
Abstract
Background
While chronological age is a major but non-specific risk factor for dementia, measures of biological age based on physiological biomarkers may more accurately reflect systemic aging.
Objective
We aimed to assess the association between a Gompertz law-based biological age (Light BioAge) and incident dementia in a national cohort of middle-aged and older adults in China, and to evaluate the potential modifying role of lifestyle.
Methods
We conducted a longitudinal analysis of 5641 participants (≥45 years) from China Health and Retirement Longitudinal Study. Light BioAge was computed at baseline (2011) using a validated algorithm incorporating chronological age, serum creatinine, fasting glucose, and high-sensitivity C-reactive protein. Dementia in 2018 was determined via cognitive tests, informant reports, and functional assessment. Logistic regression models were used to estimate odds ratios (ORs).
Results
During the follow-up, 788 (13.97%) participants were identified as having dementia. Each 1-year increment in Light BioAge was associated with 4% higher risk of dementia (OR 1.04, 95% CI 1.03–1.05). Compared to low BioAge, participants with high BioAge had a more than two-fold higher risk of dementia (OR 2.38, 95% CI 1.85–3.04). This association persisted across strata of favorable and unfavorable lifestyles. Joint exposure analysis revealed that individuals with both high BioAge and an unfavorable lifestyle faced the highest risk (OR 2.96, 95% CI 2.05–4.27).
Conclusions
Accelerated biological aging, quantified by Light BioAge, is a robust independent risk factor for dementia. Favorable lifestyle interventions offer potential strategies. However, findings require caution given the observational design and non-clinical dementia measure.
Introduction
Dementia has emerged as a critical global public health priority, with prevalence rising rapidly alongside population aging. 1 In China alone, the burden of dementia is projected to increase substantially, placing immense strain on families and the healthcare system. 2 While chronological age is the most established risk factor for dementia, 3 it is an imperfect metric for quantifying the physiological decline that precipitates neurodegeneration. 4 Individuals of the same chronological age often exhibit vastly different trajectories of health and functional capacity, suggesting that biological age—a measure of an individual's accumulated physiological damage—may be a more accurate predictor of dementia risk. 5
Recent studies have led to the development of various “aging clocks” based on DNA methylation, proteomics, or clinical biomarkers.6–10 Studies utilizing these measures have consistently demonstrated that accelerated biological aging is associated with adverse health outcomes, including mortality and frailty.11–13 While studies utilizing these measures have demonstrated that accelerated biological aging is associated with adverse health outcomes, many existing omics-based clocks show inconsistent predictive utility across different populations and rely on expensive technologies, limiting their utility in large-scale population screening or low-resource settings. The Gompertz law-based biological age (GOLD BioAge, or “Light BioAge”) offers a pragmatic alternative. Constructed from widely available clinical biomarkers—fasting glucose, C-reactive protein (CRP), and creatinine—Light BioAge captures key domains of metabolic, inflammatory, and renal dysfunction. 12
Despite its potential, the specific association between Light BioAge and risk of dementia remains underexplored, particularly within the Chinese population. Furthermore, the extent to which modifiable lifestyle factors, such as smoking, alcohol consumption, and social engagement, might mitigate or exacerbate the risk posed by accelerated biological aging is not well understood. 14 Understanding this interplay is crucial for designing targeted preventive interventions.
Therefore, this study aimed to: (1) investigate the longitudinal association between Light BioAge and the risk of subsequent dementia in a nationally representative cohort of middle-aged and older Chinese adults; and (2) examine the joint effects and potential interactions between Light BioAge and lifestyle behaviors on dementia risk.
Methods
Study design and participants
The current study utilized data from the China Health and Retirement Longitudinal Study (CHARLS), an ongoing, nationally representative survey designed to monitor the health and aging progression of Chinese residents aged 45 and older. 15 Launched in 2011, CHARLS employs a multistage, stratified probability-proportionate-to-size sampling strategy, covering 450 villages and neighborhoods across 150 counties to ensure the sample accurately reflects the national population. 15 Follow-up assessments are conducted biennially using face-to-face computer-assisted personal interviews. The detailed study protocol and data availability have been described elsewhere. The Biomedical Ethics Review Committee of Peking University approved the study (IRB00001052-11015), and all participants provided informed consent.
A total of 17,707 participants were enrolled in the baseline survey (Wave 1, 2011). For the current analysis, we applied strict exclusion criteria to ensure data quality and the validity of the study. First, 6100 participants were excluded due to missing data on age or key biological indicators (creatinine, glucose, or C-reactive protein), and 739 participants were excluded due to missing baseline cognitive function data. Subsequently, to establish a dementia-free baseline cohort, we excluded 383 participants who reported brain diseases related to cognitive impairment and 499 participants suspected of having dementia (defined as the lowest 5% of global cognitive function scores) at baseline. After further excluding participants without dementia diagnosis data in the follow-up survey (Wave 4, 2018), the final analytical sample comprised 5641 participants. The detailed selection process is illustrated in Figure 1.
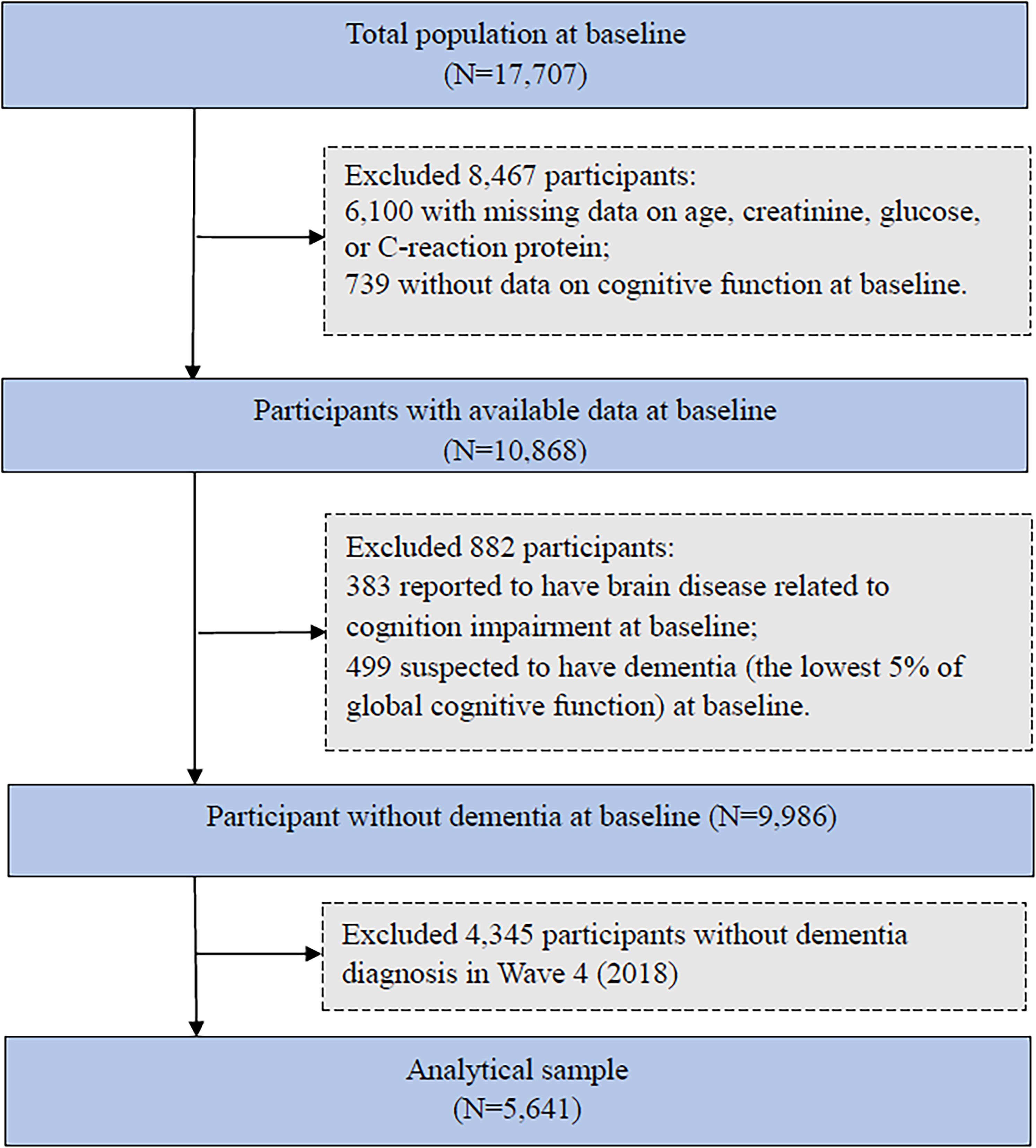
Flowchart of the study population.
Data collection
Standardized questionnaires were administered by trained interviewers through face-to-face interviews to obtain information on sociodemographic characteristics, lifestyle behaviors, and health status. Anthropometric data and blood samples were collected by professional medical staff following standard protocols. 15
Demographic variables included age, sex, place of residence (urban or rural), and marital status (categorized as married/cohabitating or other). Educational attainment was classified into three levels: no formal education, middle school and below, and high school and above. Body mass index (BMI) was calculated based on measured height and weight (kg/m 2 ) and stratified into underweight (<18.5), normal weight (18.5–24.0), overweight (24.0–28.0), and obesity (≥28.0). Lifestyle behaviors assessed included smoking status (never, former, or current), alcohol consumption (drinker or non-drinker), and social activity (classified as active or inactive based on participation in the month preceding the interview). We assigned a value of 1 to each unhealthy behavior (current or former smoking, alcohol consumption, and social inactivity) and 0 to their healthy counterparts, calculating the total score by summing these values. The aggregate lifestyle score ranged from 0 to 3. To stratified analysis, participants were categorized into two groups: the favorable lifestyle group (score 0–1) and the unfavorable lifestyle group (score 2–3).
Chronic conditions were identified through self-reported physician diagnoses, medication usage, or clinical measurements. Hypertension was defined as a self-reported history, use of antihypertensive medication, or measured blood pressure ≥140/90 mmHg. Diabetes was ascertained by a history of diagnosis, use of glucose-lowering drugs, fasting blood glucose ≥126 mg/dL, or HbA1c ≥ 6.5%. Cardiovascular disease (CVD) was defined as having a history of heart disease (including heart attack, angina, or heart failure) or stroke. Dyslipidemia was identified based on self-reported diagnosis, treatment, or abnormal blood lipid levels.
The baseline cognition score was determined through a validated face-to-face assessment covering three domains: orientation, episodic memory, and executive function. Consistent with previous studies based on CHARLS, the global cognition score was calculated as the sum of these components, ranging from 0 to 21, with higher scores reflecting better cognitive function. 16
Assessment of Light BioAge
Light BioAge was derived using the Gompertz Law-Based Biological Age (GOLD BioAge) algorithm, a validated method for quantifying biological aging. 12 This composite indicator integrates chronological age with three physiological biomarkers—serum creatinine, fasting glucose, and C-reactive protein (CRP)—to reflect metabolic and inflammatory status. The calculation followed the specific equation: Age + 8.3313 * Creatinine + 0.8270 * Glucose + 5.7305 * lnCRP - 13.5298.
In this model, age is measured in years, creatinine and CRP in mg/dL, and glucose in mmol/L, with CRP values undergoing natural log-transformation. Higher scores indicate an accelerated biological aging process. For the analysis, participants were stratified into low, moderate, and high groups based on the tertiles of the Light BioAge distribution.
Assessment of dementia
The identification of dementia in this study followed a composite protocol aligned with the established scoring thresholds of the English Longitudinal Study of Ageing (ELSA). 17 Specifically, a person's diagnosis of dementia was based on three subjects: (1) objective cognitive performance (measurement tools were used by interviewers at the subject's home); (2) informant observations (people who know the subjects very well and interact with them frequently, typically relatives, guardians, or neighbors); and (3) the subject's Activity of Daily Living (ADL) scale. The scores of the results of these three items determine the diagnosis for probable dementia. Given that the comprehensive data required for this multi-dimensional evaluation were exclusively collected in the 2018 survey, the definition and analysis of dementia cases were restricted to Wave 4. Because precise time-to-event data was unavailable prior to this wave, logistic regression was selected over time-to-event modeling (e.g., Cox regression) to appropriately analyze the odds of prevalent dementia at this specific time point.
Statistical analysis
Baseline characteristics of the study population across different levels of Light BioAge (low, moderate, and high) were compared using chi-square tests for categorical variables and one-way analysis of variance (ANOVA) for continuous variables. Continuous data were summarized as means ± standard deviations (SD), while categorical data were reported as frequencies and percentages.
Logistic regression models were employed to estimate odds ratios (ORs) and 95% confidence intervals (CIs) to evaluate the association between Light BioAge (analyzed both as a continuous variable and categorized into tertiles: low, moderate, and high) and the risk of dementia. Two sets of models were constructed: Model 1 was adjusted for sex and education; Model 2 was further adjusted for marital status, residence, BMI, smoking status, alcohol drinking, social activity, hypertension, diabetes, cardiovascular disease, and dyslipidemia. To investigate potential modifiers, stratified analyses were performed based on lifestyle profiles (favorable versus unfavorable).
Furthermore, the joint effects of Light BioAge and lifestyle on the risk of dementia were assessed using dummy variables representing combined exposure categories. We also examined the additive interaction between Light BioAge and lifestyle by calculating the relative excess risk due to interaction (RERI), the attributable proportion due to interaction (AP), and the synergy index (S).
Sensitivity analyses were carried out to verify the robustness of the primary findings. First, we additionally controlled for the baseline cognition score to rule out reverse causality. Second, to address potential bias caused by missing data, multiple imputation by chained equations (MICE) was performed to generate 10 imputed datasets, and the results were pooled according to Rubin's rules. A two-sided p < 0.05 was considered statistically significant. All statistical analyses were performed using Stata SE 16.0 (Stata Corp, College Station, TX).
Results
Characteristics of the study population
Table 1 summarizes the baseline characteristics of the study population according to tertiles of Light BioAge. Compared to participants with low BioAge, those with high BioAge were significantly older and more likely to be male. They were less likely to be married or reside in rural areas, and generally had lower educational attainment. In terms of health status and lifestyle, participants in the high BioAge group exhibited a higher mean BMI and were more likely to be current or former smokers.; however, they were less likely to be alcohol drinkers. Furthermore, they had a significantly higher prevalence of comorbidities, including hypertension, diabetes, and CVD, along with lower baseline cognition scores.
Characteristics of the study population by different levels of Light BioAge (N = 5641).
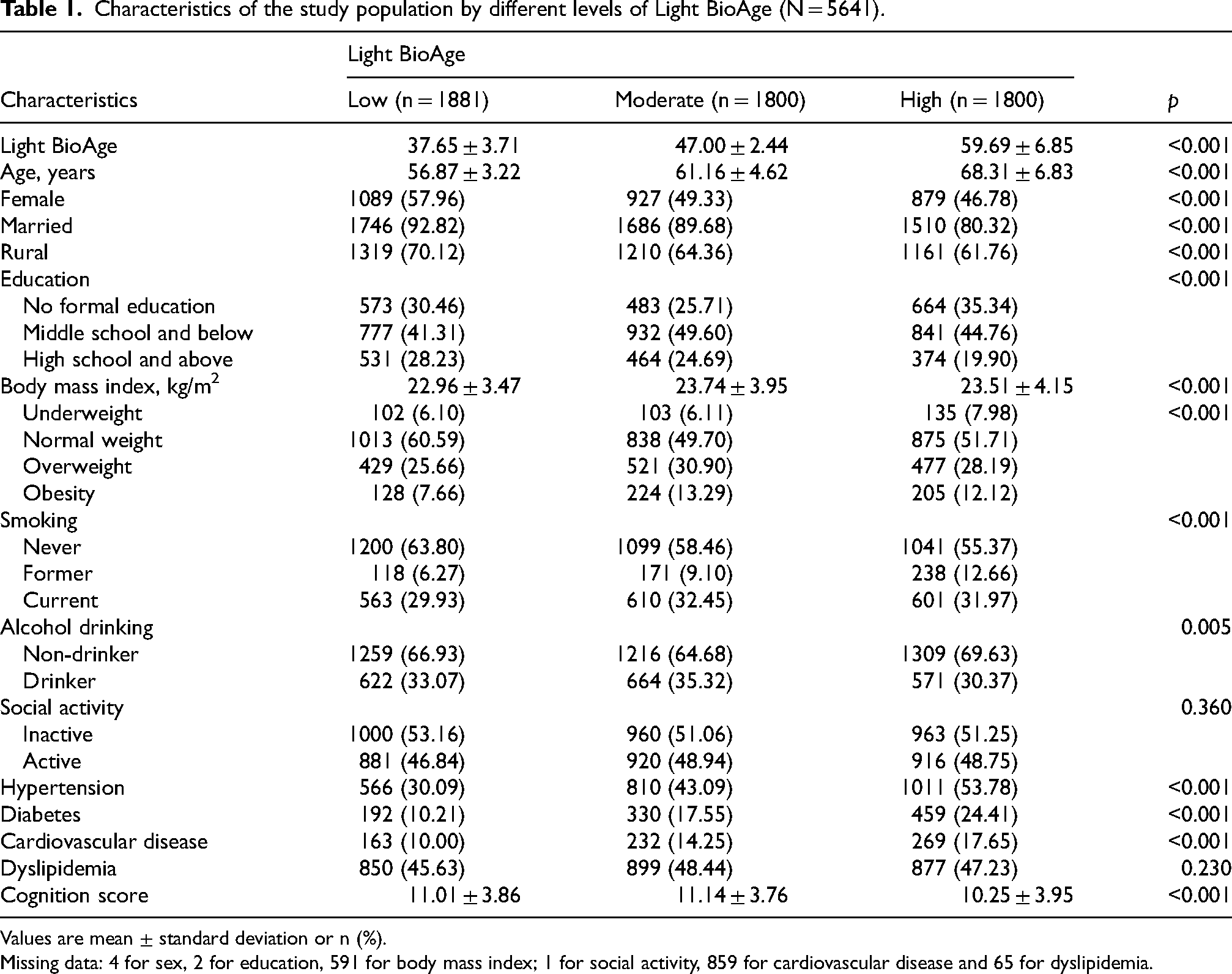
Values are mean ± standard deviation or n (%).
Missing data: 4 for sex, 2 for education, 591 for body mass index; 1 for social activity, 859 for cardiovascular disease and 65 for dyslipidemia.
Association between Light BioAge and dementia
During the follow-up period, 788 (13.97%) of the 5641 participants were diagnosed with dementia. In fully-adjusted models (Table 2), older Light BioAge was significantly associated with a higher risk of dementia. When analyzed as a continuous variable, each 1-year increment in Light BioAge was associated with a 4% higher risk of dementia (OR 1.04, 95% CI 1.03–1.05), indicating a dose-response relationship. Regarding categorical levels, compared with participants with low BioAge, those with moderate and high showed a significantly higher risk (OR 1.34 [1.04–1.73] for moderate and 2.38 [1.85–3.04] for high).
Odds ratios (ORs) and 95% confidence intervals (CIs) for the association between Light BioAge and subsequent dementia.
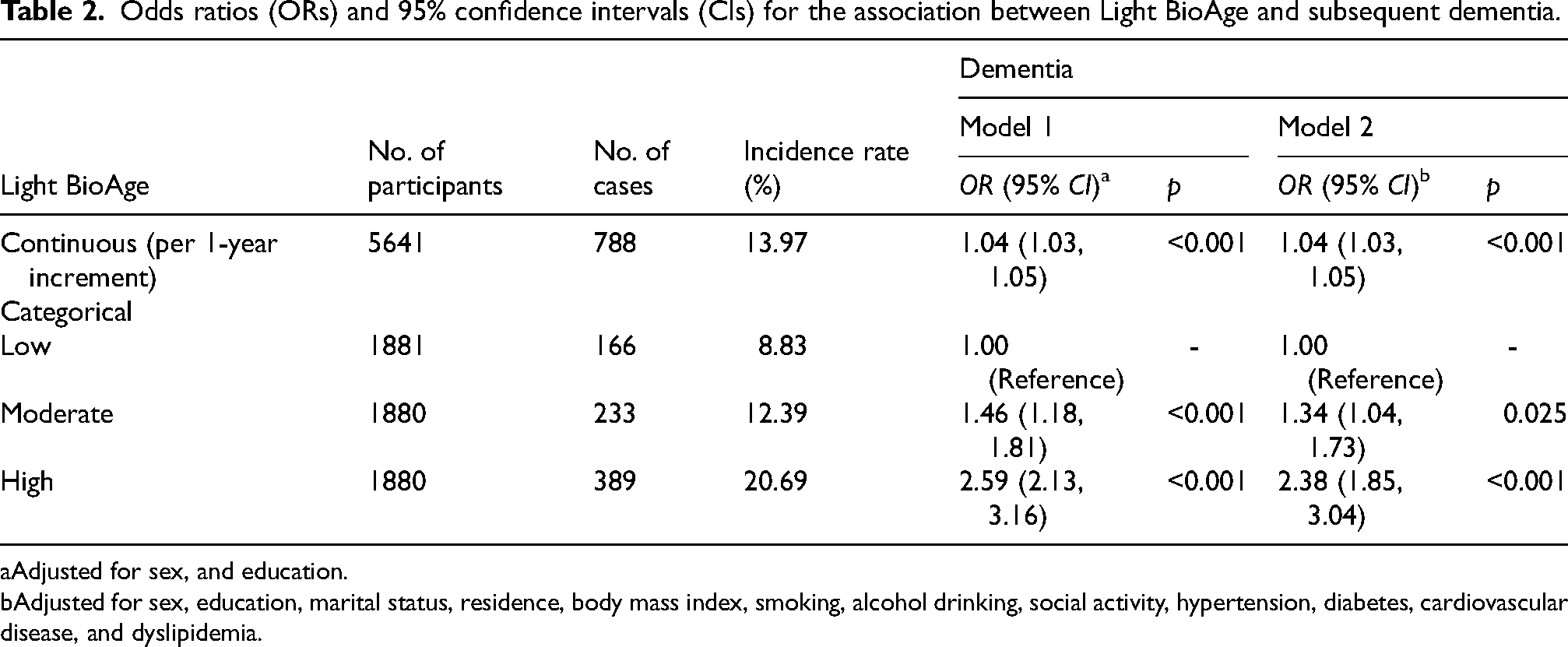
Adjusted for sex, and education.
Adjusted for sex, education, marital status, residence, body mass index, smoking, alcohol drinking, social activity, hypertension, diabetes, cardiovascular disease, and dyslipidemia.
Role of lifestyle
A higher lifestyle score was associated with an increased risk of dementia (Supplemental Table 1). After stratification by lifestyle status (Table 3), the association between Light BioAge and dementia consistent across lifestyle status. The OR (95% CI) of dementia risk for high Light BioAge was 2.32 (1.70, 3.15) and 2.57 (1.69, 3.93) among participants with favorable and unfavorable lifestyles, respectively. The interaction between Light BioAge and lifestyle on the multiplicative scale was not statistically significant (p for interaction>0.05).
Odds ratios (ORs) and 95% confidence intervals (CIs) for the association between Light BioAge and subsequent dementia: stratified by lifestyle.
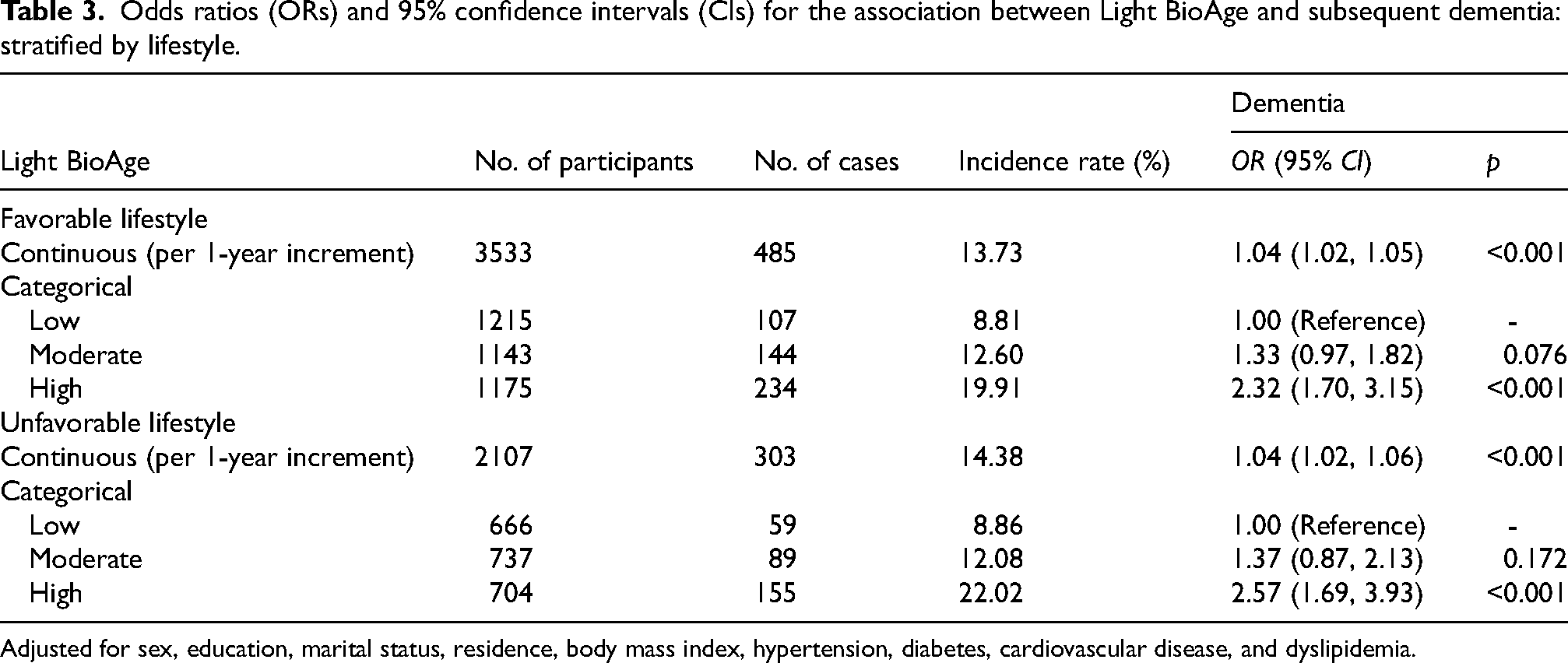
Adjusted for sex, education, marital status, residence, body mass index, hypertension, diabetes, cardiovascular disease, and dyslipidemia.
In the joint-effect analysis (Table 4), compared to participants with both low Light BioAge and a favorable lifestyle, the OR (95% CI) for dementia risk was 1.53 (1.03, 2.28) for those with low BioAge and an unfavorable lifestyle, and peaked at 2.96 (2.05, 4.27) for those with high BioAge and an unfavorable lifestyle. However, the additive interaction was not statistically significant (all p > 0.05). These findings suggest that the association between accelerated biological aging and dementia is robust, and adherence to a favorable lifestyle may not be sufficient to fully offset the elevated risk associated with older Light BioAge.
Joint exposure of light BioAge and lifestyle on the risk of dementia.
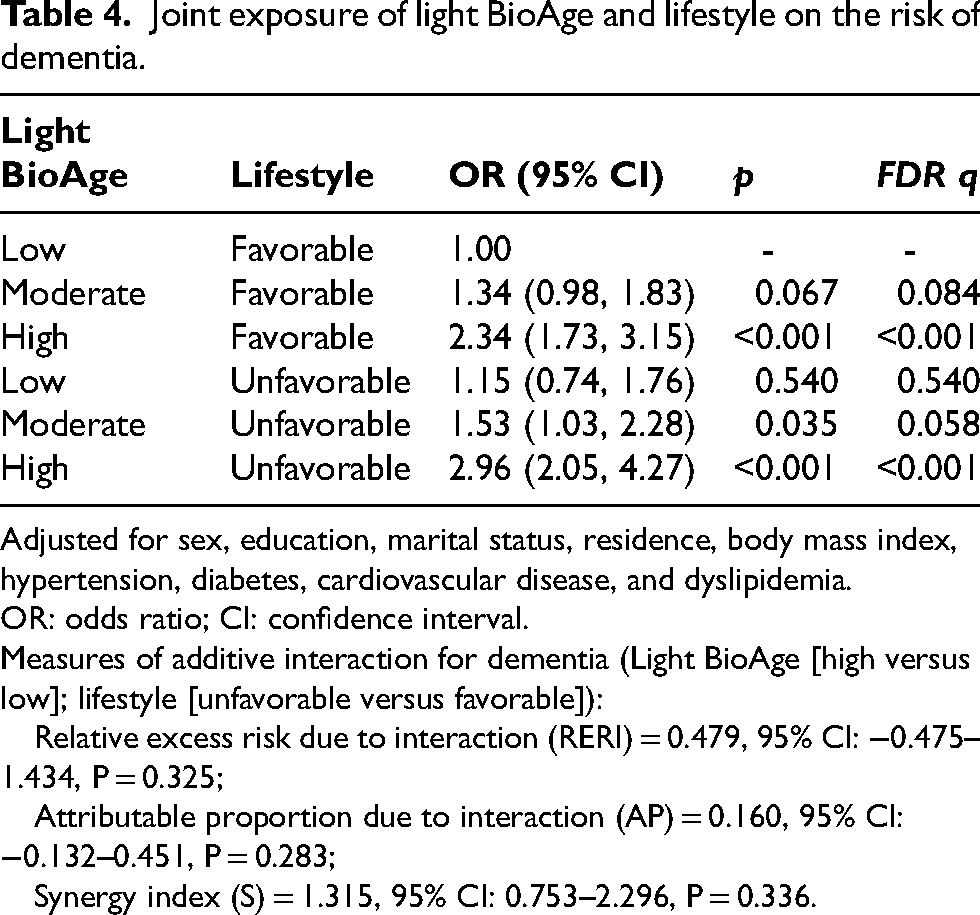
Adjusted for sex, education, marital status, residence, body mass index, hypertension, diabetes, cardiovascular disease, and dyslipidemia.
OR: odds ratio; CI: confidence interval.
Measures of additive interaction for dementia (Light BioAge [high versus low]; lifestyle [unfavorable versus favorable]):
Relative excess risk due to interaction (RERI) = 0.479, 95% CI: −0.475–1.434, P = 0.325;
Attributable proportion due to interaction (AP) = 0.160, 95% CI: −0.132–0.451, P = 0.283;
Synergy index (S) = 1.315, 95% CI: 0.753–2.296, P = 0.336.
Sensitivity analysis
The results remained consistent (Supplemental Tables 2 and 3) after further adjustment for baseline cognition scores and the use of multiple imputation for covariates.
Discussion
In this large-scale prospective analysis of middle-aged and older Chinese adults, we found that accelerated biological aging, as measured by Light BioAge, was strongly and independently associated with a higher risk of dementia. Individuals in the highest tertile of Light BioAge exhibited a 2.38-fold higher risk of dementia compared to those in the lowest tertile. This relationship demonstrated a clear dose-response pattern, with each year increase in biological age conferring a 4% incremental rise in risk. Furthermore, the joint presence of high BioAge and an unfavorable lifestyle resulted in the highest cumulative risk, nearly tripling the odds of dementia compared to those with low BioAge and a favorable lifestyle.
Our findings align with the emerging consensus that biomarker-based estimates of aging are superior to chronological age in predicting age-related pathologies. Previous research utilizing more complex metrics, such as PhenoAge or epigenetic clocks (e.g., GrimAge), has linked biological aging to cognitive decline and Alzheimer's disease.6–9 However, our study validates the utility of Light BioAge—a far more accessible metric requiring only three standard clinical blood tests. 12 The magnitude of the association observed here (OR 2.38 for the highest tertile) is comparable to, and in some cases exceeds, risk estimates reported for other established risk factors, suggesting that Light BioAge effectively captures a composite systemic vulnerability that specifically predisposes the brain to neurodegeneration.
A critical finding of our study is the lack of a significant interaction between lifestyle and Light BioAge. This suggests that the association between accelerated biological aging and dementia risk is robust and operates relatively independently of current lifestyle behaviors. In other words, a favorable lifestyle did not fully negate the elevated risk associated with high biological age in our cohort. However, the additive nature of these risks is clinically significant, as participants with high BioAge and unfavorable lifestyles fared significantly worse than any other group. This implies that while lifestyle modification remains a cornerstone of dementia prevention, individuals with accelerated biological aging may require more aggressive or targeted clinical interventions beyond standard lifestyle advice to manage their elevated baseline risk. However, this interpretation must be framed cautiously, as residual confounding from unmeasured lifestyle or environmental factors cannot be entirely ruled out. Moving forward, validating Light BioAge across diverse global populations and establishing standardized screening thresholds will be critical steps for its successful implementation in clinical practice.
The robust association between Light BioAge and dementia is likely underpinned by the specific physiological dysfunctions captured by its component biomarkers, including inflammation, glucose metabolism, and kidney function. First, elevated CRP, a key component of the Light BioAge algorithm, reflects chronic low-grade systemic inflammation. This “inflammaging” is a well-documented driver of neurodegeneration, capable of compromising the blood-brain barrier and activating microglia, thereby accelerating the accumulation of amyloid-beta and tau pathology.18,19 Second, fasting glucose levels serve as a proxy for insulin resistance and glucometabolic dysregulation. The brain is highly sensitive to insulin signaling, and peripheral insulin resistance has been linked to impaired neuronal bioenergetics, oxidative stress, and increased risk of both vascular dementia and Alzheimer's disease—a relationship often termed “Type 3 diabetes”.20,21 Finally, serum creatinine levels, indicative of renal filtration function, highlight the critical role of the kidney-brain axis. Renal dysfunction contributes to the retention of uremic toxins and vascular endothelial damage, which are strongly correlated with cerebral small vessel disease and white matter hyperintensities.22–24 By integrating these distinct but interconnected pathways, Light BioAge serves as a holistic marker of the “body-brain” connection.
The strengths of this study include the use of a large, nationally representative sample (CHARLS), rigorous data quality control which excluded participants with baseline cognitive impairment, and the application of a clinically translatable aging metric. However, several limitations should be acknowledged. First, the observational nature of the study precludes definitive causal conclusions. While we adjusted for baseline cognition to minimize reverse causality, subclinical neurodegeneration could theoretically influence baseline biomarkers, and residual confounding (such as socioeconomic status, diet, and environmental exposures) cannot be ruled out. Additionally, the substantial exclusion of participants due to missing baseline data, coupled with follow-up attrition, raises the possibility of selection and survivor biases. Second, BioAge was assessed at a single time point, analyzing trajectories of BioAge over time could provide deeper insights into the dynamic progression of risk. Third, the diagnosis of dementia was based on a composite of cognitive testing and informant reports rather than gold-standard clinical adjudication or neuroimaging, which may introduce some misclassification bias, although this method has been validated in large epidemiological studies. Finally, the lack of detailed data on specific pharmacological interventions (e.g., antihypertensives, statins) represents a potential source of unmeasured confounding; future studies incorporating comprehensive medication histories are needed to clarify potential interactions.
Conclusion
In summary, this study establishes Light BioAge as a powerful indicator of dementia in the Chinese population. By capturing systemic metabolic, inflammatory, and kidney function, Light BioAge offers a window into the physiological erosion that precedes clinical dementia. Our findings support the integration of biological age assessment into routine geriatric health screenings to identify high-risk individuals who may benefit from early, intensive preventive strategies targeting both biological, underlying comorbidities and lifestyle factors. Moving forward, as this study was restricted to middle-aged and older adults in China, validating Light BioAge across diverse global populations and establishing standardized screening thresholds will be critical steps for its successful implementation in clinical practice.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261457952 - Supplemental material for Association between Gompertz law-based biological age and dementia: A longitudinal study of middle-aged and older Chinese adults
Supplemental material, sj-docx-1-alz-10.1177_13872877261457952 for Association between Gompertz law-based biological age and dementia: A longitudinal study of middle-aged and older Chinese adults by Hua Liu, Yang Cheng and Chaofeng Fan in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We thank the China Health and Retirement Longitudinal Study team for providing data and training in using the datasets. We thank the students who participated in the survey for their cooperation. We thank all volunteers and staff involved in this research.
Ethical considerations
Ethics approval for CHARLS was obtained from the Biomedical Ethics Review Committee of Peking University (IRB00001052-11015). The protocol was in accordance with the Declaration of Helsinki.
Consent to participate
All participants provided signed informed consent.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.