
Abstract
Background
People living with Alzheimer's disease often require support from their relatives, who may face emotional and physical challenges in their role. Up to 90% of people living with cognitive impairment experience unmet needs such as wandering.
Objective
The aim of the study was to analyze the narrative of relatives of people living with Alzheimer's disease experiencing unsatisfied behavioral needs and whether this has a relationship with levels of burden.
Methods
Relatives who cared for a family member with Alzheimer's disease at home participated in a structured interview with a psychologist and completed the Zarit Burden Interview to assess caregiver burden. An analysis was conducted of the frequency of words used in the relatives’ responses to the question “What is your experience of your loved one's wandering?”.
Results
A total of 15 relatives participated in the study. Relatives with higher levels of burden related to their role as caregivers were more likely to use words such as “disorder” (on average once per interview), “problem” (on average three times per interview), and “difficulty” (on average twice per interview), than people with low levels of burden. For people with low levels of burden, the word “need” appeared as a significant expression (on average four times per interview).
Conclusions
Relatives who experience less burden are more likely to understand the reasons behind their loved ones’ need or desire to wander. They are less likely to perceive this behavior as a problem and restrict the person's freedom of movement for their own safety.
Keywords
Introduction
In 2024 in Poland, over 366,000 people have been diagnosed with Alzheimer's disease (AD) or other forms of dementia, which represents an increase of approximately 8% compared to 2014 data. 1 These numbers are expected to continue to grow, in line with global predictions. Similar trends are also being observed in other countries (e.g., China, USA), requiring a comprehensive response at the individual, national and international levels. 2 Many people living with dementia have the support of family members, most often spouses and children. 1 In Poland, supporters of persons living with dementia are mainly spouses (over 60%)—more often wives, children (around 20%) and siblings (around 10%).3–5 Family members have to transform their role and address a range of issues- architectural barriers, administrative matters, transportation to activities and medical care, responding to unmet needs of loved ones, managing finances, managing personal and work life.3–5 What's more there is absence of a unified framework to support the family system and family members have to contact multiple places in synchronous interaction, both statutory and non-profit organizations. It may be both challenging and partly empowering. Although this study did not focus mainly on the protective factors, it is crucial to note that it is possible for family members to strengthen their resilience in situations of providing support. However, there are also protective factors such as high levels of self-efficacy, personal mastery, and use of positive coping styles 6 focus on positive aspects of caregiving, having social support and spirituality to rely on. 7 Without those self-resources and support for themselves, caregivers are at risk of “caregiver burnout”, a situation in which a person uses their resources (mental and physical) to such an extent that they are no longer able to effectively support a family member. 8 As a result, many people experience chronic stress, which can significantly affect the quality of life and relationships of both parties. 9 Relatives of people with dementia are at a high risk of burnout, mainly due to the highly emotional nature of the relationship and the desire to meet their unmet needs, e.g., the need to move and walk.10,11
Some behavioral changes, such as wandering, may occur in people with dementia. While clinically they can be classified among the behavioral and psychological symptoms of dementia (BPSD), 12 they may also reflect attempts to express or meet certain unmet needs, for instance, the need for movement or social interaction. Understanding these underlying needs is crucial for improving care and the quality of life of both individuals with cognitive impairment and their family members. People with cognitive impairment who benefit from family support have on average three unmet needs. 13 The most commonly identified unmet needs were boredom or sensory deprivation, loneliness or the need for social interaction, and the need for meaningful activity. 13 Loved ones and other supporting people can help recognize these needs. 14 One of the needs that is common and crucial to address is the desire for movement.
Because this often requires the company of other people (e.g., during hikes), family members are often more involved in satisfying this need, and ensuring the safety of walks. Sometimes the pressure family members put on themselves (of satisfying unmet needs of loved ones, guaranteeing safety (e.g., fall prevention), changes in spending time together, building relationships), may lead to increased stress levels, burden, and, over a longer period, burnout.15,16 While ‘caregiver burden’ and ‘caregiver burnout’ are often used interchangeably, it is thought that they describe different stages of the caregiving experiences. Caregiver burden reflects the natural weight of the physical, emotional, and social demands that come with supporting a loved one. When these demands remain high for a long time without enough support or respite, it can lead to caregiver burnout. This is a state of deep exhaustion where a person may feel emotionally drained or disconnected, not due to a lack of compassion, but because their personal reserves have been fully depleted by the relentless nature of the role.15,16
In this article, wandering refers to the unmet need to move and engage that relatives support. The need for movement in the absence of adequate support, can cause confusion and increase risk of falls. 17 Relatives may offer support through adaptations to the environment, reshaping the relationship with their loved one and predicting situations that may be risky (e.g., removing carpets or glueing them to the floor). 18 Without support, knowledge, and tools to take care of their own emotions and needs, family members may experience burden and in longer perspective burnout.19,20
According to previous studies, the main factors that can affect the level of burden and burnout in family members are the gender of the caregiver, the number of hours spent helping and the lack of free time for themselves, the caregivers self-esteem and the severity of their (both the family member and person with cognitive impairment) medical conditions. 21 Furthermore, reshaping relationships and seeking strategies to satisfy needs may be more stressful for spouses that feel responsible for their loved one with cognitive impairment. 22 This is in line with evidence around the need to adapt the whole family system to any change, both positive and threatening to the system, the length of stressful situations and support.23,24 The way relatives describe and perceive people with cognitive impairment needs in the home environment may reflect their own levels of stress, burden, and burnout. 25 Individuals with higher levels of burden and burnout tend to perceive “wandering” more often as problematic and disruptive to daily life. Schulz and Martire 25 found that family members with higher levels of burden and potential burnout were more likely to use negative language to describe their experiences. Family members with a lower level of burden are more likely to approach these behaviors with understanding, perceiving them as an expression of unmet needs. 10 They are more likely to try to understand the causes of the behavior and find meaning in it. 9 Therefore, the narratives shared by relatives may be indicative of their current experiences and could help to tailor support interventions for them. Recent research highlights that when families have a deeper understanding of the challenges associated with AD, it can significantly improve their overall well-being and quality of life. 26 When it comes to the experience of wandering, we believe that knowing a person's life history is a vital part of this understanding. 26 By connecting a loved one's movements to their past experiences, stories and habits, caregivers can reframe what might seem like a ‘purposeless symptom’ into a meaningful expression of the person's identity. This shift in perspective can help lighten the emotional weight of caregiving and foster a deeper sense of connection. 26
This study aimed to understand the wandering narratives from the perspective of relatives caring for a person with dementia, in the context of their experience of burden in the caregiving role. It also analyzed the context of supporting the need to wander and the ability of family members to do so in context of burden levels, to answer the following questions:
does the degree of caregiver burden influence the narrative about wandering? does the degree of caregiver burden influence the view and nature of implemented strategies for wandering in home-based circumstances?”
Methods
Design
Mixed-methods design utilizing semi-structured interviews, based on an interview topic guide by Griffiths et al., 27 and a survey. This qualitative narrative approach allowed more detailed exploration of how family members construct meaning around wandering. The behavior that is closely linked to personal history, relationships, and unmet needs. The study followed O'Brien et al. 28 Standards for Reporting Qualitative Research.
Eligibility criteria
Inclusion criteria: over 18 years old; family member of person diagnosed with AD; providing informal support, meaning an unpaid family member, partner, who provides vital, often daily, support to a person living with dementia and not being hired or formal volunteer, e.g., as professional staff to provide care); providing home-based, support to a person diagnosed with AD; having experience of supporting a person with dementia who experiences wandering; willingness to participate; providing informed consent.
Exclusion criteria: being a professional caregiver; being a family member of an individual living in institutional care settings.
Sample acquisition
Recruitment was carried out using flyers distributed in local healthcare centers, care partner support groups, and community centers in Kraków and Katowice. Flyers were freely accessible at the reception desk and at the doctor's office. Digital versions of the flyers were also disseminated through social media platforms and online forums dedicated to dementia family members. Both versions of flyers had phone numbers printed on them. Family members who were interested in participation or wanted to gain more information could call and schedule a longer interview with researchers. This sampling strategy ensured the total cohort remained within the predefined parameters. To enhance thematic saturation and perspectival diversity, the inclusion criteria were designed to accommodate additional family members if necessary. Following the principle of information power, 29 we determined that the high specificity of our clinical sample and the intensive nature of the intervention provided sufficient depth to address our pilot research questions despite the modest sample size.
Procedure
The study consisted of an online survey and an interview via telephone.
Interviews lasted between 30 and 60 min, were conducted by trained psychologists experienced in qualitative interviewing, and were audio-recorded with participants’ consent using built-in recording functions. Telephone version was preferred instead of in-person interviews due to distance between cities, preferences of family members.
After the telephone interview, participants received a link to the anonymous online survey, which served as a follow-up to gather additional information. The survey was administered online using the Google Forms platform.
Participation was voluntary, and no financial or material compensation was offered. The study was conducted in accordance with the guidelines of the Declaration of Helsinki and approved by the Ethics Committee. Audio recordings were transcribed verbatim using automated speech recognition tools (speech-to-text in Microsoft Word) by the researcher (GP), followed by manual verification and correction by the researchers (GP, JD, NSH) to ensure accuracy and understanding of Polish language. Two researchers independently coded the transcripts to enhance validity in addition to the manual verification. Discrepancies were resolved through discussion between three researchers responsible for coding until consensus was reached, ensuring transparency and rigor in the coding process.
Sample
The study group consisted of 15 family members (6 men, 9 women) of individuals diagnosed with AD living in Poland. The sample size was considered sufficient based on the concept of information power, as participants shared rich, experience-based narratives closely aligned with the study aim and analytic framework.
Participants’ ages ranged from 40 to 79 years (M = 60.3). The mean age in family members diagnosed with AD was 75.5 years with an average time of 4.7 years since diagnosis (min:1 year, max.:10 years). The mean score obtained on the Zarit Burden Interview (ZBI) was 15.3 (range: 6–32), indicating variation in levels of caregiver burden and potential burnout across the sample.
Materials
Qualitative interviews were guided by the topic guide by Griffiths et al. 27 The tool was originally developed for residential care settings and adapted for home situations in this study. This incorporated demographics and background, knowledge of wandering among people with dementia, experience in supporting people with dementia to wander, understanding of any initiatives taken at home, and education and training that were individually given to people who support. In Poland there is no formal psychoeducation and medical training available for family members. They have to search for information on their own (e.g., from various unstructured support groups, courses and webinars). The questions based on the topic guide were translated first into Polish and back-translated into English for verification. The topic guide was indicative and was refined during the course of conducting interviews. Cultural differences (e.g., environmental and family) were taken into account to ensure that the guide was appropriate for the target population.
In addition, relatives completed the ZBI Questionnaire for assessing caregiver burden. The Polish version of the ZBI consists of 12 questions that assess the level of burden and was obtained from Mapi Research Trust.30,31 Responses are given on a 5-point Likert scale, where questions 1–11 are answered on a scale from 0–“never” to 4–“almost always.” The final score is a sum of points ranging from 0 to 48, where higher scores indicate a higher sense of care burden. Validation studies of the short version of the ZBI have demonstrated high reliability, and good internal consistency. 32 Analysis revealed significant correlations between ZBI scores and other scales assessing care partner stress and burden, confirming its adequacy in measuring the intended construct. 32 Furthermore, analysis of the short version among family members of people living with dementia indicated good correlation with the 22-item version and was deemed to be sufficient and effective to assess burden and burnout in caregiver roles. 33
For analytical purposes, caregiver burden was operationalized using a cut-off score of over 19 on the 12-item ZBI, consistent with previous research distinguishing lower and higher levels of burden. 33 This threshold enabled comparative analysis of narratives in relation to burden intensity. Narratives were examined not only for thematic content but also for linguistic framing, particularly the use of problem-oriented versus need-oriented language. This approach allowed exploration of how burden and burnout levels may shape both interpretation of wandering and the strategies used to support or restrict it.
Phenomenological content analysis of the responses allowed the researchers to capture the subjective experiences of Polish family members’ verbal narratives to wandering in relation to the degree of burden. Phenomenological Content Analysis is a research method used in social sciences to explore the subjective experiences of study participants. It assumes that language and narrative reflect the way individuals construct and experience their reality. This analysis involves identifying recurring patterns in participants’ statements and exploring the meanings they assign to their experiences. 34 Reflective thematic analysis (RTA) 35 was used as a complementary measure to maintain sensitivity to the need for wandering. This hybrid approach allowed us to remain close to the essence of the experiences lived, while recognizing the interpretive role of analysis.
Moreover, the analysis of family members’ perspectives was conducted using a combined deductive–inductive approach. Initially, a deductive framework was applied, based on themes identified in existing literature and theoretical models related to caregiving and dementia. This allowed for systematic exploration of established constructs such as role strain, emotional support, and family dynamics.36,37 However, during the coding process, it became evident that participants’ narratives often diverged from the predefined categories. In particular, expressions of certain themes were characterized by varying affective tones—either optimistic or pessimistic—that were not fully captured by the original framework. To address this, the analysis was extended inductively, enabling the identification of new subthemes and tone-specific variations grounded in the data itself. The iterative process of shifting between deductive coding to obtain theoretical coverage and inductive coding to obtain nuances allowed for a more comprehensive and authentic representation of participants’ relationships. As noted in recent methodological literature, such integration of approaches enhances both the breadth and depth of qualitative analysis.36,38
The verbal transcription obtained in response to the questionnaire-based interview was analyzed for the frequency of words used by relatives in response to the question “How do you perceive your loved one's wandering?” This allowed the researchers to find words that, based on their frequency of occurrence, would indicate changes related to their perception of wandering through the prism of burden and potential burnout. Our goal was also to identify patterns related to the strategies chosen to reduce burden.
Reflexivity statement
The analysis was conducted by psychologists with clinical and research experience in working with family members of people with dementia. As researchers familiar with the challenges of caregiving, the team adopted a reflexive stance to remain attentive to how their professional background and prior assumptions could shape data interpretation. Reflexive discussions were held throughout the analytic process to ensure that interpretations remained grounded in participants’ narratives rather than researchers’ expectations.
Results
The mean score obtained on the 12-item ZBI was 15.3 (range: 6–32), indicating a mild level of caregiver burden according to established cut-off values. For comparative purposes, participants were grouped into lower-burden (ZBI < 20) and higher-burden (ZBI ≥ 20) categories, and this distinction was used to examine differences in thematic framing and word use across narratives.
Themes were initially organized according to the thematic guide developed by Griffiths et al. 27 Translated and adapted to Polish conditions and the home environment, the tool served as a deductive framework for the initial stages of the analysis. Finally, themes were organized using a combined deductive–inductive framework, allowing identification of both predefined and emergent patterns in family members’ narratives. This approach facilitated the identification of predetermined themes related to support for wandering behaviors and family experiences. However, as mentioned in the methodology, the authors decided to use an inductive approach to identify the unique relations and experiences of people of Polish nationality. This combined approach enabled a structured yet flexible analysis that took into account both theoretical significance and participants’ insight.
More positive mentions of themes appeared in narratives of less burdened family members. But importantly, more positive and less often negative descriptions were present across people's narratives. The theme “impact of dementia” had the most negative mentions despite the level of burden. Most Polish family members had positive narrations among most themes. They felt connected with their loved ones. Eleven out of fifteen family members (73.33%) had only positive and supportive mentions across strategies, help and relationships. Positive narrations across themes had been more common for family members than negative ones. Out of all mentioned themes, positive perspective was reported in all of them at least 4 times, whereas maximum mention of negative theme was 3. The exception was the topic “the impact of dementia”, which had more negative mentions (8 negative, 5 positive). Seven themes had all positive mentions. Three themes had all positive mentions except for one. The detailed presence and analysis of its positive or negative aspect is shown on Figure 1.
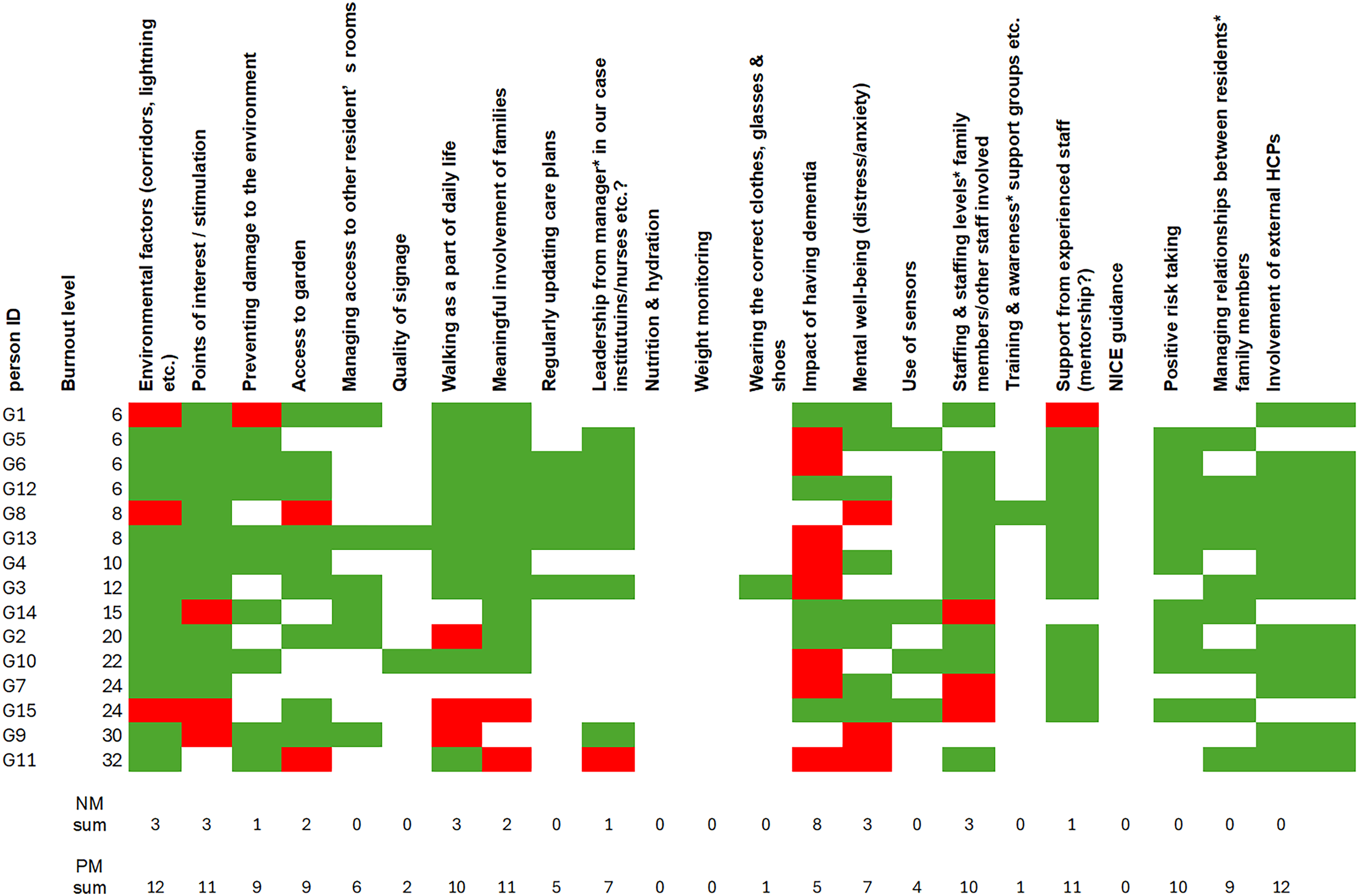
Thematic analysis. green box: positive mention; red box: negative mention; null box: not mentioned; NM: sum- sum of negative mentions among themes; PM sum: sum of positive mentions among themes.
Individuals with scores below 20 on the ZBI questionnaire, a cut-off commonly used in previous research to distinguish between lower and higher levels of caregiver burden,30,32 showed more numerous, proactive, non-pharmacological, need-driven strategies to support wandering tendencies and according to wordcount use more need-driven words to describe the behavior of their family member (see Figure 2). In the present study, this threshold was therefore applied to split the sample into “lower-burden” (< 20) and “higher-burden” (≥ 20) groups for comparative purposes.
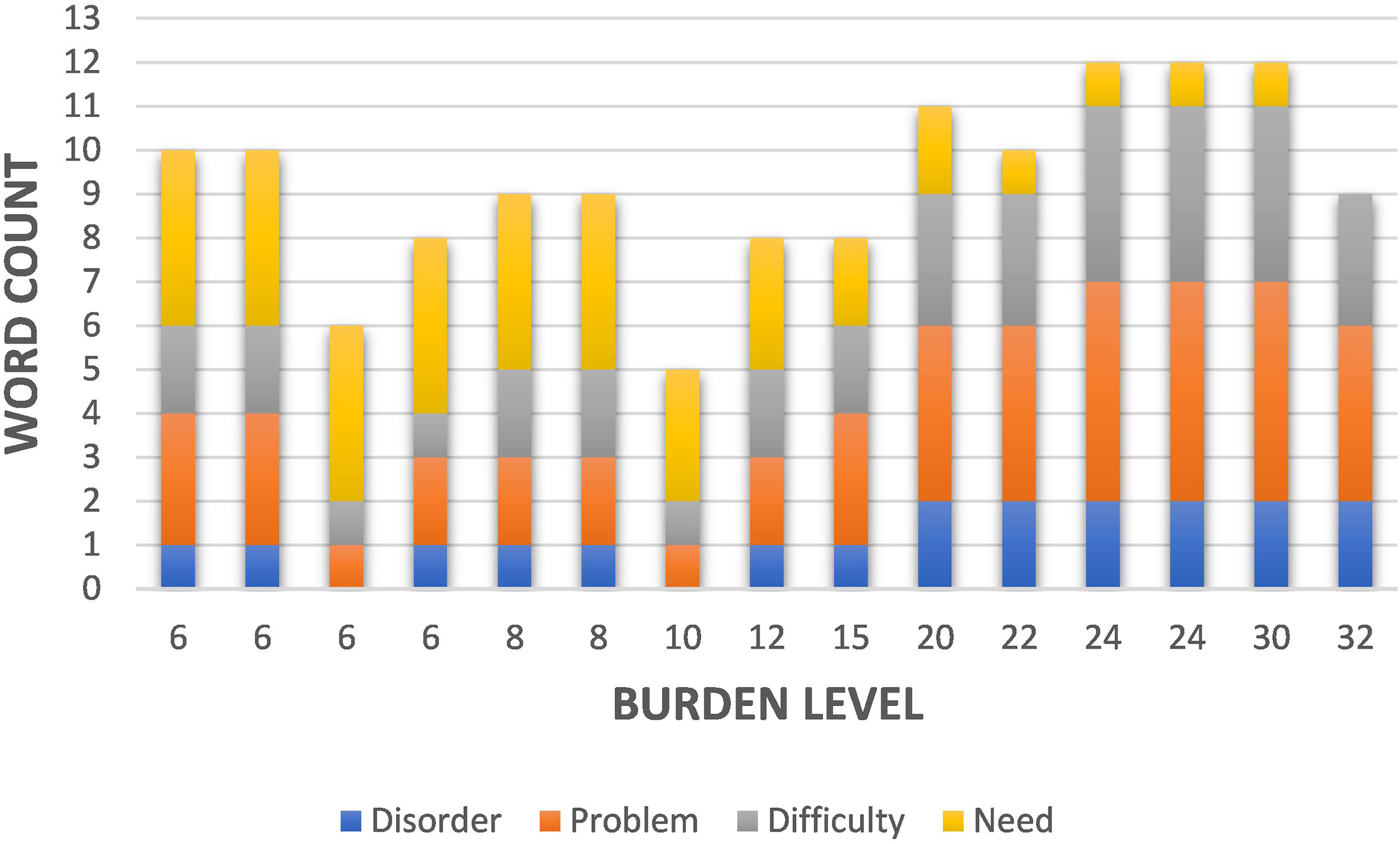
Distinction of used words according to the level of burden.
All respondents perceived a correlation between environmental conditions and ‘wandering’. More burned-out relatives saw the environment as a potential trigger for wandering and generally described it as challenging. Although despite them being over cutoff point for potential burnout they sought help, e.g., among medical professionals. In contrast less burned-out saw the potential of wandering in shaping their relation with significant others.
Less burned-out relatives were more likely to use their knowledge about the history and life story of family members, their preferences regarding spending time, places, etc., and used it for a range of activities. Also evident among this group is a shift from preventing wandering and its associated risks to joint activities that build relationships and positive attitudes toward the relative. In addition, among less burned-out relatives, a focus on the person and supporting them, rather than on the “problem” or difficulties to be eliminated, is evident.
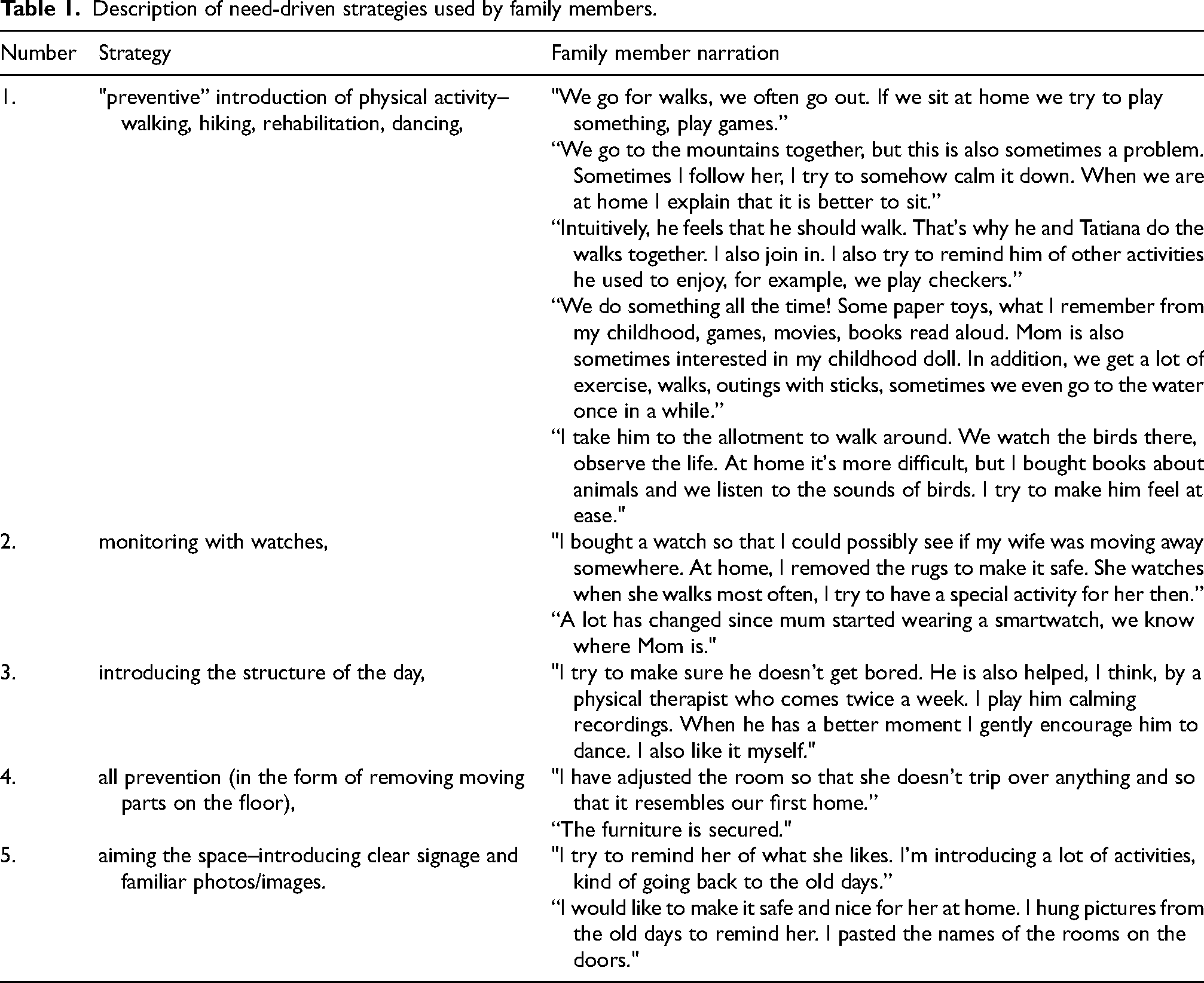
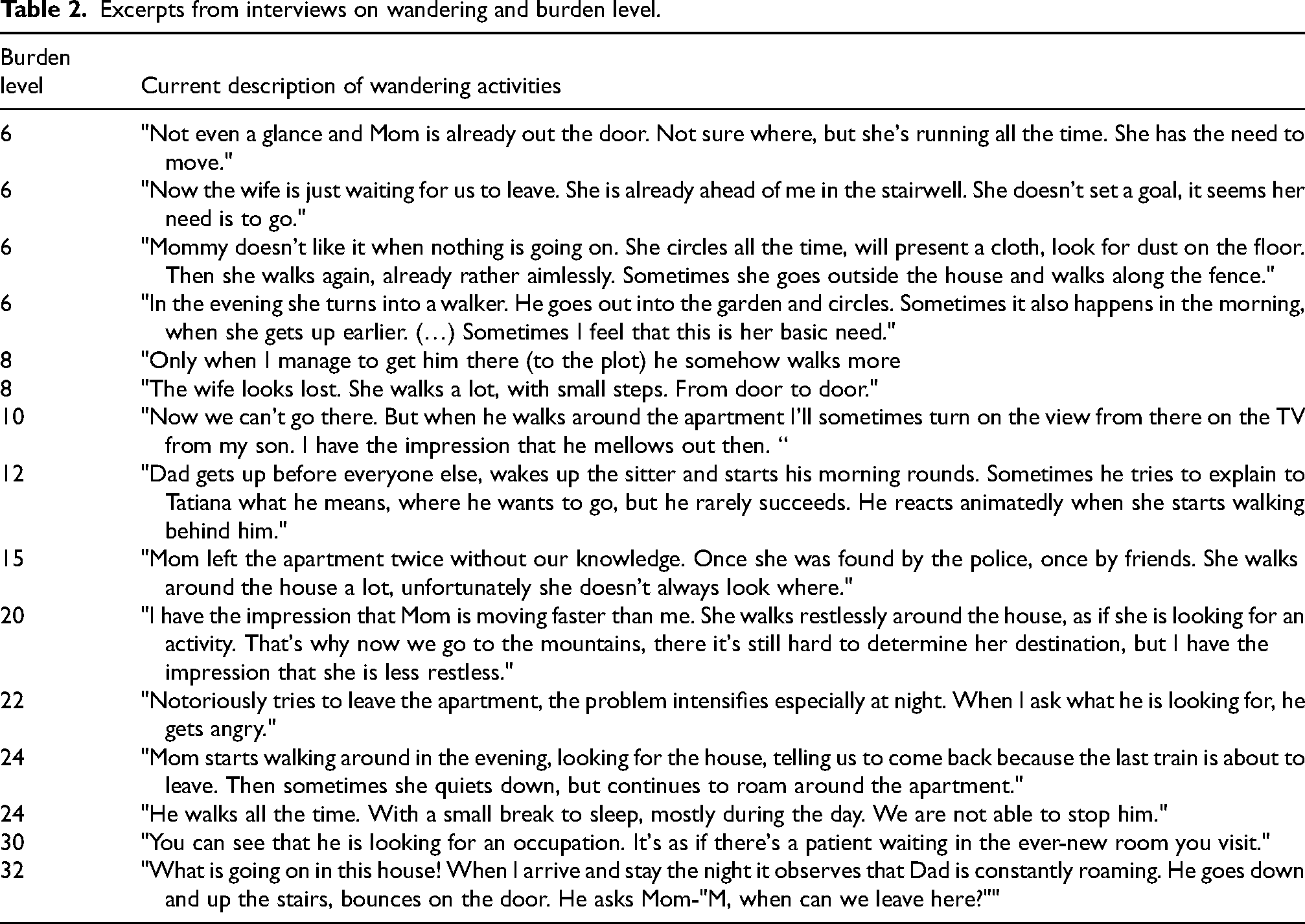
Those with scores around 20 (increased burden) tended to use less proactive supporting strategies. They focused mainly on the challenges they perceived to be around wandering (see Tables 1 and 2). They did not follow the person when they were wandering, and their main strategies were attempts to establish routines and distractions, often unrelated to the need itself (such as trying to distract themselves with food). In addition, more burdened relatives emphasized their own negative emotional reactions–anger, raising their voices or helplessness in the face of the situation.
Description of need-driven strategies used by family members.
Excerpts from interviews on wandering and burden level.
Only among relatives with higher levels of burden (over cut off for burnout—a specific threshold on a questionnaire used to categorize participants’ results into distinct levels of severity, effectively acting as a “diagnostic line” that distinguishes between a manageable level and a clinically significant degree of burden that may require professional intervention.) did a strategy emerge involving attempts to use pharmacological support to solve the problem of increased mobility needs.
Discussion
The study provided information on the relationship between the level of burden among family members of people with AD and their perception of their loved ones’ need to wander and how they support it. Relatives with lower levels of burden were more likely to use need driven terminology instead of negative terms such as “problem,” “difficulty” or “disorder.” They were more likely to show greater understanding of the need or desire to wander, seeing it as an expression of the needs of a person with cognitive impairment. They were also more prone to actively support wandering as a part of their loved ones’ nature, personality and often main life element. Previous research has shown that family members’ professional and emotional burnout is strongly related to their ability to cope with new situations.33,39 Care partners experiencing lower levels of stress and less burden are more likely to perceive their loved ones’ behaviors as normal, need driven and support it, preventing rapid negative emotional reactions and less patience in relationships. 25 The results of the present study are consistent with these observations, suggesting that family members with lower levels of burden are more likely to use the language of needs and understanding. Furthermore, participants with lower burden tended to mention more protective factors related with resilience and positive adaptation strategies as congruent with previous observations.40,41
Family members who reported low burden levels were those who supported wandering in the most flexible and positive manner. This approach is consistent with research showing that reducing stress, burden and burnout among care partners leads to an improvement in their ability to cope with new life situations, which directly translates into improved quality of care. 42
The results indicate that low or high reported burden and burnout among family members may not only be a reaction to the intensity of care, their own psychological and medical conditions, but also a factor in how they interpret and support the unmet needs. This means that interventions to support families should take into account both reducing burden and burnout levels and providing tools and ideas of how to support unmet needs of loved ones. 43 Current research on family members support programs indicates that holistic care partner support programs such as Empowerment 44 has been able to reduce the burden and increase the health functioning outcomes of older adults with AD.
The levels of burden identified in this study reflect a global phenomenon documented in recent literature. For instance, Rahman et al. 40 utilized the ZBI to demonstrate that the psychological impact of supporting a loved one with AD is a universal experience across diverse cultural contexts, emphasizing the urgent need for inclusive behavioral support strategies. Furthermore, our findings regarding the tension between ensuring a loved ones safety during wandering and the family members own well-being mirror the observations of Shi et al. 41 They noted that many family members find it uneasy to balance keeping their relative safe with taking care of themselves
The practical implications of the findings focus on the need to support family members and facilitate the implementation of existing good practices. This can be achieved through educational programs and by sharing positive experiences of family members as speakers.45,46
It has been proven to be successful in the context of supporting family members diagnosed with dementia, knowledge about the diagnosis, the use of health and community resources and support groups.45,46 The educational component should include workshops focusing on techniques for stimulating and ensuring safety during wandering and on providing a safe, adapted space for people with cognitive disability. In addition, it would be valuable to offer emotional support to entire families to prevent burnout.44–46 Combining support and empowerment of care giving partners could improve the quality of relationships and extend the time during which family members are able to effectively connect with their loved ones. 47
The results of the study support the need for further research to better understand the dynamics of family support and its impact on quality of relationships and the health of family members. In particular, future research should focus on long-term monitoring of changes in the dynamic of support to meet individual needs (both of family members and people with cognitive impairment).
We propose creating an intervention that will fully include a person's Life History into the management of wandering offers more than just a safety protocol; it provides ‘cognitive relief’ by transforming a challenging behavior into a meaningful narrative. 48 This person-centered approach honors the individual's identity and past, potentially fostering a more sustainable balance for the caregiver by reducing the subjective weight of the role.
Apart from in-depth interview with family members and people with dementia themselves, undertaken actions should focus on both–person's life history and key values. Meaningful non-pharmacological approaches support meeting the needs one has, e.g., wandering by engaging individuals in activities that foster purpose and dignity.49,50 Dimitriou et al. 51 emphasize that effective management requires a collaborative, multidisciplinary framework not limited to just one specialty. Recent person-centered methods, such as Montessori-based interventions, focus on an individual's remaining abilities and interests to promote positive outcomes. 52 Crucially, clinical educators must train family members in specialized communication techniques and the recognition of wandering signals. This professional support of family members not only improves the quality of life for the individual but also serves as a critical buffer against the progression of caregiver burden into clinical burnout. 53
Recommendations for family members: While supporting your family member, pay attention to needs one may have. Don’t stop on symptoms. Remember to incorporate one's life history into the whole process. It enables to engage loved ones in a meaningful manner in both everyday and “artistic” engagement. Those activities should be built into a structure, which gives more safety. Remember about environmental adaptations like visual cues, GPS and more. Engage as many senses as possible—do not focus solely on one. Do not hesitate to ask for professional support, e.g., from psychologists, physiotherapists.
Recommendations for professionals working with family members (psychologists, physiotherapists, doctors, nurses, professional caregivers, occupational therapists): During supporting of family members, focus on teaching effective strategies, show inspirations and how to search for valuable strategies on their own. Focus on relation rather than on illness and symptoms. Try to manage unmet needs of both parties (family member and person diagnosed with dementia). Use psychoeducation and adaptive coping strategies. Focus on strengthening self-efficacy of family members.
Limitations
All participants were care partners of people diagnosed with AD and living in home settings, which may limit the generalizability of the results to relatives of people with other forms of cognitive impairment or to caregiving contexts outside of home-based family care (e.g., institutional or community-based settings).
The use of structured interviews and the ZBI may not capture the full complexity of families’ emotional and psychological experiences. A more comprehensive approach, including observational data or psychological assessments, could provide a richer understanding of the multifaceted nature of care partners’ burden and burnout and should be taken into account whilst planning future research.
Implications for social care practice
From a social care perspective, the findings highlight the importance of supporting family members not only through practical guidance but also through interventions aimed at reducing burden. Lower levels of caregiver burden were associated with greater use of person-centered, need-driven strategies that supported wandering as a meaningful activity rather than a behavioral problem.
Conclusions
The results of the present study confirm the impact of family members’ burden levels on their perceptions and support of behaviors related to wandering by their loved one. Relatives with lower levels of burden more often analyzed the reasons for their loved ones’ need to move and tried to understand them, perceiving them as an expression of basic needs, and tried to support them rather than restrain them. In contrast, relatives with higher levels of burden were more likely to identify wandering as a problem that needed to be addressed. These findings highlight the need for a comprehensive approach to support family members, taking into account both the practical and emotional aspects of caring for people with cognitive impairment. Further research is warranted, particularly in the area of educating caregivers about strategies for supporting individuals who wander and implementing regular, structured interventions aimed at improving their health.
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Silesian Medical University (BNW/NWN/0052/KB/266/23).
Consent to participate
All participants, or their legally authorized representatives where appropriate, provided informed consent prior to participation. Consent was written or verbal recorded and documented according to ethics committee requirements.
Consent for publication
Consent to publish anonymized data obtained during interviews, including anonymized excerpts from participants’ narratives where applicable, was obtained from all participants or their legally authorized representatives. Special consideration was given to ensuring the dignity, autonomy, and comfort of people living with dementia. Capacity to consent was assessed and monitored throughout the study, and participants were reminded that they could withdraw at any time without consequence.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study did not receive any grant from funding agencies in the public, commercial, or not-for-profit sectors. The article publication charge was covered by Jagiellonian University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.