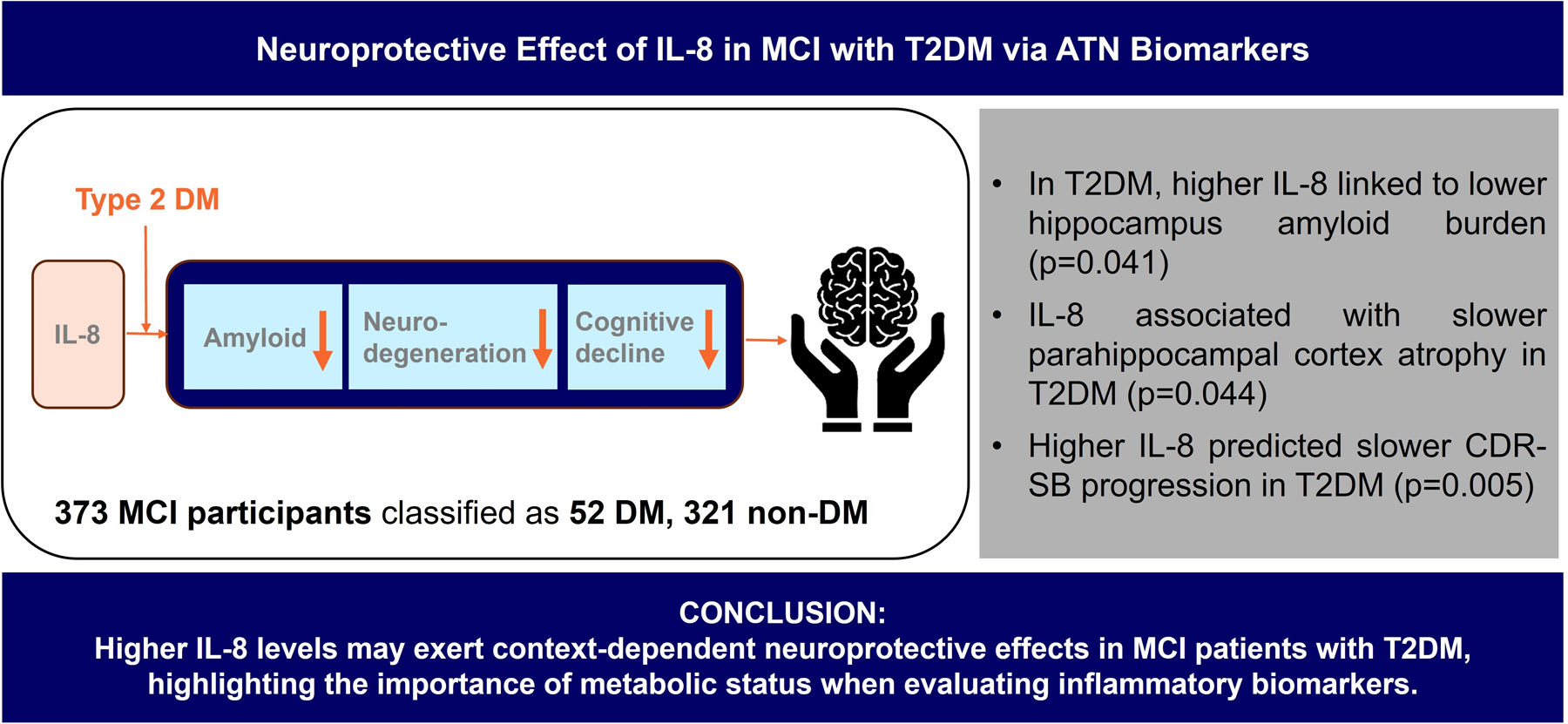
Keywords
Introduction
Interleukin-8 (IL-8), a potent CXC chemokine, serves as a critical mediator of inflammatory responses within the central nervous system. 1 While traditionally characterized as a pro-inflammatory cytokine upregulated by pathological stimuli such as amyloid-β (Aβ) and tumor necrosis factor-α, recent evidence suggests that IL-8 may possess a nuanced, dualistic role in Alzheimer's disease (AD) pathogenesis.2,3 Clinical investigations have yielded heterogeneous results; while some studies report elevated IL-8 in cerebrospinal fluid (CSF) correlating with AD biomarkers, 4 others observe decreased or stable levels in both CSF and peripheral blood. 5 Notably, emerging data indicate that IL-8 may exert neuroprotective effects and support cognitive function during the early stages of AD, particularly when the overall pathological burden remains limited. 6
The progression of AD is increasingly understood through the “Amyloid–Tau–Neurodegeneration (ATN)” framework, 7 wherein type 2 diabetes mellitus (T2DM) acts as a formidable metabolic catalyst. T2DM accelerates this cascade by fostering chronic low-grade inflammation, insulin resistance, and oxidative stress.8,9 The systemic pro-inflammatory environment induced by T2DM likely exacerbates the ATN pathway, further complicating the immune-metabolic interface.10,11 Epidemiological shifts, such as the rising dementia risk associated with early-onset T2DM and poor glycemic control, highlight the urgency of elucidating how metabolic dysfunction influences inflammatory mediators like IL-8.12,13
In the context of metabolic disorders, IL-8 has been identified as a biomarker that promotes insulin resistance by interfering with the Akt signaling pathway.14,15 However, the inconsistent findings in AD research suggest that IL-8 may function as a “context-dependent” modulator rather than a strictly neurotoxic agent. 16 The author posits that in the presence of chronic metabolic stress, such as T2DM, IL-8 may reflect an adaptive or compensatory immune response that differs significantly from its role in metabolically healthy individuals.
Mild cognitive impairment (MCI) represents the critical prodromal stage of AD, where patients exhibit heightened vulnerability to metabolic stressors like T2DM.17,18 Despite the clinical importance of this population, empirical research investigating how IL-8 influences longitudinal cognitive trajectories specifically within the context of T2DM remains insufficient. Therefore, the present study aims to investigate the association between baseline IL-8 levels and longitudinal cognitive changes in patients with MCI. Specifically, the author evaluates the moderating effect of T2DM status to determine how the metabolic milieu governs the relationship between neuroinflammation and clinical progression.
Methods
Data acquisition and participants
Data used in the preparation of this article were obtained from the Alzheimer's Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu). ADNI was launched in 2003 as a public-private partnership, led by Principal Investigator Michael W. Weiner, MD. The primary goal of ADNI has been to test whether serial magnetic resonance imaging (MRI), positron emission tomography (PET), other biological markers, and clinical and neuropsychological assessment can be combined to measure the progression of MCI and early AD. ADNI, which is a large-scale, multicenter, longitudinal study carried out across various sites in the United States and Canada. 19 Detailed information on participant recruitment and eligibility criteria was previously outlined. 20 Eligible participants were scheduled for follow-up visits every 12 to 24 months, with a maximum duration of up to 138 months.
To investigate factors associated with cognitive progression, the analysis was restricted to participants diagnosed with MCI at baseline.21,22 Out of 562 individuals with baseline diabetes information and longitudinal records, 189 were excluded because they were cognitively normal, had dementia, or lacked essential baseline information. The final sample included 373 participants with MCI, and 83 of them had amyloid PET or structural MRI data available for analysis.
Every procedure was conducted in accordance with the ethical guidelines established by the Institutional Review Boards at each participating center, and written consent was obtained from all participants or their legal representatives.
Selection of inflammatory biomarker
IL-8 was preselected as the primary biomarker for analysis based on prior evidence suggesting its involvement in both metabolic dysregulation and neuroinflammatory processes.23,24 In particular, IL-8 mediates immune cell recruitment and vascular responses, which are recognized as shared pathophysiological mechanisms underlying T2DM and cognitive decline. 25 In addition, considering the data availability and the proportion of missing values among other cytokines within the ADNI cohort, IL-8 was identified as the biomarker with the most suitable data quality and completeness for examining cognitive changes according to T2DM status.
Classification of baseline cognitive status
All participants included in this study met criteria for MCI (n = 373) at baseline. Classification was based on the Clinical Dementia Rating-Sum of Boxes (CDR-SB), requiring a total score of ≥0.5 and a memory box score of at least 0.5. 20 Additionally, Mini-Mental State Examination (MMSE) scores ranged from 24–30. The memory criterion, based on delayed recall of a paragraph from the Logical Memory II subscale of the Wechsler Memory Scale-Revised, had cutoff scores adjusted for education level: ≤8 for 16 years of education, ≤4 for 8–15 years, and ≤2 for 0–7 years.
Classification of baseline DM status
DM status was defined according to the American Diabetes Association diagnostic criteria. 26 Participants were classified as having DM (n = 52) if they met one of the following criteria: (1) fasting plasma glucose level of 126 mg/dL or higher, (2) a self-reported or documented diagnosis of diabetes, or (3) current use of antidiabetic medication. Relevant data were extracted from ADNI clinical files, including “ADSXLIST.csv,” “RECCMEDS.csv,” and “RECMHIST.csv.” Participants who didn’t meet these criteria were categorized as non-diabetic (n = 321).
PET and structural brain MRI analysis
Amyloid PET scans were conducted every 12–24 months. Amyloid burden was measured using standardized uptake value ratios (SUVRs) derived from [18F] florbetapir PET scans, with the whole cerebellum as the reference region. Amyloid PET imaging data were obtained from the ADNI files “UCBERKELEY_AMY_6MM.csv.”
MRI scans were conducted annually. Structural MRI data were preprocessed using Freesurfer version 7.1.1 for cortical and subcortical segmentation and parcellation. Brain volumetric measures were obtained from the same dataset used for amyloid PET imaging. The baseline and follow-up MRI scans were aligned with the PET acquisitions that happened closest in time to ensure alignment.
Regions of interest (ROIs) included the entorhinal cortex, hippocampus, parahippocampal cortex, and middle temporal cortex. The entorhinal cortex and hippocampus are among the earliest regions to exhibit AD-related changes, such as amyloid accumulation and tau pathology, both are closely linked to memory decline and early cognitive deficits.27,28 As the disease advances, atrophy typically extends to the parahippocampal and middle temporal regions, which are involved in higher-order cognitive processing and memory.29–31 These regional changes are widely recognized as imaging biomarkers indicative of AD progression.32–35
Researchers acquired and preprocessed all imaging data at the Helen Wills Neuroscience Institute, University of California, Berkeley, and Lawrence Berkeley National Laboratory.
Cognitive function assessment
Cognitive performance was assessed using two standardized tools: CDR-SB 36 and MMSE. 37 These evaluations were conducted at baseline and repeated at regular 6 to 12-month intervals thereafter.
Other clinical variables
Hypertension and apolipoprotein E (APOE) ε4 allele status were included as covariates due to their established associations with both DM and AD.38,39 Hypertension was defined by the presence of any among: current use of antihypertensive medication, systolic blood pressure ≥140 mmHg, or diastolic blood pressure ≥90 mmHg. APOE genotype information was obtained from ADNI database, which provides detailed protocols for genotyping procedures. 40 Participants’ educational attainment, known to be linked with cognitive decline, was included as a covariate in the analyses.
Statistical analysis
Baseline demographic and clinical variables were compared between groups using independent t-tests for continuous variables and chi-square tests for categorical variables, to identify differences in participants with and without DM.
To examine whether DM moderates the relationships among AD biomarkers within the ATN framework, moderation analyses were conducted using Hayes’ methodology. 41 For all biomarker and cognitive measures, rates of change were computed monthly to account for individual variation in follow-up duration.
Three moderation models were tested:
Our first model examined whether DM status influenced the relationship between IL-8 levels and cognitive decline, using changes in CDR-SB and MMSE scores as the outcome measures. The second model looked at whether having DM affected the relationship between IL-8 levels and amyloid, using amyloid SUVR as the outcome variable. The third model evaluated how DM affects the connection between IL-8 levels and neurodegeneration, using ROI volume as the outcome measures.
Statistical models were adjusted for potential confounding factors, including age, sex, years of education, hypertension status, and the number of APOE ε4 alleles. We used IBM SPSS Statistics software version 27.0 (IBM Corp., Armonk, New York) to perform the analyses, setting statistical significance at p < 0.05. For moderation analyses, we used PROCESS macro version 4.3.
Results
Baseline characteristics of participants
The baseline characteristics of the study participants are presented in Table 1. No statistically significant differences were observed between the DM and non-DM groups regarding baseline amyloid levels, ROI volumes, CDR-SB scores, or MMSE scores.
Clinical, brain, and cognitive characteristics of the MCI group at baseline.

Data are presented as mean (standard deviation) for continuous variables and n (%) for categorical variables. The quantification of amyloid PET was conducted by measuring the SUVRs of florbetapir.
Data not available for all participants (10 DM and 73 without DM). The analysis was adjusted for age, sex, years of education, hypertension, and the number of APOE ε4 alleles. APOE: apolipoprotein E; CDR-SB: clinical dementia rating-sum of boxes; DM: diabetes mellitus; MCI: mild cognitive impairment; MMSE: Mini-Mental Status Examination; nDM: non-diabetes mellitus; PET: positron emission tomography.
Moderating effect of DM on the relationship between IL-8 and cognitive change
The moderating effect of DM status on the relationship between IL-8 levels and clinical severity was analyzed using the CDR-SB score as the primary outcome. In participants with DM, higher IL-8 levels were significantly associated with a slower monthly rate of change in CDR-SB (ΔCDR-SB/month), indicating a slower clinical progression (p = 0.005; Figure 1). In contrast, no significant moderation effect of DM was observed in the relationship between IL-8 and baseline CDR-SB scores (Supplemental Table 1).

Moderating effect of DM on the relationship between IL-8 and longitudinal changes in CDR-SB.
Furthermore, DM status did not significantly influence the relationship between IL-8 levels and the monthly rate of change in MMSE or baseline MMSE scores (all p > 0.05; Supplemental Figure 1, Supplemental Table 2).
Moderating effect of DM on the relationship between IL-8 and amyloid accumulation
At baseline, higher IL-8 levels were associated with lower amyloid accumulation in the hippocampus among MCI participants with DM (p = 0.041). Specifically, while the amyloid SUVR decreased by 0.002 units in the non-DM group (Figure 2), a more substantial decrease of 0.02 units was observed in the DM group (Figure 2).

Moderating effect of DM on the relationship between IL-8 and amyloid levels at baseline in the hippocampus.
However, no significant moderation effect of DM on the relationship between IL-8 and amyloid SUVR was found in other ROI regions at either baseline or during the follow-up period (Supplemental Tables 3 and 4).
Moderating effect of DM on the relationship between IL-8 and ROI brain volume
At baseline, higher IL-8 levels were correlated with smaller hippocampal volumes in MCI participants with DM (p = 0.005). Specifically, hippocampal volume decreased by 0.01 units in the non-DM group (Figure 3), compared to a larger decrease of 0.17 units in the DM group (Figure 3). No significant DM moderation was found in other brain regions (Supplemental Table 5).

Moderating effect of DM on the relationship between IL-8 and volume at baseline in the hippocampus.
Regarding the longitudinal changes in ROI volumes, a significant interaction between IL-8 levels and DM status was observed. Specifically, in individuals with DM, higher IL-8 levels were significantly associated with a slower rate of atrophy in the parahippocampal cortex (p = 0.044; Figure 4). In the non-DM group, no significant association was found between IL-8 levels and brain volume changes (Figure 4). No significant DM effect was observed for volume changes in other ROI regions (Supplemental Table 6).

Moderating effect of DM on the relationship between IL-8 and longitudinal changes in parahippocampal cortex volume.
Discussion
The present study demonstrates that the metabolic context of T2DM significantly modulates the association between the pro-inflammatory chemokine IL-8 and markers of AD pathology and cognitive decline in individuals with MCI. The central finding of this research is that the clinical and pathological significance of IL-8 is highly context-dependent, contingent upon the patient's underlying metabolic state. Specifically, in MCI patients with T2DM, higher baseline IL-8 levels were associated with a slower rate of clinical progression (CDR-SB), reduced hippocampal Aβ burden, and attenuated neurodegeneration in the parahippocampal cortex.
Prior literature has frequently reported elevated circulating IL-8 levels in patients with T2DM compared to non-DM. 14 However, it is noteworthy that in the current cohort, no significant difference in baseline IL-8 concentrations was observed between the T2DM and non-DM groups. The author suggests that because the study population consisted entirely of MCI patients, who likely exhibit systemic inflammatory activation regardless of metabolic factors, the differences in cognitive trajectories cannot be explained by IL-8 absolute concentrations alone. Instead, the results indicate that T2DM status fundamentally moderates the relationship between IL-8 and cognitive outcomes, suggesting a shift in the functional role of IL-8 signaling based on the metabolic milieu.
The observation that higher IL-8 levels correlate with slower cognitive decline in the presence of T2DM is intriguing, as IL-8 is traditionally characterized as a pro-inflammatory mediator of neurotoxicity. 6 However, these results align with emerging evidence suggesting that IL-8 may exert a dual role, shifting from neurotoxic to neuroprotective depending on the pathological stage and biological background.42,43 Within the ATN framework, T2DM acts as a potent metabolic stressor promoting chronic low-grade inflammation. 10 In this specific environment, the author posits that elevated IL-8 may represent a compensatory immune activation or adaptive inflammatory modulation rather than a purely damaging signal.44–46
The present results are clinically consistent with prior observations showing that higher IL-8 levels correlate with lower amyloid PET SUVR, specifically within the T2DM group. This alignment reinforces the role of IL-8 in the modulation of Aβ levels in the diabetic brain.2,45
Furthermore, given the prevalence of microvascular dysfunction and blood-brain barrier impairment in T2DM, results align with established reports regarding IL-8's involvement in maintaining neurovascular integrity and activating antioxidant pathways.16,25,47,48 These parallels suggest that IL-8 acts as a protective factor in this study population, potentially contributing to the deceleration of cognitive deterioration in diabetic patients.
A discrepancy was observed where higher IL-8 levels were associated with smaller baseline hippocampal volumes in the T2DM group, despite predicting slower longitudinal decline. This suggests that elevated IL-8 may initially reflect pre-existing inflammatory damage or structural vulnerability. 49 However, the lack of association with further longitudinal hippocampal atrophy, coupled with slower parahippocampal thinning, suggests a temporal shift in IL-8 function. While early inflammatory responses may contribute to tissue loss, in the prodromal stage of MCI, where neuroplasticity is partially preserved, subsequent IL-8 signaling may pivot toward homeostatic maintenance. 6
Notably, no significant associations between IL-8 and AD biomarkers were observed in the non-DM group. This underscores that the functional impact of peripheral inflammatory markers is dormant or negligible in the absence of metabolic stress. The synergy between T2DM and IL-8 highlights the necessity of considering “metabolic-inflammatory crosstalk” when evaluating AD risk.50,51 In MCI patients, who are at a critical transition point to AD, the immune system's response to metabolic dysregulation appears to be a key determinant of the cognitive trajectory.
Strengths and limitations
From a clinical perspective, these findings suggest that IL-8 could serve as a precision biomarker for predicting disease progression, but only when interpreted alongside a patient's metabolic profile. It further implies that anti-inflammatory therapeutic strategies should be personalized; a “one-size-fits-all” approach to suppressing cytokines like IL-8 might inadvertently eliminate protective compensatory responses in certain metabolic subgroups.
Despite these insights, several limitations warrant caution. First, as an observational study, the identified associations do not prove a direct causal link between IL-8 and neuroprotection. Second, the analysis was restricted to IL-8 based on a hypothesis-driven approach and data availability.23,24,52 While IL-8 plays a unique role in immune cell recruitment and vascular signaling, it remains unclear whether these findings reflect a specific IL-8 pathway or a broader inflammatory signature. Future studies utilizing a wider panel of cytokines are needed to map the full inflammatory landscape. Third, the absence of longitudinal tau PET data limits the ability to explain baseline hippocampal atrophy within the full ATN framework. 7 Fourth, the study focused exclusively on MCI patients to investigate progression. Future research should include cognitively normal individuals with T2DM to determine if this IL-8-mediated modulation begins during the preclinical stages of AD. Finally, the ADNI cohort primarily consists of North American populations, necessitating validation in more ethnically diverse cohorts to ensure the generalizability of these metabolic-inflammatory interactions.
Conclusion
In conclusion, IL-8 exhibits a context-dependent property in the progression of MCI. In the presence of T2DM, IL-8 appears to be associated with a more favorable cognitive trajectory and reduced amyloid burden, possibly reflecting an adaptive response to chronic metabolic stress. This study emphasizes that the interplay between systemic metabolism and neuroinflammation is a critical factor in the heterogeneous progression of AD.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261457565 - Supplemental material for Metabolic context modulates neuroinflammation: Type 2 diabetes mellitus moderates the association of interleukin-8 with amyloid pathology and cognitive decline in mild cognitive impairment
Supplemental material, sj-docx-1-alz-10.1177_13872877261457565 for Metabolic context modulates neuroinflammation: Type 2 diabetes mellitus moderates the association of interleukin-8 with amyloid pathology and cognitive decline in mild cognitive impairment by Eun Woo Kim and in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
Data collection and sharing for the Alzheimer's Disease Neuroimaging Initiative (ADNI) is funded by the National Institute on Aging (National Institutes of Health Grant U19AG024904). The grantee organization is the Northern California Institute for Research and Education. In the past, ADNI has also received funding from the National Institute of Biomedical Imaging and Bioengineering, the Canadian Institutes of Health Research, and private sector contributions through the Foundation for the National Institutes of Health (FNIH) including generous contributions from the following: AbbVie, Alzheimer's Association; Alzheimer's Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics.
Ethical considerations
All data used in this study were obtained from the Alzheimer's Disease Neuroimaging Initiative (ADNI). The ADNI study was approved by the IRB or Research Ethics Board (REB) at each participating site, in accordance with the Declaration of Helsinki.
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.