
Abstract
Background
Auricular transcutaneous vagus nerve stimulation (atVNS) has been proposed as a non-invasive neuromodulation approach for cognitive disorders, including Alzheimer's disease (AD). Sleep represents a physiological state characterized by enhanced vagal activity and memory consolidation, making it a potentially optimal window for stimulation.
Objective
To investigate the cognitive effects of nocturnal atVNS in individuals diagnosed with mild cognitive impairment (MCI) and AD.
Methods
Participants underwent nightly atVNS using a Vguard device, specifically designed for non-invasive stimulation during sleep. Cognitive performance was evaluated using four standardized neuropsychological instruments, including the Alzheimer's Disease Assessment Scale Cognitive Subscale (ADAS-Cog).
Results
Repeated nocturnal atVNS over several months was associated with significant improvements in global cognitive function. Among the administered tests, the ADAS-Cog demonstrated the greatest sensitivity in detecting stimulation-related changes.
Conclusions
Nocturnal atVNS may constitute a promising therapeutic strategy for enhancing cognition in patients with MCI and AD. By leveraging sleep-related vagal activity, this approach could potentially delay or prevent the progression of MCI to AD and dementia.
Keywords
Introduction
The vagus nerve (cranial nerve X) is a major component of the parasympathetic nervous system. Twenty percent of the vagus nerve is efferent motor fibers. The modulatory role of this nerve on the central nervous system (CNS) has been discussed for decades.1–3 The electrical stimulation of the vagal nerve (VNS) was initially offered as a medical treatment for patients with refractory epilepsy who were not candidates for resective surgery. 4 Currently, this clinical procedure is recognized as a low-risk intervention and viable procedure for patients suffering from a broad spectrum of CNS disturbances.5,6 Generally, VNS is effective in approximately 30–60% of patients.7,8
One of the most promising directions of VNS is the treatment of cognitive disorders, including Alzheimer's disease (AD).3,9,10 VNS was shown to improve attention, arousal, various types of memory, mood, and decision-making in patients. However, some clinical studies have reported inconsistent effects of VNS on memory. 11 Undoubtedly, these discrepancies in the physiological effects of VNS may result from controlled and uncontrolled variables present during stimulation, including, among other factors: current intensity, pulse width, frequency of stimulation, “on” and “off” period durations, and the route of VNS administration.
In clinical practice, two different methods of VNS are applied. In case of invasive vagus nerve stimulation (iVNS), cuff electrodes are attached around the left cervical branch of the vagus nerve.12–14 Implanted electrodes affect not only the targeted afferent fibers but also the visceral efferent fibers of the mixed vagal branch. 6 This undesired stimulation of motor vagal fibers leads to multiple side effects, such as cough, voice alteration, swallowing difficulties, and bradycardia,13,15 which can complicate long-lasting treatment. Non-invasive transcutaneous stimulation of the vagal nerve (tVNS) is applied via surface skin electrodes. In contrast to iVNS, relatively strong currents are required to circumvent skin resistance. Since the induced stimulation field is diffuse, it may also affect the efferent fibers, which may result in neck pain, dizziness, headache, nasopharyngitis, and oropharyngeal pain. 13 These side effects are especially common in the case of cervical transcutaneous vagal nerve stimulation (ctVNS).16,17 The second type of non-invasive stimulation is labelled auricular transcutaneous vagal nerve stimulation (atVNS). The feasibility of auricular atVNS was first demonstrated using recordings of vagal somatosensory evoked potentials from the scalp. 18 The auricular branch of the vagus nerve is also known as Arnold's nerve. 19 The cervical vagus nerve at the level of the jugular ganglion, where the VN contains the bodies of the sensory ganglionic neurons, is located just outside the cranium. 13 In contrast to previously mentioned stimulation techniques, atVNS affects mainly afferent fiber endings. This approach results in a pronounced reduction in side effects. Hence, this technique is currently considered to be the most promising electroceutical therapy in humans. 13
The scientific rationale for VNS as a treatment for cognitive disorders is based on evidence that vagal stimulation affects widespread brain structures involved in regulating cognitive functions. 20 In the present clinical study, we took advantage of the properties of atVNS. We investigated the effects of long-lasting atVNS on cognitive function in individuals recognized as suffering from mild cognitive impairment (MCI) and AD. MCI stage is characterized by the presence of single- or multiple-domain cognitive disorders without impairment in independent functioning. 21 In most cases, MCI precedes the onset of AD. Therefore, treatment involving the use of VNS in the MCI stage has the potential to provide neuroprotection in AD.
The present study employed the VGuard device (Figure 1) (www.cogniguard.com), specifically designed to minimize the mechanical burden associated with the presence of a mini-neurostimulator and concha electrodes. We hypothesized that compared to sham stimulation, atVNS would enhance cognitive function in individuals diagnosed with MCI and AD. To increase compliance and the likelihood of obtaining the expected positive effect of VNS on cognitive function, the stimulation protocol was applied for the first time on a nightly basis, a period of increased vagal nerve activity. 22
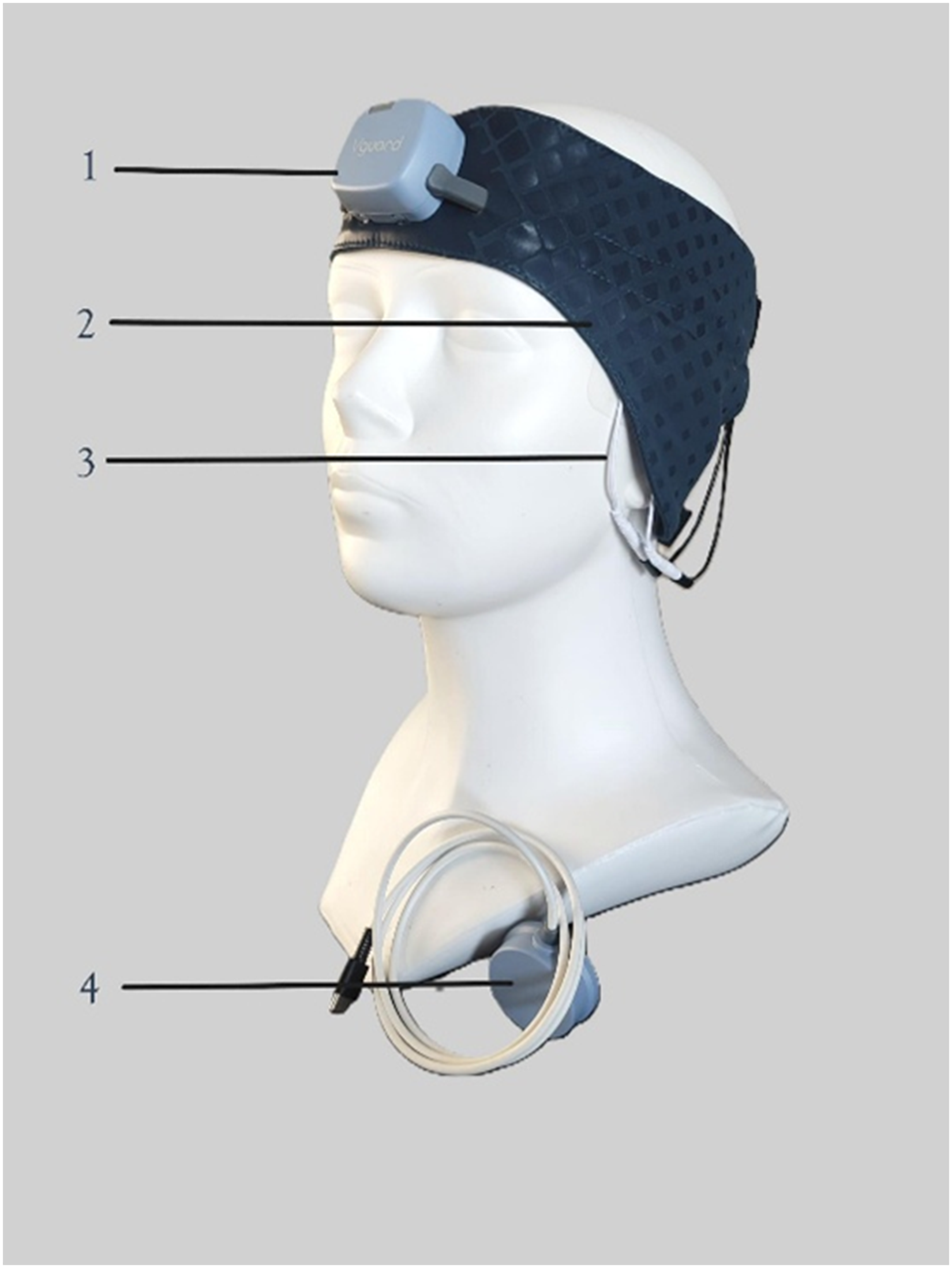
The Vguard device. 1-stimulator, 2- headband, 3-electrodes, 4-wireless charger.
Methods
The study was conducted between Jan 2021 and December 2022. The study was reviewed and approved by the Ethics Committee of the Medical University of Lodz (decision no. RNN/320/19/KE) and conformed to the ethical standards of the Declaration of Helsinki (1964).
Study overview
This study assessed the impact of atVNS stimulation on cognitive abilities. Stimulation was administered nightly using a Vguard device during sleep, a period of increased activity of the vagus nerve, and the period of processing newly acquired memory traces into permanent ones, known as memory consolidation. 23 This process is disrupted in the initial phase of AD. 20 A randomized, double-blind, sham-controlled clinical evaluation was conducted on a group of patients diagnosed with MCI and AD. Patients enrolled in the study met the criteria specified by the National Institute on Ageing-Alzheimer's Association workgroups on diagnostic recommendations for AD for the symptomatic predementia phase of AD, referred to in this study as MCI and AD.
Inclusion and exclusion criteria
Inclusion criteria: patients aged ≥ 40 and ≤85 years who met the diagnostic criteria for MCI and AD as defined by the National Institute on Aging-Alzheimer's Association workgroups on diagnostic recommendations for AD.
Cognitive impairment was confirmed by the Mini-Mental State Examination (MMSE) and Alzheimer's Disease Assessment Scale (ADAS-Cog) tests.
Exclusion criteria
Subjects meeting any of the following criteria were not enrolled in the study: 1) Current or past history of active psychosis, intellectual disability, major depression, bipolar disorder, alcohol abuse, addiction to psychoactive substances, or any other major psychiatric condition. 2) Current or past history of any neurological disorder other than dementia, such as epilepsy, stroke, transient ischemic attack, Huntington's disease, Hakim syndrome, Parkinson's disease, multiple sclerosis, intracranial hematoma or brain lesions, and history of previous neurosurgery or head trauma that resulted in residual neurologic impairment. 3) Anticancer treatment administered within 12 months before the screening visit. 4) Clinically relevant serious comorbid medical conditions within 3 months prior to the screening visit, including but not limited to a. current active or persistent infection, b. clinically significant cardiac disease, including unstable angina, acute myocardial infarction, congestive heart failure (NYHA III or NYHA IV), uncontrolled hypertension (>2nd stage), c. severe liver disease, d. severe renal impairment, e. uncontrolled diabetes, f. chronic obstructive pulmonary disease, g. other metabolic, endocrine, or systemic diseases affecting the central nervous system, which, in the physician's opinion, may be the cause of dementia, h. permanent usage of benzodiazepines, i. insomnia, j. known positive status for human immunodeficiency virus (HIV), k. metal implants (excluding dental fillings) or devices such as pacemakers, medication pumps, nerve stimulators, TENS units, ventriculo-peritoneal shunts, and cochlear implants, unless cleared by the study investigator, l. serious communication barrier, and m. clinically significant abnormalities in screening laboratory tests.
The patients were randomly divided into two groups: the sham group and the active group. All the patients who were qualified and included in the study, as well as the researchers who qualified the patients in the study, did not know to which study group (treatment or sham) the patient was randomly assigned. All participants provided verbal and written informed consent and followed the same treatment protocol.
Clinical procedures
The following clinical procedures were used within the medical experiment: demographics and health survey, physical examination, questionnaires, and four different tests: MMSE, ADAS-cog, Color Trails Test (CTT), and Verbal Memory Probing (VMP). 24
The demographics and health survey
This survey consisted of questions concerning age, education, professional activity, past and current medical conditions, concomitant medications, medical interventions, and hospitalizations, family status, psychiatric diseases among family members, history of cognitive impairment and AD in family, head trauma, alcohol abuse, and addiction to psychoactive substances.
Physical examination
A general medical history and physical, psychiatric, and neurological examinations were required at the screening/baseline visit.
The questionnaires and tests
The questionnaires and psychological tests listed above were administered at each patient's study visit. Typically, the tests were repeated after 1, 2, and 3 months. However, in patients who continued the study longer than 3 months, the tests were performed after 6 months. The time required to perform all the tests during the study visit was approximately 1–1.5 h.
Concomitant therapy
Individuals receiving a stable pharmacotherapy regimen for coexisting diseases were included in the study, provided that their treatment aligned with the exclusion criteria. Patients treated with cholinesterase inhibitors were also included in the study.
Stimulation parameters
Active atVNS delivered stimulation at the frequency of 25 Hz, 0.5–2.0 mA current intensity, and with a duty exchangeable off/on cycles. The sham device was identical in appearance and interface but delivered no current.
Auricular transcutaneous vagal nerve stimulation device, stimulation procedure, and parameters
The atVNS was applied every night through the Vguard device, which was specifically designed for patients to use on a nightly basis under home conditions. It is composed of four parts: a stimulator, a headband, concha electrodes, and a wireless charger (Figure 1).
During the night, the device was automatically cycled through the stimulation phases. Activation and stimulation reports were wirelessly sent from the device to the controller smartphone and the cloud-based data collection center. Each device was equipped with specialized software enabling the assessment of the effectiveness of stimulating electrode contact with the skin through continuous impedance measurements and a time and stimulation cycle registration system. Following the completion of each stimulation cycle, data from the stimulator were transmitted to the central monitoring “cloud” base system. This approach allowed for the evaluation of patient compliance and the stimulation quality of each participant.
Stimulation was delivered by specifically designed adhesive concha electrodes in repeated “on” and “off” cycles. Stimulation was applied in repetitive cycles interspersed with “washout” periods.
Statistical analysis
As this is a pilot study, the sample size was based on study feasibility and subject safety considerations, rather than on power analysis and formal hypothesis testing. Linear mixed effect models were used to analyze the change in test results over time; each model included interaction between group and timepoint as well as subject ID as a random effect. Then contrasts were created for comparisons between groups and different time points. Model residuals were checked for homoscedasticity, normality, and independence. Results were presented using estimated marginal means with standard error.
As a sensitivity analysis, missing data were imputed using multiple imputation for longitudinal data, using chained equations. To support study findings, a complete case analysis was also performed in which changes over time, pairwise comparisons were analyzed using the Wilcoxon signed-rank test; to account for multiple comparisons, p-values were adjusted using the Holm method. For complete case analysis
Analyses were performed using R 4.5.0 (R Foundation for Statistical Computing, Vienna, Austria, 2025) with package “gtsummary” version 2.2.0, “rstatix” version 0.7.2, “mice” version 3.19.0, “emmeans” version 1.11.1, and “lme4” version 1.1–37.
Linear mixed-effects models with random intercepts (participant-level) assessed group × time interactions on outcomes, estimated using restricted maximum likelihood was used. Interpretation of ADAS-Cog accounts for item-level reliability considerations over time per recent guidance (item and domain level analysis) 25 and similarly to other research. 26
In the primary analysis, handling of missing data was performed by using multiple imputation by chained equations (m = 10) under a missing-at-random assumption; estimates were combined with Rubin's rules. Complete-case analyses are presented as supportive and involved non-parametric tests (Mann–Whitney/Wilcoxon with Holm correction). Sensitivity analyses, including analyzing data using a linear mixed-effect model without imputing missing data was performed.
Outcomes
The prespecified primary endpoint was the change from baseline in ADAS-Cog total score at months 1–3 (with 6 months exploratory). Secondary endpoints included MMSE, CTT, and VMP at matching timepoints. Exploratory outcomes included device adherence, blinding integrity, adverse events, and self-reported sleep and mood (if available).
Sample size rationale
Given the paucity of longitudinal data for nocturnal atVNS in early AD, we designed this as a pilot trial to evaluate feasibility and generate variance estimates for future powering. We targeted n≈60 with a 2:1 allocation to optimize safety and learning regarding active stimulation exposure. No formal hypothesis-testing sample size was prespecified.
Randomization and allocation concealment: A computer-generated random sequence with variable block sizes was prepared by an independent statistician not involved in enrollment or assessment; assignments were concealed using secured web-based system operated by an independent engineer.
Implementation
Investigators enrolled participants; allocation was revealed to the unblinded device programmer (independent engineer) only after baseline assessments. Participants, study clinicians, study sponsor, and outcome assessors were blinded to assignment.
Study design
Randomized, double-blind, sham-controlled, parallel-group pilot trial with a 2:1 allocation (active: sham). The protocol and statistical analysis plan adhered to CONSORT 2025 guidance; a participant flow diagram is provided (Figure 2).
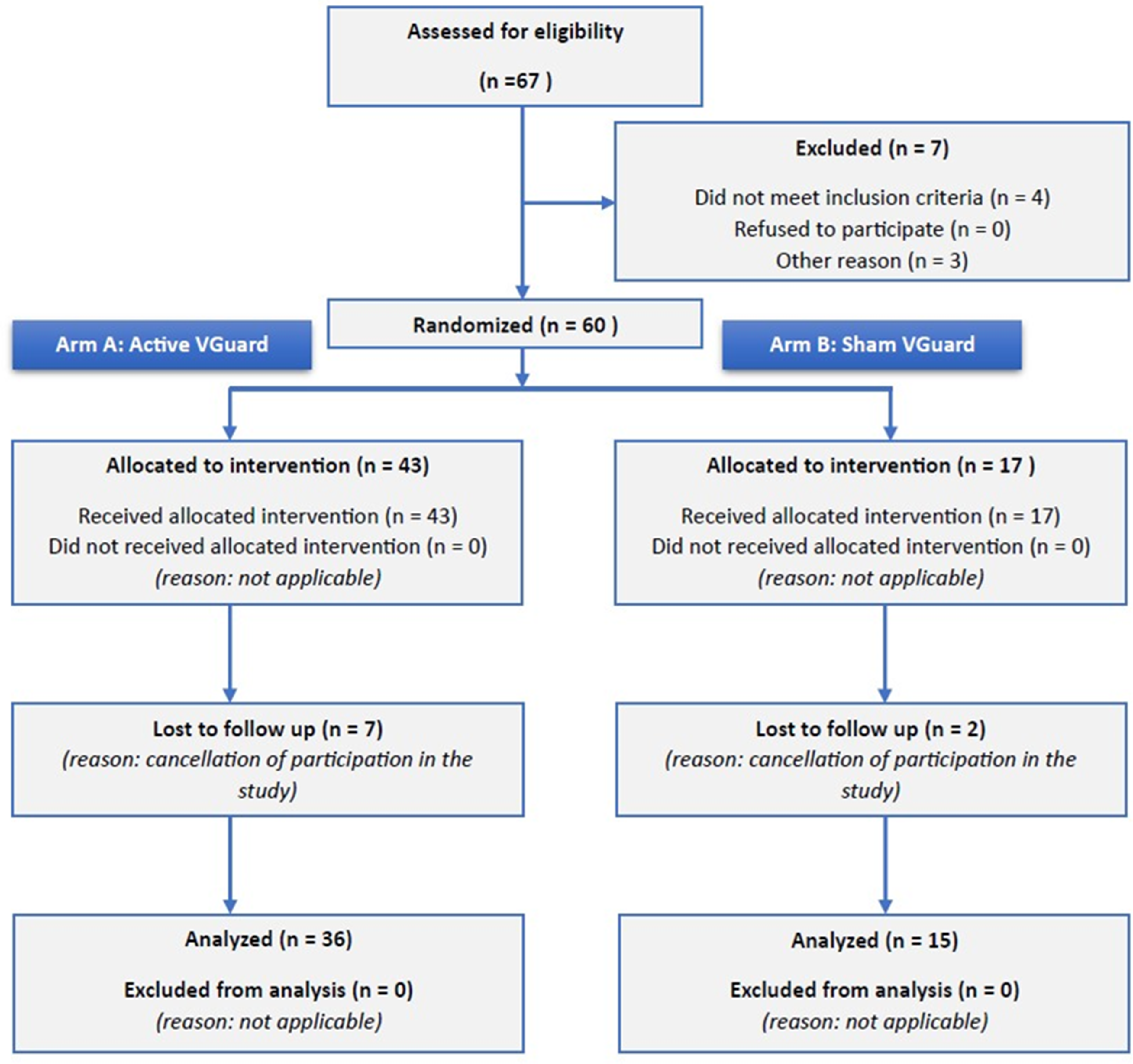
The study flowchart.
Trial registration
This trial was registered at ClinicalTrials.gov (Identifier: NCT06620640).
Results
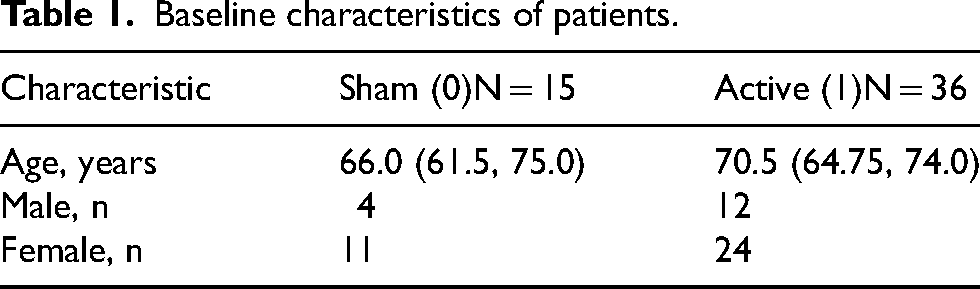
271 patients were reviewed in the screening process. An eligibility assessment was conducted for 67 patients, 60 of whom were randomized. The patients were randomly divided into two groups: the sham group and the active group. Forty-three patients were included in the active group, and 17 patients were included in the sham group. During the study, 9 patients dropped out of the study (7 from the active group and 2 from the sham group). Finally, the results of 51patients were analyzed, including 36 from the active group and 15 from the sham group. The participants’ median (IQR) age was 70 (63;75) years. In the study cohort, 16 patients were males, and 35 were females. The basic characteristics of the groups are presented in Table 1. The baseline study lasted for 3 months, with extension to 6 months. The study flowchart was presented in Figure 2.
Baseline characteristics of patients.
Primary study objective
ADAS-Cog tests
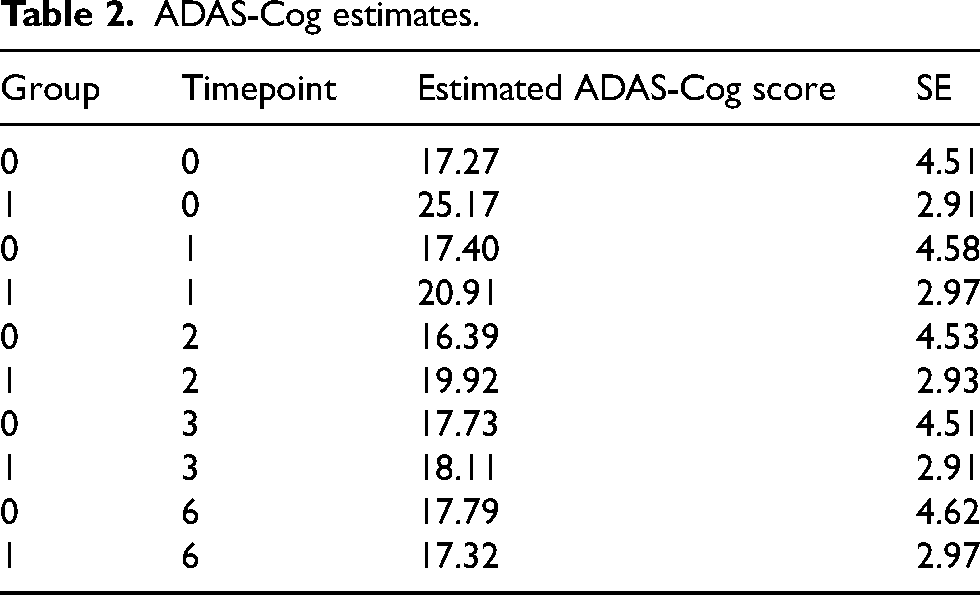
The effect of atVNS was assessed based on changes observed in the ADAS-Cog scale. Results were compared between the sham group and the active group, both before the initiation of stimulation (baseline, at week 0) and after its completion (at the 3rd or 6th month; Tables 2 and 3; Figure 3A, B).
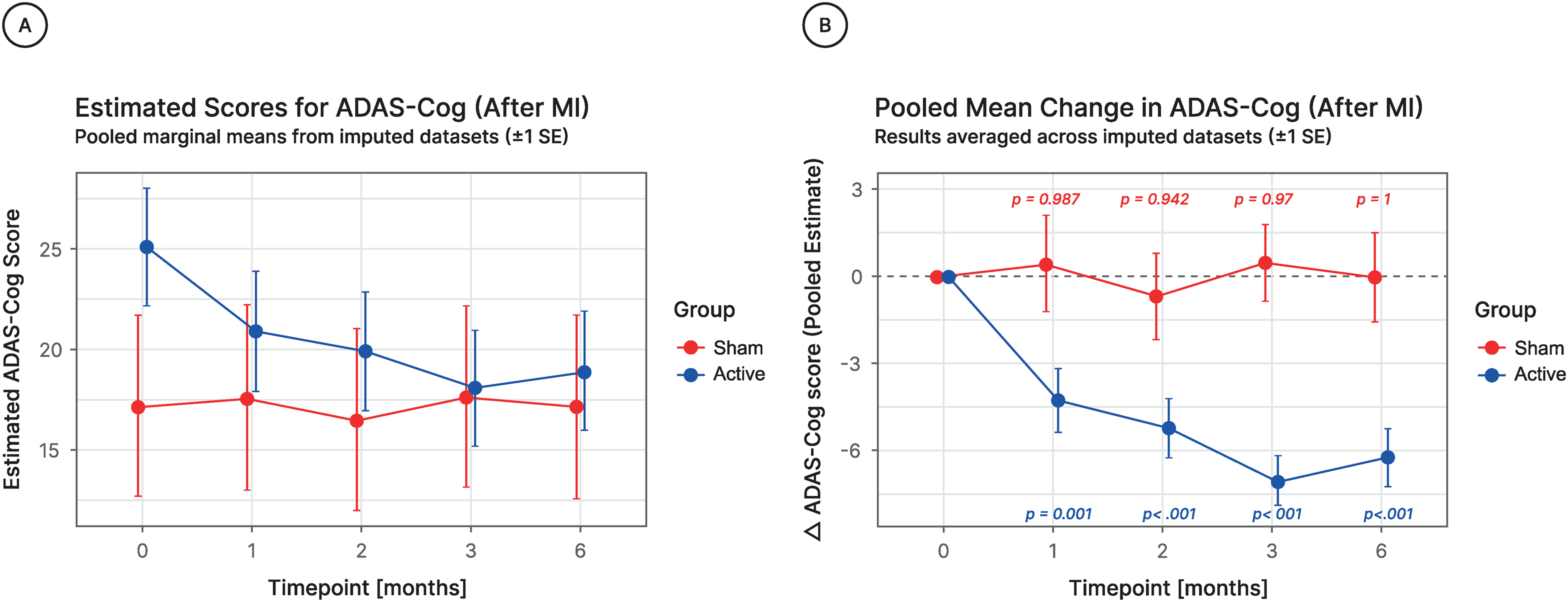
(A) Estimated ADAS-cog scores after imputation of missing data (MI) at baseline and 1, 2, 3, and 6 months follow-up visit for both sham and active groups. Values presented as estimated mean with ±1 SE, calculated using a mixed-effects model for longitudinal data. (B) Estimated change in ADAS-Cog scores from baseline to 1, 2, 3, and 6 months follow-up visit for both Sham and Active groups. Values presented as estimated mean change from baseline with ±1 Standard Error, calculated using mixed-effects model for longitudinal data. P-values are calculated for change between analyzed follow-up visit and baseline.
ADAS-Cog estimates.
Pairwise comparisons—by timepoint and group.
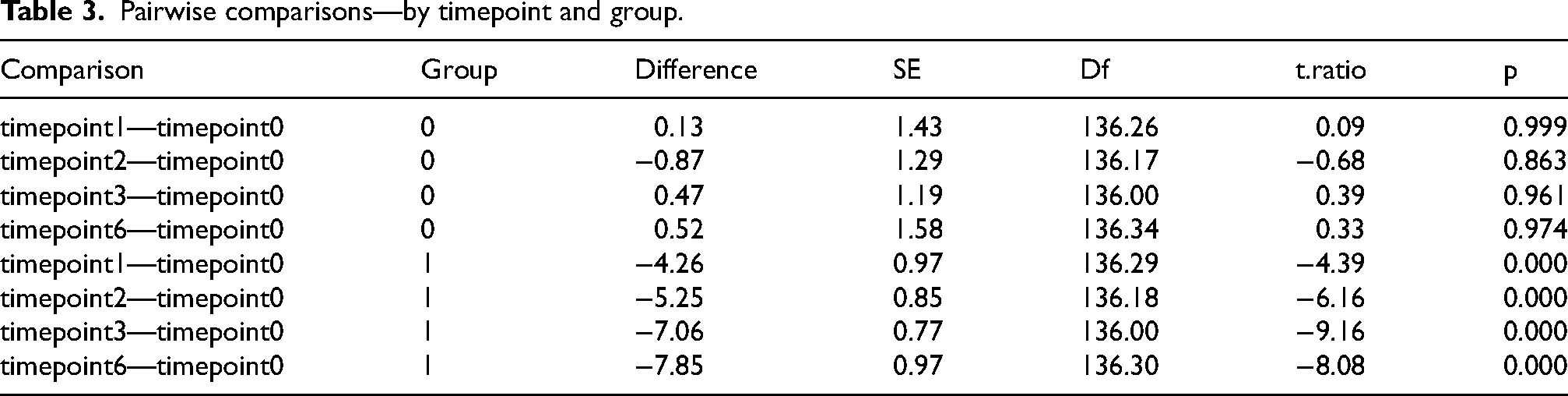
Tables 2 and 3 demonstrate the estimated scores at baseline and each follow-up visit, as well as the change from the baseline with SE and p-value, for sham and active groups, values estimated from the mixed-effect model for longitudinal data; p-values adjusted for multiple comparisons.
Figure 3A and 3B show that a statistically significant improvement in cognitive function, as measured by the ADAS-Cog test, was observed at the end of the first month of atVNS treatment only in the active group. No statistically significant differences were noted in the ADAS-Cog test in the sham group. Figure 3A and 3B also show the time course of atVNS's effect on ADAS-Cog scores over 6 months.
VMP test
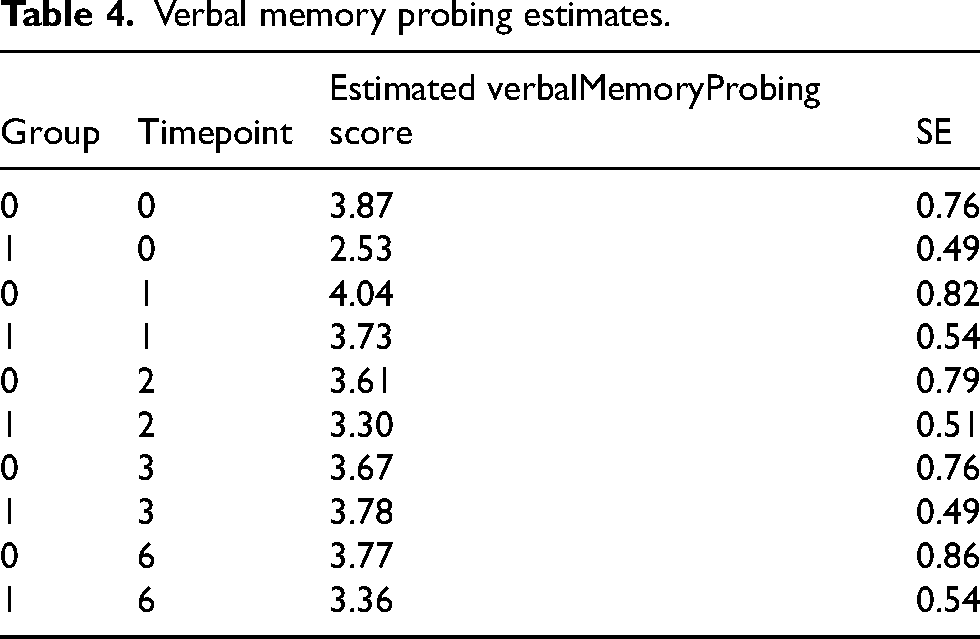
The effect of atVNS was assessed based on changes observed in the VMP scale. Results were compared between the sham group and the active group, both before the initiation of stimulation (baseline, at week 0) and after its completion (between the 1st and 6th month; Tables 4 and 5; Figure 4A, 4B).
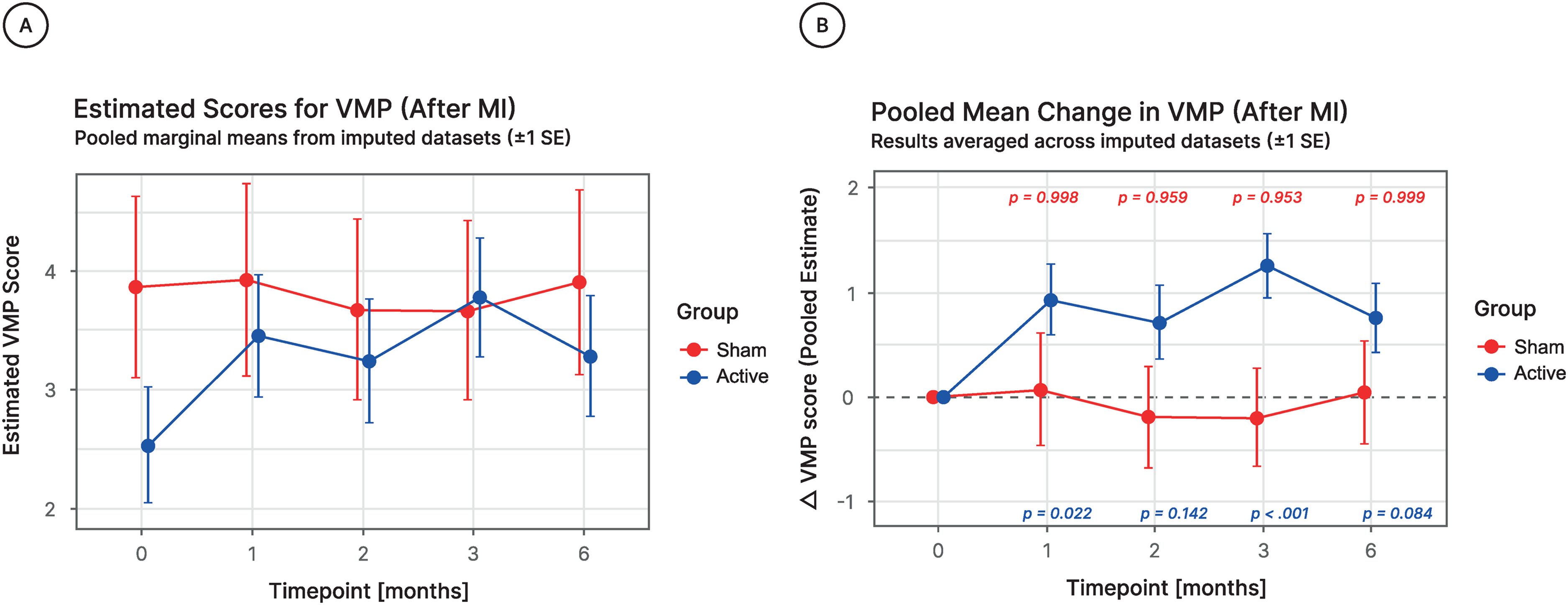
(A) Estimated VMP scores after imputation of missing data (MI) at baseline and 1, 2, 3, and 6 months follow-up visit for both sham and active groups. Values presented as estimated mean with ±1 SE, calculated using a mixed-effects model for longitudinal data. (B) Estimated change in VMP scores from baseline to 1, 2, 3, and 6 months follow-up visit for both Sham and Active groups. Values presented as estimated mean change from baseline with ±1 Standard Error, calculated using mixed-effects model for longitudinal data. P-values are calculated for change between analyzed follow-up visit and baseline.
Verbal memory probing estimates.
Pairwise comparisons by timepoint and group.
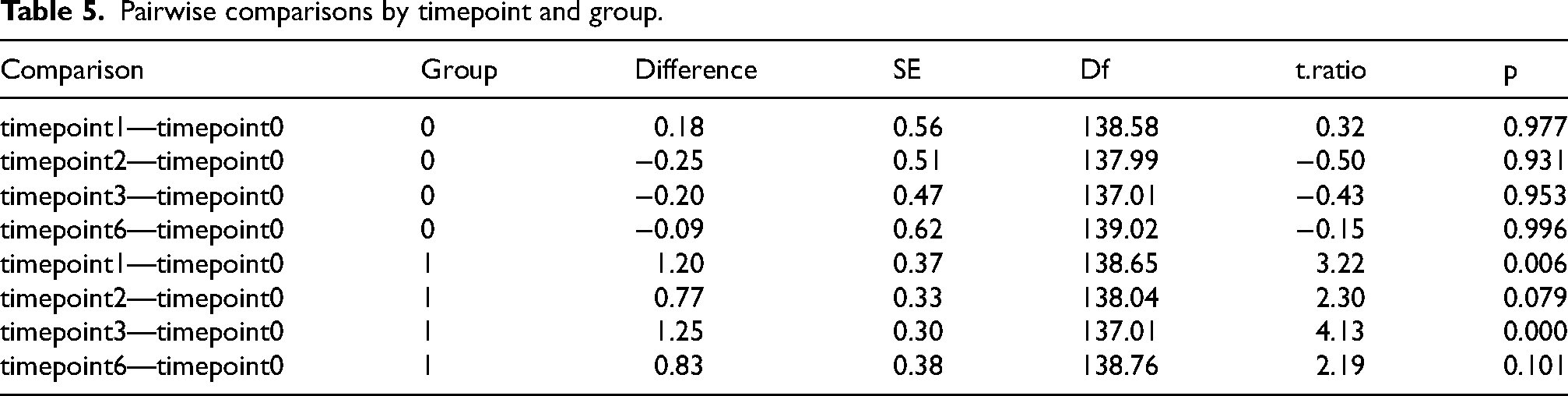
Tables 4 and 5 demonstrate the estimated scores at baseline and each follow-up visit, as well as the change from the baseline with SE and p-value, for sham and active groups, values estimated from the mixed-effect model for longitudinal data; p-values adjusted for multiple comparisons.
Figure 4A and 4B show that a statistically significant improvement in cognitive function (measured by the VMP test) was observed at the end of the first month of atVNS treatment only in the active group. No statistically significant differences were noted in the VMP test in the sham group. Figure 4A and 4B also demonstrate the time course of the effect of atVNS on the VMP test over 6 months.
CTT
The effect of atVNS was assessed based on changes observed in the CTT scale. Results were compared between the sham group and the active group, both before the initiation of stimulation (baseline, at week 0) and after its completion (between the 1st and 6th month; Tables 6 and 7; Figure 5A, B).
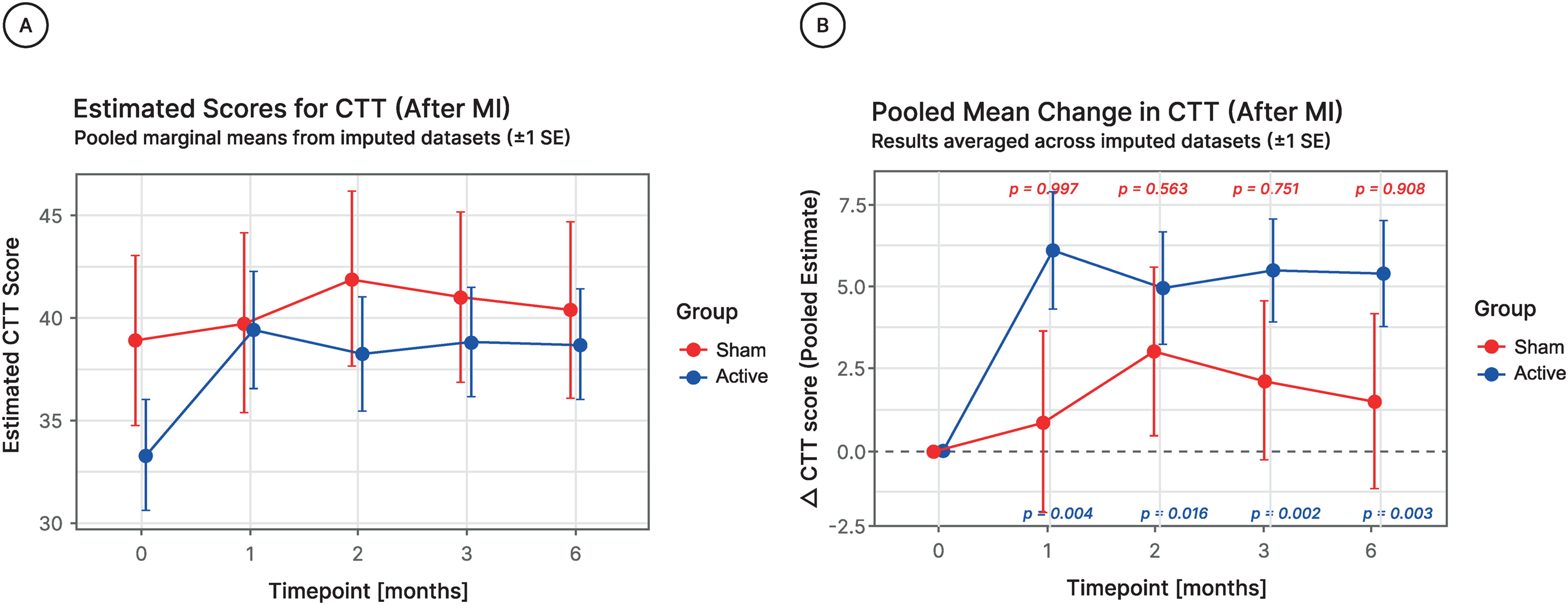
(A) Estimated CTT scores after imputation of missing data (MI) at baseline and 1, 2, 3, and 6 months follow-up visit for both sham and active groups. Values presented as estimated mean with ±1 SE, calculated using a mixed-effects model for longitudinal data. (B) Estimated change in CTT scores from baseline to 1, 2, 3, and 6 months follow-up visit for both Sham and Active groups. Values presented as estimated mean change from baseline with ±1 Standard Error, calculated using mixed-effects model for longitudinal data. P-values are calculated for change between analyzed follow-up visit and baseline.
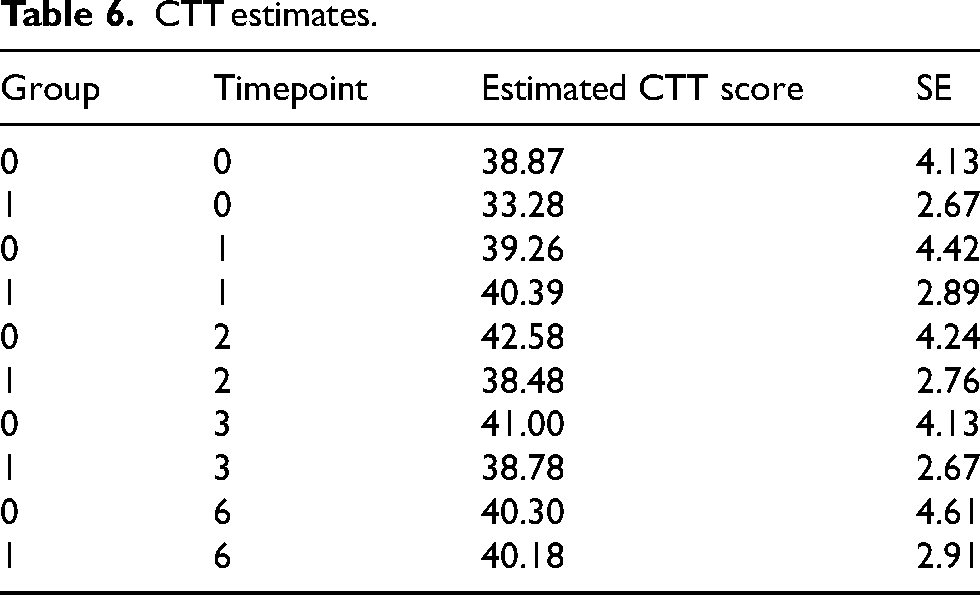
CTT estimates.
Pairwise comparisons by timepoint and group.
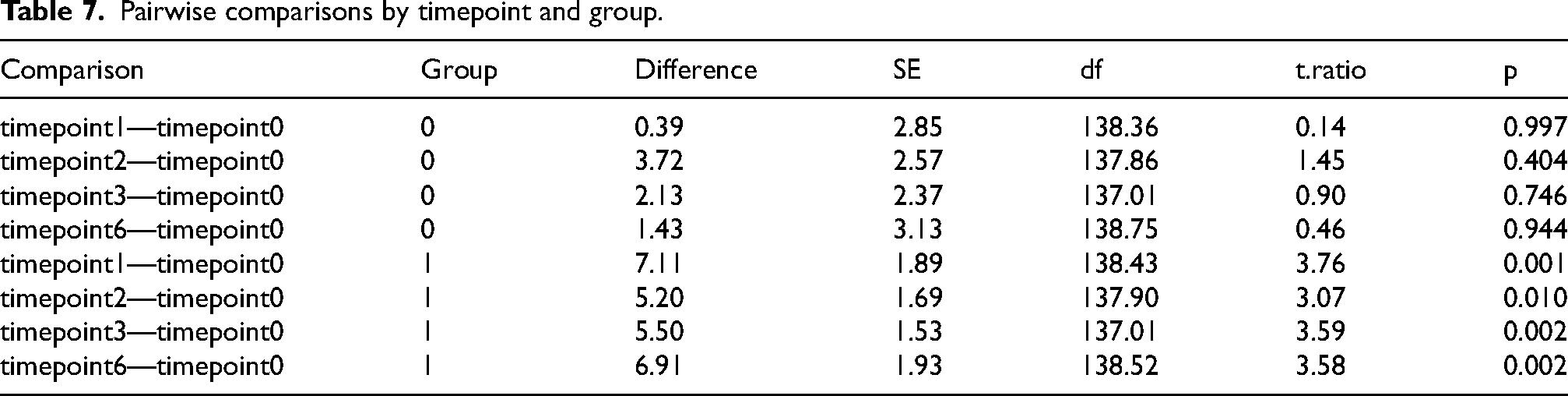
Tables 6 and 7 demonstrate the estimated scores at baseline and each follow-up visit, as well as the change from the baseline with SE and p-value, for sham and active groups, values estimated from the mixed-effect model for longitudinal data; p-values adjusted for multiple comparisons.
Figure 5A and 5B show that a statistically significant improvement in cognitive function (measured by the CTT test) was observed at the end of the first month of atVNS treatment only in the active group. No statistically significant differences were noted in the CTT test in the sham group. Figure 5A and 5B also demonstrate the time course of the effect of atVNS on the VMP test over 6 months.
MMSE test
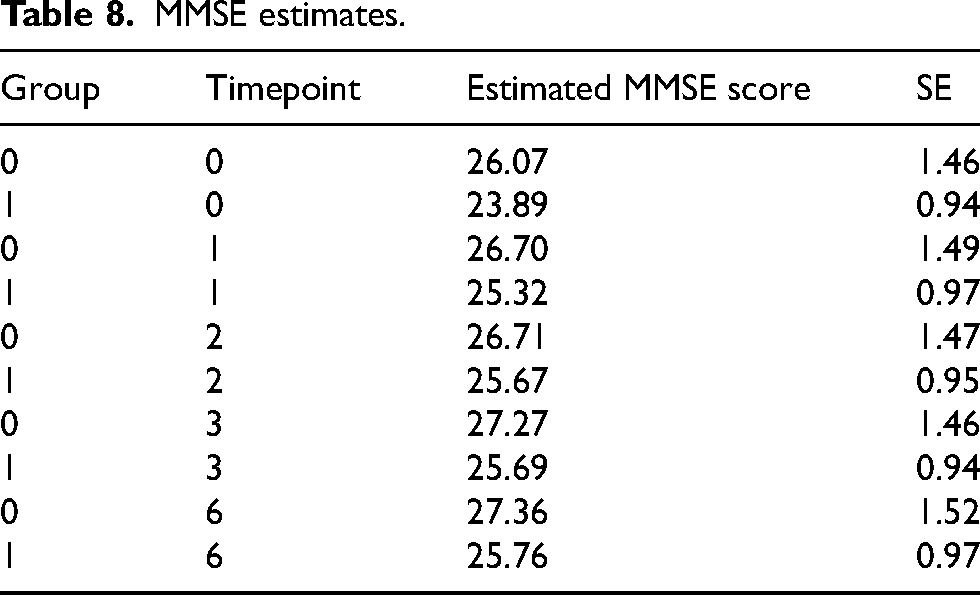
The effect of atVNS was assessed based on changes observed in the MMSE test. Results were compared between the sham group and the active group, both before the initiation of stimulation (baseline, at week 0) and after its completion (between the 1st and 6th month; Tables 8 and 9; Figure 6A, B).
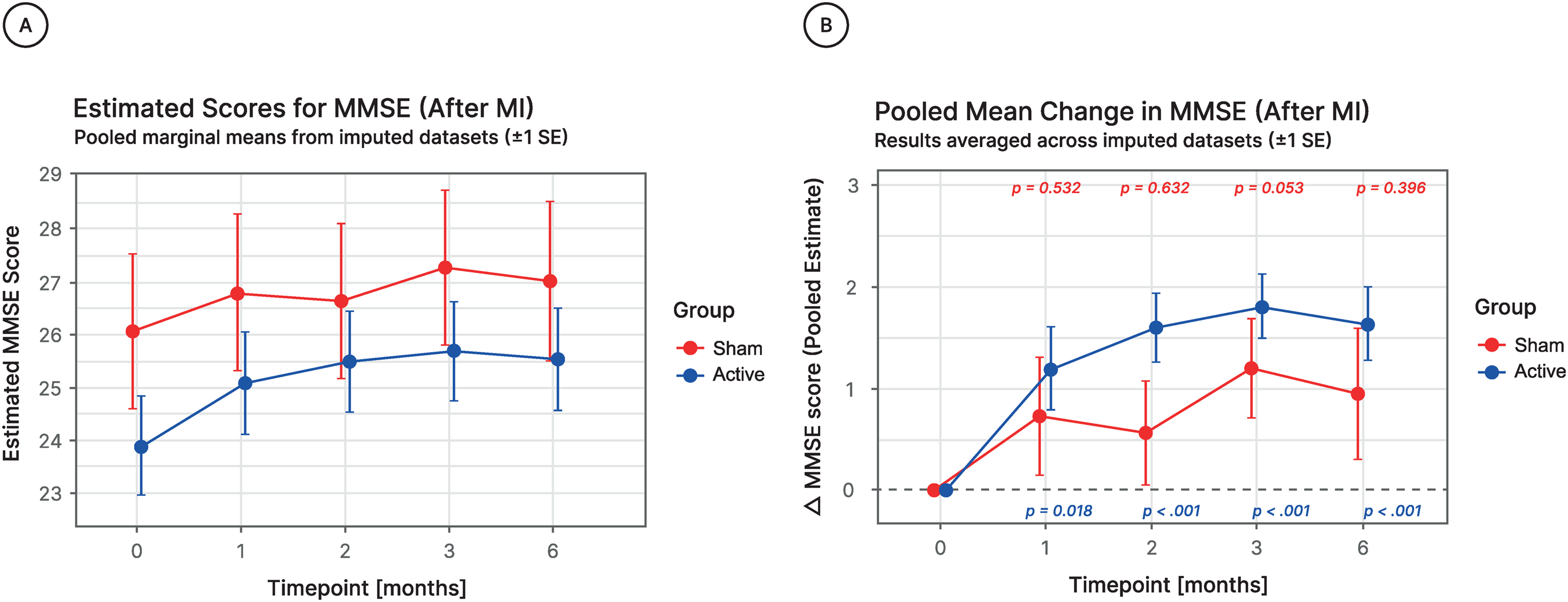
(A) Estimated MMSE scores after imputation of missing data (MI) at baseline and 1, 2, 3, and 6 months follow-up visit for both sham and active groups. Values presented as estimated mean with ±1 SE, calculated using a mixed-effects model for longitudinal data. (B) Estimated change in MMSE scores from baseline to 1, 2, 3, and 6 months follow-up visit for both Sham and Active groups. Values presented as estimated mean change from baseline with ±1 Standard Error, calculated using mixed-effects model for longitudinal data. P-values are calculated for change between analyzed follow-up visit and baseline.
MMSE estimates.
Pairwise comparisons by timepoint and group.
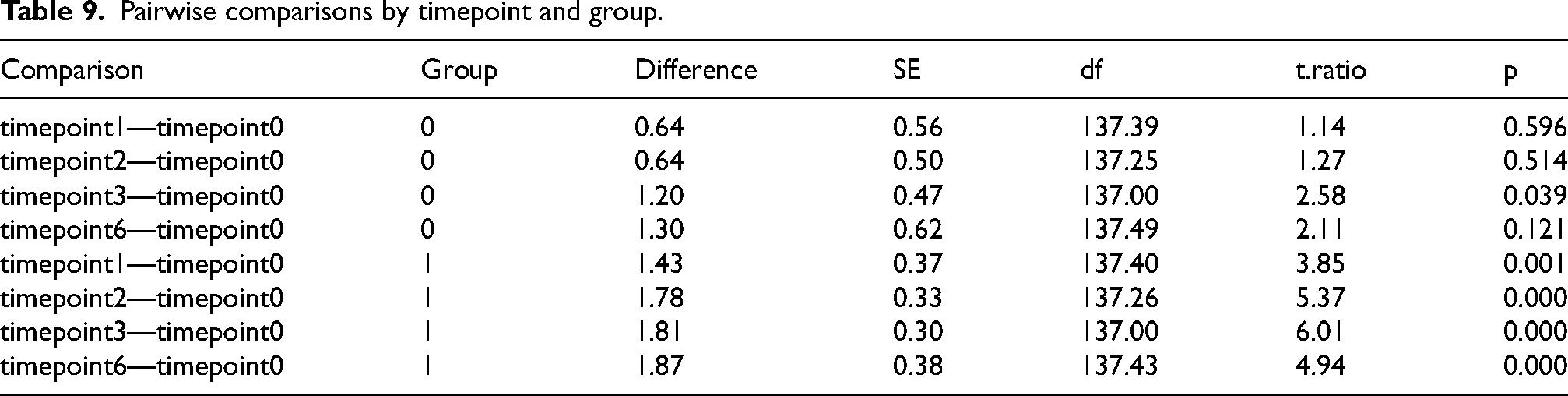
Tables 8 and 9 demonstrate the estimated scores at baseline and each follow-up visit, as well as the change from the baseline with SE and p-value, for sham and active groups, values estimated from the mixed-effect model for longitudinal data; p-values adjusted for multiple comparisons.
Figure 6A and 6B show that a statistically significant improvement in cognitive function, tested by MMSE score, was observed already at the end of the first month of atVNS only in the active group. No statistically significant differences were noted in the MMSE test in the sham group. Figure 6A and 6B also demonstrate the time course of the effect of atVNS on MMSE score over 6 months.
Trial registration and protocol transparency
The trial was registered at ClinicalTrials.gov (NCT06620640). Any deviations from the protocol/statistical analysis plan are documented and justified.
Safety of the study
In the clinical trial, Vguard stimulation was well tolerated by the patients, with no recorded serious adverse events. The most reported mild side effects were skin reactions at the electrode–skin contact site and headache. None of the reported symptoms required urgent medical intervention or led to study discontinuation.
Discussion
The study was designed as a double-blind, sham-controlled trial to evaluate the effects of atVNS on cognition in patients with MCI and AD. Participants diagnosed with MCI or AD were enrolled based on the NINCDS-ADRDA criteria. The selection of this pathological condition is not arbitrary but arises from several clinical considerations. Firstly, in most cases, patients diagnosed with MCI due to AD typically progress towards full-blown AD. 27 Secondly, from a clinical diagnostic standpoint, precise differentiation of patients in the MCI group and the initial phase of AD is clinically challenging, given the lack of effective treatment methods at each stage of disease development. Another crucial reason for choosing this stage of the disease is the relatively low degree of advancement of the neurodegenerative process in the MCI phase, allowing more effective activation of brain structures associated with cognitive function and memory processing.2,17 These structures (including the locus coeruleus, hippocampus, and neocortex) are known to undergo degenerative processes in the early preclinical phase of AD. 20 The cognitive-enhancing effects of VNS were previously reported in several clinical studies.3,9 However, typically this procedure has been applied only during the daytime, and the studies were not randomized or blinded. 9 The present study describes the first time the effect of a novel, nocturnal application of atVNS. This was technically possible due to the development of a specially designed VGuard stimulator for conducting the study, along with the selection of stimulation parameters that do not induce sleep disturbance in the patient. To the best of our knowledge, the atVNS procedure used in the present study has never been employed in nighttime treatment. Interestingly, a circadian variation in vagal activity was previously demonstrated in humans.10,28 Vagal activity was observed to be higher at night and lower during the daytime. The advantage of atVNS application during sleep was also dictated by the fundamental importance of the REM phase in the memory consolidation process. 23
Analyzing the etiology of the relatively fast and pronounced improvement in cognitive function in MCI-diagnosed individuals, one important factor must be taken into consideration: the possibility of the interaction of the nocturnal pattern of atVNS with the appearance of REM sleep cannot be ruled out. This suggestion is supported by observations delivered from rats: specifically, the REM sleep indicator in anesthetized rats is recognized to be a hippocampal formation (HPC) type 2 theta rhythm, and VNS was previously demonstrated to induce this type of theta in urethanized rats.1 In other words, more type 2 theta in HPC field potential in anesthetized rats, more REM sleep, and hence increased probability of improved memory consolidation. However, based on current observations in individuals diagnosed with MCI and AD we are not yet able to explore this possibility in detail. Nonetheless, it clearly warrants further investigation.
In this study, a statistically significant improvement in ADAS-Cog score change from baseline was observed between the sham and active groups at all monthly assessments, with the greatest improvement recorded at 6 months. Time-course analysis of atVNS effect with the use of the remaining tests did not reveal such a spectacular effect. However, the time-course analysis demonstrated that, except for the CTT test, to reach a distinct effect (i.e., 40% improvement), less than three months of nocturnal application of atVNS was necessary. These findings suggest that the relatively rapid and robust improvement in cognitive function in response to nocturnal atVNS may result from an additive effect of naturally elevated vagal activity at night combined with nocturnal electrical stimulation.
The primary outcome of the study was the significant improvement in patients’ cognitive abilities, rather than merely halting or delaying the progression of the disease. The results also confirmed the safety of non-invasive atVNS application.
In the study, standardized cognitive tests that are validated and accepted in the dementia research community were used. Longer stimulation studies are required to establish the durability of the observed cognitive improvement and evaluate whether sustained atVNS use can alter the trajectory of cognitive decline in AD.
This study has several limitations that should be acknowledged. First, we did not perform a domain-level analysis of the ADAS-Cog. Although the scale comprises multiple subdomains reflecting distinct cognitive functions, our analysis focused on the total score. A more granular evaluation may yield insights into domain-specific effects of stimulation and will be addressed in a subsequent publication. Second, we did not assess potential effects of stimulation on sleep parameters or depressive symptoms, as these measures were beyond the scope of the present work, which focused primarily on cognitive outcomes.
In summary, the results from this randomized, sham-controlled, double-blind study confirm the positive effect of atVNS on the cognitive functions of patients diagnosed with MCI and AD. These results are in line with previous findings on the efficacy of the atVNS method.29,30 Due to its effectiveness and simplicity, the methodology used in the present study may represent a promising therapeutic approach for delaying or even preventing the conversion of MCI and the initial stages of AD into a fully manifested dementia disorder.
Footnotes
Acknowledgements
We thank the study participants and their caregivers, as well as the clinical and data management teams.
Ethical considerations
The study was reviewed and approved by the Ethics Committee of the Medical University of Lodz(decision no. RNN/320/19/KE) and was conducted in accordance with the ethical standards set out in the Declaration of Helsinki (1964). All participants gave their written informed consent prior to participating in the study.
Consent to participate
All participants provided written informed consent before participating in the study. Each person signed an approved consent form after receiving detailed information about the study's objectives, procedures, potential risks, and benefits.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was co-financed by the European Funds under Priority Axis I: Research, development, and commercialization of knowledge of the Regional Operational Program of the Lodz Voivodeship, Poland, for the years 2014-2020. Project no: RPLD.01.02.02-10-0067/17-00. ClinicalTrials.gov ID: NCT06620640.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AB, MK, TBD are employees of Cogniguard Medical Holding and Neuromedical. AB, TBD have patent applications assigned to Cogniguard Medical Holding.
Data availability statement
The data sets generated and analyzed in this study are available from the corresponding author upon reasonable request.