
Abstract
This study investigated the long-term clinical effects of multisession gamma transcranial alternating current stimulation (tACS) over the precuneus in early-stage Alzheimer's disease. Forty-six patients from a previous randomized, double-blind, sham-controlled trial with an open-label extension underwent follow-up at 36 and 72 weeks. Participants received either 8 or 16 weeks of gamma tACS. Both treatment durations showed comparable long-term outcomes. Alzheimer's Disease Assessment Scale–Cognitive Subscale did not significantly worsen at 36 weeks, and Face–Name Association Test remained stable at both follow-up time points, whereas Clinical Dementia Rating–Sum of Boxes and Alzheimer's Disease Cooperative Study–Activities of Daily Living worsened over time. These findings suggest relative preservation of selected cognitive measures, despite worsening in broader clinical and functional outcomes.
Keywords
Introduction
An increasing body of evidence suggests that gamma brain oscillations (typically 30–100 Hz) play a crucial role in the pathogenesis of Alzheimer's disease (AD). 1 Gamma oscillations are prominent across multiple brain regions including the hippocampus, and are implicated in cognitive functions including long-term memory, working memory, and attention. 2
A promising approach for modulating brain oscillations is transcranial alternating current stimulation (tACS) stimulation, a non-invasive neuromodulatory technique that delivers weak sinusoidal electrical currents to the scalp, generating oscillatory electric fields within the cortex.3,4 Gamma-frequency tACS may partially restore disrupted gamma-band synchronization observed in AD and improve cognitive functions.5,6 Recent longitudinal studies, sham-controlled 40 Hz tACS investigations, and meta-analytic findings have further expanded the clinical framework of gamma-frequency tACS and related non-invasive interventions in AD and dementia, further supporting the growing clinical interest in gamma-frequency stimulation approaches.7–9
In a home-based double-blind, randomized, sham-controlled clinical trial followed by an open label phase, we have recently demonstrated that multisession gamma tACS applied over the precuneus showed significant clinical efficacy in patients with early-stage AD at short term, with 8 weeks treatment comparable to 16 weeks treatment at 24 weeks follow-up. In the parent study, stimulation was delivered at home 5 days per week, 1 h per day, after an initial in-person training phase for caregivers, with subsequent remote monitoring by the study team. We also observed improvements in short-latency afferent inhibition, an indirect measure of cholinergic neurotransmission, together with increased electroencephalogram (EEG) gamma-band activity, supporting target engagement and gamma entrainment. 10 Although these data suggest that gamma tACS represents a promising therapeutic approach for AD, offering potential insights into novel treatment strategies, longer-term effects of multisession gamma tACS remain unknown, particularly in the context of home-based interventions.
In this study, we leveraged the previously conducted trial to perform an extended long-term follow-up of the patients to evaluate long-lasting clinical effects of gamma tACS over the precuneus in early-stage AD in 8 week- and 16 week-treatments groups.
Methods
Participants
We included 46 of the 50 patients previously enrolled in the study by Cantoni et al. 10 Four participants were not included in the extended long-term follow-up because geographical distance from the study center prevented completion of the in-person assessments; this was unrelated to clinical worsening or unwillingness to participate. All participants met current clinical criteria for AD 11 and underwent either amyloid PET imaging or cerebrospinal fluid analysis, including measurements of Aβ42, phosphorylated tau (p-tau181), and total tau, to confirm the etiologic diagnosis of AD. Demographic and clinical characteristics were systematically collected.
At baseline (T0), participants were randomized to receive either sham tACS (Group 1) or gamma-frequency tACS (Group 2), administered 5 days per week, 1 h per day, for 8 weeks (double-blind phase). Subsequently, all participants received real gamma tACS for an additional 8 weeks (open-label phase), delivered 5 days per week, 1 h per day. Short-term clinical effects of gamma tACS through week 24 have been previously reported. 10 Participants subsequently underwent long-term follow-up assessments at weeks 36 (T36) and 72 (T72) (see Supplemental Figure 1).
Because all participants received real stimulation after the initial randomized phase, no untreated control group was available at long-term follow-up. Therefore, the 36- and 72-week assessments should be interpreted as an extended observational follow-up of the parent trial rather than as a controlled long-term comparison.
Based on the clinical efficacy observed at short-term follow-up, standardized clinical evaluations at long-term follow-up included the Clinical Dementia Rating–Sum of Boxes (CDR-SB), the Alzheimer's Disease Assessment Scale–Cognitive Subscale (13-item version; ADAS-Cog-13), the Alzheimer's Disease Cooperative Study–Activities of Daily Living (ADCS-ADL), and the Face–Name Association Test (FNAT).
Statistical analysis
To assess the effect of tACS treatment over time, we used linear mixed-effects models (LME). 12 The TIME variable (T0, T36, T72) was modelled as a categorical factor, and TREATMENT (sham/real stimulation versus real/real stimulation) was included as between-subject factor. No additional covariates were included in the models. Missing follow-up observations were handled within the mixed-effects modelling framework, without ad hoc imputation.
Two-sided p-values<0.05 were considered statistically significant.
Results
Forty-six of the previously enrolled participants completed the T36-week follow-up (22 in Group 1 and 24 in Group 2), and thirty-four completed the T72-week follow-up (16 in Group 1 and 18 in Group 2). The demographic and clinical characteristics of the included patients are reported in Table 1.
Baseline demographic and clinical characteristics of AD patients by tACS group (sham/real versus real/real).
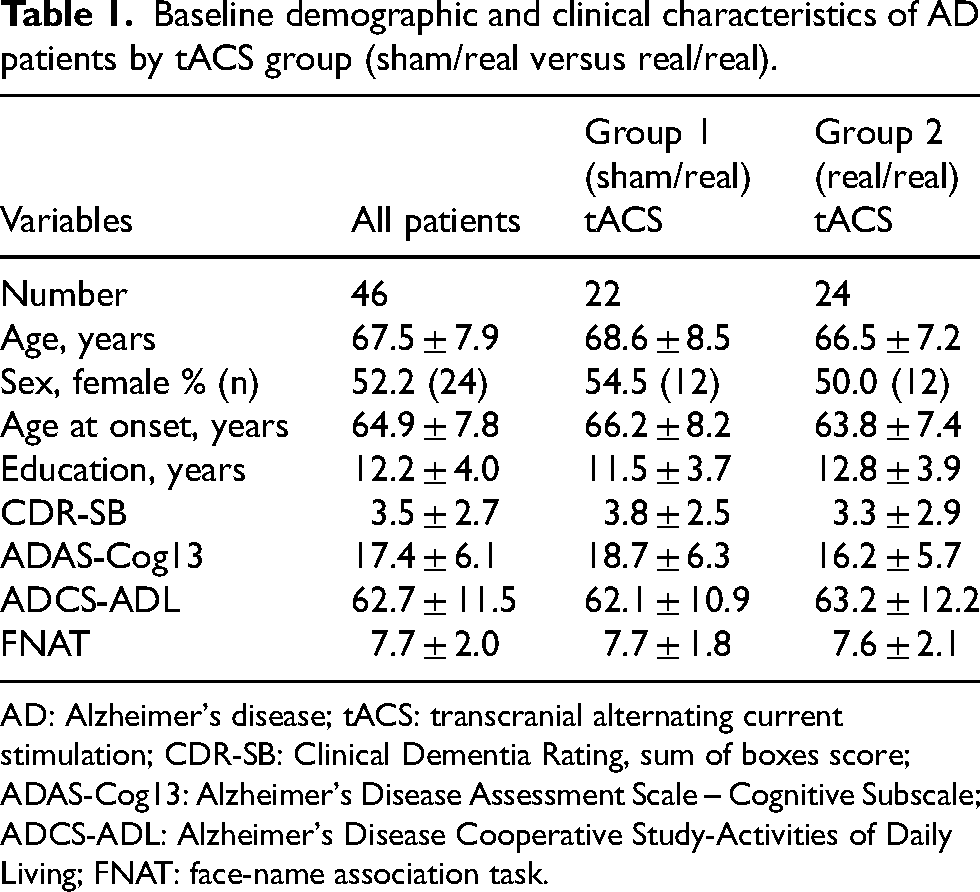
AD: Alzheimer's disease; tACS: transcranial alternating current stimulation; CDR-SB: Clinical Dementia Rating, sum of boxes score; ADAS-Cog13: Alzheimer's Disease Assessment Scale – Cognitive Subscale; ADCS-ADL: Alzheimer's Disease Cooperative Study-Activities of Daily Living; FNAT: face-name association task.
No significant effect of treatment duration (8 weeks versus 16 weeks) was observed on ADAS-Cog13 scores (estimated marginal difference=+0.29, standard error [SE] = 0.28, p = 0.29). Notably, in the overall sample, no statistically significant change in ADAS-Cog13 scores was observed between T0 and T36 (−0.05 [0.10], p = 0.60). Conversely, a significant increase was observed between T0 and T72 (+0.40 [0.11], p < 0.001) (Figure 1A).
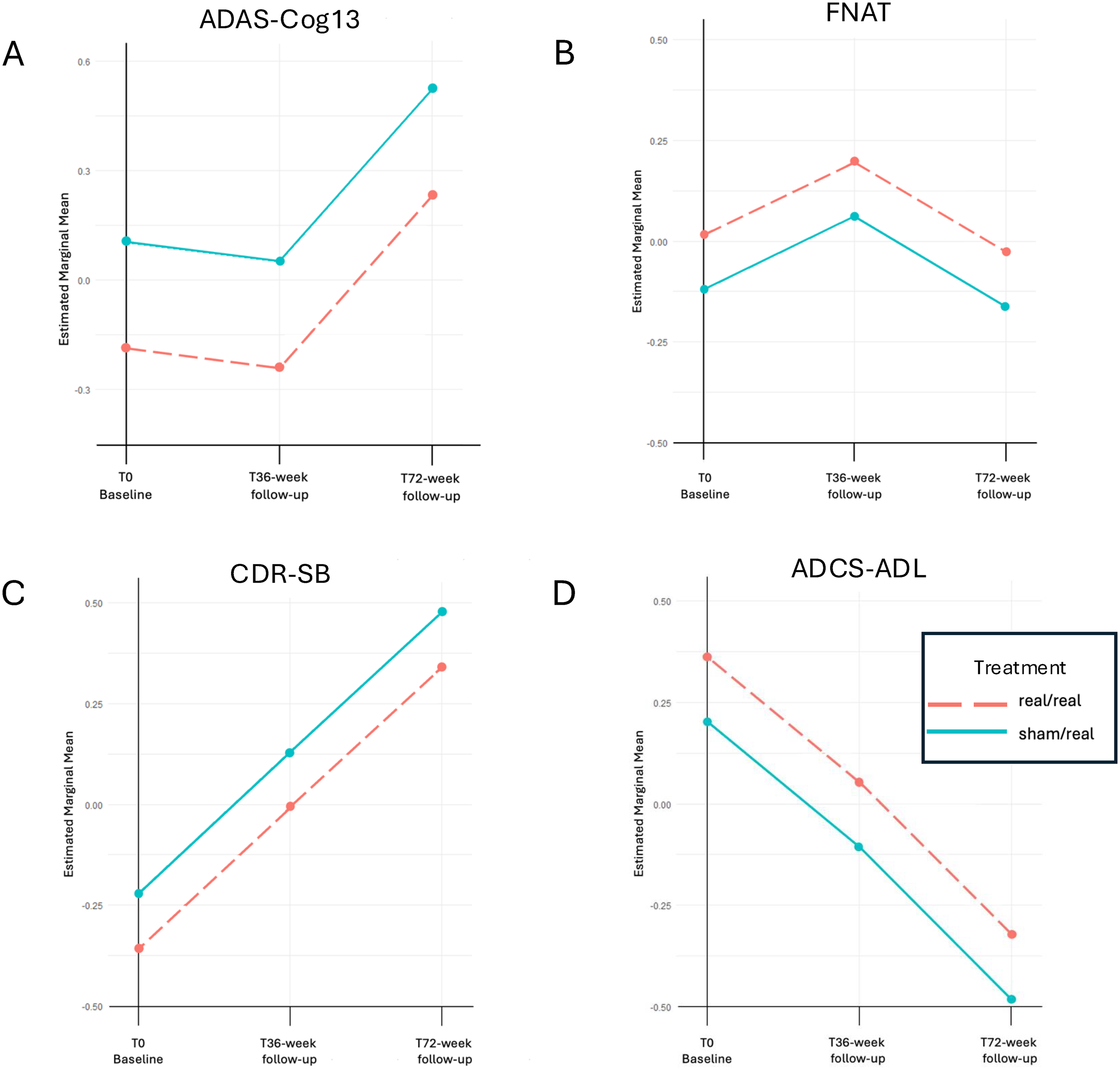
Neuropsychological scores in Group 1 (sham/real tACS) and Group 2 (real/real tACS) at baseline (T0) and at 36 weeks (T36) and at 72 weeks (T72) follow-up. A) Alzheimer's Disease Assessment Scale – Cognitive Subscale (ADAS Cog13); B) Face-Name Association Task (FNAT); C) Clinical Dementia Rating scale sum of boxes (CDR-SB); D) Alzheimer's Disease Cooperative Study Activities Daily Living (ADCS-ADL).
For the FNAT, we did not observe significant effect of treatment (−0.13 [0.23], p = 0.56), and no statistically significant change at T36 (+0.18 [0.16], p = 0.27) and T72 (−0.04 [0.18], p = 0.81) (Figure 1B).
Regarding the CDR-SB, no significant effect of treatment was found (+0.13 [0.27], p = 0.62); however, CDR-SB scores increased significantly both at T36 (+0.35 [0.10], p < 0.001) and at T72 (+0.70 [0.11], p < 0.001) (Figure 1C).
Comparable results were obtained for the ADCS-ADL, with no significant effect of treatment (−0.16 [0.28], p = 0.57), but with significant score reductions at both T36 (−0.31 [0.10], p < 0.001) and T72 (−0.68 [0.11], p < 0.001) (Figure 1D).
Discussion
In this extended follow-up study, we provide evidence that the clinical effects of multisession gamma tACS applied over the precuneus in patients with early-stage AD can persist over time, with comparable outcomes observed after 8 or 16 weeks of treatment. Our previous home-based, double-blind, randomized, sham-controlled clinical trial, followed by an open-label phase, demonstrated that 8 weeks of gamma tACS were sufficient to induce clinically meaningful short-term benefits lasting up to 24 weeks. The present findings extend these observations at long-term follow-up, although they should be interpreted cautiously given the absence of a long-term untreated control group.
Notably, the long-term findings showed a domain-specific pattern rather than a uniform stabilization across all outcomes. While patients did not show significant worsening between baseline and the 36-week follow-up in ADAS-Cog13 scores, and FNAT scores remained stable over follow-up, both CDR-SB and ADCS-ADL showed progressive worsening at 36 and 72 weeks. This pattern suggests that gamma tACS over the precuneus may preferentially influence selected cognitive processes, particularly those related to associative memory and aspects of global cognitive performance, while having a more limited impact on the broader clinical and functional decline that characterizes AD over time. These findings may suggest prolonged benefit in selected cognitive domains over extended follow-up, although not across all clinical and functional measures.
The requirement for prolonged treatment to achieve durable clinical effects is consistent with evidence from both animal and human studies on gamma entrainment, although the optimal treatment duration necessary to maximize clinical benefit remains to be determined. 13 From a clinical perspective, our results have important implications for the development of non-invasive neuromodulation protocols in AD and further suggest that an 8-week tACS treatment duration may represent an optimal balance for achieving therapeutic benefits in patients with early-stage AD. Moreover, the feasibility of home-based tACS delivery supports the implementation of repeated treatment cycles as a realistic and scalable approach.
These findings should be interpreted in light of important methodological limitations. Most notably, because all participants eventually received real gamma tACS after the initial sham-controlled phase, no untreated control group was available at the 36- and 72-week follow-up assessments. As a result, the observed longitudinal trajectories cannot be fully disentangled from the expected natural progression of AD, and the long-term findings should be considered exploratory.
In this context, the relative stability observed in selected cognitive measures should not be interpreted as evidence of global disease stabilization, but rather as a possible signal of prolonged benefit in specific domains. This interpretation is further supported by the fact that broader clinical and functional measures, such as CDR-SB and ADCS-ADL, continued to worsen over time.
A further limitation is that neurophysiological measures were not repeated at the 36- and 72-week follow-up. Therefore, although the parent trial demonstrated changes in short-latency afferent inhibition and gamma-band activity, the persistence of these biological effects over time could not be assessed in the present study.
Overall, this study strengthens the rationale for gamma tACS as a promising supportive neuromodulatory intervention in AD, potentially associated with prolonged clinical benefits in selected domains, while warranting confirmation in future controlled long-term studies.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261461248 - Supplemental material for Long-term effects of multisession gamma transcranial alternating current stimulation in Alzheimer's disease
Supplemental material, sj-docx-1-alz-10.1177_13872877261461248 for Long-term effects of multisession gamma transcranial alternating current stimulation in Alzheimer's disease by Valentina Cantoni, Mario Grassi, Enrico Premi, Chiara Cupidi, Elisa Zummo, Maria Sofia Cotelli, Alberto Benussi and Barbara Borroni in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors wish to thank all patients for their participation in this research.
Ethical considerations
This study was approved by the local ethics committee (Brescia Hospital, #NP5395).
Consent to participate
Written informed consent was obtained from all participants in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by an Italian Ministry of Health grant (PNRRPOC-2022–12376021). The funding was granted in compliance with Missione 6/Componente 2/Investmento: 2.1 “Rafforzamento e potenziamento della Ricerca Biomedica del SSN”, funded by the European Union - Next GenerationEU (CUP: G55E22001130001). The work is supported by Italian Ministry of Health (Ricerca Corrente).
Declaration of conflicting interests
BB is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review. The authors report no other potential conflicts of interest.
Data availability statement
Data are available upon reasonable request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.