
Abstract
Background
Dementia is a growing health challenge in the Asia-Pacific region, where family caregivers experience substantial burden shaped by cultural expectations of filial piety. Psychoeducational interventions are recommended non-pharmacological strategies to support caregivers; however, no systematic review has evaluated their effectiveness specifically within Asian populations. Understanding their effectiveness is critical given cultural factors influencing caregiving experiences in Alzheimer's disease and other dementias.
Objective
To synthesize the effectiveness of psychoeducational interventions in reducing caregiver burden among Asian family caregivers of people with dementia, describe intervention characteristics, and identify factors influencing effectiveness.
Methods
This systematic review followed PRISMA 2020 guidelines. CINAHL, Cochrane, Embase, PubMed, PsycINFO, Scopus, and Web of Science were searched for studies published between 1 January 2012 and 1 November 2025. Two investigators independently conducted study selection, quality appraisal using the Joanna Briggs Institute critical appraisal tool, and data extraction. A narrative synthesis was conducted due to study heterogeneity.
Results
Ten randomized controlled trials were included. Interventions varied in conceptual theories, delivery mode, format, and duration. Six studies reported significant reductions in caregiver burden. More effective interventions were delivered via telephone, provided individually, and implemented over three months. Some studies also reported improvements in self-efficacy, depression, perceived stress, and distress. None incorporated gender-sensitive approaches in intervention design or evaluation.
Conclusions
Psychoeducational interventions show promise in alleviating burden among Asian family caregivers of people with dementia, including those with Alzheimer's disease. Tailoring delivery mode, format, and duration may optimize effectiveness. Future research should include diverse Asian populations and incorporate gender-sensitive approaches.
Keywords
Introduction
Dementia poses a significant global health challenge, with an exponentially increasing prevalence, particularly in the Asia-Pacific region. In Singapore, one in ten people over the age of 60 have dementia, and this prevalence is projected to rise as a quarter of the population will be over 60 by 2030. 1 The escalating prevalence implies that more individuals will need to assume the role of a family caregiver to people with dementia.
Singapore is a Southeast Asian country with a multi-racial society comprising Chinese, Malay, and Indian communities. Many people in these Asian communities hold traditional beliefs in filial piety and the responsibility to care for one's parents. 2 Consequently, 80% of people with dementia in Singapore are cared for by family members within the community. 3 However, these caregivers face numerous challenges in their caregiving journey.
Dementia presents a complex and demanding experience for both the diagnosed individuals and their caregivers. As cognitive abilities decline and behavioral patterns change, caregivers encounter a significant increase in responsibilities, leading to heightened dependence, stress, and emotional burden. 4 Compared to caregivers of individuals without dementia, dementia caregivers experience greater levels of stress, burden, susceptibility to depression, and cardiovascular diseases. 5 They often make sacrifices, such as leaving their jobs or adjusting social commitments, to cater to the evolving needs of the people with dementia. 6 In some cases, overwhelmed caregivers face an increased risk of transitioning to nursing home care, adding pressure on already stretched healthcare systems. 7
The adverse effects of caregiving underscore the urgent need for proactive measures from public health professionals and policymakers. Implementing feasible interventions that prioritize caregiver support and well-being is crucial. By providing necessary assistance and resources, caregivers may be better equipped to navigate their caregiving journey and mitigate the negative impacts on their health and quality of life.
Psychoeducation is a highly recommended non-pharmacological intervention to minimize the adverse effects of caregiving. It involves educational programs covering various topics such as information about dementia, skills training, and advice on self-care. 8 The aim is to improve caregivers’ knowledge and skills in providing care for people with dementia while also addressing their own mental health and emotional well-being. Globally, dementia caregivers are supported through diverse services including day care centers, respite care, and Alzheimer Cafés.9–11 Healthcare systems vary substantially in how they organize and fund caregiver support, 12 with comprehensive frameworks in countries like Italy integrating psychoeducation into national care pathways. 13 Cultural factors significantly influence caregiver service preferences and effectiveness, with Asian systems emphasizing family-based care rooted in filial piety versus Western systems with greater institutional care utilization.
Psychoeducational interventions often utilize different conceptual theories, including Cognitive Behavioral Therapy (CBT), Stress Appraisal and Coping Theory, Mindfulness-Based Cognitive Therapy, Behavioral Activation, and Benefit-Finding Therapy. These theories provide a foundation and framework for understanding the problem and offer evidence-based strategies to address them. 14 Each theory provides distinct mechanisms: CBT modifies maladaptive thoughts and behaviors; Stress Appraisal and Coping Theory enhances appraisal and coping resources; Mindfulness-Based Cognitive Therapy develops present-moment awareness and acceptance; Behavioral Activation increases meaningful activities and reduces avoidance; Benefit-Finding Therapy promotes identification of positive aspects and growth. These theoretical foundations may interact with delivery characteristics, with CBT's skill-building may suit individual formats, while mindfulness practices may benefit from group settings providing peer support. 14 The validated therapeutic approaches lend credibility to the interventions and provide a benchmark for expected outcomes. By drawing on these established theories, researchers can offer sound explanations for the effectiveness of the interventions and evaluate their positive impacts on caregivers of people with dementia.
Psychoeducational interventions can be categorized as either active or passive. Passive psychoeducation provides caregivers with educational materials to read at their convenience, while active psychoeducation involves the dynamic participation and collaboration of caregivers, leading to frequent interactions with healthcare professionals. 15 Active psychoeducation can be delivered in-person, virtually, or over the telephone. The mode of delivery may influence the effectiveness of the intervention. A systematic review highlighted that internet-based interventions were most effective in reducing stress and depressive symptoms but had no effect on anxiety, burden, self-efficacy, or quality of life for family caregivers. 16
Additionally, the format of the intervention, whether conducted individually or in groups, can also impact its effectiveness. The systematic review showed evidence that, compared to individual-based interventions, group-based interventions were more effective in reducing anxiety, depression, insomnia, and burden, as well as improving self-efficacy and quality of life for family caregivers. 4 Group formats may benefit anxiety and depression through peer support, normalization of challenges, and social learning. 4 Internet-based interventions offer accessibility advantages but may require greater technological literacy, with effectiveness varying by outcome, as they are effective for stress and depression but not for burden or self-efficacy, suggesting some outcomes require direct human interaction. 16 Telephone delivery combines convenience with personal contact, potentially explaining broad effectiveness. Duration and intensity influence sustainability of behavior change, with short-term interventions providing immediate relief but potentially lacking lasting impact without ongoing support.
While previous systematic reviews have explored the effectiveness of psychoeducational interventions on a global scale, there is no known systematic review examining the effectiveness of these interventions specifically in the Asian context. The absence of such a review limits the ability to further develop generalizable evidence-based policies and practices that are specifically tailored to Asian communities. Therefore, this review aims to address this gap in the literature.
Aims
The aim of this systematic review was to synthesize the effectiveness of psychoeducational interventions in reducing caregiver burden amongst Asian family caregivers of people with dementia.
The specific objectives were:
To describe the characteristics of the psychoeducational interventions identified; To assess the effectiveness of psychoeducational interventions in reducing caregiver burden amongst Asian family caregivers of people with dementia; To identify the factors that influence the effectiveness of the psychoeducational interventions in reducing caregiver burden amongst Asian family caregivers of people with dementia.
The findings from this review will hopefully inform healthcare professionals and policymakers in Asia to understand, tailor, and implement similar psychoeducational interventions to address the specific needs of their local populations; thereby, improving the support and caregiving experience for family caregivers of people with dementia.
Methods
A systematic review of published articles from 1 January 2012 to 1 November 2025 was conducted. This review adhered to the PRISMA 2020 framework 17 to ensure completeness, transparency, and clarity of the review process. The study protocol, Registration Number: CRD42023493206, was registered on the Prospective Register of Systematic Reviews (PROSPERO) to ensure transparency and prevent unplanned duplications of systematic reviews. 18 The use of both PRISMA 2020 framework and PROSPERO minimized reporting bias and strengthened methodological transparency, ensuring comprehensive reporting of this systematic review.
Search strategies
A comprehensive literature search was performed across multiple databases, including CINAHL, Cochrane Library, Embase, PubMed, PsycINFO, Scopus, and Web of Science. The search terms were based on the “Population, Intervention, Comparison, and Outcome (PICO)” framework and were identified as caregivers, dementia, psychoeducation, and caregiver burden. The search terms and strategies for the various databases were developed systematically and underwent an independent review to ensure their appropriateness and comprehensiveness prior to implementation (details in the Supplemental Material).
Inclusion and exclusion criteria
The “Population, Intervention, Comparison, Outcome and Study (PICOS)” framework was utilized to establish the inclusion and exclusion criteria. Publications that fulfilled all five domains of the PICOS design were included in this systematic review, while those that did not were excluded.
The inclusion criteria were as follows: (1) Asian family caregivers of people with dementia, (2) Psychoeducational interventions targeted at family caregivers of people with dementia, (3) Comparison group, (4) Studies that measured burden and other psychological outcomes using reliable and validated tools, (5) Randomized controlled trials (RCTs) conducted in Asia. All studies included had to be published in English, between 1 January 2012 and 1 November 2025.
Quality appraisal
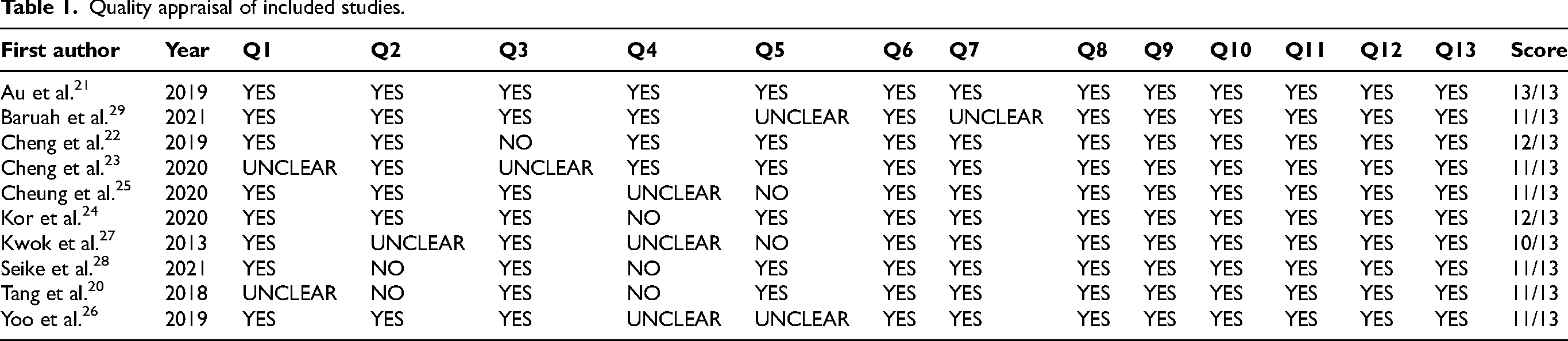
All included articles underwent appraisal using the Joanna Briggs Institute (JBI) critical appraisal checklist. 19 This tool was employed to assess how thoroughly an article addressed the potential for bias in the study's design, methodology, and analysis. The appraisal process was independently conducted by two investigators. Discussions between the two investigators took place after each study appraisal to ensure consistency and to resolve any discrepancies in results. In the event that a disagreement could not be resolved, the third investigator was on standby to evaluate the quality of the studies. Studies that did not meet at least 70% of the criteria specified in the JBI critical appraisal checklist were considered to have methodological flaws and were not included in the review (Table 1).
Data extraction
Extraction of data from each study was independently completed by two investigators. A third investigator cross-checked all the extracted data and resolved any inconsistencies or conflicts during a team discussion. The extracted information included authors, year of publication, country, study design, sample size, intervention details, measurement instruments, and results.
Data synthesis
Characteristics of all studies, including the country, intervention, and comparison group, were summarized. Additionally, psychoeducational interventions were elaborated upon, covering their conceptual theories, mode of delivery, format, and duration. However, due to the heterogeneity in the outcome measurement tools and intervention characteristics across the studies, a quantitative meta-analysis was deemed not suitable for this systematic review. Therefore, to ensure a robust and informative analysis, a narrative synthesis approach was employed to comprehensively examine the reviewed studies.
Results
Search results
A total of 1938 articles were identified based on the search terms. This included 236, 208, 215, 304, 287, 378, and 310 articles from CINAHL, Cochrane, Embase, PubMed, PsycINFO, Scopus, and Web of Science, respectively. After removing 943 duplicates, 995 articles were screened based on title and abstract. Subsequently, 978 articles were excluded because they were not related to the topic. Following this, the inclusion and exclusion criteria were applied to assess 17 full-text articles. A total of five articles were excluded because four were pilot studies and one study was partially conducted in Asia and Australia. The remaining 12 articles underwent critical appraisal using the JBI critical appraisal tool, where two articles did not meet at least 70% of the criteria. Consequently, ten articles were included for this review. The study selection process was summarized and depicted in Figure 1.
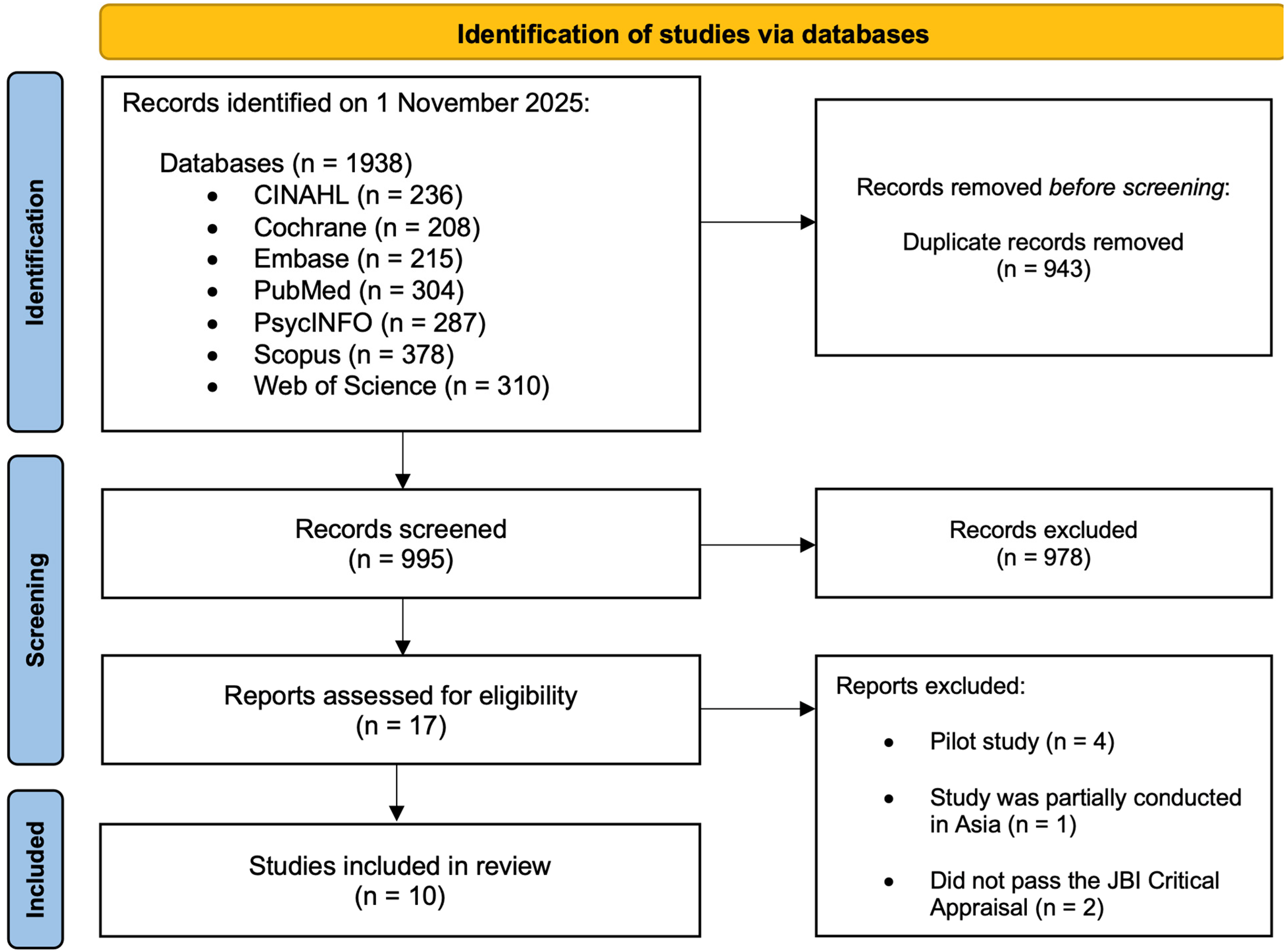
The PRISMA flow diagram to visually summarize the study selection process.
Characteristics of selected studies
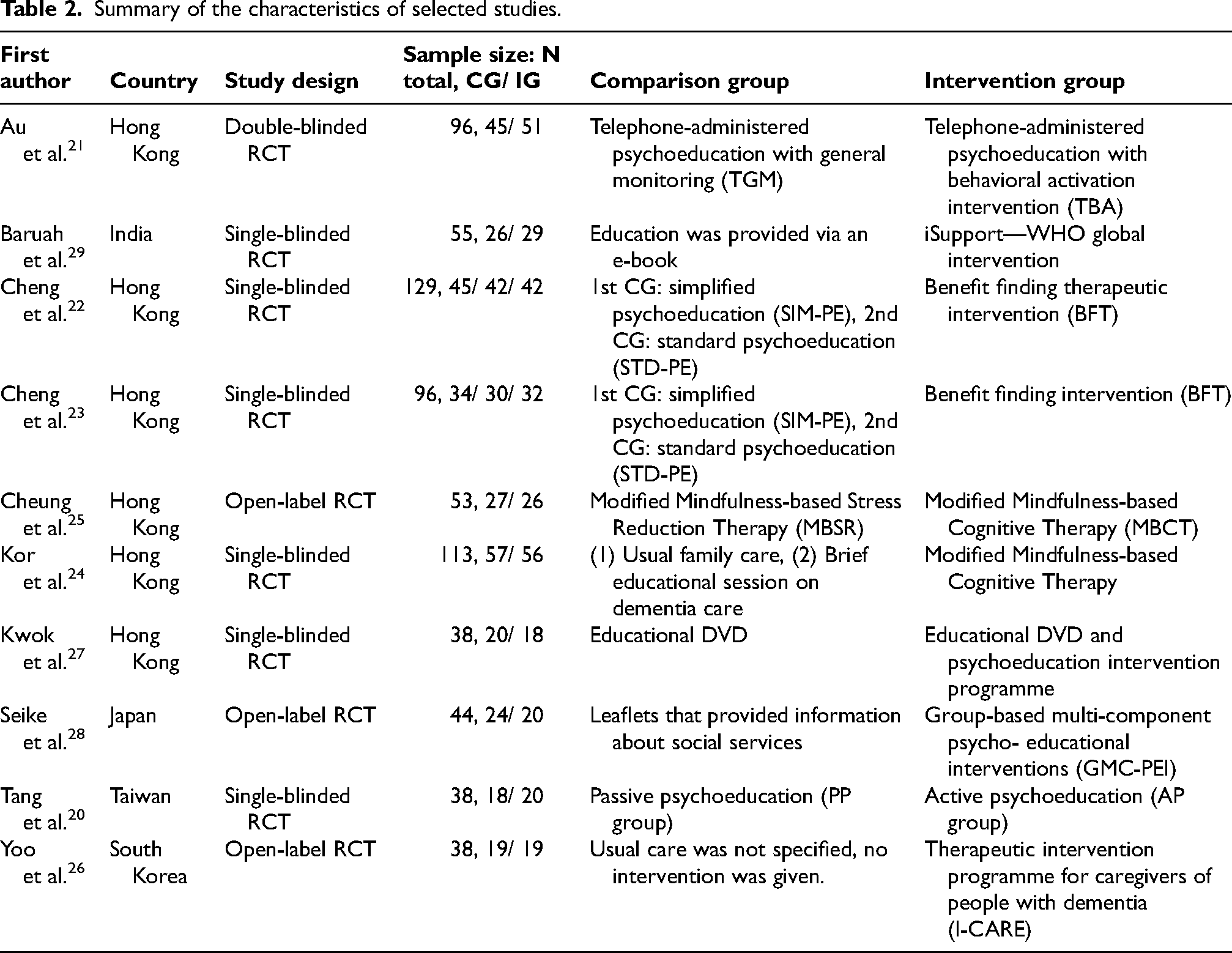
The included studies were conducted across various regions of Asia, including Hong Kong (n = 6), India (n = 1), Japan (n = 1), South Korea (n = 1), and Taiwan (n = 1). All ten studies were RCTs, with study designs classified as double-blinded (n = 1), single-blinded (n = 6), or open-labeled (n = 3). The sample sizes of these studies ranged from 38 to 129 participants.
These studies shared a common aim to investigate the impact of psychoeducational interventions on family caregivers of people with dementia. However, the intervention designs and comparison groups differed across all studies (Table 2).
Quality appraisal of included studies.
Summary of the characteristics of selected studies.
Conceptual theories and characteristics of interventions
Among the ten RCTs included, six studies employed a singular conceptual theory,20–25 while four studies integrated multiple theories.26–29 These theories subsequently informed the diverse psychoeducational interventions used in terms of mode of delivery, format, and duration (Table 3). Figure 2 summarizes the different interventions characteristics used.
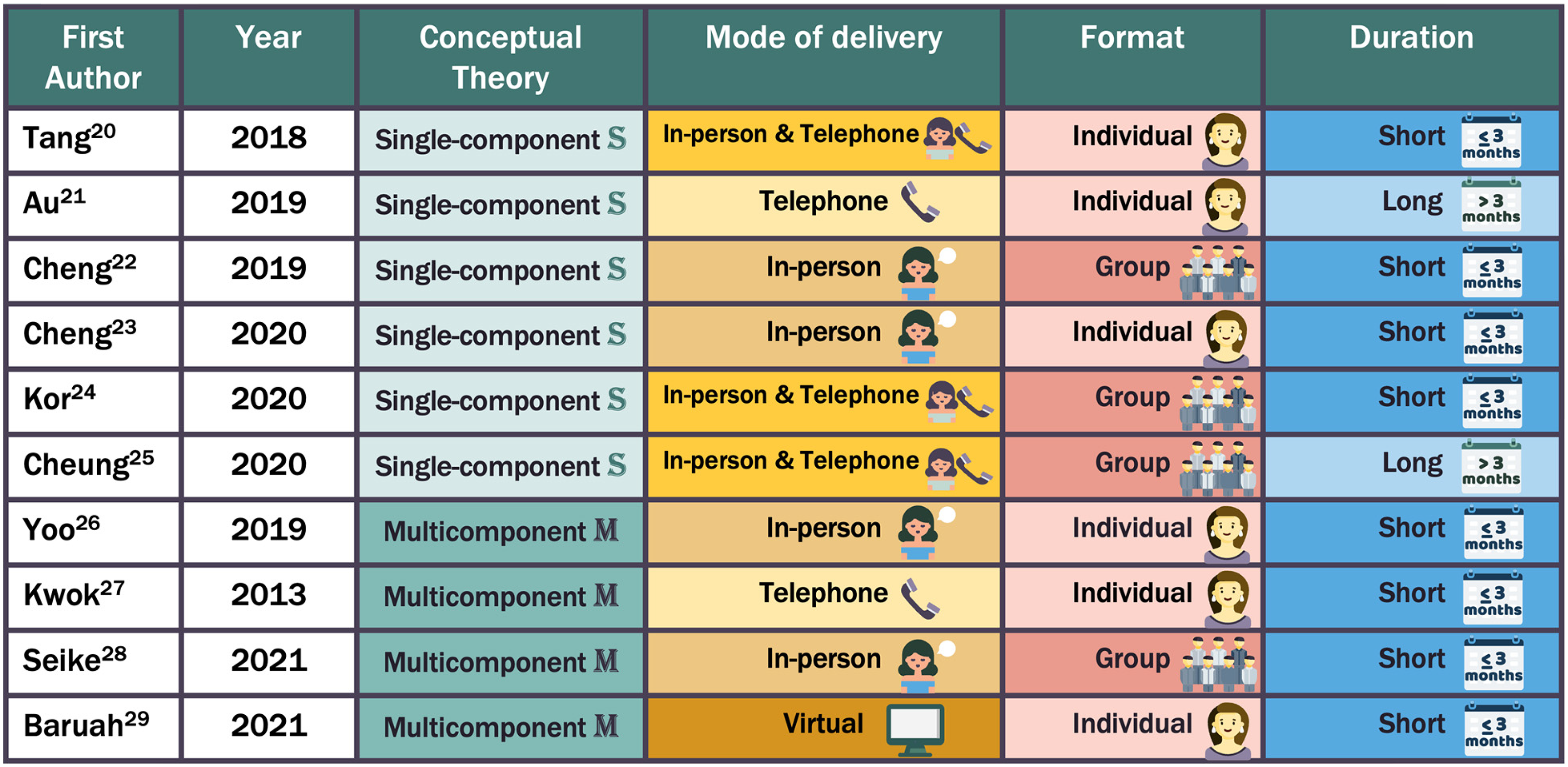
Summary of the intervention characteristics.
Summary of the characteristics of interventions.
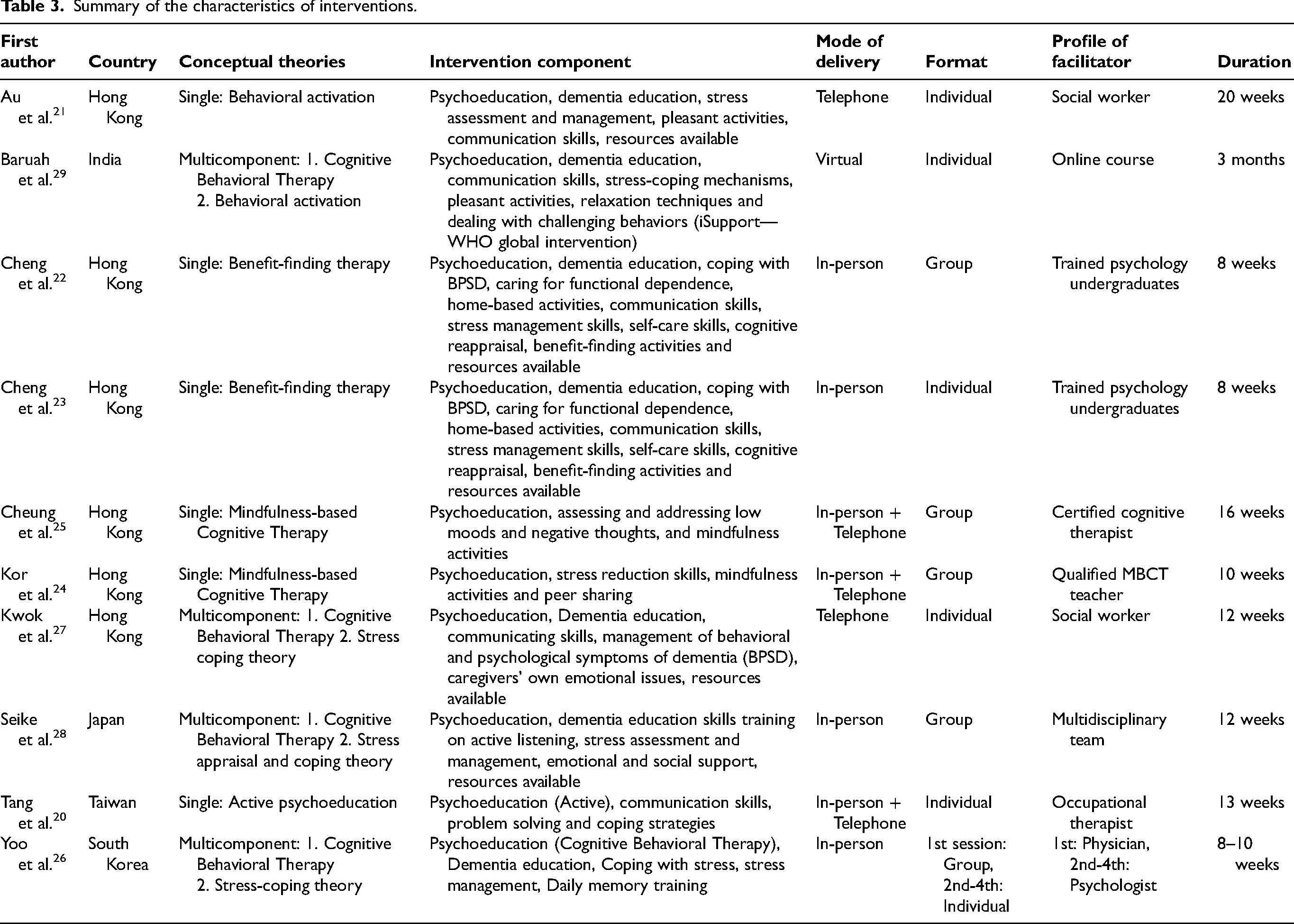
Single conceptual theory
Out of the six studies that utilized only one conceptual theory, two studies employed Benefit-Finding Therapy,22,23 two studies used Mindfulness-Based Cognitive Therapy,24,25 one study utilized Behavioral Activation, 21 and another study only used active psychoeducation. 20
Based on the conceptual theories employed, the interventions were delivered through various modes. Two studies’ interventions were conducted in-person,22,23 and one study was done over the phone. 21 The remaining three studies had a combination of both modes, with additional telephone follow-up calls after the in-person sessions to enhance adherence to the prescribed home-based psychoeducational program.20,24,25
Three studies utilized group-based interventions,23–25 while three studies facilitated their interventions individually for each participant.20,21,23 The facilitators’ profiles varied across studies. Two studies had trained psychology undergraduates,22,23 two studies employed certified cognitive therapists,24,25 one study involved an occupational therapist, 20 and the other study used a social worker. 21
The majority of the studies’ interventions were short-term, concluding within three months,20,22–24 while two studies had long-term interventions extending more than three months.21,25
Multicomponent conceptual theory
Among the four studies that utilized more than one conceptual theory, three studies employed Cognitive Behavioral Therapy and the Stress, Appraisal and Coping Theory,26–28 and the other study used Cognitive Behavioral Therapy and Behavioral Activation. 29
The mode of delivery of the interventions varied despite utilizing similar conceptual theories. two studies conducted the intervention in-person,26,28 one study facilitated the intervention over the telephone, 27 and the other study was done virtually online. 29
One study utilized group-based interventions, 28 while two studies conducted the interventions individually for each participant.27,29 Notably, one study had a combination of both, where the first session was conducted in a group format and subsequent sessions were facilitated individually. 26 The facilitators’ profiles differed across studies. Two studies utilized a multidisciplinary team,26,28 and one study involved a social worker. 27 The other study had no facilitator as it was an online course. 29
All four studies were short-term interventions that concluded within three months.26–29
Characteristics of comparison groups
The ten RCTs employed a variety of comparison groups. Two studies compared the intervention to usual care.24,26 Three studies provided educational information to the comparison group delivered through different formats: Digital Versatile Discs (DVDs), 27 leaflets 28 and e-Books. 29 The remaining five studies used alternative forms of psychoeducation as the comparison group.20–23,25 These included one study using passive psychoeducation, 20 another using telephone-administered psychoeducation with general monitoring, 21 one study employing modified mindfulness-based stress reduction therapy, 25 and two studies utilizing simplified psychoeducation for the first comparison group and standard psychoeducation for the second.23,25
Characteristics of participants
In all ten RCTs, the participants consisted of Asian family caregivers of people with dementia. Among these studies, nine had predominantly female caregivers,20–28 while one study primarily involved male caregivers. 29
The age distribution of these caregivers was predominantly above 41 years old. Specifically, two studies had a majority of participants aged between 41 to 50 years old,27,29 five studies had a majority aged between 51 to 60 years old,20–23,25 and the remaining three studies had a majority aged between 61 to 70 years old.24,26,28
The relationship between the caregivers and the people with dementia was primarily that of children caring for their parents. Nine studies reported that the majority of their participants were children of the people with dementia, while one study's participants were predominantly spouses. 26
Regarding educational background, caregivers were generally well-educated, with most having at least a secondary school education. Eight studies indicated that the majority of participants had attained a secondary education level, while two studies primarily involved participants with tertiary education levels.25,29
All participants across the ten studies had at least two years of caregiving experience. Among these, five studies reported a majority of caregivers with two to three years of experience,22,23,26,28,29 while one study reported 3.1 to 4.9 years, 21 another study reported five to six years, 24 and lastly, one study indicated eight to nine years. 25 Two studies did not specify the participants’ years of caregiving experience.20,27 Characteristics reported above represent intervention groups; comparison groups showed similar demographic distributions where reported, supporting randomization procedures.
Regarding the burden experienced by caregivers, eight studies found that most participants had baseline scores indicating mild to moderate burden.21–23,25–29 The remaining two studies reported moderate to severe burden.20,24
Regarding gender-sensitive approaches, none of the ten included RCTs explicitly adopted a gendered or gender-sensitive framework in the design, delivery, or evaluation of their psychoeducational interventions. While nine studies reported predominantly female caregiver samples and one study 29 had a predominantly male sample, no study specifically tailored intervention content or delivery to address gender-specific caregiving experiences, nor did any study conduct gender-stratified analyses of intervention effectiveness.
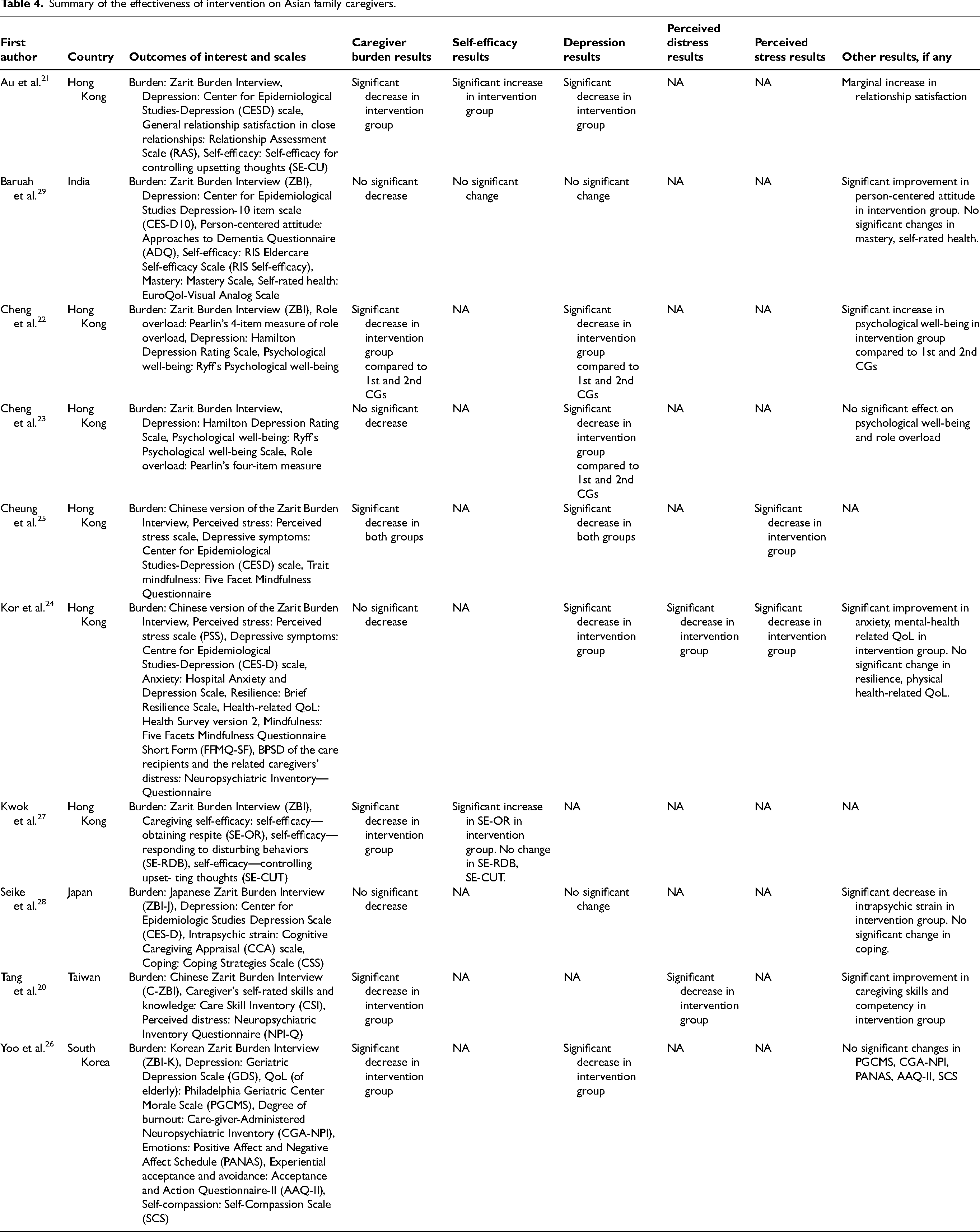
Effectiveness of interventions on Asian family caregivers
The ten RCTs varied in their outcomes of interest and instruments used to measure these outcomes. Similar outcome measures across studies were synthesized into three categories: (1) Caregiver burden, (2) Self-efficacy, and (3) Mental health (Table 4). Figure 3 summarizes the effectiveness of interventions for the three categories.
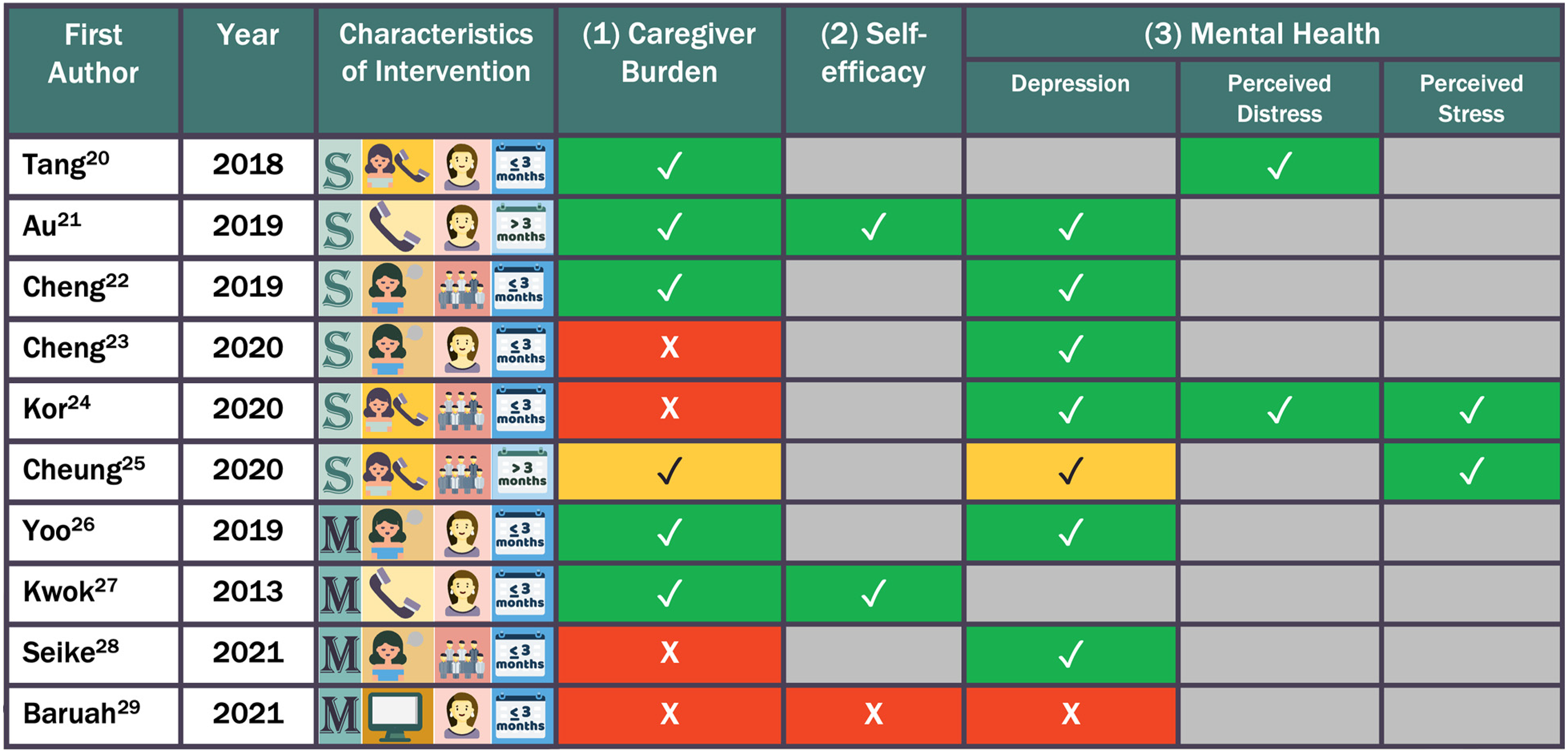
Summary of the effectiveness of interventions.
Summary of the effectiveness of intervention on Asian family caregivers.
Caregiver burden
All ten RCTs measured caregiver burden using the Zarit Burden Interview. Five studies reported significant burden reduction,20–22,26,27 while five found no significant difference.23–25,28,29
Telephone-delivered interventions showed consistent effectiveness: both studies reported significant burden reduction (p < 0.001 21 ; p < 0.01 27 ), both used an individual format, and differed only in theoretical grounding; where, Behavioral Activation was used over 20 weeks 21 versus CBT and Stress Appraisal and Coping over 12 weeks. 27
Among in-person studies, two of four reported significant burden reduction. Cheng et al. 22 used a group format grounded in Benefit-Finding Therapy over eight weeks (p = 0.05 and p = 0.048 vs. both comparison groups), while Yoo et al. 26 used a hybrid format (first session group, subsequent sessions individual) grounded in CBT and Stress Appraisal and Coping over eight to ten weeks (p < 0.01). The two in-person studies that found no significant difference23,28 were also short-term and group-based.
Among in-person with telephone follow-up studies, one reported significant burden reduction (p < 0.05), 20 delivered individually using active psychoeducation over 13 weeks. Cheung et al. 25 demonstrated within-group improvements in both groups but no between-group difference (p = 0.18), likely because the comparison condition (modified mindfulness-based stress reduction) also contained psychoeducational components; this study used a group format over 16 weeks. Kor et al. 24 found no significant burden effect, also using a group format over ten weeks.
The single virtual delivery study 29 showed no significant burden reduction, delivered individually without a human facilitator using CBT and Behavioral Activation over three months.
Self-efficacy
Only three out of ten RCTs measured self-efficacy.21,27,29 Each study employed a different instrument, including the Self-Efficacy for Controlling Upsetting Thoughts scale, 21 the RIS Eldercare Self-Efficacy Scale, 29 and domain-specific self-efficacy measures assessing obtaining respite, responding to disturbing behaviors, and controlling upsetting thoughts. 27
Among the six studies that utilized a single conceptual theory, only one study measured self-efficacy. 21 This study reported a significant increase in self-efficacy compared to the comparison group.
Out of the four studies that utilized multicomponent conceptual theories, two studies measured caregiving self-efficacy.27,29 One study showed a significant increase in self-efficacy compared to the comparison group, 27 while the other study found no significant difference. 29
Mental health
Among the ten RCTs, eight studies assessed depression using a range of instruments, including the Centre for Epidemiological Studies Depression Scale,21,24,25,28,29 the Hamilton Depression Rating Scale,22,23 and the Geriatric Depression Scale. 26 Perceived distress was measured in two studies using the Neuropsychiatric Inventory Questionnaire.20,24 Perceived stress was assessed in two studies using the Perceived Stress Scale.24,25
Among the five studies that utilized a single conceptual theory to assess depression, four reported a significant reduction in depression compared to the control group,21–24 while one found no significant difference. 25 Similarly, both studies that assessed perceived distress using a single conceptual theory20,24 showed significant improvements compared to the control group. Additionally, two studies that examined perceived stress24,25 also reported a statistically greater improvement in perceived stress compared to the comparison group.
Among the four studies that utilized multicomponent conceptual theories, three measured depression. Of these, two found a significant reduction in depression compared to the control group,26,28 while one reported no significant difference. 29 All four studies did not measure perceived distress and perceived stress.
Factors influencing the effectiveness of interventions
The effectiveness of psychoeducational interventions in reducing caregiver burden and other psychological outcomes is influenced by various intervention characteristics. The following section elaborates on other influencing factors apart from conceptual theories.
Mode of delivery
Telephone
Both studies utilizing telephone-administered interventions reported significant burden reduction, with reported effects of p < 0.001 21 and p < 0.01. 27 Improvements in self-efficacy were reported in both studies across different domains.21,27 One study reported significant improvement in self-efficacy for controlling upsetting thoughts (p < 0.01), 21 while another study reported improvement in self-efficacy for obtaining respite (p = 0.05), although no significant differences were observed for responding to disturbing behaviors or controlling upsetting thoughts. 27 One study measured depression and found significant reduction, with reported effects of p < 0.001. 21 Neither study measured perceived distress or perceived stress.
In-person
Two of the four studies found significant burden reductions, with reported effects of p = 0.05 and p = 0.048 compared with simplified and standard psychoeducation respectively, 22 and p < 0.01, 26 while two studies found no significant differences.23,28 All four studies showed significant depression reduction.22,23,26,28 Reported effects included p < 0.001 compared with both comparison groups, 22 p < 0.001 and p = 0.002 compared with simplified and standard psychoeducation respectively, 23 and p < 0.05. 26 One study also demonstrated improvement, although specific statistical values were less clearly reported. 28 None of these studies measured self-efficacy, perceived distress, or perceived stress.
In-person with telephone follow-up
Two studies found burden reduction, with one study reporting p < 0.05 20 and another demonstrating significant within-group improvement; although, no significant between-group difference was observed, with p = 0.18. 25 Whereas in comparison, one study found no significant effect on burden. 24 Two studies measured depression and reported significant reductions, including p = 0.001 at Time 1 and p = 0.04 at Time 2, 24 and significant within-group improvements. 25 Both studies measuring perceived distress found significant reductions with reported effects of p < 0.05 20 and p = 0.003 at Time 1 and p = 0.04 at Time 2. 24 Both studies measuring perceived stress found significant reductions, including p = 0.02 at Time 1 and p = 0.03 at Time 2, 24 and p = 0.030 from Time 0 to Time 1. 25 None of the studies measured self-efficacy.
Virtual
The single study using virtual delivery showed no significant changes in burden, depression, or self-efficacy. 29 However, it found significant improvement in person-centered attitudes toward people with dementia, with p = 0.03. 29 This study did not measure perceived distress or perceived stress.
Format
Individual
Four of the six studies using an individual format showed significant burden reduction,20,21,26,27 while two found no significant difference.23,29 Three of the four studies measuring depression showed significant reductions, including p < 0.001, 21 p < 0.001 and p = 0.002 compared with both comparison groups, 23 and p < 0.05. 26 Whereas in comparison, one study found no significant difference. 29 Two studies measured self-efficacy and reported improvements, including p < 0.01 21 and partial improvement in obtaining respite at p = 0.05 only. 27 One study measured perceived distress and reported a significant reduction, p < 0.05. 20 None of the studies measured perceived stress.
Group
Two studies clearly showed burden reduction, including p = 0.05 and p = 0.048 compared with both comparison groups, 22 and significant within-group improvements although the comparison group also improved, 25 while two found no significant difference.24,28 All four studies showed significant reductions in depression, including p < 0.001, 22 p = 0.001 at Time 1 and p = 0.04 at Time 2, 24 as well as significant within-group improvements 25 and overall improvement. 28 One study measured perceived distress and reported significant reductions, with p = 0.003 at Time 1 and p = 0.04 at Time 2. 24 Two studies measured perceived stress and reported significant reductions, including p = 0.02 at Time 1 and p = 0.03 at Time 2, 24 and p = 0.030. 25 None of the studies measured self-efficacy.
Duration
Long-term
Both long-term interventions showed significant burden reduction, including p < 0.001 21 and within-group p = 0.014 for modified mindfulness-based cognitive therapy and p = 0.013 for modified mindfulness-based stress reduction, although the comparison group also improved. 25 Both interventions also demonstrated significant reductions in depression, including p < 0.001 21 and significant within-group improvements. 25 One study measured self-efficacy and reported significant improvement, with p < 0.01. 21 One study measured perceived stress and reported a significant reduction, indicating p = 0.030. 25 Neither study measured perceived distress.
Short-term
Four studies showed significant reductions burden reduction, including p = 0.05 and p = 0.048, 22 p < 0.01, 27 p < 0.05, 20 and p < 0.01, 26 while four found no significant difference.23,24,28,29 Five of the six studies measuring depression showed significant reductions, including p < 0.001, 22 p < 0.001 and p = 0.002, 23 p = 0.001 at Time 1 and p = 0.04 at Time 2, 24 p < 0.05, 26 and overall improvements were observed, 28 while one found no significant difference. 29 One study measured self-efficacy and reported partial improvement, with obtaining respite at p = 0.05 only and no significant difference observed for other domains. 27 Two studies measured perceived distress and reported significant reductions, including p < 0.05 20 and p = 0.003 at Time 1 and p = 0.04 at Time 2. 24 One study measured perceived stress and reported significant reductions, including p = 0.02 at Time 1 and p = 0.03 at Time 2. 24
Discussion
Overview
This is the first systematic review to examine the effectiveness of psychoeducational interventions in reducing caregiver burden among family caregivers of people with dementia in Asia. Of the ten RCTs included, six studies reported that psychoeducation was effective in reducing caregiver burden.20–22,25–27 Additionally, in the studies that measured self-efficacy, depression, perceived distress, and perceived stress, psychoeducation was found to have some positive effect on these outcomes. Rather than attributing effectiveness to any single characteristic, the findings suggest that outcomes reflect the interplay between mode of delivery, format, duration, and theoretical grounding, each of which is discussed below in relation to the others.
Role of professional delivery
Facilitator backgrounds varied substantially: social workers,21,27 certified therapists,24,25 occupational therapists, 20 trained undergraduates,22,23 multidisciplinary teams,26,28 and unguided online. 29 This heterogeneity represents a significant source of variation. Specialized training may enhance delivery of theory-specific techniques, as certified therapists achieved consistent depression reduction.24,25 Social workers’ holistic support and resource connection skills contributed to multi-outcome effectiveness.21,27 The unguided online intervention's lack of effectiveness 29 suggests human facilitation may be critical, though the comparison group also received materials. Future research should systematically examine optimal facilitator characteristics for different intervention types and cultural contexts, addressing training requirements and fidelity monitoring for scalable implementation.
Mode of delivery
Findings of this review indicate that interventions delivered via telephone yielded more effective results in reducing caregiver burden, depression, and improving self-efficacy compared to in-person or virtual modes. This effectiveness stemmed from the capability to support caregivers without the added inconvenience of traveling outside their home.21,27 These results align with previous reviews, which also highlighted that telephone-administered interventions were effective in reducing depression and anxiety. 4 This efficacy is attributed to healthcare professionals being able to provide immediate advice and support at the convenience of the caregiver's own time and place. 4 Direct human interaction, whether by telephone or in person, appears critical for effectiveness, and the virtual intervention's failure may reflect insufficient interactivity rather than inherent technology limitations. Future research should distinguish self-directed programs from technology-mediated human interaction (videoconferencing), which may combine accessibility with interpersonal support.
The advantage of telephone delivery was consistently observed when paired with individual format and adequate duration, suggesting these characteristics operate synergistically rather than independently.
Format
Findings from this review revealed that interventions delivered individually are more effective for Asian caregivers compared to group formats. This finding contrasts with previous global reviews, which highlighted that group format is a key component for the effectiveness of psychoeducational interventions. 4
This difference could potentially be attributed to Asian cultural norms surrounding privacy and personal boundaries. While collectivism and group harmony hold significant importance in Asian cultures, these values may translate into a preference for individual formats. 30 Individualized approaches may resonate better with the emphasis on personalized attention and maintaining family privacy. Moreover, Asian communication styles, often characterized by indirectness and context sensitivity, prioritize harmony and the avoidance of confrontation. 30 Consequently, individual formats are more conducive for caregivers to comfortably express their concerns, especially when dealing with sensitive topics involving their parents or loved ones. This underscores the values placed on respecting privacy boundaries and creating a safe space for open communication and sharing of personal information. 30 Therefore, tailoring psychoeducational interventions to individual formats could potentially offer a more effective approach to reducing caregiver burden in Asian societies.
However, findings from this review also suggest that group-based formats demonstrate consistent effectiveness in reducing depressive symptoms, indicating that peer support may offer distinct therapeutic benefits for emotional well-being that are not necessarily captured by burden-related outcomes. This pattern suggests that optimal intervention design may require variation in delivery format depending on the targeted outcomes or the adoption of hybrid approaches that integrate both individual and group components. Furthermore, the effectiveness of intervention formats may interact with their underlying theoretical frameworks. CBT and Behavioral Activation approaches may be particularly well suited to individual delivery, where personalized guidance and skills practice can be emphasized, whereas mindfulness-based interventions may derive added benefit from shared group experiences. From an implementation perspective, decisions regarding intervention format should balance effectiveness with cultural appropriateness, resource availability, and logistical feasibility. Individual formats often demand greater facilitator time, while group-based interventions may face challenges related to scheduling coordination and participant availability.
Format thus interacts with both delivery mode and theoretical approach, and should not be considered in isolation when designing interventions.
Duration of intervention
Findings from this review suggest that long-term interventions (lasting more than three months) are more effective in reducing caregiver burden, depression, perceived stress, and improving self-efficacy compared to short-term interventions (concluding within three months). This finding aligns with the notion that these positive outcomes require sustained intervention to achieve lasting behavioral and emotional changes.21,25 Short-term interventions might be insufficient to modify ingrained coping mechanisms or address deeply rooted burden, and stress accumulated over extended periods. Previous reviews reported that in cases where short-term interventions did show initial reductions in these outcomes, the positive results may diminish over time. 4 A possible reason could be the absence of ongoing reinforcement and support.
In contrast, long-term interventions offer the advantage of sustained professional healthcare support. This extended timeframe allows caregivers to gradually learn new coping skills, adapt their caregiving approach, and solidify positive changes in their emotional well-being.21,25 The ongoing support fosters the development of long-term resilience and empowers caregivers to manage the challenges of caregiving. Thus, long-term interventions are more suitable to accommodate the time needed for behavioral change and maintenance of a positive emotional state.
Duration should therefore be considered alongside delivery mode and format, as sustained contact across multiple modalities appears to be a common driver of lasting burden reduction.
Conceptual theories and mechanisms
Interventions grounded in a single theoretical framework appeared to be more effective in reducing caregiver burden, with four studies out six reporting significant improvements,20–22,25 compared with interventions integrating multiple theories, of which only two out of four studies showed significant effects.26,27 However, this apparent advantage may be confounded by differences in delivery characteristics rather than reflecting the effect of theoretical focus alone. Theory-outcome patterns suggest differential mechanisms: Benefit-Finding Therapy consistently improved depression22,23 but variably reduced burden; cognitive reappraisal may be insufficient without practical skill training. Mindfulness-Based Cognitive Therapy effectively addressed depression, stress and anxiety24,25 but less consistently burden, aligning with theory's emphasis on acceptance versus problem-solving. Behavioral Activation showed broad effectiveness, 21 potentially addressing both practical functioning and emotional well-being through activity engagement.
Cultural context may moderate theory effectiveness. Asian filial piety values may make Benefit-Finding particularly resonant by reframing caregiving as fulfilling family obligations. Multicomponent approaches offer comprehensive mechanism targeting but introduce implementation complexity. Future research should examine theory-by-delivery interactions and cultural moderators through designs isolating theoretical approach while controlling delivery characteristics.
Important heterogeneity exists across Asian cultures requiring tailored approaches. Countries with Asian diaspora populations, such as America, Canada, the United Kingdom and Australia, need guidance for culturally appropriate adaptations. Key considerations: language accessibility, cultural concepts of dementia and caregiving, family decision-making patterns, delivery preferences, integration with culturally-specific resources. Interventions should incorporate filial piety values while addressing guilt and stigma around institutional care. Facilitators need cultural competency training regarding immigration status, acculturation levels, and intergenerational differences. Assessment tools should be culturally validated to account for differences in the expression of distress, including somatic versus emotional manifestations. System-level approaches must address structural barriers, including limited service awareness, language barriers, cultural stigma, and immigration concerns. Outreach through Asian community organizations could improve access and engagement.
Gender lens in caregiving
The findings of this review reveal a notable absence of gender-sensitive approaches across the included studies, despite the overwhelmingly gendered nature of dementia caregiving in Asia. Nine of the ten studies reported predominantly female caregiver samples, reflecting broader societal patterns in which women disproportionately assume caregiving roles due to cultural expectations rooted in filial piety and traditional gender norms. 5 This gendered distribution creates additional burdens for female caregivers, including role conflict between caregiving and employment, economic vulnerability from reduced workforce participation, and social isolation stemming from the all-encompassing nature of care responsibilities.
This gender distribution reflects broader societal patterns where women disproportionately assume caregiving roles due to cultural expectations and traditional norms, creating additional burdens including role conflict, economic vulnerability, and social isolation.5 Despite this clear gender dimension, none of the included studies explicitly adopted a gender-sensitive framework in intervention design, delivery, or evaluation. No study tailored intervention content to address the distinct experiences of male versus female caregivers, nor were gender-stratified analyses conducted to examine whether intervention effectiveness varied by caregiver gender. This represents a significant gap, as the mechanisms through which psychoeducational interventions reduce burden may differ between genders. For instance, female caregivers may benefit more from interventions addressing role conflict and self-compassion, while male caregivers may respond better to problem-focused skill-building and practical resource navigation.
Several studies highlighted the importance of societal-level supports beyond individual-level interventions, including workplace policies such as paid family leave and flexible work arrangements, enhanced respite care services, subsidized day care, and accessible community-based support.9,11,31 Healthcare systems should employ gender-sensitive approaches that acknowledge the unique challenges faced by women in caregiving while also engaging male family members in shared caregiving responsibilities.
Future research should explicitly incorporate gender sensitivity into the design, delivery, and evaluation of psychoeducational interventions. This includes conducting gender-stratified analyses to identify differential intervention effects, tailoring intervention content to address gender-specific stressors and coping mechanisms, and examining how cultural gender norms across different Asian societies moderate intervention effectiveness. Additionally, future studies should consider how interventions can promote more equitable distribution of caregiving responsibilities within families, rather than focusing solely on supporting the primary (often female) caregiver.
Strengths and limitations
This review demonstrates several strengths. Firstly, it rigorously adhered to a methodical and validated approach in accordance with the PRISMA 2020 guidelines. This ensured a robust and systematic process throughout the review. Secondly, a diverse array of databases from various disciplines were thoroughly searched and included in the review. This comprehensive approach enhances the breadth and depth of the findings, minimizing the risk of overlooking relevant studies. Lastly, the review's rigor was further strengthened by the involvement of two independent investigators in the key stages of article selection, quality appraisal, and data extraction for all included studies. This dual-investigator process not only enhances the reliability of the findings but also mitigates potential biases, ensuring a more rigorous and trustworthy synthesis of evidence.
However, this review also had several limitations. Firstly, the studies in this review were limited to only those published in English. This may result in the inadvertent exclusion of studies published in other languages, including Mandarin, Malay, or Tamil. Consequently, valuable findings and diverse perspectives relevant to Asian family caregivers may not be fully represented. Secondly, the synthesis of data was constrained by the heterogeneous nature of the included studies, which exhibited variations in study design, sample size, intervention design, comparison groups, and outcome measures. This diversity introduced challenges in drawing conclusive interpretations. Lastly, the majority of studies originated from Hong Kong. This geographical concentration may introduce potential biases and limit the generalizability of the review findings.
Future studies
Given the public health significance of caregiver burden and the limited research conducted in Asia, further studies are highly recommended. These studies should build upon the findings of this review, particularly considering the limitations discussed above. Future studies should consider conducting a two-arm RCT in Singapore. This study would examine the effectiveness of psychoeducational interventions in reducing caregiver burden compared to usual care within the local population. The intervention should utilize multicomponent conceptual theories to structure and guide its intervention components. Moreover, this intervention could be delivered over the telephone over a period of six months. The outcomes of interest include caregiver burden, self-efficacy, and depression. Furthermore, future studies should incorporate gender-sensitive approaches in intervention design and delivery, including gender-stratified analyses to examine differential effectiveness across male and female caregivers, and consider how cultural gender norms influence intervention uptake and outcomes.
Public health implications for family caregivers of people with dementia in Singapore
This systematic review sheds light on psychoeducational interventions aimed at alleviating caregiver burden among Asian family caregivers. Psychoeducational interventions demonstrate promising outcomes in reducing caregiver burden, depression, perceived distress, and perceived stress, while also enhancing self-efficacy. These findings are particularly pertinent in the context of Singapore, where current support for caregivers primarily consists of dementia education and caregiver skills training. Incorporating psychoeducational interventions into existing programs could significantly enhance the support provided to caregivers of people with dementia, thereby addressing critical gaps in care and improving overall well-being within the community.
For Singapore specifically, telephone-delivered psychoeducational interventions grounded in a multicomponent theoretical framework, such as cognitive-behavioral therapy combined with Stress Appraisal and Coping, and delivered individually over a six-month period, may be particularly appropriate. This approach integrates evidence supporting the effectiveness of telephone delivery across multiple outcomes, aligns with cultural preferences for privacy through individual delivery, allows sufficient duration to promote sustained change, and employs a multicomponent theoretical framework to comprehensively address the multifaceted nature of caregiver burden.
Implementation should consider linguistic and cultural accessibility, providing services in English, Mandarin, Malay, and Tamil, with facilitators matched to participants’ cultural backgrounds. Integration with existing services, such as the Dementia Caregiver Support Program and Caregiver Training Grants, as well as partnerships with organizations like the Alzheimer's Disease Association Singapore, could enhance program reach and uptake.
Pilot evaluations should include recommended outcome measures, such as Zarit Burden Interview, Center for Epidemiologic Studies Depression Scale, Perceived Stress Scale, self-efficacy measures, assessed at baseline, post-intervention, and three-month follow-up. Inclusion of cost-effectiveness analyses is recommended to inform decisions regarding service scaling and sustainability.
Recommended assessment tools
Based on the included studies, several key assessment tools are recommended for implementation in Singapore. The Zarit Burden Interview emerged as the primary burden measure, used across all ten studies with demonstrated excellent cross-cultural validity and sensitivity to intervention effects, with culturally validated versions available in multiple Asian languages. For depression assessment, the Center for Epidemiological Studies-Depression Scale showed consistent utility across studies, while the Hamilton Depression Rating Scale provided an alternative for clinician-administered assessments and the Geriatric Depression Scale proved suitable for older caregivers. Self-efficacy measurement benefited from domain-specific instruments aligned with intervention targets, including the Self-Efficacy for Controlling Upsetting Thoughts scale for cognitive control and the Self-Efficacy for Obtaining Respite scale for support-seeking confidence. The Perceived Stress Scale effectively captured general stress perception while the Neuropsychiatric Inventory Questionnaire distress subscale provided symptom-specific distress assessment related to behavioral and psychological symptoms of dementia. Additional tools including the Five Facet Mindfulness Questionnaire-Short Form for mindfulness-based interventions and the Short Form Health Survey (SF-12 or SF-36) for quality-of-life assessment demonstrated utility depending on intervention type. For successful Singapore implementation, all assessment tools should undergo cultural validation and be available in Chinese, Malay, and Tamil to ensure accessibility across major ethnic groups, with score interpretation considering cultural norms regarding distress expression and help-seeking behaviors, as clinically significant thresholds may vary across cultural contexts. Table 5 provides a summary of the recommended assessment tools by outcome domain.
Recommended assessment tools by outcome domain.
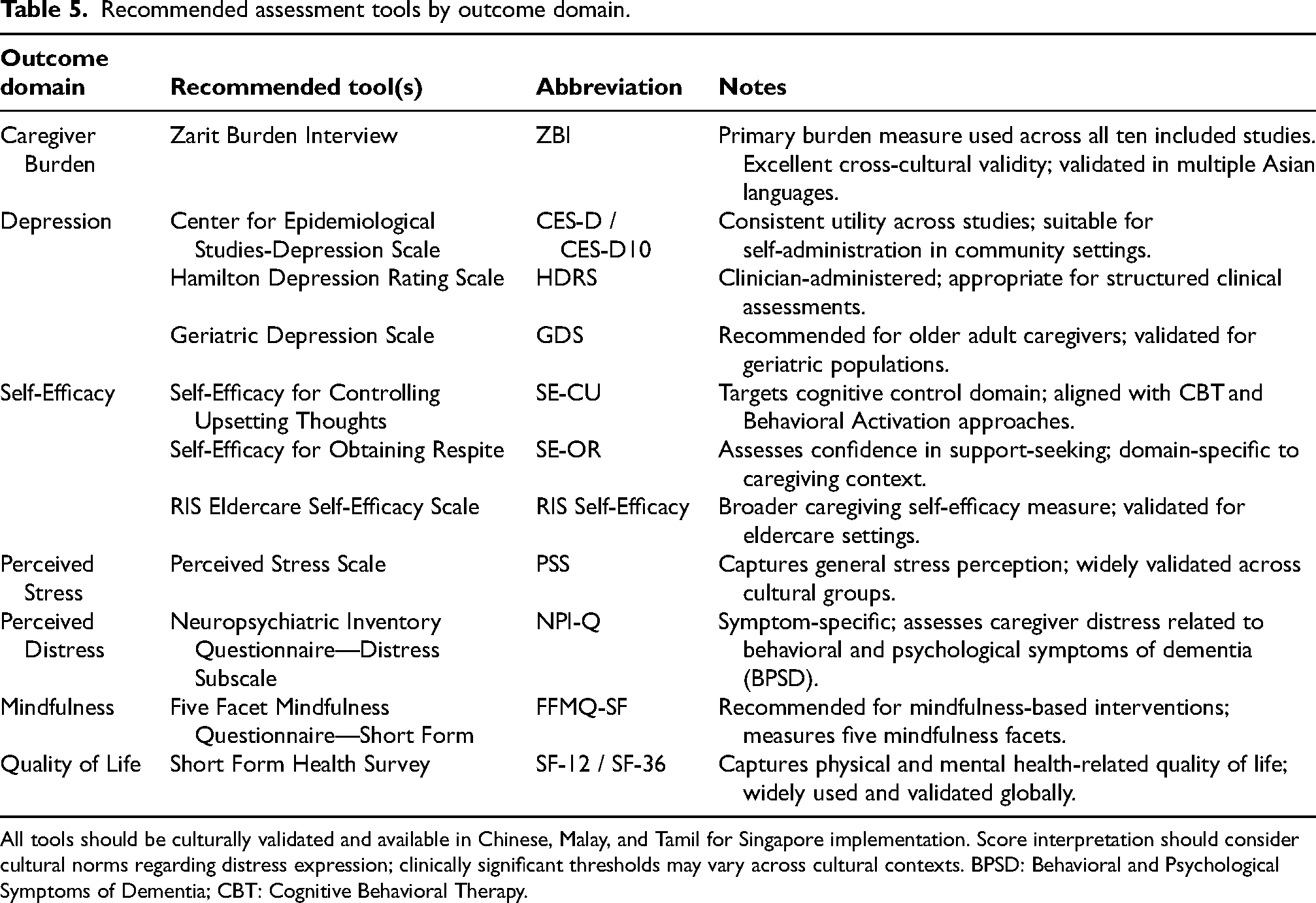
All tools should be culturally validated and available in Chinese, Malay, and Tamil for Singapore implementation. Score interpretation should consider cultural norms regarding distress expression; clinically significant thresholds may vary across cultural contexts. BPSD: Behavioral and Psychological Symptoms of Dementia; CBT: Cognitive Behavioral Therapy.
Conclusion
This review details the characteristics of psychoeducational interventions, summarizes their effectiveness in reducing caregiver burden and improving other psychological outcomes, and identifies the factors influencing these effects. Addressing the gap in systematic reviews that specifically focus on the Asian context, this review synthesizes findings from published literature across various regions of Asia. The insights from this review should benefit public health and guide healthcare professionals in implementing similar interventions tailored to the needs of family caregivers in their local populations. Future research should build on these findings to deepen the understanding of psychoeducational interventions’ effectiveness within Asian communities.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261461174 - Supplemental material for The effectiveness of psychoeducational interventions for family caregivers of people with dementia in Asia: A systematic review
Supplemental material, sj-docx-1-alz-10.1177_13872877261461174 for The effectiveness of psychoeducational interventions for family caregivers of people with dementia in Asia: A systematic review by Emily Yong An Yap, Dennis Bingzhu Chia, Jeannette Jen-Mai Lee, Ming Hui Choo, Hin Kiat Cheng and Ravi Shankar in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We acknowledge support of Ms. Loh Mee Lan, from the NUS Research Library Team, your teaching and guidance in developing search terms and strategies have been immensely helpful. Thank you for your support.
ORCID iDs
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
This systematic review is based on data extracted from previously published articles, which are all cited within the manuscript. No new primary data were generated. The protocol for this review is registered with PROSPERO (CRD42023493206). Data extraction sheets and summary tables generated during the review are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.