
Abstract
Background
Population aging is accompanied by increasing multimorbidity and medication exposure, raising concerns regarding the role of polypharmacy as a potential modifiable risk factor for cognitive decline and Alzheimer's disease. However, polypharmacy is a heterogeneous construct, and its cognitive impact may depend more on regimen complexity and pharmacological burden than on medication count alone.
Objective
To estimate the prevalence and determinants of polypharmacy and to examine its association with functional status and cognitive performance in community-dwelling older adults from southern Chile.
Methods
A cross-sectional study was conducted between 2023 and 2025 including 848 adults aged ≥60 years from four provinces in the Los Lagos Region. Sociodemographic, clinical, and psychosocial data were collected through structured interviews and standardized assessments. Functional status was evaluated using EFAM-Chile, Barthel, and Pfeffer scales, and Cognitive performance and functional status were assessed using the Preventive Medicine Examination for Older Adults (EFAM-Chile). Polypharmacy was defined as the concurrent use of ≥5 medications, including prescribed and over-the-counter drugs. Regimen complexity and anticholinergic/sedative burden were quantified using the Medication Regimen Complexity Index (MRCI) and the Drug Burden Index (DBI).
Results
Polypharmacy was associated with better functional and cognitive scores in unadjusted analyses (p < 0.05), although these associations were not independent after adjustment. Multimorbidity was the strongest predictor of medication count. Despite greater medication exposure, MRCI and DBI values remained within low-to-moderate ranges, indicating limited pharmacological burden relevant to cognitive vulnerability. These findings may be explained by reverse causation or by confounding related to health status
Conclusions
In this population, polypharmacy was not associated with cognitive screening outcomes, although the absence of detailed neuropsychological assessment limits conclusions regarding cognitive impairment or dementia risk and may reflect optimized management of chronic conditions. Qualitative pharmacological indices may improve the identification of medication-related cognitive risk in aging populations.
Introduction
A profound demographic transformation is underway globally, driven by sustained declines in fertility rates and significant increases in life expectancy. 1 Consequently, the proportion of older adults within the population is expanding rapidly, reshaping the social and healthcare landscapes.2,3 This demographic transition poses considerable public health challenges, particularly in relation to chronic disease management, long-term care, and medication use in aging populations. 4
Polypharmacy, commonly defined as the concurrent use of five or more medications, has become increasingly prevalent among older adults.5,6 While often clinically justified in the context of multimorbidity, polypharmacy carries substantial risks when not adequately tailored to the patient's health status. 7 In older adults, age-related physiological changes and the high burden of multimorbidity frequently lead to the use of multiple medications, increasing the risk of adverse drug reactions and clinically significant drug–drug interactions, particularly when treatments are not individualized. 8 Older adults respond differently to medication regimens due to age-related pharmacokinetic and pharmacodynamic changes, which increase susceptibility to adverse drug reactions and drug–drug interactions.8–10 Importantly, several chronic conditions commonly managed through polypharmacy such as hypertension, diabetes, and dyslipidemia are established risk factors for cognitive decline and Alzheimer's disease. At the same time, their adequate pharmacological management has been associated with a reduced risk of dementia, highlighting the complex role of pharmacological treatment in modulating cognitive outcomes in later life.11,12 Thus, medication use in older adults may simultaneously represent both a potential risk and a preventive strategy in the context of neurodegenerative disease.
Polypharmacy is increasingly recognized as a multidimensional phenomenon that cannot be fully captured by medication count alone. 13 The clinical impact of polypharmacy depends not only on the number of medications prescribed but also on their pharmacological properties, potential interactions, and regimen complexity.14,15 Regimen complexity, including dosing frequency, formulation, and specific administration instructions, has been shown to influence adherence, medication errors, and health outcomes independently of medication count. 16 These considerations have led to the development of instruments such as the Medication Regimen Complexity Index (MRCI) 17 and the Drug Burden Index (DBI), 18 which aim to quantify qualitative aspects of medication use that are often overlooked in traditional polypharmacy definitions. Despite the growing international evidence, these dimensions remain underexplored in Latin American populations, limiting the ability to distinguish between appropriate and potentially harmful polypharmacy in older adults. These qualitative dimensions may be particularly relevant when examining functional autonomy, cognitive vulnerability, and dementia risk in later life.
In this context, assessing functional and cognitive capacities is essential for individualized care and for evaluating medication-related vulnerability in older adults. In Chile, EFAM-Chile is widely used in primary care as a multidimensional screening tool for functional and cognitive assessment, although its performance may be influenced by educational level. 19 The instrument evaluates performance in activities of daily living and incorporates a brief cognitive assessment based on a short-form version of the Mini-Mental State Examination (MMSE), a globally recognized tool for detecting cognitive impairment. 20 However, cognitive screening performance and cutoff scores are strongly influenced by educational attainment, which is particularly relevant in populations with low schooling.21,22
Therefore, this study examines the associations of polypharmacy, medication burden (DBI), and regimen complexity (MRCI) with functional and cognitive performance among community-dwelling older adults in southern Chile, using a multidimensional dataset that includes sociodemographic, clinical, and psychosocial indicators.
Methods
This study employed a cross-sectional design and was conducted between 2023 and early 2025 in four provinces of southern Chile: Llanquihue (LL), Palena (PA), Osorno (OS), and Chiloe (CH). The research was embedded within a regional public health surveillance project aimed at comprehensively assessing health, functional status, and medication use among community-dwelling older adults residing in both urban and rural settings. Data collection followed a standardized protocol and was carried out by trained health professionals in collaboration with primary healthcare centers and community organizations.
Population and sampling
The study population comprised 848 community-dwelling individuals aged 60 years or older from the Los Lagos Region, Chile. Participants were identified through local primary healthcare centers (CESFAMs) and community-based organizations as part of a regional aging surveillance initiative. In particular, CESFAMs provided predefined lists of older adults for home-based assessments, especially in rural areas. Thus, recruitment was not based exclusively on self-initiated attendance at healthcare centers. A non-probabilistic convenience sampling strategy was used.
All participants provided written informed consent prior to enrollment. Exclusion was not based on a prior diagnosis of severe cognitive impairment or communication difficulties per se, but only on the inability to provide informed consent or to complete the interview and assessment protocol due to severe cognitive, sensory, or communication impairment, as judged during field evaluation.
Data collection
Data was obtained through structured face-to-face interviews and standardized clinical assessments conducted by trained health personnel. The dataset included the following domains:
Sociodemographic variables
Age, sex, educational attainment (years of formal education), area of residence (urban or rural), and household income.
Anthropometric and clinical measurements
Height, weight, body mass index (BMI), systolic and diastolic blood pressure (sitting and standing), and heart rate.
Chronic conditions and comorbidities
Presence of self-reported and/or diagnosed diseases, including hypertension, diabetes, arthritis, cardiovascular disease, osteoarthritis, and other long-standing illnesses.
Pharmacological profile
Medication use was documented by direct report and medical record verification, considering both prescribed and over-the-counter drugs. Polypharmacy was defined as the concurrent use of five or more medications, in line with standard definitions.6,23 For descriptive analyses, individual medications were additionally classified according to ATC level 1 groups and by OTC status. For each ATC level 1 category, the percentage of OTC drugs was calculated as the proportion of observed medication uses within that category corresponding to medications classified as OTC.
In addition, the MRCI and the DBI were calculated for each participant to further characterize pharmacological exposure. The MRCI was used to quantify the structural and dosing complexity of medication regimens, while the DBI assessed the cumulative anticholinergic and sedative load. These indices provided complementary proxy measures of regimen complexity (MRCI) and anticholinergic/sedative burden (DBI), enabling a more qualitative characterization of pharmacologic exposure beyond medication count.
Functional status was assessed using three validated instruments
Barthel Index 24
Assesses an individual's ability to perform basic activities of daily living (ADLs), including feeding, bathing, dressing, and mobility. Has been validated for Chilean population nationwide. 19 Scores range from 0 to 100, with higher values reflecting greater functional independence. Standard cutoffs classify functional status as follows: 0–20 = total dependence, 21–39 = severe dependence, 40–55 = moderate dependence, 56–99 = mild dependence, and 100 = complete independence.
Pfeffer functional activities questionnaire 25
Assesses instrumental activities of daily living (IADLs), such as handling finance, managing medications, and shopping, based on information provided by the person with closest and most regular contact with the older adult (e.g., caregiver, family member, other). PFAQ has been validated in three different Chilean surveys applied to older people. 26 The scale ranges from 0 to 33, where higher scores indicate greater functional impairment. A score above 5 suggests functional decline.
EFAM-ChileScale 19
A national screening instrument used in Chile to evaluate functional capacity in older adults, integrating both basic (ADLs) and instrumental activities of daily living (IADLs). Scores range from 0 to 55, with higher values indicating better functional status. Standard cutoffs classify individuals as follows: 0–42 = at risk of dependency, 43–46 = functionally independent, and 47–55 = functionally independent without risk.
Cognitive measures were evaluated using
Subjective Memory Complaint Questionnaire (SMCQ) 26 : A self-reported measure evaluating an individual's perceived memory difficulties. Has been validated in the GERO Cohort Protocol, Chile, 2017–2022. 27 Scores range from 0 to 14, with higher scores reflecting greater concern or perception of memory decline. Standard thresholds classify responses as follows: 0–2 = no complaint, 3–6 = mild complaint, 7–10 = moderate complaint, and 11–14 = severe complaint.
Psychosocial measures were evaluated using:
Hospital anxiety and depression scale (HADS) 28
A validated self-report instrument designed to screen symptoms of anxiety and depression in medical and community settings. It consists of 14 items, divided into two subscales (7 for anxiety and 7 for depression), each scored from 0 to 21. Higher scores indicate greater symptom severity, with cutoff values typically categorized as 0– 7 = normal, 8–10 = borderline abnormal (possible case), and 11–21 = abnormal (probable clinical case). This tool is widely used in older adult populations for detecting affective disorders in a non-stigmatizing and practical manner.
APGAR family Scale 29
A brief questionnaire developed to assess an individual's perception of family support and functioning across five domains: Adaptation, Partnership, Growth, Affection, and Resolve. Each item is scored from 0 to 2, yielding a total score ranging from 0 to 14. Interpretation is commonly classified as 0–4 = severely dysfunctional, 5–9 = moderately dysfunctional, and 10–14 = highly functional family. This scale provides insight into the role of social and family support in overall well-being and health outcomes among older adults.
Statistical analysis
Descriptive statistics were used to characterize the study population across sociodemographic, clinical, functional, cognitive, and pharmacological variables. The prevalence of polypharmacy was estimated, and participants were stratified by functional and cognitive performance.
To evaluate the relationship between polypharmacy status and functional/cognitive performance, mean scores were compared between participants with and without polypharmacy, stratified by sex, using Student's t-tests. Differences between means were reported with 95% confidence intervals (CIs) and accompanied by p-values and Cohen's d effect sizes to quantify the magnitude of differences.
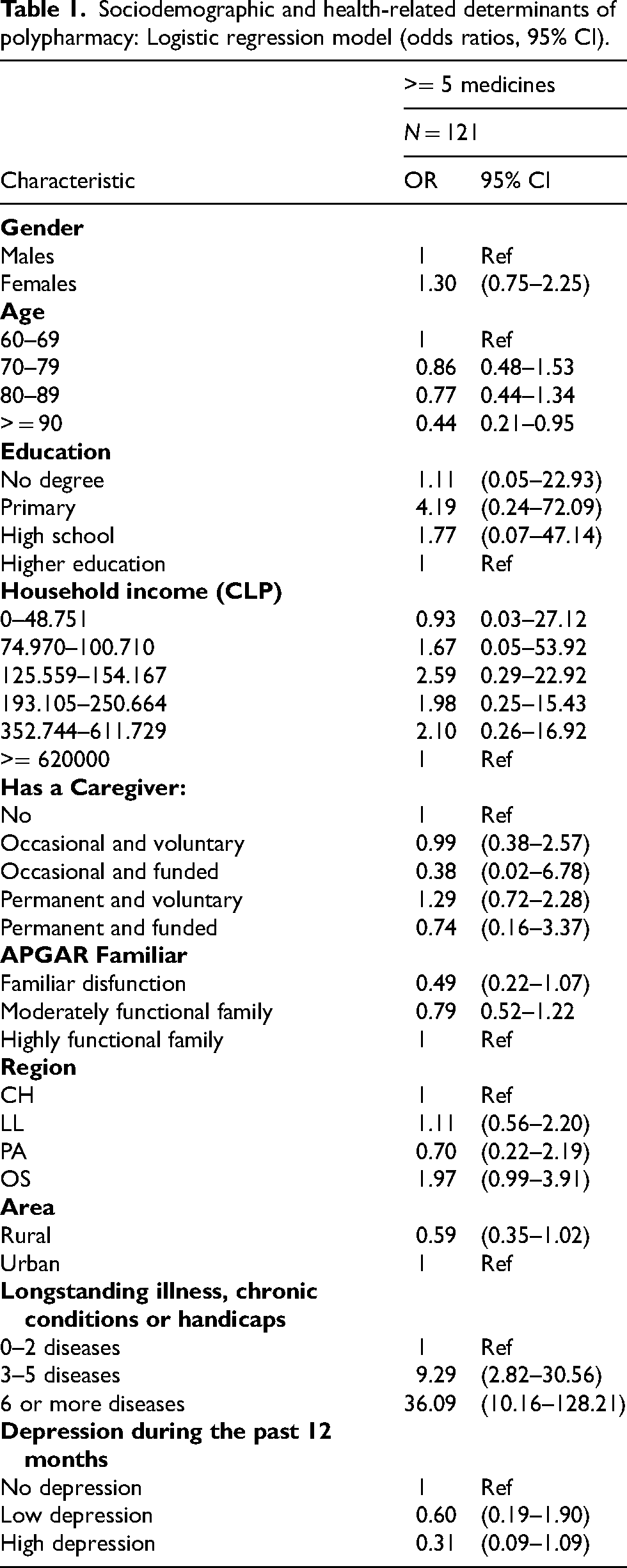
Associations between polypharmacy and sociodemographic variables were evaluated using binomial logistic regression models to estimate odds ratios (ORs) with 95% confidence intervals (Table 1). In addition, multivariable binomial logistic regression models were fitted to evaluate the independent association between polypharmacy and sociodemographic characteristics, together with functional and cognitive test scores to identify which factors showed the strongest association with polypharmacy after adjustment. Results are reported as odds ratios with their corresponding 95% confidence intervals and p-values, reflecting the strength and direction of associations. Complementarily, Poisson regression models were employed to evaluate the total number of medications used as a count outcome, with results expressed as rate ratios (RR) with 95% CIs and p-values.
Sociodemographic and health-related determinants of polypharmacy: Logistic regression model (odds ratios, 95% CI).
Given the large sample size, parametric tests (t-tests) were considered sufficiently robust to moderate deviations from normality. Distributional assumptions were evaluated through graphical inspection, which indicated deviations from strict normality. Therefore, while group comparisons were conducted using t-tests, associations between pharmacological complexity (MRCI and DBI) and functional/cognitive scores were assessed using Spearman's rank correlation (ρ), a non-parametric method less sensitive to distributional assumptions. Results are reported as Spearman's ρ with corresponding p-values.
All analyses were performed in R version 4.3.1. A significance level of 5% (p < 0.05) was considered for all statistical tests.
Results
Socio-demographic characteristics
Results are presented in three stages: (1) prevalence and determinants, (2) associations with outcomes, and (3) comparative analysis of pharmacological burden.
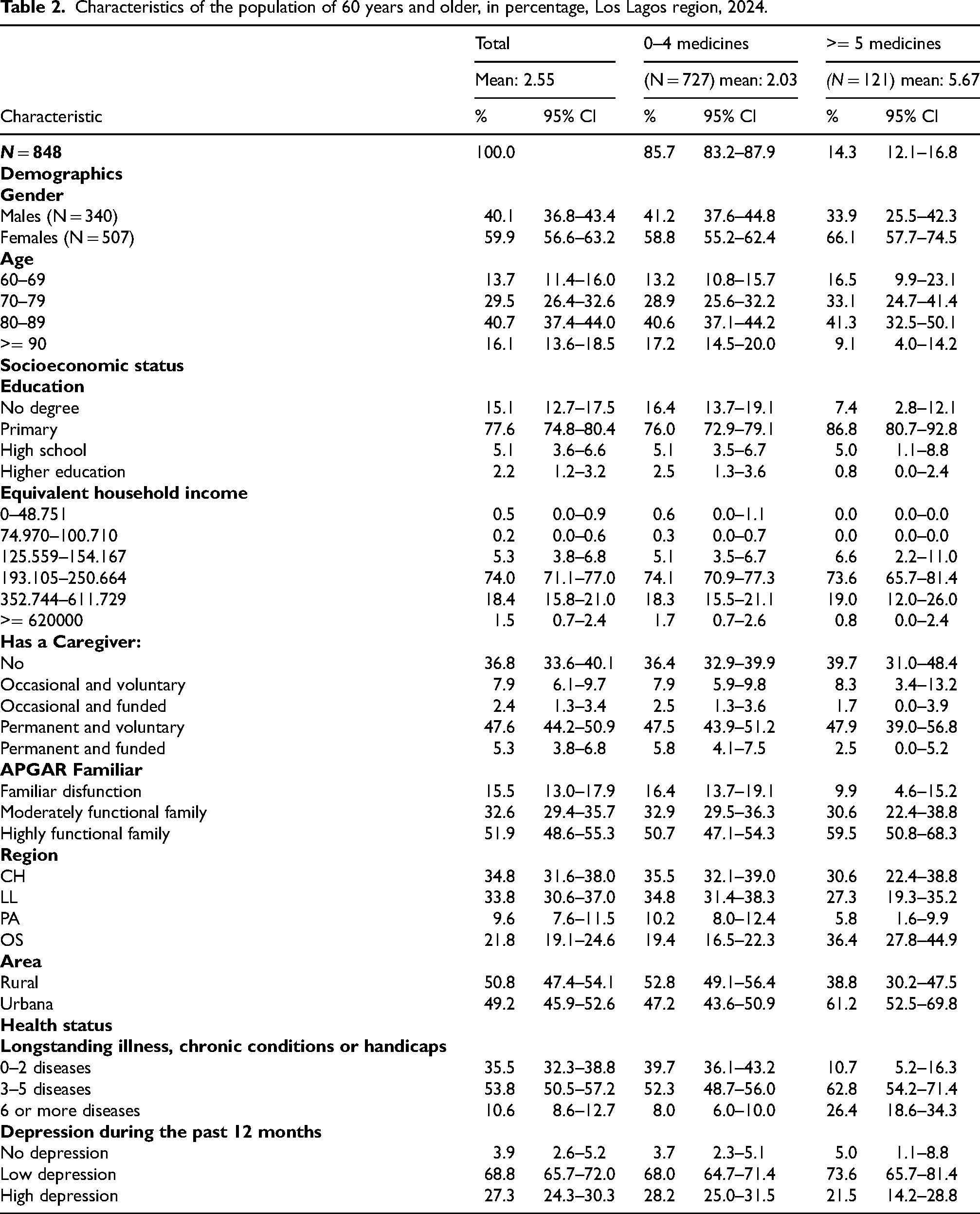
A total of 848 community-dwelling adults aged 60 years and older were included in the analysis. The sample was characterized by advanced age, with a mean age of 80.5 years, and a predominance of women (59.9%). Approximately half of the participants resided in rural areas (50.8%). Educational attainment was generally low, with a mean of 3.9 years of formal education; 68.8% of participants had completed four years of schooling or less.
The burden of chronic disease was high, with participants reporting a mean of 3.27 chronic conditions. Hypertension (69.8%), dyslipidemia (39.5%), type 2 diabetes (32.8%), and osteoarthritis (29.4%) were the most prevalent conditions. These characteristics describe a population with substantial clinical complexity and socioeconomic vulnerability (Table 2).
Characteristics of the population of 60 years and older, in percentage, Los Lagos region, 2024.
Prevalence of polypharmacy
Polypharmacy, defined as the concurrent use of five or more medications, was identified in 14.3% of the study population (n = 121). The mean number of medications used per participant was 2.55, ranging from 0 to 11. Among the polypharmacy group, the mean number of medications was 5.67. Polypharmacy was more frequent among women, younger, urban participants, and individuals with a higher burden of chronic diseases (Table 1).
Reference categories: Males (Gender); 60–69 years (Age); Higher education (Education); ≥620,000 CLP (Income); No caregiver (Caregiver); Highly functional family (APGAR); CH (Region); Urban (Area); 0–2 diseases (Longstanding illness, chronic conditions or handicaps); No depression (Depression during the past 12 months). Model N = 848.
In multivariable analyses, multimorbidity emerged as the main determinant of polypharmacy. In the logistic regression model including clinical, cognitive, functional, and psychosocial variables, the number of chronic diseases was the only factor independently associated with polypharmacy status (OR = 1.63, 95% CI 1.43–1.85; p < 0.001), whereas cognitive and functional measures were not significantly associated after adjustment (Table 3).
Determinants of polypharmacy: Binomial logistic regression model (R2 = 0.147) expressed as odds ratios (OR) and, determinants of the number of medicines used: Poisson regression model (R2 = 0.076) expressed as rate ratios (RR). 95% confidence intervals and p-values are shown. Model N = 848.
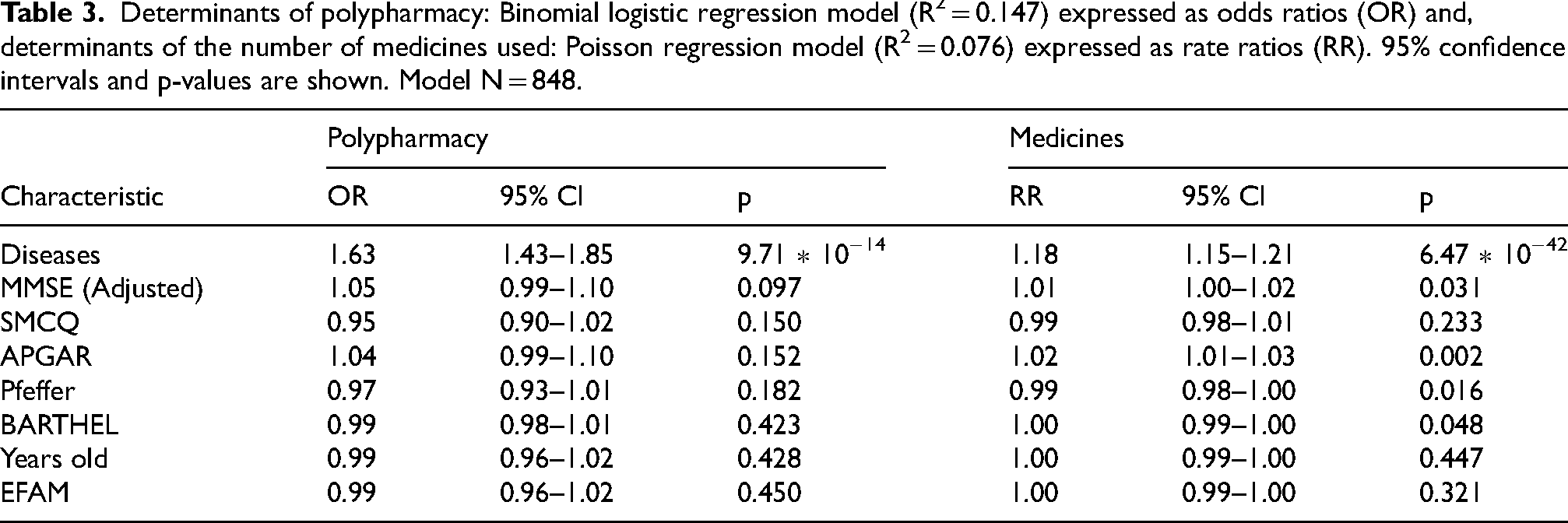
Consistent findings were observed when the total number of medications was analyzed as a count outcome. In the Poisson regression model, the number of chronic diseases again showed the strongest association with medication use (RR = 1.18, 95% CI 1.15–1.21; p < 0.001). Additional but smaller associations were observed for family support (APGAR), functional status as measured by Pfeffer, and objective cognitive performance as measured by the education-adjusted MMSE (Table 3).
Association between polypharmacy, functional status, and cognitive performance
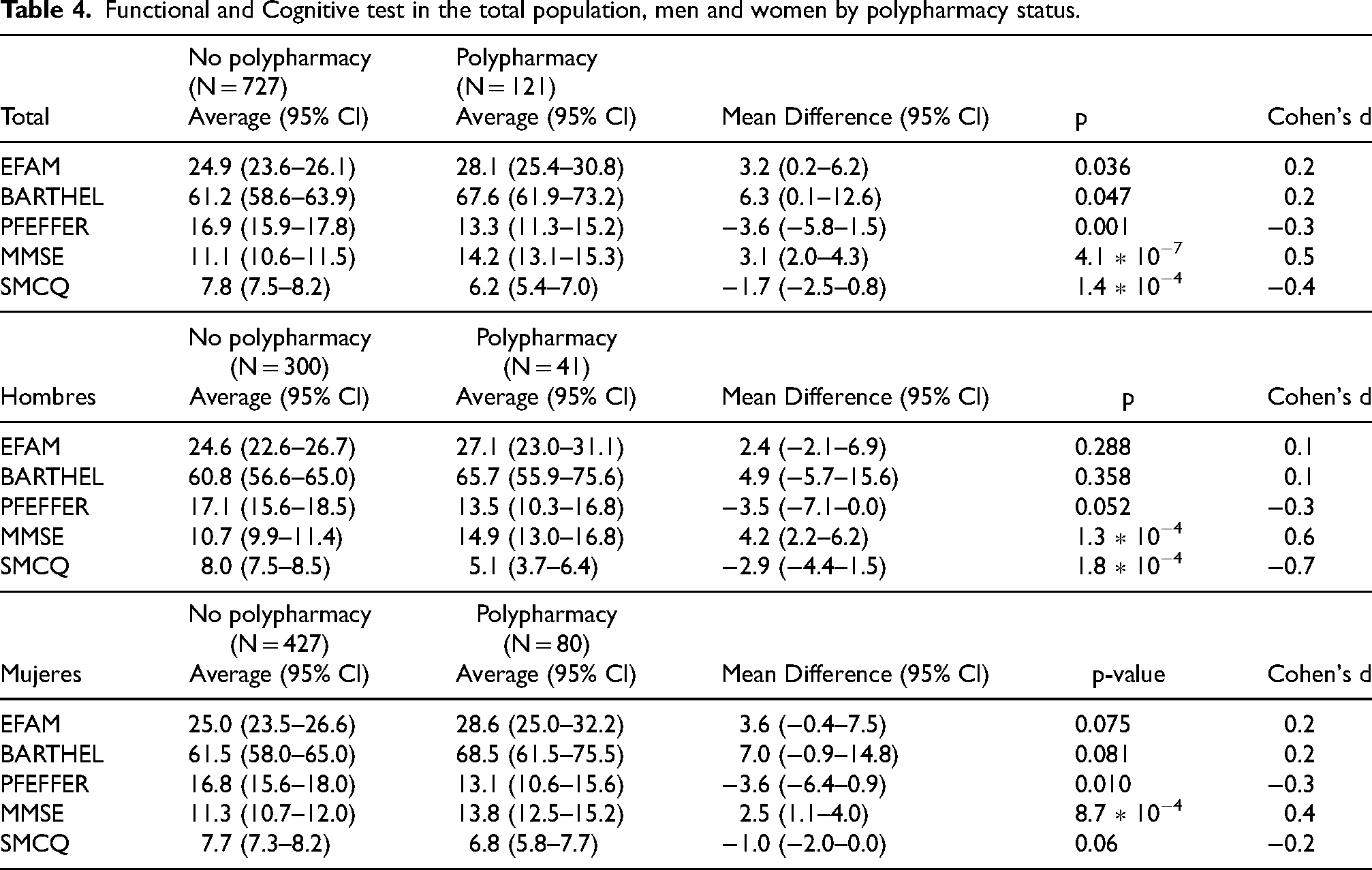
Participants with polypharmacy showed a more favorable functional profile, with higher EFAM and Barthel scores and lower Pfeffer scores. They also showed a more favorable cognitive screening profile, with higher education-adjusted MMSE scores and lower SMCQ scores. These patterns were directionally consistent in sex-stratified analyses, although not all subgroup comparisons reached statistical significance (Table 4,Figure 1).
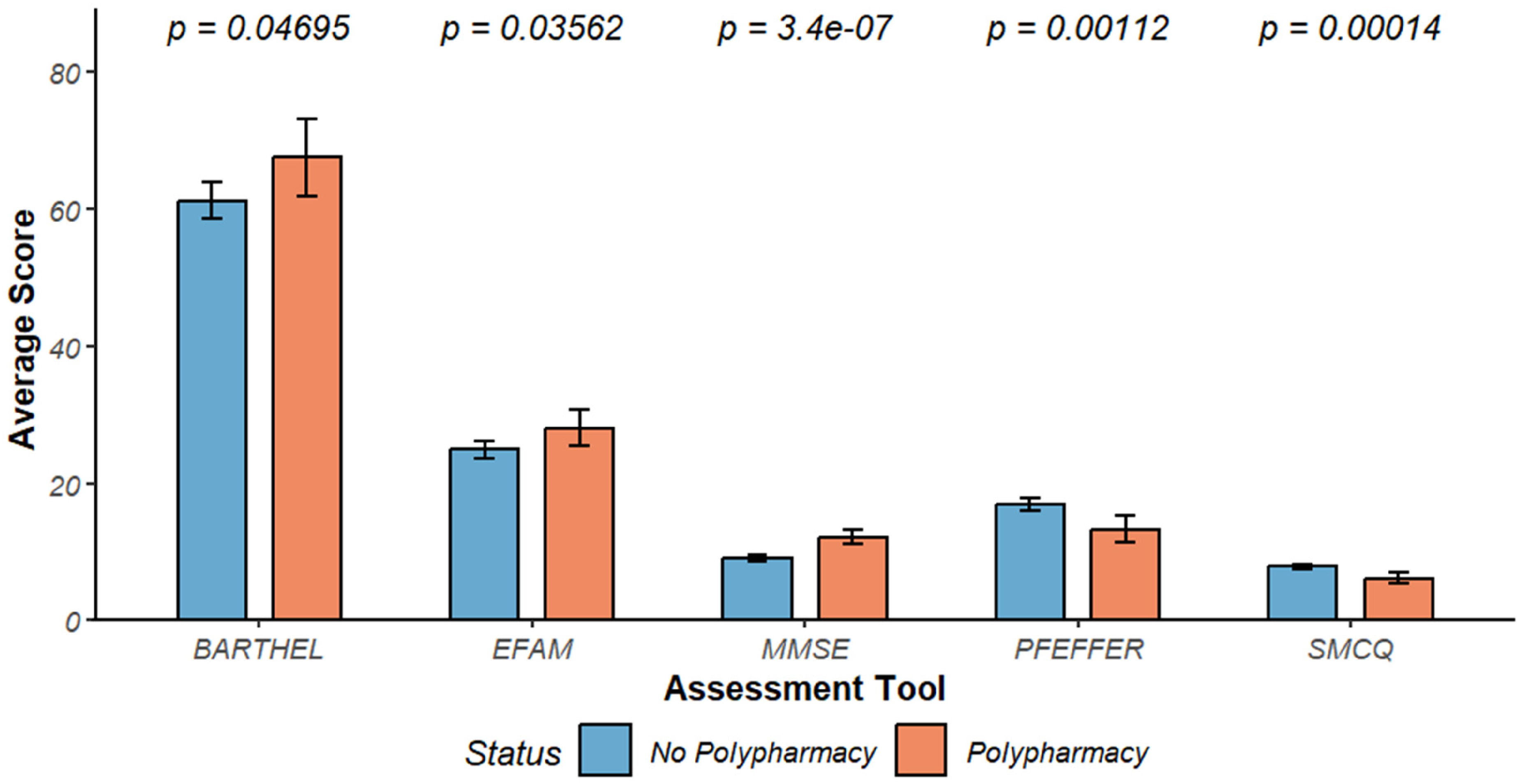
Mean (±95% CI) functional and cognitive scores according to polypharmacy status.
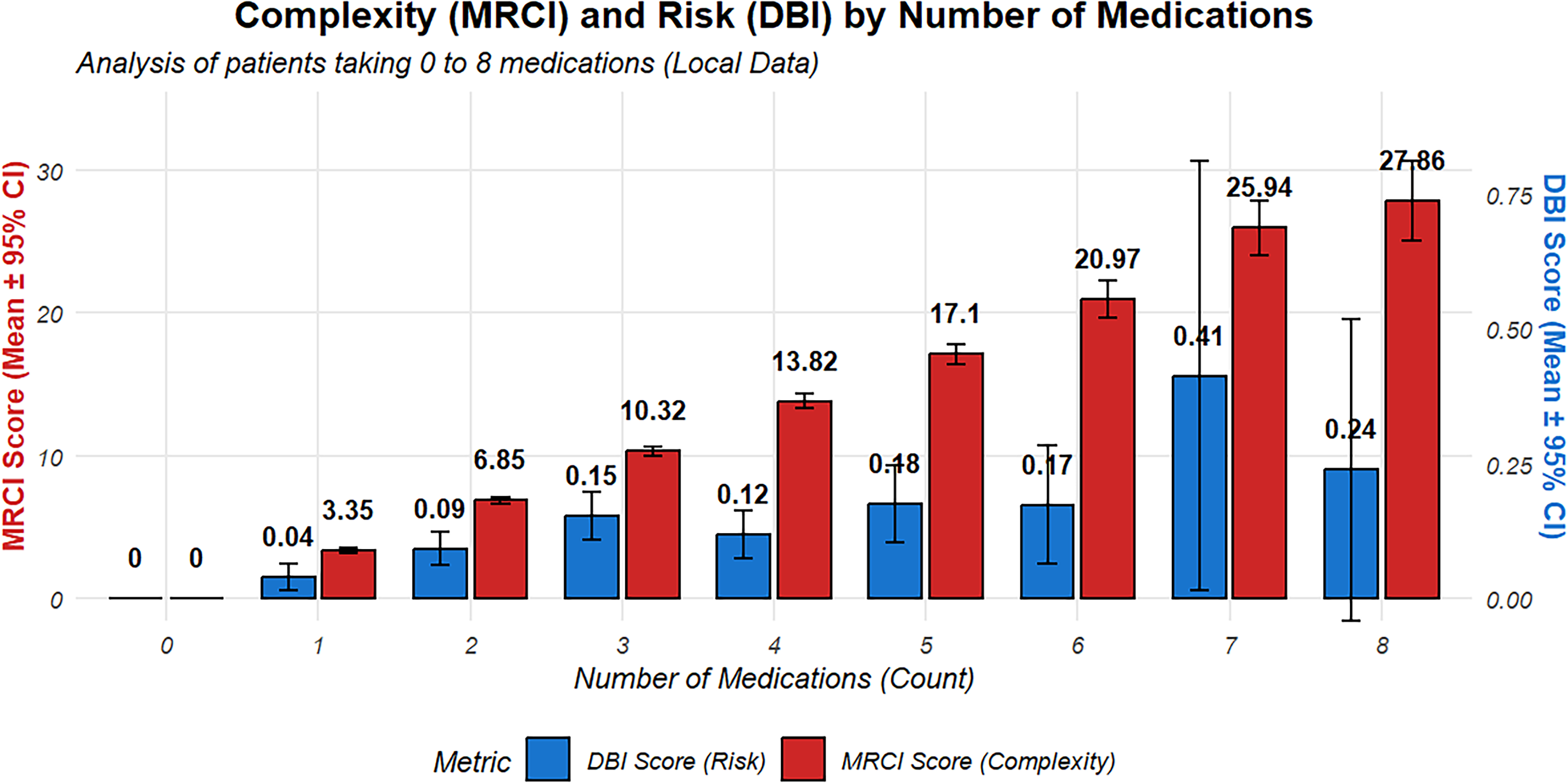
Histogram shows the distribution of Medication Regimen Complexity Index (MRCI, red) and Drug Burden Index (DBI, blue) according to the number of medications used.
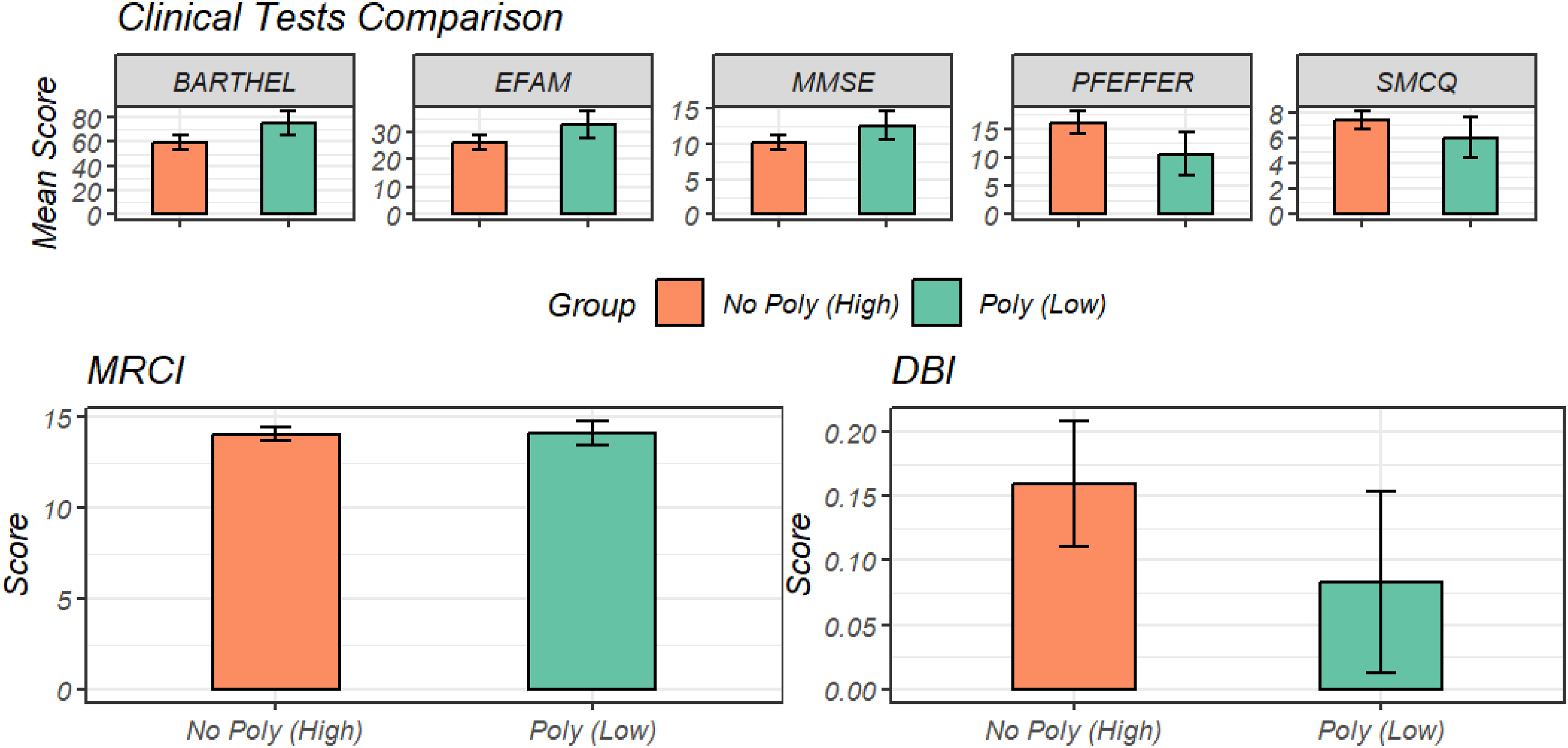
Comparison of functional (Barthel, EFAM, Pfeffer) and cognitive (MMSE, SMCQ) scores between individuals without polypharmacy but higher pharmacological burden/complexity (No Poly–High) and those with polypharmacy but lower burden/complexity (Poly–Low).
Functional and Cognitive test in the total population, men and women by polypharmacy status.
Use of specific groups of medicines by level of polypharmacy
Medication-use patterns were examined using the Anatomical Therapeutic Chemical (ATC) classification system (Table 5).
Percentage of population (60 years and older) using medicines, in function of ATC classification, according to polypharmacy status, Los Lagos region, 2024.
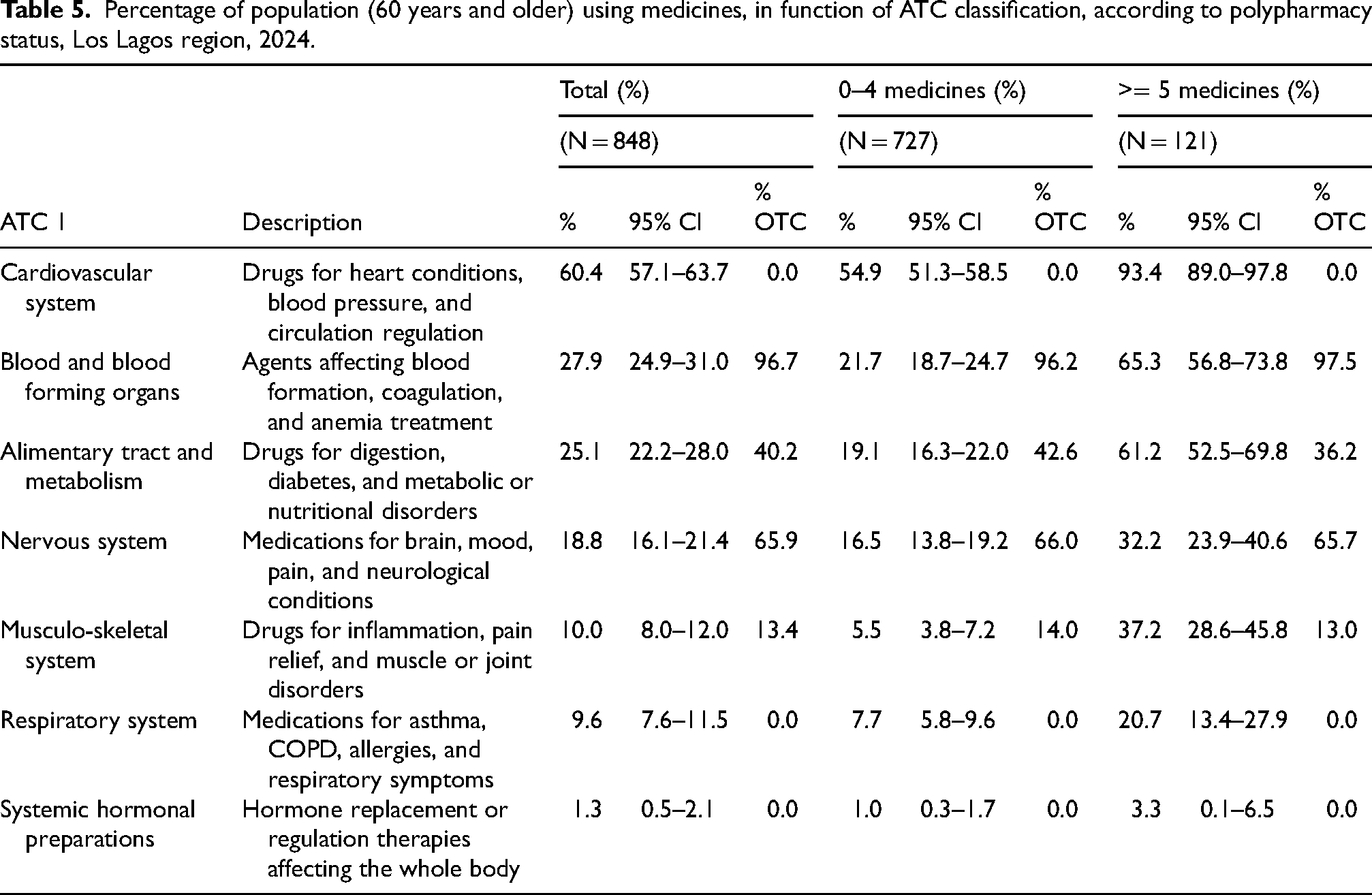
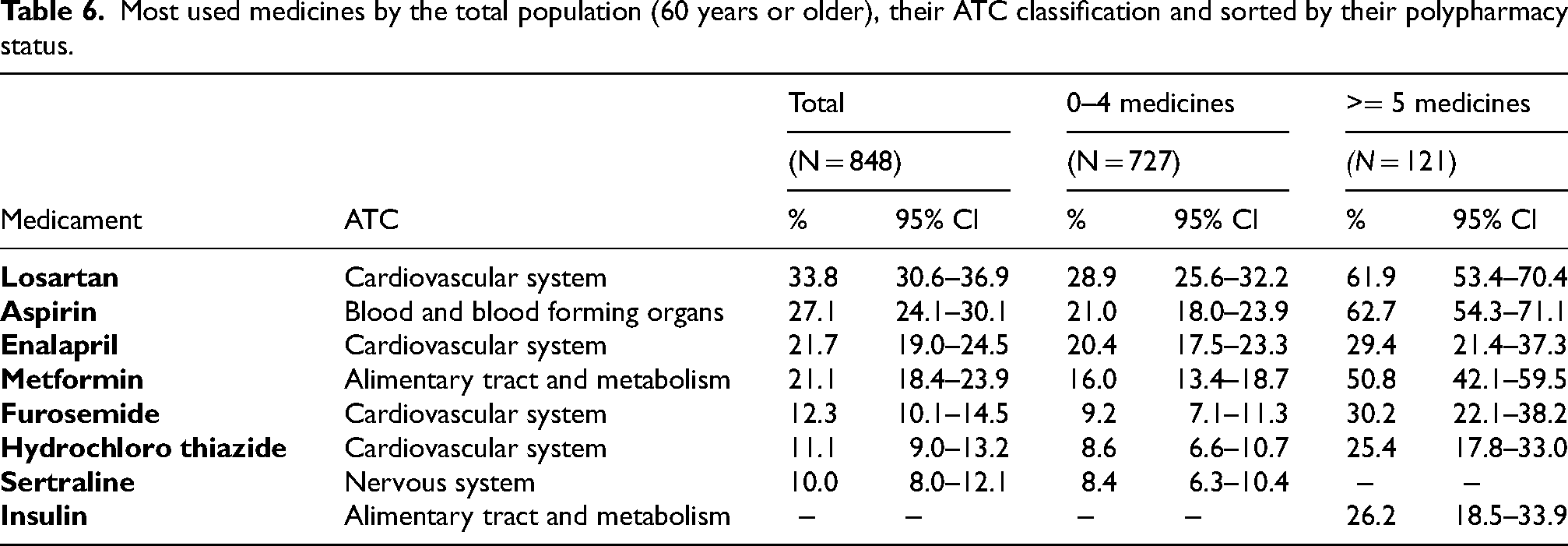
Cardiovascular drugs were the most frequently used ATC category, followed by blood and blood-forming agents and alimentary tract and metabolism drugs. Prevalence was consistently higher in the polypharmacy group across all major ATC categories. The revised Table 5 additionally shows the OTC contribution within each ATC category, which was greatest for blood and blood-forming organs, the nervous system, and alimentary/metabolism groups. At the individual-drug level, losartan, aspirin, metformin, and enalapril were the most frequently used medications (Table 5 and Table 6).
Most used medicines by the total population (60 years or older), their ATC classification and sorted by their polypharmacy status.
Regimen complexity and drug burden across medication-use groups
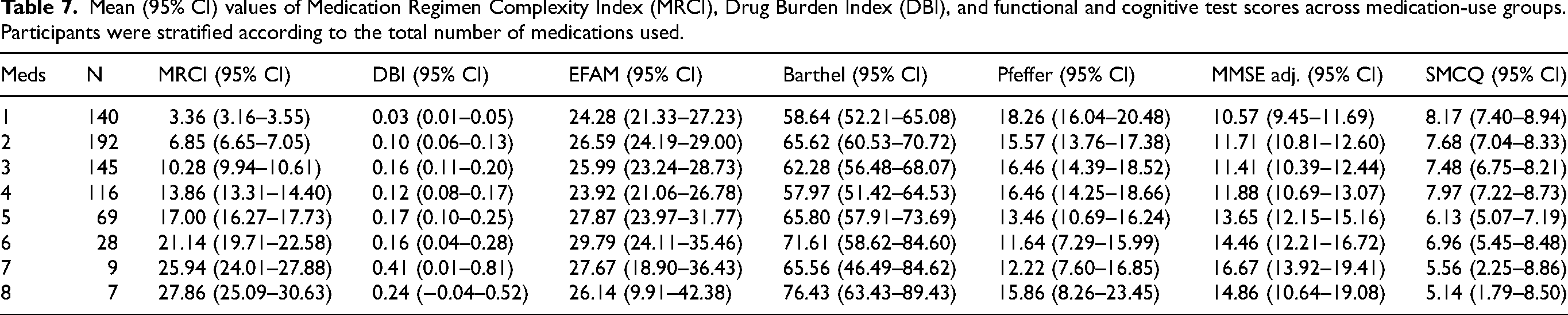
Medication regimen complexity (MRCI) and anticholinergic/sedative burden (DBI) increased progressively with the number of medications used (Table 7, Figure 2). Despite this increase, MRCI values remained within the low-to-moderate complexity range, and DBI values were consistently low across medication-use categories.
Mean (95% CI) values of Medication Regimen Complexity Index (MRCI), Drug Burden Index (DBI), and functional and cognitive test scores across medication-use groups. Participants were stratified according to the total number of medications used.
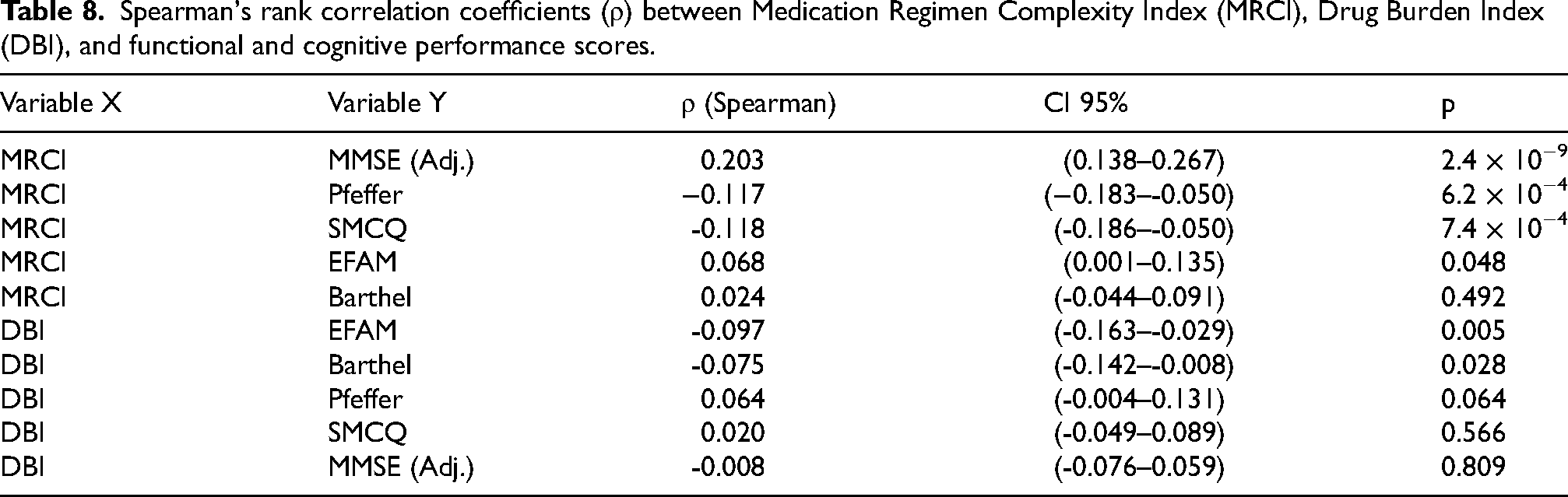
Higher MRCI scores were associated with better cognitive screening and lower functional impairment, whereas higher DBI scores were associated with worse functional outcomes and showed no significant correlation with cognitive measures (Table 8).
Spearman's rank correlation coefficients (ρ) between Medication Regimen Complexity Index (MRCI), Drug Burden Index (DBI), and functional and cognitive performance scores.
Comparative analysis of medication count versus pharmacological burden profiles
To further examine whether medication count alone adequately reflects medication-related vulnerability, we compared participants with polypharmacy but low pharmacological complexity/burden to participants without polypharmacy but higher complexity/burden.
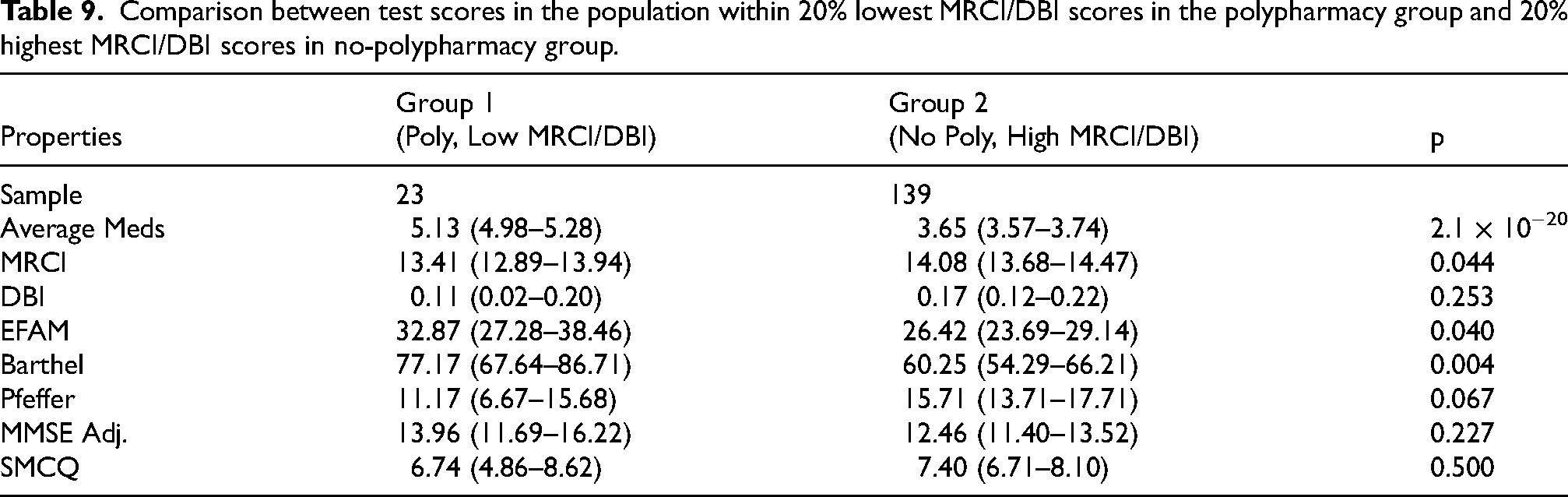
Despite using more medications on average, the polypharmacy–low burden group showed lower MRCI and DBI values and better functional performance, with a similar directional pattern for cognitive measures (Table 9, Figure 3).
Comparison between test scores in the population within 20% lowest MRCI/DBI scores in the polypharmacy group and 20% highest MRCI/DBI scores in no-polypharmacy group.
These findings highlight the dissociation between medication count and pharmacological burden, supporting the use of qualitative indices such as MRCI and DBI beyond medication count alone.
Discussion
In this cross-sectional study of community-dwelling older adults, we examined the associations between polypharmacy, medication regimen complexity (MRCI), anticholinergic/sedative burden (DBI), and cognitive–functional performance. The main finding is that polypharmacy, defined as the use of ≥5 medications, was not independently associated with worse cognitive performance after multivariable adjustment. Moreover, individuals with polypharmacy exhibited better functional and cognitive scores in unadjusted analyses. In our cohort, these findings suggest that medication count alone may be an insufficient indicator of cognitive vulnerability in older adults.
Our findings support the notion that the clinical relevance of medication exposure lies not in the number of drugs prescribed, but in their pharmacological profile and their relationship with underlying disease processes. Although polypharmacy has been consistently associated with adverse outcomes such as frailty, hospitalization, and mortality9,13 its relationship with cognitive decline remains heterogeneous and appears to be mediated by inappropriate prescribing, anticholinergic burden, and multimorbidity rather than medication count per se.7,30,31
In our cohort, multimorbidity was the primary determinant of medication use, while cognitive and functional measures were not independently associated with polypharmacy status after adjustment, reinforcing the role of clinical complexity as the main driver of medication exposure.
A central observation of this study is the low anticholinergic and sedative burden across medication-use strata. DBI values remained consistently low even among participants with polypharmacy, and were not independently associated with global cognitive performance as measured by the adjusted MMSE. This finding may explain the absence of negative cognitive associations, and is consistent with evidence indicating that the risk of dementia associated with anticholinergic exposure depends on cumulative dose, duration, and drug class rather than medication count.32,33 While high anticholinergic burden has been linked to increased dementia risk in large cohort studies,32,33 systematic reviews highlight methodological heterogeneity and limitations in causal inference, including confounding by indication and reverse causation 34
Furthermore, studies in community-based populations have reported inconsistent associations when overall exposure is low or moderate.35,36
In this context, our findings suggest that in low-exposure settings, anticholinergic/sedative burden may exert a greater impact on functional domains than on global cognitive screening measures, as reflected by the modest associations observed between DBI and functional outcomes.
An additional relevant finding is the positive association between medication regimen complexity (MRCI) and cognitive performance. A key limitation in the interpretation of this association is the high likelihood of reverse causation, whereby individuals with preserved executive function are more capable of managing complex pharmacological regimens, adhering to treatment, and accessing healthcare services. This may artificially generate a protective-looking association between regimen complexity and cognitive performance, rather than reflecting a true beneficial effect of pharmacological exposure. Although higher MRCI values were correlated with better MMSE scores, this relationship should not be interpreted as causal. A more plausible explanation is that individuals with preserved cognitive function and executive capacity are better able to manage complex medication regimens, reflecting a form of reverse causation or confounding by cognitive reserve.37,38
This interpretation is further supported by evidence showing that executive function and treatment capacity are key determinants of medication adherence and self-management in older adults. Therefore, regimen complexity may act as an indirect marker of preserved functional and cognitive capacity rather than a protective factor per se.
The pharmacological profile of this cohort provides important contextual insight. Medication use was predominantly driven by cardiometabolic therapies, including renin–angiotensin system inhibitors, antiplatelet agents, and glucose-lowering drugs. 39 This pattern differs substantially from clinical scenarios in which polypharmacy is dominated by centrally acting psychotropic or strongly anticholinergic medications. Evidence from observational and longitudinal studies suggests that certain cardiometabolic agents, such as statins and metformin, may be associated with reduced risk of cognitive decline and dementia,39,40 potentially through mechanisms involving vascular protection, reduced neuroinflammation, and metabolic regulation.39,40 In this context, polypharmacy driven by cardiometabolic management may reflect optimized control of modifiable dementia risk factors rather than a source of harm. 41 Participants without polypharmacy do not necessarily represent lower clinical complexity; in some cases, they may also reflect lower treatment intensity, undertreatment, reduced access to care, or poorer continuity of care 42
These findings should be interpreted with caution, as medication count alone does not capture the clinical appropriateness of treatment. Lower medication use may reflect either a lower burden of disease or, alternatively, undertreatment of existing conditions.
Therefore, the observed associations between polypharmacy and cognitive outcomes cannot be interpreted as evidence that fewer medications are necessarily beneficial.
The comparative analysis between medication count and pharmacological burden further supports this interpretation. Participants with polypharmacy but low MRCI/DBI values exhibited better functional performance than those without polypharmacy but with higher pharmacological burden. This finding underscores the dissociation between medication count and clinically relevant pharmacological exposure, and reinforces the value of qualitative indices such as DBI and MRCI in identifying medication-related vulnerability beyond simple numerical definitions.
Taken together, these findings support a shift from a quantitative to a qualitative framework in the evaluation of polypharmacy. Rather than focusing on reducing the number of medications per se, clinical strategies should prioritize the optimization of pharmacological profiles, minimizing exposure to high-risk agents, particularly those with anticholinergic or sedative properties, while maintaining therapies that contribute to the control of vascular and metabolic risk factors. 40 This perspective has direct implications for deprescribing strategies, which should evolve toward precision-based approaches tailored to individual risk profiles rather than uniform thresholds.
The results provide relevant insight into the complexity of medication use in aging populations. Rather than supporting a simplistic view of polypharmacy as inherently harmful, our findings highlight the importance of distinguishing between quantitative and qualitative dimensions of pharmacological exposure. In particular, they suggest that medication burden profiles such as anticholinergic load and regimen complexity may be more informative than medication count alone when assessing vulnerability in cognitive and functional domains.
From a neuropsychological and clinical perspective, these results underscore the need for a more nuanced framework in which medication use is interpreted in the context of underlying disease, cognitive reserve, and functional capacity. Future longitudinal studies incorporating comprehensive neuropsychological assessment and diagnostic evaluation are required to clarify the temporal and causal relationships between pharmacological exposure and cognitive decline. Such approaches will be essential to determine whether optimizing medication profiles can meaningfully contribute to the prevention or delay of dementia in aging populations.
Strength and limitations
This study has several limitations that should be considered when interpreting the findings. The cross-sectional design precludes causal inference and limits the ability to establish the temporal relationship between medication exposure and cognitive outcomes. In this context, the observed association between pharmacological complexity and cognitive performance may reflect reverse causation, as individuals with better preserved executive function, functional capacity, or cognitive reserve may be more capable of managing complex medication regimens.
Although recruitment extended beyond self-initiated healthcare attendance, the inclusion of participants who were able to complete the assessment protocol may have resulted in a sample biased toward individuals with relatively preserved functional and cognitive status. In addition, residual confounding cannot be excluded, particularly in relation to healthcare access, treatment adherence, and other unmeasured clinical factors.
Cognitive function was assessed using brief screening instruments. While MMSE scores were adjusted for education, this does not fully address measurement limitations in populations with very low educational attainment, including reduced sensitivity, educational bias, and potential floor effects. Although the observed variability in MMSE scores suggests that a floor effect alone is unlikely to fully explain the findings, these instruments may still fail to capture subtle or domain-specific cognitive impairment. Accordingly, the results should be interpreted as screening-based associations rather than definitive evidence of cognitive status.
Medication exposure was characterized using both count-based and qualitative indices; however, prescribing appropriateness, treatment indications, and unmet clinical needs were not assessed in sufficient detail. As such, lower medication counts should not be interpreted as indicative of better clinical status, as undertreatment of chronic conditions remains a plausible alternative explanation.
Finally, although over-the-counter medications were included in the definition of polypharmacy, some degree of misclassification may persist due to recall bias or incomplete reporting of non-prescribed drug use.
Despite these limitations, this study provides novel evidence from a large community-based Latin American cohort, highlighting the importance of pharmacological quality over quantity in the evaluation of medication-related cognitive risk.
Footnotes
Acknowledgements
We gratefully acknowledge the Government of the Los Lagos Region and the Municipal Health Department of the Ilustre Municipalidad de Puerto Montt, Los Lagos Region, Chile, for their valuable institutional support and for facilitating access to healthcare users across the provinces of Osorno, Llanquihue, Puerto Montt, and Chiloé.
Ethical considerations
The study was reviewed and approved by an accredited Research Ethics Committee N°: 24-2023. The research was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and applicable national regulations governing research involving human subjects. Participant confidentiality and data anonymization were ensured throughout the study.
Consent to participate
All participants were fully informed about the objectives and procedures of the study and provided written informed consent prior to enrollment.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Agencia Nacional de Investigación y Desarrollo (ANID), Chile, under grant FONIS SA24I0065, and received additional institutional support from Interdisciplinary Project No. 11340012.; Fondo Nacional de Desarrollo Científico y Tecnológico.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author.