
Abstract
Background
The associations between agitation, cerebrospinal fluid (CSF) biomarkers, and cognitive decline, and whether these relationships vary by APOE genotype, remain unclear in Alzheimer's disease (AD) and mild cognitive impairment (MCI).
Objective
To investigate the association between CSF biomarkers and agitation in cognitively impaired individuals, with a focus on the potential moderating role of APOE ε4 status.
Methods
We analyzed 491 cognitively impaired individuals (359 MCI and 132 AD) from the Alzheimer's Disease Neuroimaging Initiative (ADNI) with available CSF biomarker data. Neuropsychiatric symptoms were assessed using the Neuropsychiatric Inventory (NPI), focusing on agitation.
Results
Among APOE ε4 carriers, agitation was significantly associated with higher CSF GAP-43 (OR = 1.584, 95% CI: 1.159–2.195, p = 0.005) and p-tau levels (OR = 1.49, 95% CI: 1.073–2.101, p = 0.02). These associations were not observed in non-carriers. In addition, APOE ε4 carriers with agitation showed a higher risk of progression to dementia compared with other groups (HR = 4.422, 95% CI: 2.542–7.692, p < 0.001).
Conclusions
CSF GAP-43 and p-tau levels are associated with agitation in APOE ε4 carriers. Agitation in this subgroup is also associated with an increased risk of progression to dementia, suggesting that it may reflect underlying disease-related processes.
Introduction
Alzheimer's disease (AD) has a high prevalence and poses a significant societal burden, making early identification and intervention crucial. Neuropsychiatric symptoms (NPS) are common across the AD clinical continuum, from mild cognitive impairment (MCI) to dementia, and often precede overt cognitive decline.1–3 Among them, agitation is particularly prevalent, affecting approximately 60% of patients with MCI and up to 76% of those with AD, 4 and it substantially reduces quality of life for patients and caregivers. 5 Despite its clinical significance, the biological mechanisms underlying agitation in AD remain poorly understood. Notably, previous studies examining the associations between agitation and core AD pathologies, including amyloid-β (Aβ) and tau, have yielded inconsistent findings,6–8 suggesting that traditional pathological frameworks may not fully explain the emergence of neuropsychiatric symptoms.
Emerging evidence indicates that synaptic dysfunction is a central feature of AD pathophysiology and may link molecular pathology to clinical manifestations.9–11 Importantly, converging evidence from psychiatric disorders implicates synaptic dysfunction in the development of behavioral and emotional symptoms,12–14 suggesting that synaptic vulnerability may represent a shared mechanistic pathway underlying both neurodegeneration and neuropsychiatric symptoms. In this context, cerebrospinal fluid (CSF) growth-associated protein 43 (GAP-43), a presynaptic protein involved in synaptic plasticity and remodeling, has emerged as a promising biomarker of synaptic integrity. Postmortem studies have shown that GAP-43 expression is reduced in the frontal cortex of patients with AD. Moreover, CSF GAP-43 levels are associated with Aβ-related tau pathology and cognitive decline.15–18 However, the relationship between agitation and CSF GAP-43 remains unclear among individuals with cognitive impairment.
Accumulating evidence suggests that psychiatric disorders and neurodegenerative diseases share common genetic and molecular foundations. 19 Genetic factors may further modulate the relationship between synaptic dysfunction and neuropsychiatric manifestations. The apolipoprotein E (APOE) ε4 allele, the strongest genetic risk factor for sporadic AD, has been shown to exacerbate Aβ deposition, tau pathology, and synaptic impairment.20,21 Beyond its role in AD pathology, recent evidence suggests that APOE ε4 may also increase susceptibility to agitation, independent of disease severity. 22 These findings raise the possibility that APOE ε4 may act as a biological amplifier, enhancing the impact of synaptic vulnerability and tau pathology on behavioral symptoms.
Therefore, this study aimed to investigate the association between CSF biomarkers of AD and agitation in AD and MCI, and whether this association is moderated by APOE ε4 status. In addition, we examined whether the combined presence of agitation and APOE ε4 predicts cognitive progression in MCI.
Methods
Study population
This study used the database from the ADNI (https://adni.loni.usc.edu), which was launched in 2003 as a public-private partnership, led by Principal Investigator Michael W. Weiner, MD. The original goal of ADNI was to test whether serial magnetic resonance imaging (MRI), positron emission tomography (PET), other biological markers, and clinical and neuropsychological assessment can be combined to measure the progression of MCI and early AD. The ADNI study was approved by the institutional review boards of all participating centers, and all participants provided written informed consent. This study was carried out according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. 23
The data were acquired in November 2025. Participants were included if they had a clinical diagnosis of AD or MCI and available data on CSF GAP-43, Mini-Mental State Examination (MMSE), Neuropsychiatric Inventory (NPI), age, sex, and APOE genotype. Participants were excluded if they had major depression or bipolar disorder within the previous 12 months, or exhibited psychotic features or significant behavioral disturbances within three months prior to screening. In addition, individuals with significant neurological disorders other than AD (e.g., Parkinson's disease, Huntington's disease, multiple sclerosis, or brain tumors) were excluded.
The ADNI criteria for MCI were: 1) subjective memory complaints; 2) objective memory loss defined as scoring below an education adjusted cut-off score on delayed recall of the Wechsler Memory Scale-Revised (WMS-R) logical memory test II subscale: ≤ 11 for 16 or more years of education, ≤ 9 for 8–15 years of education, and ≤ 6 for 0–7 years of education (the maximum score is 25); 3) a global Clinical Dementia Rating (CDR) score of 0.5, memory box score must be at least 0.5; 4) a Mini-Mental State Examination (MMSE) score of equal to, or higher than 24 (the maximum score is 30); and 5) general cognitive and functional performance sufficiently preserved such that a diagnosis of dementia could not be made by the site physician at the time of screening. The ADNI criteria for AD were: 1) subjective memory concern; 2) abnormal memory function documented by scoring within the education-adjusted ranges on the WMS-R logical memory II: ≤ 8 for 16 or more years of education, ≤ 4 for 8–15 years of education, ≤ 2 for 0–7 years of education (the maximum score is 25); 3) MMSE score between 20 and 26 (inclusive); 4) CDR ≥ 0.5; 5) met the NINCDS/ADRDA criteria for probable AD. 24 Cognitive progression was defined as conversion from MCI to AD during the follow-up.
Neuropsychological assessment
Cognitive function was evaluated using the MMSE and the CDR–Sum of Boxes (CDR-SB) to assess dementia severity. Depressive symptoms were assessed using the 15-item Geriatric Depression Scale (GDS), with a score of ≥6 indicating depression. 25
Assessment of NPS
NPS were assessed using the Neuropsychiatric Inventory (NPI), an informant-based scale that evaluates 12 neuropsychiatric domains through a structured caregiver interview. In the present study, all domains were dichotomized as present (score ≥1) or absent (score = 0), with analysis focused solely on the agitation domain.
APOE genotype
APOE genotype data for ADNI-GO and ADNI-2 participants were obtained from the ADNI Genetics Core. Genotyping was performed by Prevention Genetics and LGC Genomics using PCR-based allele-specific methods, followed by quality control. Final, quality-controlled genotypes were made available through the ADNI LONI database. 26
Fluid biomarkers
CSF Aβ42, phosphorylated tau (P-tau) 181 were measured by fully automated Elecsys® assays (Roche Diagnostics). CSF measures from ADNI, with notes indicating potential analytical problems (e.g., above limit of quantification), were removed from analysis. 27 CSF GAP-43 levels were assessed using an in-house enzyme-linked immunosorbent assay at the Clinical Neurochemistry Laboratory of Sahlgrenska University Hospital, Mölndal, Sweden, as described previously. 18 To ensure temporal consistency between biomarkers, only participants whose CSF GAP-43 measurements were obtained within one year of the CSF p-tau assessment were retained for analysis.
Neuroimaging
All MRI and Aβ-PET examinations were performed according to standardized ADNI imaging protocol. Cerebral Aβ deposition was assessed using [18F] Florbetapir PET imaging. Composite regions of interest (including frontal, anterior/posterior cingulate, lateral parietal, and lateral temporal cortices) were defined, and the summary standardized uptake value ratio (SUVR) was calculated using the whole cerebellum as reference. Participants were classified as amyloid-PET positive if their global SUVR exceeded the established threshold of 1.11 as recommended by ADNI. 28 To ensure temporal consistency between PET and CSF biomarkers, PET data acquired more than 365 days from CSF collection were not included in the analysis and were coded as missing. White matter hyperintensity (WMH) quantification was performed using a Bayesian probabilistic segmentation framework integrating high-resolution 3D T1-weighted and fluid-attenuated inversion recovery (FLAIR) sequences. Native-space T1 images were automatically segmented into grey matter, white matter, and CSF compartments through validated pipelines, with hippocampal volume derived from automated segmentation.
Statistical analysis
Differences between groups were compared using Student's t-test or Mann–Whitney U test for continuous variables, and the chi-square test or Fisher's exact test for categorical variables. CSF biomarkers were log-transformed and standardized (centered to mean zero and scaled to unit variance) before regression analyses.
Interaction terms between CSF biomarkers and APOE ε4 status were first tested to assess potential effect modification. Additional moderation analyses considered age, sex, and Aβ-PET positivity. Main-effect models were constructed as follows: Model 1 was adjusted for age, sex, education, and clinical diagnosis; Model 2 was additionally adjusted for GDS score, antidepressant use, and benzodiazepine use. Stratified analyses by APOE ε4 status were performed when appropriate. Multiple comparisons were controlled using the Benjamini–Hochberg false discovery rate (FDR) method. Spearman correlation was used to assess associations between CSF biomarkers and agitation scores. Sensitivity analyses tested the robustness of primary associations, including further adjustment for smoking, alcohol use, medical comorbidities, and WMH volume, as well as subgroup analyses among Aβ-PET positive participants or after excluding individuals with depression or sleep medication use.
For longitudinal outcomes in the MCI cohort, survival analyses were performed to examine the risk of conversion to dementia. Kaplan–Meier curves were generated for each group and compared using the log-rank test. Cox proportional hazards models were applied with the Agitation-/APOE- group as the reference. Model 1 was adjusted for age, sex, and education; Model 2 was additionally adjusted for GDS score, antidepressant use, and benzodiazepine use. Hazard ratios (HRs) with 95% confidence intervals were reported. All analyses were performed using R version 4.5.2.
Results
Demographic characteristics
Participants were stratified by APOE ε4 carrier status, including 222 non-carriers (APOE−) and 269 carriers (APOE+), as shown in Table 1. The mean age was 74.05 years in the APOE− group and 72.2 years in the APOE + group. Compared with the APOE− group, APOE + group had a higher prevalence of AD and poorer cognitive performance. They also exhibited smaller hippocampal volumes and a substantially greater prevalence of Aβ-PET positivity (86.9% versus 41.6%). Hyperlipidemia was also more common among APOE + carriers (p = 0.006). Regarding CSF biomarkers, APOE + individuals exhibited lower Aβ42 but higher p-tau, GAP-43, and p-tau/Aβ42 ratios. The prevalence of the 12 NPS assessed by the NPI did not differ significantly between APOE groups.
Demographic, neuropsychological, and biomarker characteristics of the total sample and grouped by apolipoprotein E ε4 allele carriage.
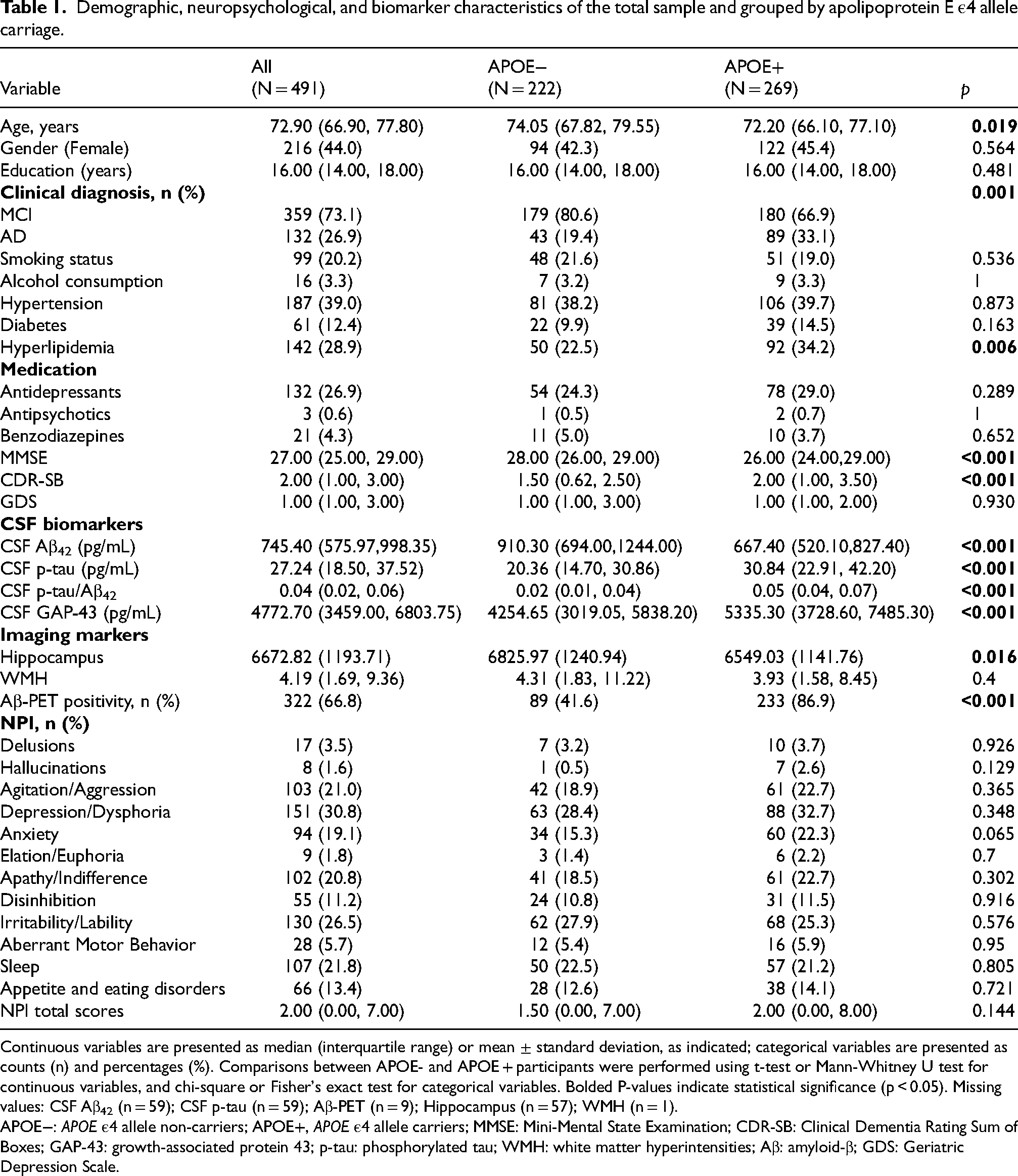
Continuous variables are presented as median (interquartile range) or mean ± standard deviation, as indicated; categorical variables are presented as counts (n) and percentages (%). Comparisons between APOE- and APOE + participants were performed using t-test or Mann-Whitney U test for continuous variables, and chi-square or Fisher's exact test for categorical variables. Bolded P-values indicate statistical significance (p < 0.05). Missing values: CSF Aβ42 (n = 59); CSF p-tau (n = 59); Aβ-PET (n = 9); Hippocampus (n = 57); WMH (n = 1).
APOE−: APOE ε4 allele non-carriers; APOE+, APOE ε4 allele carriers; MMSE: Mini-Mental State Examination; CDR-SB: Clinical Dementia Rating Sum of Boxes; GAP-43: growth-associated protein 43; p-tau: phosphorylated tau; WMH: white matter hyperintensities; Aβ: amyloid-β; GDS: Geriatric Depression Scale.
Participants were further stratified by agitation status, including 388 individuals without agitation (Agitation−) and 103 with agitation (Agitation+), as shown in Table 2. The mean age was 72.7 years in the Agitation− group and 74.4 years in the Agitation + group. Compared with Agitation− individuals, those with agitation had a lower proportion of females (32% versus 47.2%), a higher prevalence of AD, and poorer cognitive performance (higher CDR-SB scores). They also had smaller hippocampal volumes, whereas WMH and Aβ-PET positivity did not differ. Regarding CSF biomarkers, the p-tau/Aβ42 ratio was higher in the Agitation + group. Agitation + individuals also exhibited higher prevalence of most other NPS assessed by the NPI, except hallucinations.
Demographic, neuropsychological, and biomarker characteristics of the total sample and grouped by agitation status.
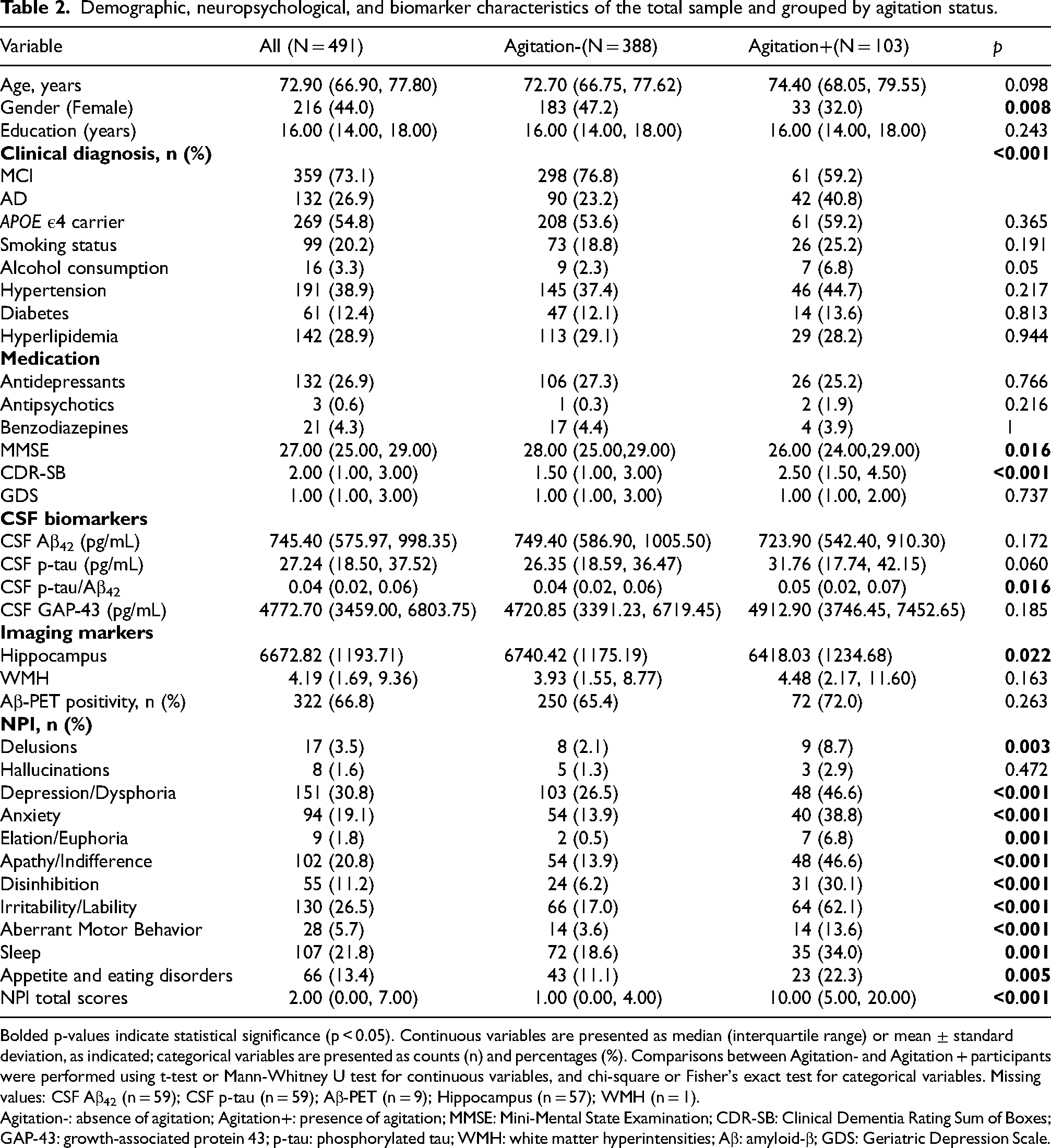
Bolded p-values indicate statistical significance (p < 0.05). Continuous variables are presented as median (interquartile range) or mean ± standard deviation, as indicated; categorical variables are presented as counts (n) and percentages (%). Comparisons between Agitation- and Agitation + participants were performed using t-test or Mann-Whitney U test for continuous variables, and chi-square or Fisher's exact test for categorical variables. Missing values: CSF Aβ42 (n = 59); CSF p-tau (n = 59); Aβ-PET (n = 9); Hippocampus (n = 57); WMH (n = 1).
Agitation-: absence of agitation; Agitation+: presence of agitation; MMSE: Mini-Mental State Examination; CDR-SB: Clinical Dementia Rating Sum of Boxes; GAP-43: growth-associated protein 43; p-tau: phosphorylated tau; WMH: white matter hyperintensities; Aβ: amyloid-β; GDS: Geriatric Depression Scale.
Moderation of APOE ε4 status on the association between agitation and CSF biomarkers
Interaction analyses revealed a significant interaction between APOE ε4 status and CSF GAP-43 (p = 0.008). Participants were then stratified by APOE ε4 status. Among APOE ε4 carriers, those with agitation exhibited higher CSF GAP-43 and p-tau levels compared with those without agitation (p < 0.05; Figure 1A–D). Logistic regression indicated that agitation was significantly associated with CSF GAP-43 (OR = 1.584, 95% CI: 1.159–2.195, p = 0.005) and CSF p-tau (OR = 1.49, 95% CI: 1.073–2.101, p = 0.02), but not with CSF Aβ42 (OR = 1.121, 95% CI: 0.814–1.552, p = 0.487) or the p-tau/Aβ42 ratio (OR = 1.278, 95% CI: 0.914–1.816, p = 0.16). These associations remained significant after further adjustment for GDS score, antidepressant use, and benzodiazepine use (Model 2).
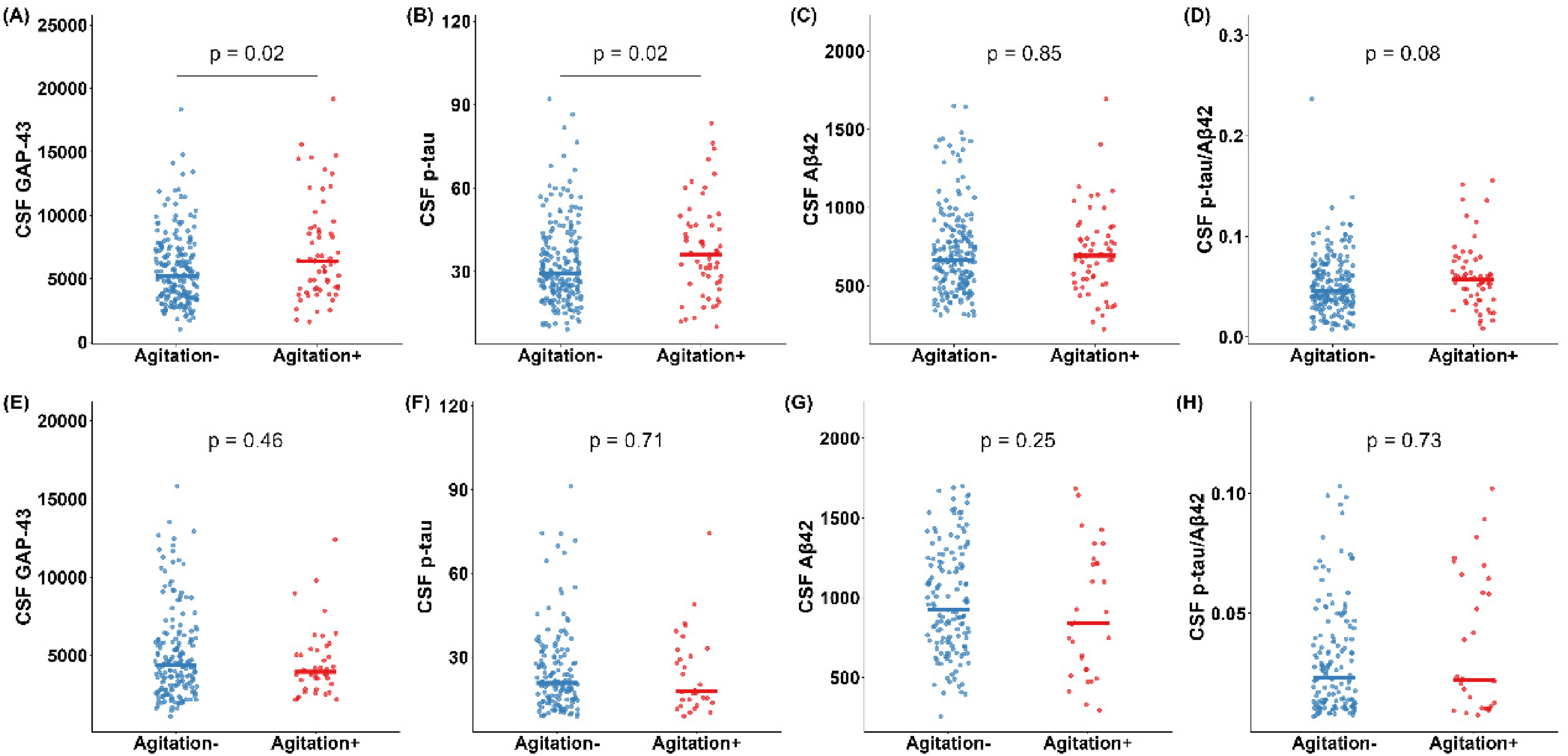
Associations between agitation and CSF biomarkers in participants stratified by APOE ε4 status. (A-D) APOE ε4 carriers; (E-H) APOE ε4 non-carriers.
In APOE ε4 non-carriers, no significant differences in biomarker levels were observed between agitation groups (Figure 1E–H), and regression models showed no significant associations (Table 3). No significant interactions were found for Aβ-PET positivity, sex, or age (Supplemental Table 1).
Associations of agitation with CSF biomarkers stratified by APOE ε4 carrier status.
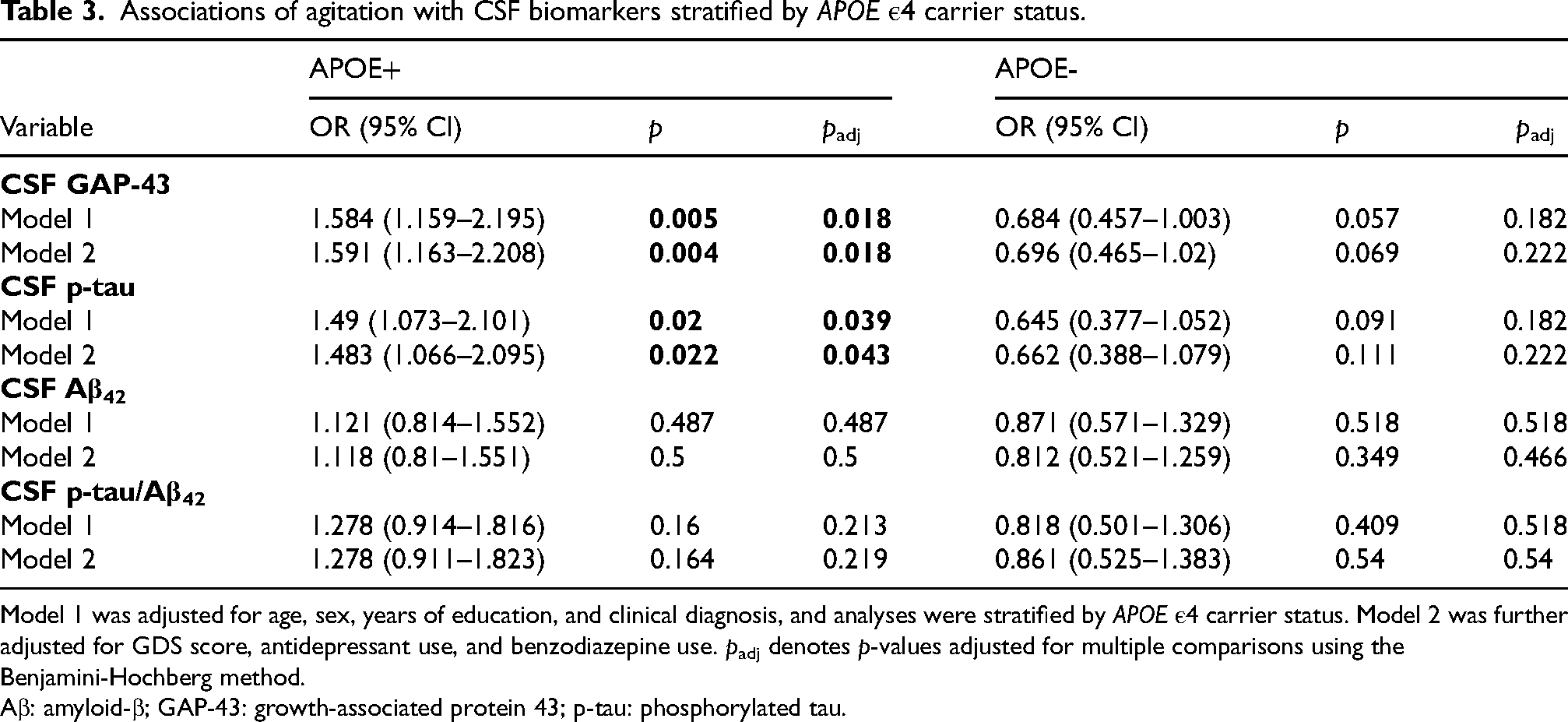
Model 1 was adjusted for age, sex, years of education, and clinical diagnosis, and analyses were stratified by APOE ε4 carrier status. Model 2 was further adjusted for GDS score, antidepressant use, and benzodiazepine use. padj denotes p-values adjusted for multiple comparisons using the Benjamini-Hochberg method.
Aβ: amyloid-β; GAP-43: growth-associated protein 43; p-tau: phosphorylated tau.
Correlation analyses
Spearman correlations showed weak but statistically significant positive correlations between CSF GAP-43 and agitation total scores (r = 0.133, p = 0.03), and between CSF p-tau and agitation scores (r = 0.127, p = 0.041) among APOE ε4 carriers.
Sensitivity analyses
The associations remained robust after additional adjustment for smoking, alcohol use, medical comorbidities and white matter hyperintensities. Among Aβ-PET positive participants, CSF GAP-43 remained significantly associated with agitation (OR = 1.602, p = 0.006), whereas the association with p-tau approached statistical significance (OR = 1.376, p = 0.06). Excluding participants with depression (GDS score ≥ 6) did not materially change these results. Similarly, after excluding participants using sleep medications, CSF GAP-43 continued to show a significant association with agitation (OR = 1.491, p = 0.016), while the association with p-tau again approached statistical significance (OR = 1.393, p = 0.053) (Supplemental Tables 2–5).
Survival analysis for conversion to dementia
Of the 359 participants with MCI, 18 had only one observation and were not included in the survival analysis. Therefore, we analyzed 341 participants in the survival analysis, of whom 122 experienced cognitive progression. Kaplan-Meier curves showing survival from conversion to MCI or dementia in the four groups are depicted in Figure 2.
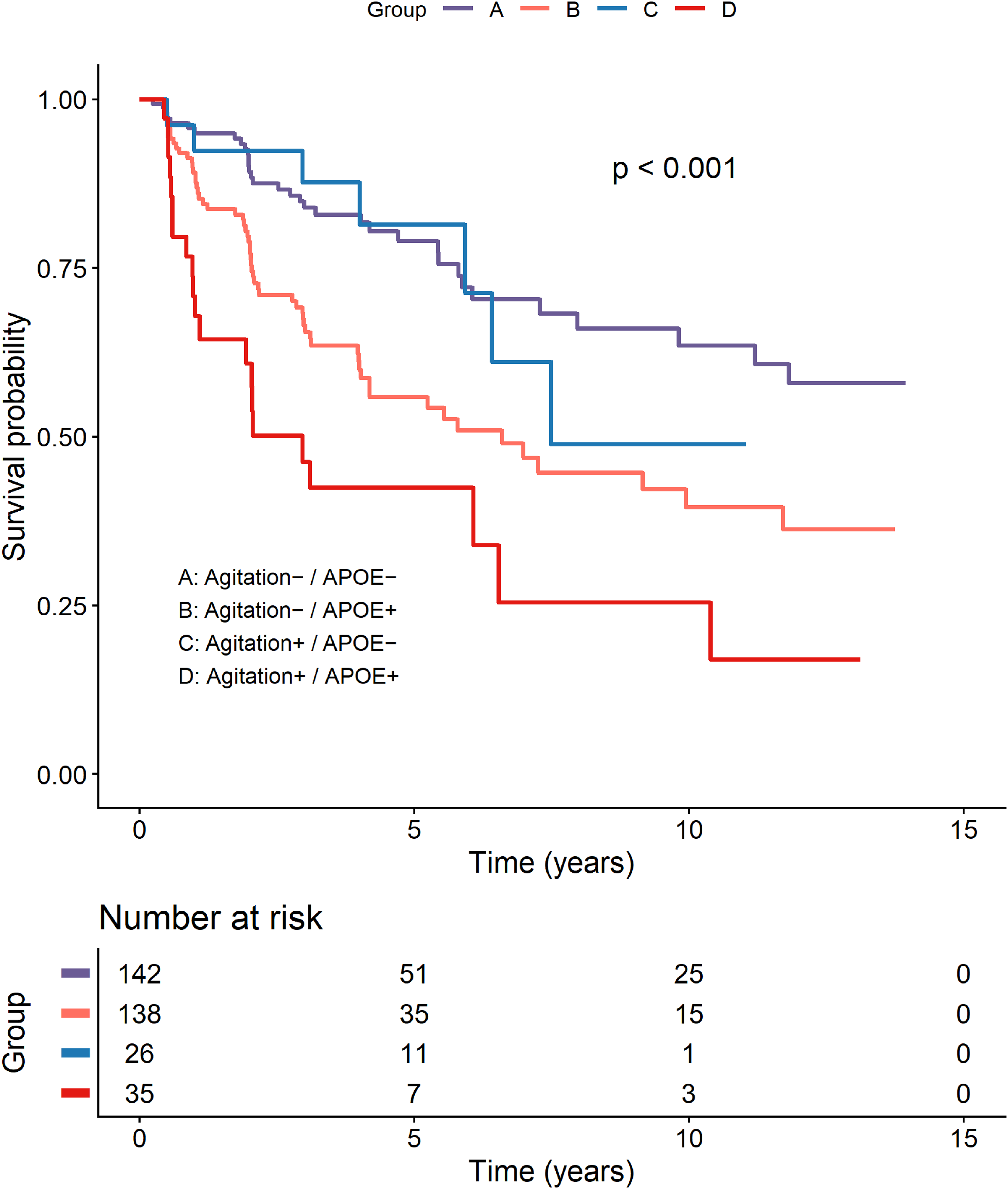
Kaplan–Meier curves showing progression to dementia stratified by agitation status and APOE ε4 carrier status.
Compared with the reference group (Agitation−/APOE−), the Agitation+/APOE + group had the highest risk of conversion to dementia (HR = 4.422, 95% CI: 2.542–7.692, p < 0.001). The Agitation−/APOE + group also exhibited an increased risk (HR = 2.291,95% CI: 1.499–3.501, p < 0.001), whereas the Agitation+/APOE− group showed no significant increase (HR = 0.843, 95% CI: 0.367–1.937, p = 0.687) (Table 4). These associations remained robust after additional adjustment for GDS score, antidepressant use, and benzodiazepine use (Model 2). Proportional hazards assumption was confirmed using Schoenfeld residuals (p > 0.05), and no multicollinearity was detected among covariates (all VIF < 2).
Cox proportional hazard ratios for conversion to dementia.
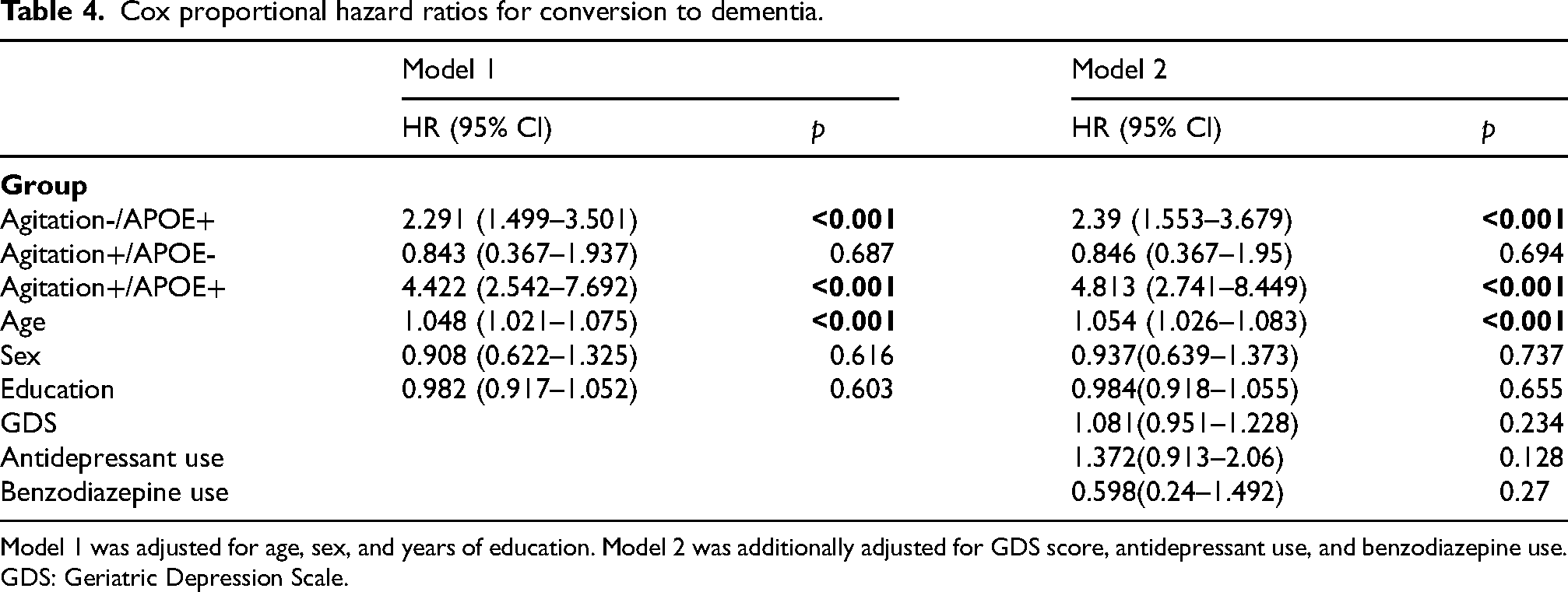
Model 1 was adjusted for age, sex, and years of education. Model 2 was additionally adjusted for GDS score, antidepressant use, and benzodiazepine use. GDS: Geriatric Depression Scale.
Discussion
In this study, we observed that APOE ε4 status significantly modulates the association between agitation and CSF biomarkers, particularly p-tau and GAP-43. Among APOE ε4 carriers, agitation was specifically associated with elevated CSF p-tau and GAP-43 levels and a higher risk of progression to dementia. These findings suggest a potential interaction among genetic risk, neuropathology, and behavioral symptoms, and highlight the importance of stratifying individuals by genetic susceptibility and neuropsychiatric profiles to better predict risk and characterize AD.
Among participants with cognitive impairment, agitation was more frequently observed in males. This may reflect sex-related differences in neuropsychiatric vulnerability, consistent with previous reports. 29 Agitation-positive individuals also exhibited greater neuropathological burden, including smaller hippocampal volumes and elevated CSF p-tau levels. These results support a more specific link between agitation and tau-related neurodegeneration, rather than amyloid-β deposition.30,31 The APOE ε4 allele is a major genetic risk factor for AD and has been strongly associated with amyloid-β accumulation, tau phosphorylation, and synaptic dysfunction.21,32 In our study, agitation was not directly associated with APOE ε4 status. However, among APOE ε4 carriers, those with agitation showed significantly higher CSF GAP-43 and p-tau levels than those without agitation, whereas no such differences were observed among non-carriers. These findings suggest an interaction between synaptic vulnerability and genetic risk in the development of neuropsychiatric symptoms, highlighting a gene–pathology mechanism underlying agitation in AD.
Mechanistically, the association between GAP-43 and agitation in APOE ε4 carriers may reflect converging pathological processes centered on synaptic dysfunction. Microglial activation has been implicated in agitation in AD.33,34 GAP-43, a marker of synaptic remodeling, has been linked to microglial activity; for example, TREM2-related microglial activation has been associated with increased CSF GAP-43 levels.35,36 Both agitation and elevated GAP-43 levels have also been linked to neuroinflammation.37,38 Vascular factors may also contribute, as cerebral microbleeds and small vessel disease have been associated with hyperactive neuropsychiatric symptoms, including agitation, 39 and may contribute to neuronal injury and network disruption. CSF GAP-43 has also been linked to cerebral microbleeds, suggesting that vascular pathology may be related to synaptic alterations. 40 In addition, GAP-43 levels may be influenced by tau-related synaptic toxicity, 41 which is associated with impaired synaptic integrity.
In our study, the association between GAP-43 and agitation was observed only in APOE ε4 carriers. This finding is consistent with previous reports showing that APOE ε4 modulates the relationship between GAP-43 and longitudinal hippocampal volume as well as cognitive decline, 42 suggesting a role for APOE in linking synaptic vulnerability to clinical phenotypes. This APOE ε4-specific effect observed in our study may therefore reflect an amplification of synaptic susceptibility under APOE ε4–related pathological conditions, and may help explain previously inconsistent findings regarding GAP-43 and neuropsychiatric symptoms in unstratified AD populations. 43
Importantly, APOE ε4 carriers with agitation exhibited the most rapid cognitive decline and a significantly increased risk of progression from MCI to dementia compared with both non-carriers and carriers without agitation. These findings suggest that agitation may serve as a potential early clinical indicator of accelerated disease progression, especially in genetically vulnerable individuals. Consistent with prior longitudinal studies,44,45 our results highlight the value of integrating genetic and behavioral markers for early risk stratification and for guiding personalized monitoring and intervention strategies in AD.
Our study has several limitations. First, neuropsychiatric symptoms were assessed only using the NPI, without agitation-specific instruments, potentially limiting symptom characterization precision. Second, the cross-sectional design precludes causal inference between agitation and CSF biomarkers, and the observed associations require further confirmation through experimental or longitudinal studies. Third, potential residual confounding, including unmeasured clinical variables, may have influenced the observed associations. Finally, the ADNI cohort is relatively homogeneous and lacks diversity, which may limit the generalizability of our findings. Despite these limitations, our results provide valuable insights and warrant confirmation through future longitudinal studies in our cohort to further validate the association between agitation and AD-related biomarkers.
Conclusions
In conclusion, our study reveals two key findings in cognitively impaired patients. First, the association between agitation and tau pathology, as well as CSF GAP-43, is observed predominantly in APOE ε4 carriers. Second, the combination of APOE ε4 and agitation is associated with an increased risk of cognitive progression. Together, these findings suggest that, in APOE ε4 carriers, agitation may serve as a behavioral marker of active AD pathology, reflecting an elevated risk of cognitive decline. Incorporating agitation screening into the clinical assessment of APOE ε4-positive cognitively impaired individuals may provide a valuable early indicator of impending cognitive deterioration, facilitating targeted monitoring and intervention.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261464188 - Supplemental material for APOE ε4-specific associations between agitation, cerebrospinal fluid biomarkers, and cognitive decline in cognitively impaired patients
Supplemental material, sj-docx-1-alz-10.1177_13872877261464188 for APOE ε4-specific associations between agitation, cerebrospinal fluid biomarkers, and cognitive decline in cognitively impaired patients by Xiaochen Du, Yuye Wang, Jingwei Zhao, Yuchen Liu, Dantao Peng and in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
Data collection and sharing for the Alzheimer's Disease Neuroimaging Initiative (ADNI) is funded by the National Institute on Aging (National Institutes of Health Grant U19AG024904). The grantee organization is the Northern California Institute for Research and Education. In the past, ADNI has also received funding from the National Institute of Biomedical Imaging and Bioengineering, the Canadian Institutes of Health Research, and private sector contributions through the Foundation for the National Institutes of Health (FNIH) including generous contributions from the following: AbbVie, Alzheimer's Association; Alzheimer's Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; EliLilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research &Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; PfizerInc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer's Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer's Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
Ethical considerations
ADNI was approved by the regional ethical committees of all participating institutions and all study procedures were conducted in accordance with the principles of the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from all participants or their authorized representatives at the time of enrollment.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Oiandongnan zhou kehe pingtai (2024) NO.0002-1 and the Science and Technology Fund Project of the Guizhou Provincial Health Commission (grant number gzwkj2024-109)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data used in preparation of this article were obtained from the Alzheimer's Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.