
Abstract
Background
Anti–amyloid-β monoclonal antibodies represent a new class of disease-modifying therapies for Alzheimer's disease (AD). Their clinical adoption is complicated by amyloid-related imaging abnormalities (ARIA), encompassing vasogenic edema (ARIA-E) and hemorrhagic changes (ARIA-H). The comparative ARIA risk across agents and the influence of genetic factors remain incompletely characterized.
Objective
To quantify the pooled incidence of ARIA-E and ARIA-H associated with anti–amyloid-β immunotherapies and to compare relative risks across agents using network meta-analytic modeling.
Methods
Following PRISMA guidelines (PROSPERO: CRD420250653157), we searched PubMed, EMBASE, Scopus, Web of Science, and Ovid through January 2026 for Phase II/III randomized controlled trials of anti–amyloid-β immunotherapies in AD. Random-effects models estimated pooled prevalence and odds ratios (ORs). A penalized likelihood network meta-analysis addressed sparse events. APOE ε4–stratified analyses and Bayesian sensitivity models were also performed.
Results
Twenty-two trials (up to 23,120 participants) were included. Pooled ARIA-E prevalence was 6.8% and ARIA-H was 15.8%, with substantial heterogeneity. Anti–amyloid-β therapy significantly increased odds of ARIA-E (OR 7.93; 95% CI 4.50–13.98) and ARIA-H (OR 1.87; 95% CI 1.28–2.72) versus placebo. The highest ARIA-E risk was seen with donanemab and aducanumab, followed by gantenerumab and lecanemab. APOE ε4 carriage significantly elevated ARIA-E (OR 2.28) and ARIA-H (OR 2.07) risk, with a clear gene-dose effect in homozygotes.
Conclusions
ARIA risk varies substantially across anti–amyloid-β therapies and is strongly modulated by APOE ε4 status. These findings support genotype-informed risk stratification and individualized MRI monitoring to optimize the benefit–risk balance of disease-modifying therapies in AD.
Keywords
Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disorder characterized by extracellular amyloid-β (Aβ) deposition, tau pathology, and gradual cognitive decline.1,2 Over the past decade, immunotherapeutic strategies targeting Aβ aggregates have emerged as potential disease-modifying approaches. Several monoclonal antibodies have advanced through preclinical and clinical development, with three agents aducanumab, lecanemab, and donanemab receiving regulatory approval in the United States. 3
While these therapies have renewed hope for meaningful disease modification in individuals affected by this relentlessly progressive illness, they have also raised substantial concerns regarding real-world effectiveness, high treatment costs, and treatment-related risks. Among these, the most common and clinically significant adverse events are amyloid-related imaging abnormalities (ARIA). 4
During early clinical development of anti-amyloid immunotherapies, characteristic magnetic resonance imaging (MRI) abnormalities most notably vasogenic edema and cerebral microhemorrhages were observed in a subset of treated patients. These findings have been documented throughout the three-decade history of human anti-Aβ immunotherapy, contributing to early termination of initial active immunization trials and persisting as a major safety concern as the field transitioned toward passive antibody-based therapies. In response to growing regulatory and clinical concern, a workshop convened by the Alzheimer's Association Research Roundtable in 2010 formally introduced the term amyloid-related imaging abnormalities to standardize the description and reporting of these MRI findings.5–7
ARIA is broadly categorized into two subtypes. ARIA-E (edema/effusion) refers to vasogenic edema and sulcal effusions resulting from increased vascular permeability, typically visualized as hyperintense parenchymal or sulcal abnormalities on T2-weighted and fluid-attenuated inversion recovery (FLAIR) MRI sequences. ARIA-H (hemosiderin deposition) encompasses cerebral microhemorrhages and superficial siderosis, which appear as hypointense lesions on susceptibility-weighted imaging due to iron accumulation following blood product breakdown. 8
Reported ARIA incidence varies considerably across therapeutic agents, dosing regimens, and patient population. 7 Risk is strongly influenced by genetic factors, particularly carriage of the APOE ε4 allele, as well as baseline amyloid burden and underlying cerebrovascular pathology. 9 Although many ARIA cases are asymptomatic and detected only on surveillance MRI, some patients develop headache, confusion, dizziness, focal neurological symptoms, or seizures, occasionally necessitating dose modification, treatment interruption, or discontinuation. Symptomatic cases may require corticosteroid therapy or hospitalization, increasing clinical complexity and healthcare burden.5,6
Variability in ARIA definitions, imaging schedules, reporting standards, and study populations across trials has limited the ability to draw consistent conclusions regarding the magnitude of risk. A rigorous comparative synthesis of the available evidence is therefore essential to clarify safety profiles, guide MRI monitoring protocols, and support balanced risk–benefit discussions in AD.
Accordingly, this study was designed as a systematic review and meta-analysis with an integrated network meta-analytic approach to quantify the incidence of ARIA-E and ARIA-H and to compare the relative odds of these events across different anti-amyloid therapeutic strategies. By combining pooled prevalence estimates with comparative risk modeling derived from both direct and indirect evidence, we aim to provide a more precise and clinically actionable assessment of ARIA risk to inform safer implementation of disease-modifying therapies in AD.
Methods
This systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and followed a pre-registered protocol (CRD420250653157) in the PROSPERO database. 10
Literature searching
A systematic literature search was conducted across PubMed (MEDLINE), EMBASE, Scopus, Web of Science, and Ovid from database inception to January 2026. To maximize sensitivity, precision, and overall search quality, Cochrane-validated filters were applied for each database. The complete search strategies are provided in Supplemental Table 1. The objective was to identify controlled studies evaluating anti-amyloid therapies in patients with AD that reported at least one of the following adverse events: amyloid-related imaging abnormalities edema (ARIA-E) and amyloid-related imaging abnormalities hemorrhage (ARIA-H).
Inclusion and exclusion criteria
Studies were eligible if they were Phase 2 or Phase 3 randomized controlled trials evaluating anti-Aβ immunotherapy in patients with AD and provided sufficient data to assess the incidence of ARIA-E or ARIA-H. Studies were excluded if they were open-label trials, book chapters, short surveys, notes, comments, editorials, letters, review articles, or conference abstracts. Non-clinical studies, studies with overlapping patient populations, and publications representing summaries of previously reported research were also excluded. Studies that did not report ARIA-E and ARIA-H separately or provided data unsuitable for quantitative synthesis were excluded.
All retrieved records were exported and managed using Rayyan.ai. 11 Two independent reviewers screened titles and abstracts, and full-text articles were subsequently assessed for eligibility. Disagreements were resolved through discussion or consultation with a third reviewer until consensus was reached.
Data extraction
Data were extracted independently by two reviewers using a standardized data extraction form. The following information was collected from each included study: study name, country, diagnostic criteria for AD, mean age of participants, total number of participants, sex distribution, intervention details, treatment frequency, duration of therapy, and main clinical findings. We additionally extracted the incidence of ARIA-E and ARIA-H in each study arm, the prevalence of ARIA-E and ARIA-H according to APOE ε4 carrier and non-carrier status where available, and any other reported adverse events. Beyond ARIA outcomes, volumetric data were obtained from ClinicalTrials.gov and peer-reviewed publications to assess treatment-associated structural brain changes. When available, mean and 95% CIs were obtained for volumetric changes from baseline; however, several sources reported data as mean (SE) or mean (SD). Percentage changes were used to calculate mean volume changes using baseline volumes of whole brain, hippocampus, and lateral ventricle when these were reported in the publication or on ClinicalTrials.gov. Any discrepancies in extracted data were resolved through discussion and verification against the original publication.
Statistical analysis
All statistical analyses were performed using R version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria). For incidence (prevalence) analyses, we used the meta package. A random-effects model was applied using the inverse-variance method. Between-study variance (τ2) was estimated using the DerSimonian–Laird estimator, with confidence intervals (CIs) for τ2 and τ calculated using the Jackson method. Statistical heterogeneity was quantified using I2 derived from Cochran's Q statistic. A logit transformation was applied to stabilize variances, and Clopper–Pearson CIs were used for individual study estimates.
For pairwise meta-analysis of odds ratios (ORs), we also used the inverse-variance method under a random-effects model. Between-study variance (τ2) was estimated using the Paule–Mandel estimator, with CIs for τ2 and τ derived using the Q-profile method. Heterogeneity was assessed using I2 based on Cochran's Q statistic.
For the network meta-analysis, we employed a penalized likelihood network meta-analysis (PL-NMA) framework to address sparse binary data and rare events. Given the rarity of ARIA in certain trials, we implemented a logistic regression–based common-effect model using Firth's bias-reducing penalized likelihood approach via the brglm package in R. 12
Conventional inverse-variance network meta-analysis models rely on large-sample approximations and may yield biased or unstable estimates when event counts are low or zero. To overcome these limitations, we fitted the following model:


Modelling heterogeneity
To account for between-study heterogeneity within the penalized framework, we implemented a two-stage multiplicative overdispersion adjustment, as additive heterogeneity models are not directly compatible with penalized likelihood estimation. After fitting the PL-NMA model, arm-specific variances were adjusted as:

This approach avoids arbitrary continuity corrections, accommodates studies with zero events in both arms, and provides more robust variance estimates in sparse data settings.
Assessment of publication bias
Potential publication bias was assessed through visual inspection of funnel plots and formally tested using Egger's regression asymmetry test. A p-value <0.05 was considered indicative of significant small-study effects.
Bayesian sensitivity analysis
To assess robustness of findings, a Bayesian network meta-analysis was conducted as a sensitivity analysis. A random-effects normal likelihood model with identity link and vague priors for treatment effects was applied. Bayesian models were implemented using four Markov Chain Monte Carlo chains with 50,000 burn-in iterations followed by 100,000 sampling iterations. Convergence was evaluated using the Brooks–Gelman–Rubin diagnostic. Surface under the cumulative ranking curve (SUCRA) plots were generated to complement treatment ranking assessment.
Risk of bias assessment
The risk of bias in included studies was assessed using the Cochrane Risk of Bias 2.0 (RoB 2.0) tool. 13 Each study was rated as having low, some concerns, or a high risk of bias. Two independent reviewers performed the assessments, and any discrepancies were resolved through consensus.
Assessment of certainty of evidence
Certainty of evidence was assessed using CINeMA, which evaluates six domains: within-study bias, reporting bias, indirectness, imprecision, heterogeneity, and incoherence. Domains were rated as no concerns, some concerns, or major concerns (low/high risk for reporting bias).14,15
Imprecision and heterogeneity were assessed manually based on PL-NM) estimates and pairwise forest plots, as PL-NMA does not provide prediction intervals and is more appropriate for rare events. Default CINeMA rules were applied for other domains, with manual overrides documented when clinically justified.
Downgrading was conservative: two or more “some concerns” led to one-level downgrading, while “major concerns” led to one-level downgrading (two levels for imprecision). Overlapping domains were not double-downgraded. Intervention rankings were based on the confidence level applying to the majority of comparisons.
Results
Selection of studies
A total of 3018 records were identified through database searches, including PubMed (n = 226), Embase (n = 1106), Scopus (n = 356), Ovid (n = 1108), and Web of Science (n = 222). After removal of 1020 duplicate records, 1998 studies underwent title and abstract screening, of which 1946 were excluded.
Subsequently, 52 full-text reports were sought and successfully retrieved for eligibility assessment. Following full-text evaluation, 30 studies were excluded due to being protocols (n = 4), review articles (n = 7), or having an ineligible study design (n = 19). Ultimately, 22 studies met the inclusion criteria and were included in the qualitative synthesis. The study selection process is illustrated in Figure 1 and Table 1.
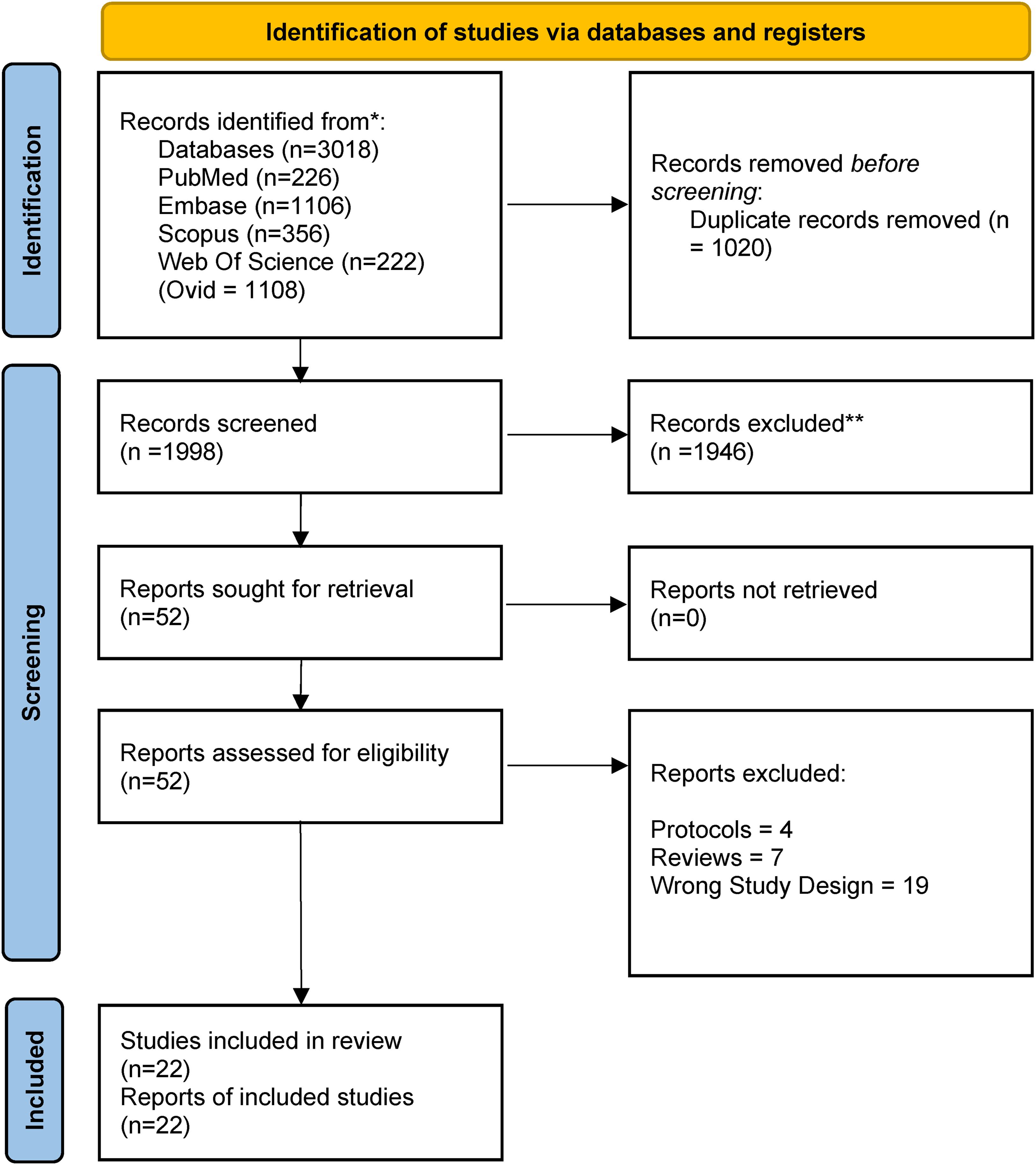
PRISMA flow diagram.
Characteristics of included studies.
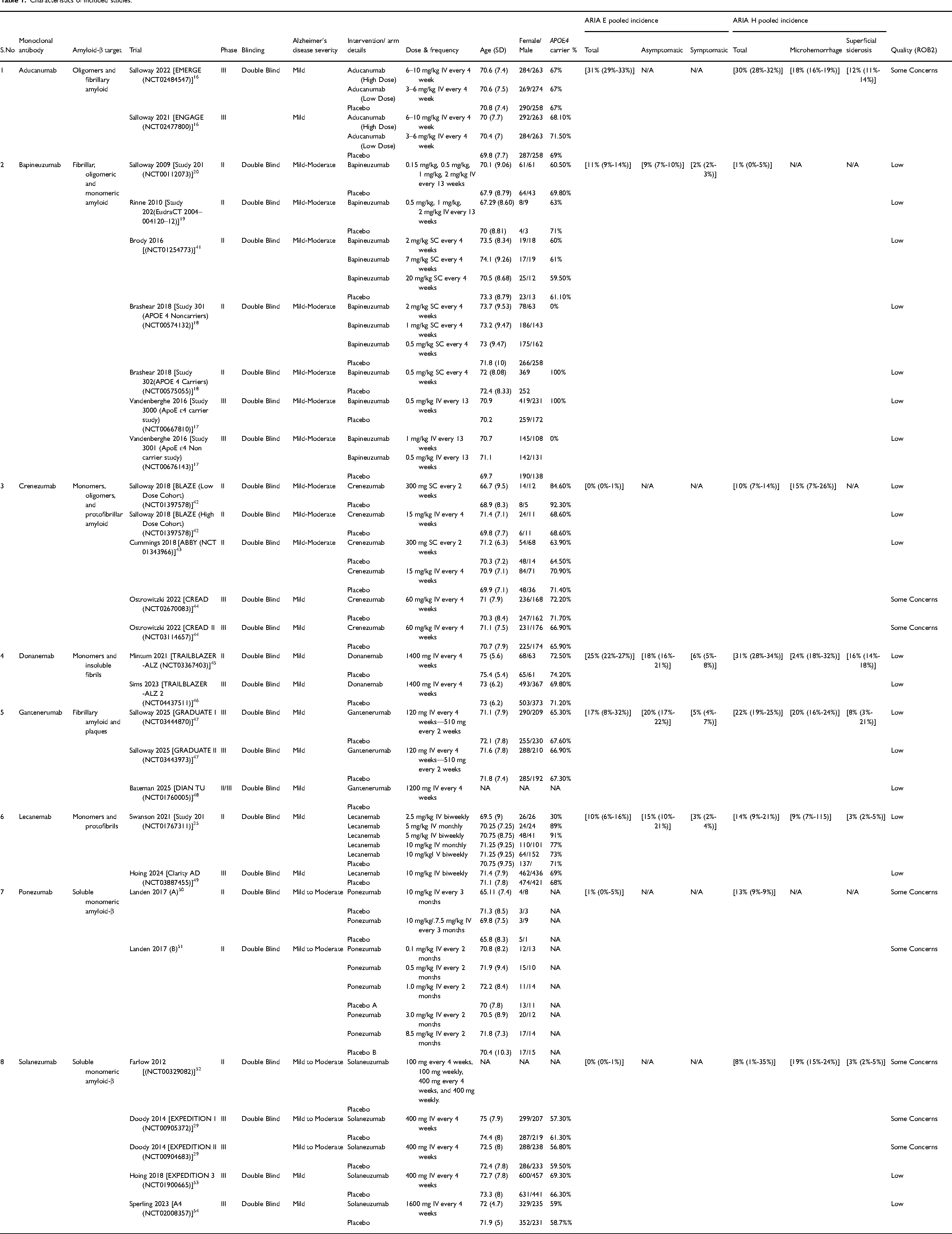
Characteristics of included studies
The included studies were published between 2009 and 2025 and were conducted across multiple geographic regions, all designed as randomized, double-blind, placebo-controlled trials. Most trials enrolled patients with early or mild-to-moderate AD, reflecting a progressive shift toward intervention at earlier disease stages.
Of the included trials, 12 were Phase II and 10 were Phase III studies. APOE ε4 carrier status was reported in 8 trials, underscoring its relevance as a risk modifier for both efficacy and safety outcomes. Additionally, 5 trials provided detailed classification of ARIA-E into asymptomatic and symptomatic events, and 8 trials reported ARIA-H subtypes, including microhemorrhages and superficial siderosis, enabling standardized safety comparisons across interventions.
Systematic review of interventions
The included monoclonal antibodies differ in their Aβ targets, trial designs, and stages of disease studied, resulting in heterogeneous efficacy and safety profiles. The following sections summarize the clinical trial evidence for each agent individually.
Aducanumab
Aducanumab was evaluated in two Phase III trials, EMERGE and ENGAGE, comparing low- and high-dose regimens with placebo in early AD. Both trials were halted prematurely in 2019 following a futility analysis. Subsequent post-hoc analyses suggested that the high-dose arm in EMERGE met its primary endpoint (Clinical Dementia Rating–Sum of Boxes), whereas ENGAGE failed to demonstrate consistent benefit. These discordant outcomes raised substantial concerns regarding reproducibility and clinical interpretability, highlighting the challenges of dose escalation and trial heterogeneity. 16
Bapineuzumab
Bapineuzumab is a humanized monoclonal antibody targeting the N-terminus of Aβ. It was evaluated in five Phase II double-blind trials (including Studies 201, 202, 301, 302, and NCT01254773) and two Phase III trials (Studies 3000 and 3001).17–20 The Phase III trials enrolled patients with mild-to-moderate AD and stratified participants by APOE ε4 carrier status. Despite long-term follow-up, bapineuzumab failed to demonstrate significant improvement in primary cognitive endpoints, including Alzheimer's Disease Assessment Scale–Cognitive Subscale 11 and Disability Assessment for Dementia, compared with placebo.
Crenezumab
Crenezumab targets multiple forms of Aβ, including monomers, oligomers, and fibrils. Two Phase III trials (CREAD 1 and CREAD 2) conducted in early AD were terminated early after failing to meet their primary clinical efficacy endpoints. 21
Donanemab
Donanemab selectively targets a modified form of Aβ present in established plaques. The Phase II TRAILBLAZER-ALZ trial demonstrated a statistically significant slowing of cognitive decline on the Integrated Alzheimer's Disease Rating Scale compared with placebo, alongside substantial amyloid plaque reduction. 22 However, the clinical relevance of the modest absolute treatment effect remained debated. The Phase III TRAILBLAZER-ALZ 2 trial further showed significant slowing of cognitive and functional decline in early symptomatic AD, particularly among participants with low-to-medium tau burden. 23
Gantenerumab
Gantenerumab is an IgG1 monoclonal antibody targeting Aβ oligomers and fibrils, facilitating microglial-mediated plaque clearance. Despite evaluation in Phase II and Phase III trials, including Scarlet RoAD, GRADUATE I, GRADUATE II, and DIAN-TU, gantenerumab failed to demonstrate clinically meaningful cognitive benefit in early or prodromal AD, leading to discontinuation of its development in 2022.21,24
Lecanemab
Lecanemab preferentially binds soluble amyloid protofibrils. The Phase IIb Study 201 identified 10 mg/kg biweekly as the optimal dose using a Bayesian adaptive design. Although prespecified probability thresholds for success were not fully met, signals of clinical benefit were observed. 25 The Phase III CLARITY-AD trial (18 months; n = 1795) demonstrated a statistically significant reduction in decline on the Clinical Dementia Rating–Sum of Boxes, with a 0.45-point difference versus placebo, corresponding to approximately 27% slowing of disease progression, providing more consistent evidence of efficacy than earlier antibodies. 26
Ponezumab
Ponezumab, targeting the C-terminal region of Aβ1−40, was developed primarily for cerebral amyloid angiopathy. Phase II trials confirmed safety and tolerability but failed to demonstrate reductions in vascular amyloid burden, limiting further clinical development.27,28
Solanezumab
Solanezumab binds the mid-domain of soluble Aβ and also recognizes truncated species present in plaques. Early Phase II trials demonstrated target engagement with dose-dependent changes in cerebrospinal fluid Aβ levels. However, large Phase III trials (EXPEDITION 1, 2, and 3) in mild-to-moderate AD failed to meet primary cognitive and functional endpoints. A prespecified subgroup analysis suggested modest slowing in mild AD, prompting further investigation. The A4 Study evaluated solanezumab in cognitively normal individuals with amyloid positivity (preclinical AD). However, it did not demonstrate significant slowing of cognitive decline.29,30
Prevalence of ARIA
ARIA-E
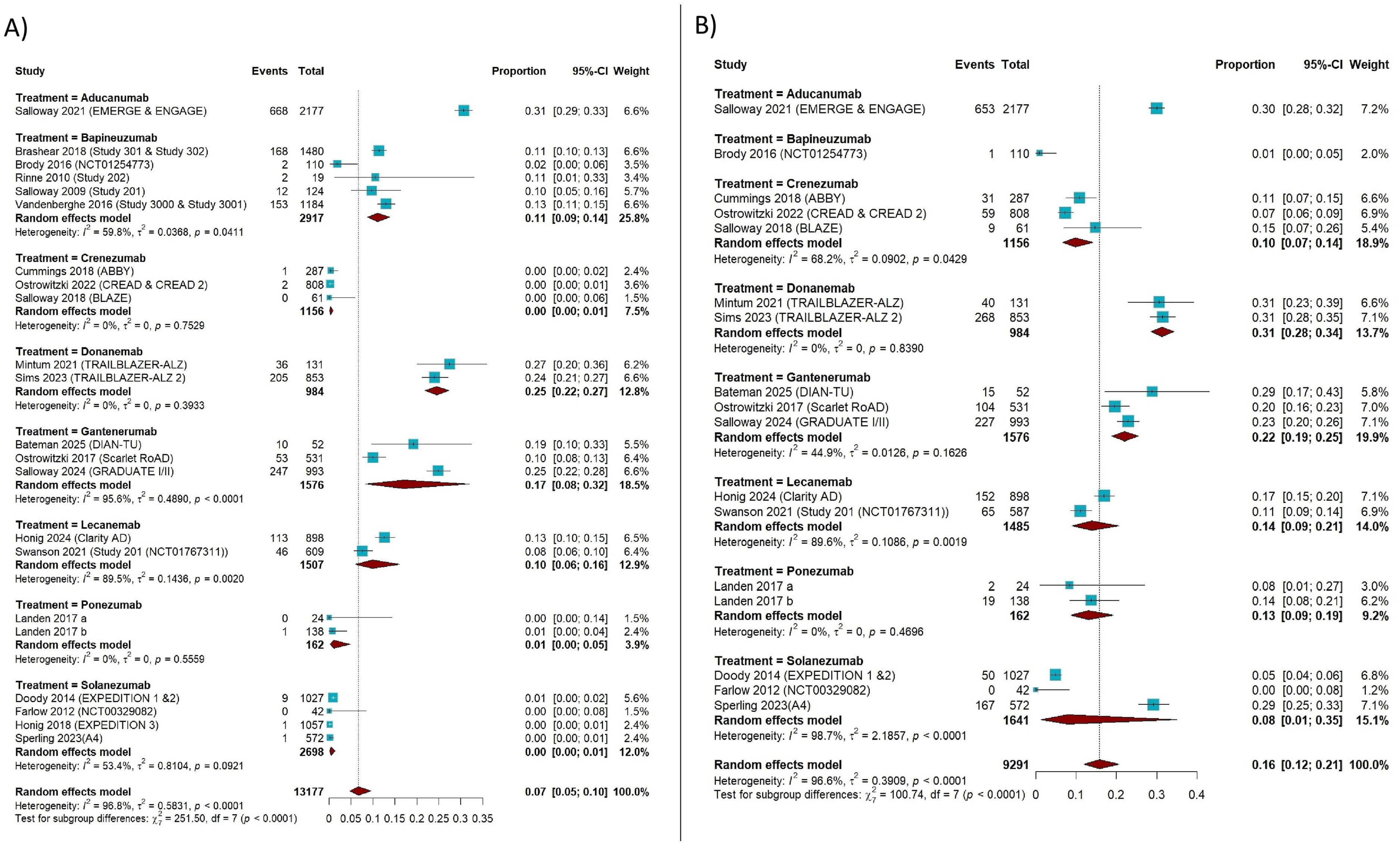
Across 22 studies including 13,177 participants and 1715 ARIA-E events, the pooled prevalence of ARIA-E under a random-effects model was 6.78% (95% CI, 4.73%–9.62%), with substantial heterogeneity (I2 = 96.7%; p < 0.001). Prevalence differed significantly across therapeutic agents (Q_between = 243.65; p < 0.001). The highest ARIA-E prevalence was observed with aducanumab (31.0%) and donanemab (24.5%), followed by gantenerumab (17.0%). Intermediate rates were noted for bapineuzumab (11.1%) and lecanemab (9.9%), whereas crenezumab, ponezumab, and solanezumab demonstrated consistently low prevalence (<1.5%) (Figure 2A).
(A) Prevalence of ARIA-E (Forest Plot). (B) Prevalence of ARIA-H (Forest Plot).
When stratified by clinical presentation, asymptomatic ARIA-E comprised the majority of cases, with a pooled prevalence of 14.72% and significant between-agent variability (Q_between = 87.51; p < 0.001). The highest asymptomatic rates were observed with gantenerumab (19.8%) and donanemab (18.4%), followed by lecanemab (9.8%) and bapineuzumab (8.9%). In contrast, symptomatic ARIA-E was uncommon. Across five studies (4355 participants; 172 events), the pooled prevalence was 4.14% (95% CI, 2.80%–6.07%), with the highest rates reported for donanemab (6.1%) and gantenerumab (5.0%), and lower rates for lecanemab (2.8%) and bapineuzumab (2.5%) (Q_between = 25.18; p < 0.001) (Supplemental Figures 1 and 2).
ARIA-H
Seventeen studies comprising 9291 participants and 1862 ARIA-H events were included. The pooled prevalence of ARIA-H was 15.8% (95% CI, 11.9%–20.7%), with substantial heterogeneity (I2 = 96.6%). Prevalence varied significantly across agents (p < 0.001), with the highest rates observed for donanemab (31.3%) and aducanumab (30.0%), followed by gantenerumab (22.0%). Intermediate prevalence estimates were reported for lecanemab (13.9%), ponezumab (13.1%), crenezumab (9.8%), and solanezumab (8.0%), while bapineuzumab demonstrated the lowest rate (0.9%) (Figure 2B).
Subtype analyses indicated that cerebral microhemorrhages were more frequent than superficial siderosis. The pooled prevalence of microhemorrhages was 19.1% (95% CI, 14.7%–24.4%; I2 = 94.2%), with significant between-agent differences, highest for solanezumab (27.6%) and donanemab (24.1%), and lowest for lecanemab (8.7%). Superficial siderosis was less common, with a pooled prevalence of 10.1% (95% CI, 7.6%–13.4%; I2 = 90.7%), occurring most frequently with donanemab (16.0%) and aducanumab (12.2%), and least frequently with solanezumab (3.3%) (Supplemental Figures 3 and 4).
Other adverse events
Across anti–Aβ monoclonal antibodies, adverse events were common, with a pooled prevalence of 16.9% (95% CI, 14.6%–19.6%) and substantial heterogeneity. Treatment-related adverse events occurred in 71.8% of participants, whereas discontinuation due to adverse events was relatively infrequent (7.5%). Serious adverse events occurred at comparable rates across agents, and overall mortality was low (1.1%).
The most frequently reported adverse events included headache (10.7%), falls (10.7%), nausea (9.7%), anxiety (8.5%), back pain (8.1%), depression (7.1%), vomiting (7.2%), dizziness (6.6%), diarrhea (6.0%), and fatigue (5.2%). Infusion-related reactions occurred in 13.4% of participants, with notable variability across agents. Detailed findings are provided in Supplemental Figure 5.
Volumetric brain changes
Hippocampal atrophy. Across 20 studies, anti–Aβ therapies showed a non-significant trend toward hippocampal atrophy (MD −5.11%, 95% CI −12.38% to 2.15%; p = 0.168) with moderate heterogeneity (I2 = 49.9%). Lecanemab demonstrated the largest reduction in hippocampal volume (MD −24.00%), followed by bapineuzumab (MD −6.38%). Crenezumab, aducanumab, and solanezumab showed no significant effects on hippocampal volume. No significant differences were observed between drugs (p = 0.569). Detailed findings are provided in Supplemental Figure 6. Whole brain atrophy. Across 22 studies, anti–Aβ treatment was associated with significant whole-brain volume loss (MD −1.12%, 95% CI −1.92% to −0.31%; p = 0.007), with moderate heterogeneity (I2 = 57.3%). Significant differences were observed between agents (p < 0.0001). The largest reductions occurred with lecanemab (MD −4.78%) and donanemab (MD −4.60%), whereas bapineuzumab and aducanumab showed smaller, non-significant decreases. Crenezumab and solanezumab produced negligible changes. Detailed findings are provided in Supplemental Figure 7. Lateral ventricular enlargement. Across 20 studies, anti–Aβ therapies were associated with significant lateral ventricular enlargement (MD +1.30%, 95% CI 0.80% to 1.80%; p < 0.0001), with substantial heterogeneity (I2 = 88.2%). Between-drug differences were significant (p < 0.0001). The greatest increases were observed with aducanumab (MD +2.56%) and donanemab (MD +2.30%), followed by lecanemab (MD +1.47%) and bapineuzumab (MD +0.96%). Crenezumab and solanezumab showed no significant effects. Overall, anti–Aβ therapies, particularly lecanemab, donanemab, and aducanumab, were associated with measurable structural brain changes, including whole-brain atrophy and ventricular enlargement, warranting further evaluation and clinical monitoring. Detailed findings are provided in Supplemental Figure 8.
Pairwise meta-analysis of ARIA risk
Odds ratios for ARIA-E
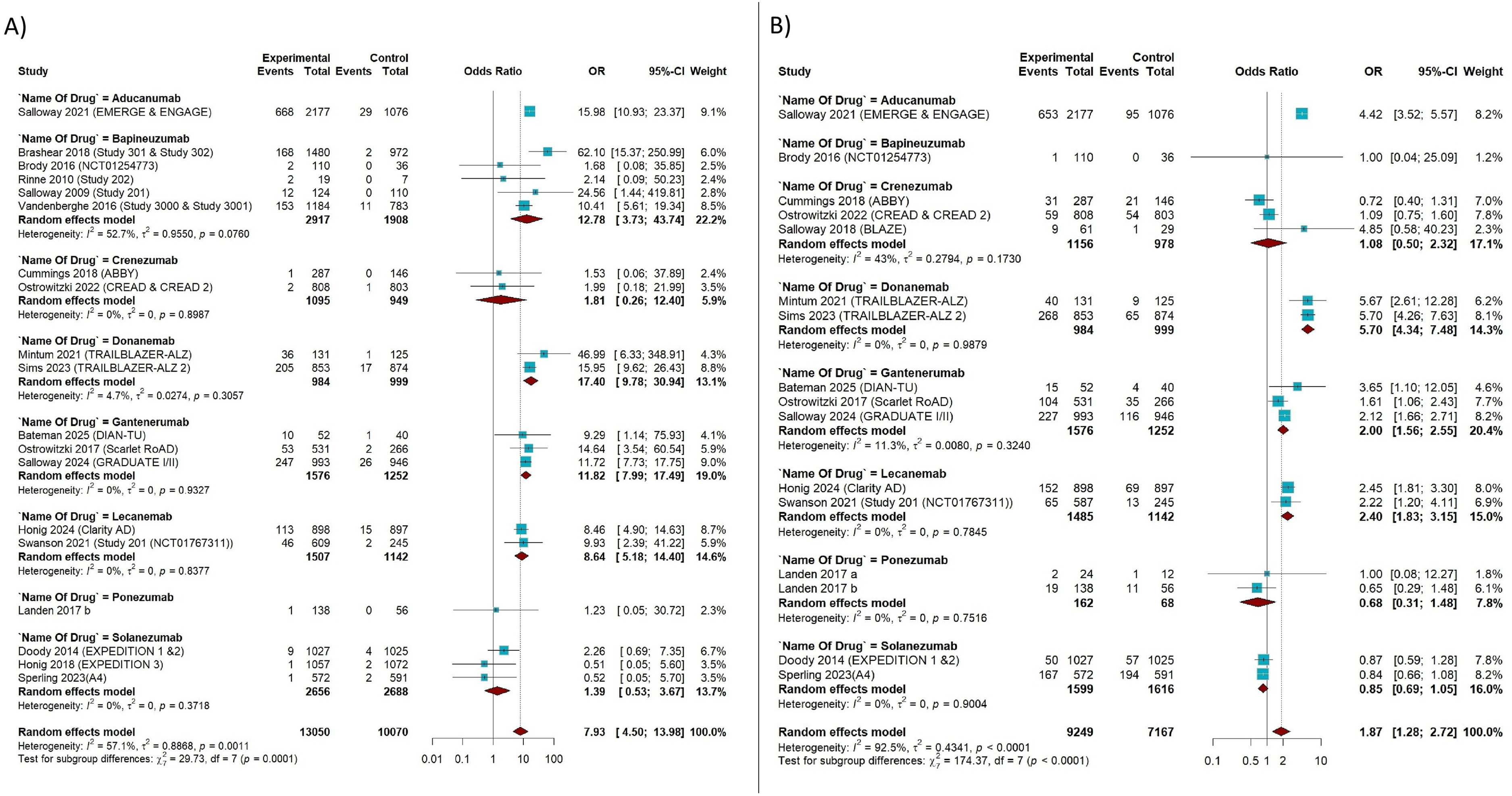
Nineteen studies comprising 23,120 participants (13,050 treated; 10,070 controls) and 1845 ARIA-E events were analyzed. Overall, anti–Aβ immunotherapies were associated with a significantly increased risk of ARIA-E compared with control (pooled OR, 7.93; 95% CI, 4.50–13.98; p < 0.0001), with moderate heterogeneity (τ2 = 0.89; I2 = 57.1%; Q = 41.97; p = 0.001). Subgroup analyses demonstrated significant between-agent differences (Q_between = 29.73; p = 0.0001) (Figure 3A).
(A) Odds ratio pairwise meta analysis for ARIA-E. (B) Odds ratio pairwise meta analysis for ARIA-H.
The highest odds were observed with donanemab (OR, 17.40; 95% CI, 9.78–30.94) and aducanumab (OR, 15.98; 95% CI, 10.93–23.37), followed by bapineuzumab (OR, 12.78; 95% CI, 3.73–43.74) and lecanemab (OR, 8.64; 95% CI, 5.18–14.40). Associations were more modest or non-significant12 for gantenerumab, crenezumab, solanezumab, and ponezumab. Within-agent heterogeneity was generally low, with notable variability only for bapineuzumab.
Odds ratios for ARIA-H
Sixteen studies including 16,416 participants (9249 treated; 7167 controls) and 2607 ARIA-H events were included. Anti–Aβ immunotherapies were associated with a significant increase in the odds of ARIA-H compared with control (pooled OR, 1.87; 95% CI, 1.28–2.72; p = 0.0011), with substantial heterogeneity (τ2 = 0.43; I2 = 92.5%; Q = 199.17; p < 0.0001). Significant between-agent differences were observed (Q_between = 174.37; p < 0.0001) (Figure 3B).
The highest odds were reported for aducanumab (OR, 4.42; 95% CI, 3.52–5.57) and donanemab (OR, 5.70; 95% CI, 4.34–7.48), followed by gantenerumab (OR, 2.00; 95% CI, 1.56–2.55) and lecanemab (OR, 2.40; 95% CI, 1.83–3.15). Associations were weaker or non-significant for crenezumab, solanezumab, ponezumab, and bapineuzumab. Within-agent heterogeneity was generally low, with moderate inconsistency observed for crenezumab.
ARIA risk stratified by APOE ε4 status
Across eight studies including 9109 participants (5862 APOE ε4 carriers; 3247 non-carriers) and 1702 ARIA-E events, APOE ε4 carriage was associated with a significantly increased risk of ARIA-E (pooled OR, 2.28; 95% CI, 2.01–2.60; p < 0.0001), with no between-study heterogeneity (I2 = 0%; Q = 6.67; p = 0.46) and no evidence of subgroup differences across agents (Q_between = 0.77; p = 0.94) (Figure 4A).
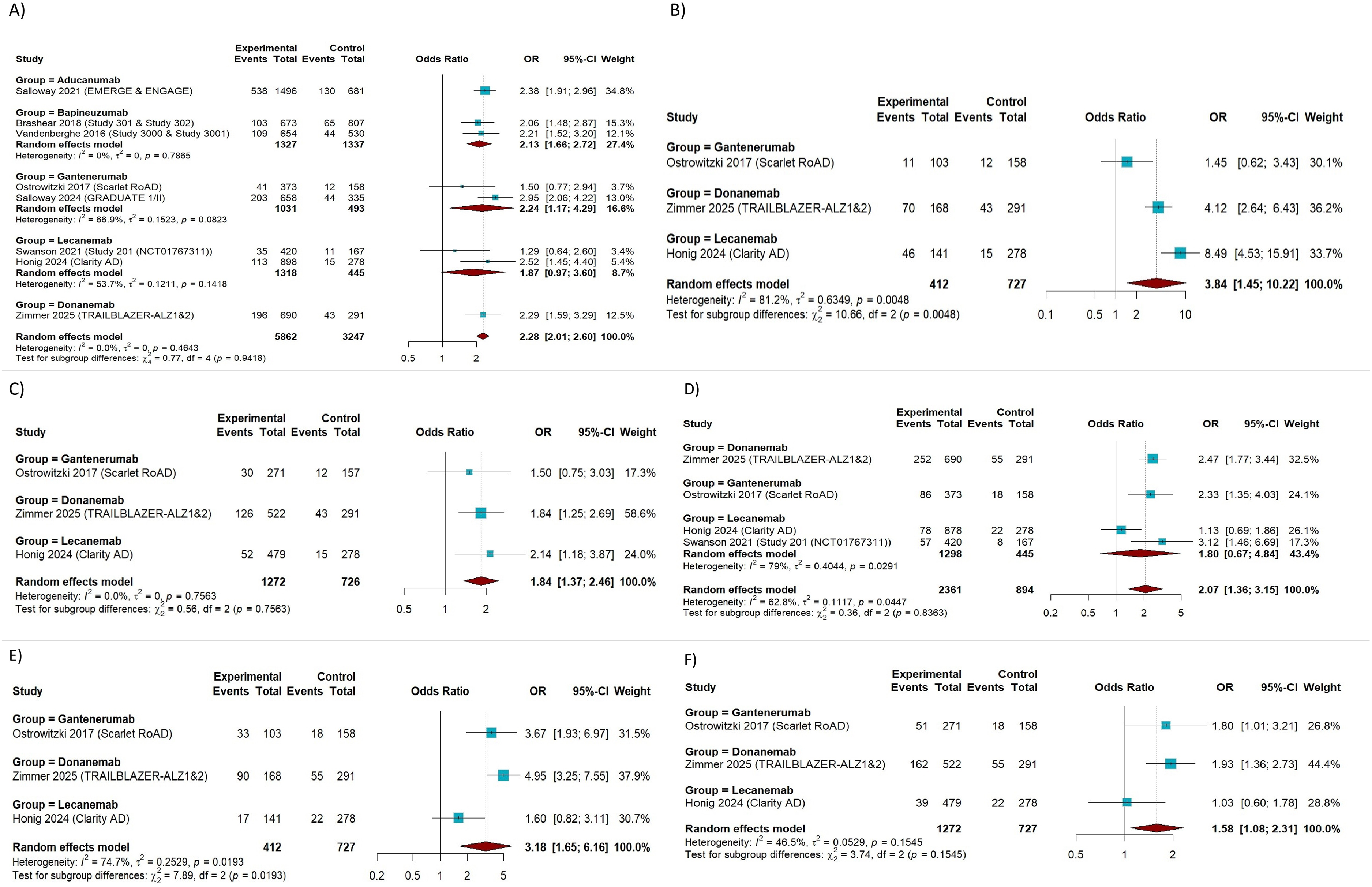
(A) Odds ratio pairwise meta analysis for ARIA-E (APOE ε4 versus non-carriers). (B) Odds ratio pairwise meta analysis for ARIA-H (APOE ε4 versus non-carriers). (C) Odds ratio pairwise meta analysis for ARIA-E (APOE ε4 homozygotes versus non-carriers). (D) Odds ratio pairwise meta analysis for ARIA-E (APOE ε4 heterozygotes versus non-carriers). (E) Odds ratio pairwise meta analysis for ARIA-H (APOE ε4 homozygotes versus non-carriers). (F) Odds ratio pairwise meta analysis for ARIA-H (APOE ε4 heterozygotes versus non-carriers).
Genotype-stratified analyses demonstrated a gene-dose effect. APOE ε4 homozygotes exhibited a markedly increased risk of ARIA-E compared with non-carriers (OR, 3.84; 95% CI, 1.45–10.22; p = 0.0069), although substantial heterogeneity was present (I2 = 81.2%). APOE ε4 heterozygotes showed a more modest but significant increase in risk (OR, 1.84; 95% CI, 1.37–2.46; p < 0.0001) without detectable heterogeneity (I2 = 0%) (Figure 4B, C).
For ARIA-H, four studies including 3255 participants (2361 APOE ε4 carriers; 894 non-carriers) and 576 events were analyzed. APOE ε4 carriage was associated with a significantly increased risk of ARIA-H (pooled OR, 2.07; 95% CI, 1.36–3.15; p = 0.0007), with moderate heterogeneity (I2 = 62.8%; Q = 8.06; p = 0.045) and no significant subgroup differences (Q_between = 0.36; p = 0.84) (Figure 4D).
A gene-dose relationship was also observed for ARIA-H. APOE ε4 homozygotes had a substantially higher risk compared with non-carriers (OR, 3.18; 95% CI, 1.65–6.16; p = 0.0006), with considerable heterogeneity (I2 = 74.7%), whereas heterozygotes demonstrated a modest but significant increase in risk (OR, 1.58; 95% CI, 1.08–2.31; p = 0.018), with low-to-moderate heterogeneity (I2 = 46.5%). Overall, these findings indicate that APOE ε4 status, particularly homozygosity, confers heightened susceptibility to both ARIA-E and ARIA-H among patients receiving anti–Aβ immunotherapies (Figure 4E, F).
Network meta-analysis for ARIA (penalized likelihood model and Bayesian sensitivity analysis)
A PL-NMA was conducted to estimate comparative ORs for ARIA outcomes versus placebo, explicitly accounting for sparse events and rare-study bias. Between-study variability was addressed using a multiplicative overdispersion parameter, improving robustness of inference in the presence of heterogeneous trial designs.
For ARIA-E, a clear risk gradient was observed. The highest odds versus placebo were seen with bapineuzumab (OR 18.70; 95% CI 10.83–32.28), donanemab (OR 17.20; 95% CI 10.62–27.86), and aducanumab (OR 15.73; 95% CI 10.78–22.93), followed by gantenerumab (OR 11.66; 95% CI 7.91–17.18) and lecanemab (OR 8.43; 95% CI 5.10–13.94). In contrast, crenezumab (OR 2.00; 95% CI 0.31–12.79), solanezumab (OR 1.36; 95% CI 0.57–3.25), and ponezumab (OR 1.23; 95% CI 0.05–31.48) demonstrated modest and statistically non-significant associations, with wide CIs reflecting limited event counts. Moderate heterogeneity was detected (ĉ = 1.71, Fletcher's estimator), supporting the use of variance inflation (Supplemental Figures 9 and 10).
For ARIA-H, a similar but attenuated pattern emerged, indicating overlapping yet quantitatively distinct safety profiles. Donanemab (OR 5.66; 95% CI 4.32–7.43) and aducanumab (OR 4.41; 95% CI 3.50–5.54) showed the strongest associations, while lecanemab (OR 2.39; 95% CI 1.82–3.13) and gantenerumab (OR 2.02; 95% CI 1.64–2.48) were associated with moderate risk increases. Crenezumab, solanezumab, and ponezumab were not significantly associated with ARIA-H, and bapineuzumab yielded a highly imprecise estimate due to sparse data. Heterogeneity was minimal in this network (ĉ = 1.00), with no evidence of excess dispersion (Supplemental Figures 11 and 12).
Bayesian SUCRA rankings were concordant with these findings, and model convergence diagnostics were satisfactory (Supplemental Figures 13 and 14), reinforcing the internal consistency of the comparative hierarchy.
Publication bias
Publication bias was assessed using Egger's linear regression test of funnel plot asymmetry. For ARIA-E, there was no evidence of small-study effects (t = −0.03, df = 17, p = 0.98), with a negligible bias estimate (−0.05, SE = 1.85) despite substantial residual heterogeneity (τ2 = 19.35). Similarly, for ARIA-H, Egger's test did not indicate funnel plot asymmetry (t = −0.03, df = 17, p = 0.98), with an identical bias estimate and heterogeneity parameter. Overall, these findings suggest no statistically significant evidence of publication bias for either ARIA-E or ARIA-H (Supplemental Figures 15 and 16).
Risk of bias
Risk of bias (within-study bias) was assessed using the Cochrane Collaboration Risk of Bias 2.0 (RoB 2.0) tool. Of the 22 included randomized controlled trials, 14 were judged to have a low risk of bias across domains, while 8 were rated as having some concerns, primarily related to deviations from intended interventions or missing outcome data. No study was classified as having a high risk of bias. A detailed summary of domain-level assessments is presented in Figure 5.
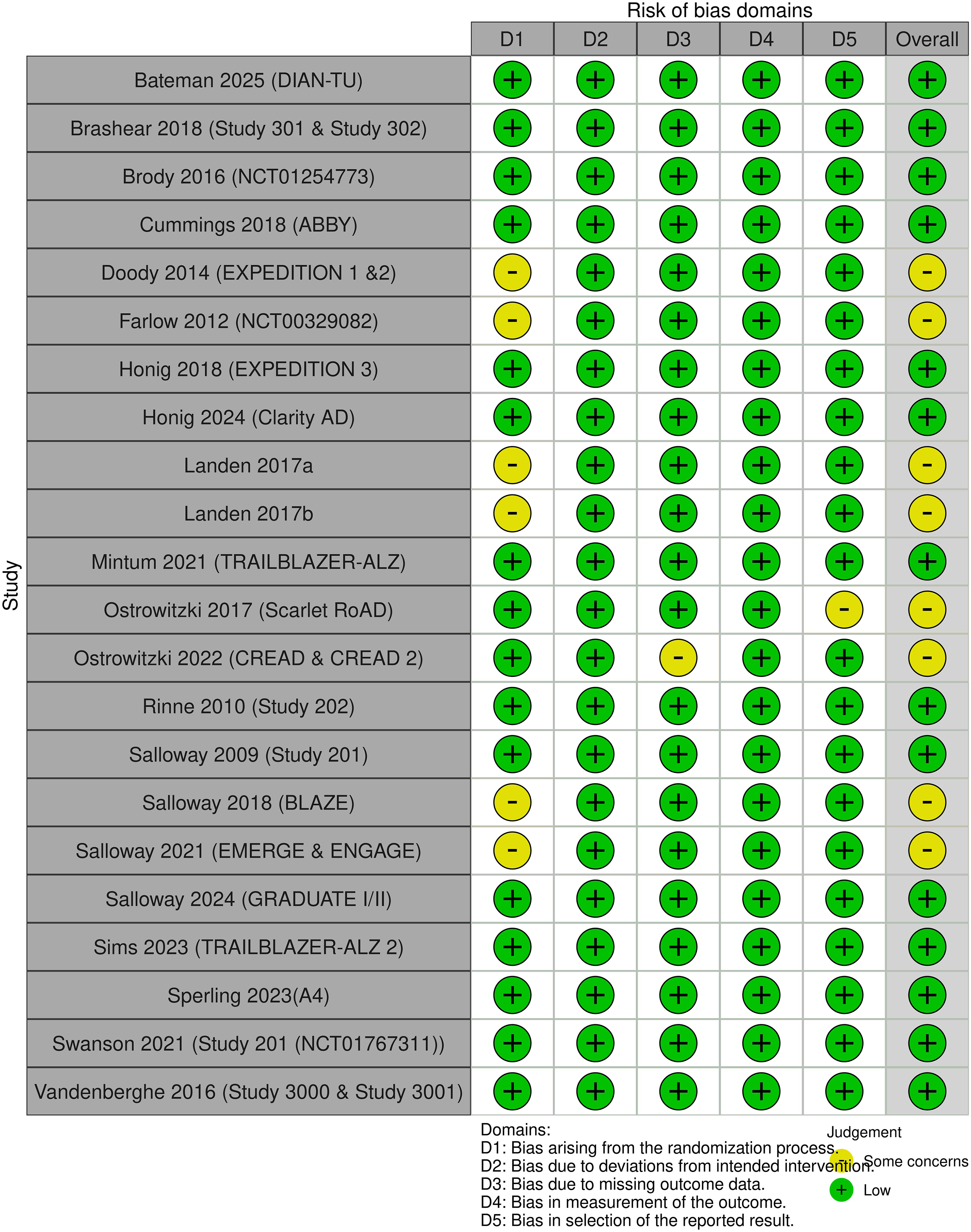
Risk Of Bias (2.0).
Certainty of evidence assessment of ARIA-E and ARIA-H
Markedly elevated ORs for ARIA-E were seen with bapineuzumab (OR 18.70), donanemab (OR 17.2), and aducanumab (OR 15.73), signaling substantially increased risk; evidence certainty was downgraded mainly due to imprecision in indirect comparisons underpinning most evaluations. Risk of bias (ROB) was low for donanemab and bapineuzumab but raised concerns for aducanumab and lecanemab from methodological issues; indirectness was limited except for gantenerumab (e.g., inherited AD populations), while heterogeneity stayed generally low despite spikes in some indirect comparisons (e.g., solanezumab), with no evident publication bias or incoherence. For ARIA-H, donanemab topped risks (OR 5.66), followed by aducanumab (OR 4.41), lecanemab (OR 2.39), and gantenerumab (OR 2.02); imprecision again yielded low certainty via wide CIs for most agents (e.g., ponezumab, bapineuzumab, solanezumab) and sparse direct comparisons even for donanemab while ROB, indirectness (mainly gantenerumab), and heterogeneity patterns mirrored ARIA-E, including some inconsistency in indirect comparisons (Supplemental Tables 2 and 3).
Discussion
Our systematic review and meta-analysis of 22 randomized controlled trials comprehensively examined the risk of ARIA associated with monoclonal anti–Aβ immunotherapies in AD. Drawing on pooled data from 23,120 participants for ARIA-E and 16,416 for ARIA-H, this represents, to our knowledge, one of the largest comparative safety syntheses of these agents to date. By integrating prevalence estimates, pairwise meta-analyses, genotype-stratified models, and network-based comparisons, our findings provide detailed and clinically meaningful insights into the evolving safety landscape of amyloid-targeting therapies.
Overall risk of ARIA-E
The pooled prevalence of ARIA-E approached 7% overall; however, this aggregate estimate obscures substantial between-agent heterogeneity. The highest prevalence was observed with aducanumab, followed by donanemab and gantenerumab, with progressively lower rates for bapineuzumab and lecanemab, and negligible estimates (≈1–0%) for solanezumab, ponezumab, and crenezumab. Importantly, most ARIA-E events were asymptomatic; nevertheless, symptomatic ARIA-E, although less frequent, was clinically meaningful and occurred in up to 6% of treated participants for certain agents. This distinction is critical, as asymptomatic ARIA-E is often radiographic and self-limited, whereas symptomatic ARIA-E may necessitate dose interruption, intensified MRI surveillance, or permanent treatment discontinuation.
Consistent with prior systematic reviews, among currently FDA-approved therapies, aducanumab and donanemab demonstrated higher ARIA-E prevalence compared with lecanemab. However, as these agents are supported by a limited number of pivotal phase III trials, pooled prevalence estimates for approved drugs should be interpreted with caution—particularly when extrapolating findings to broader real-world populations that may have greater comorbidity burden, concomitant anticoagulant use, or more advanced cerebral amyloid angiopathy. 31
OR analyses further clarified the relative risk gradient, particularly aducanumab and donanemab demonstrated the highest event rates and ORs versus placebo. In both pairwise and penalized network models, these agents exhibited approximately 15- to 17-fold higher odds of ARIA-E compared with control. bapineuzumab also showed a high point estimate, though with wider CIs in network analyses, reflecting smaller sample sizes and greater statistical imprecision. Intermediate risk was observed with gantenerumab and lecanemab, whereas crenezumab, solanezumab, and ponezumab were not associated with statistically significant increases in ARIA-E risk in comparative models.
Our findings are consistent with prior analyses, including those by Shim et al., which focused exclusively on FDA-approved agents and similarly demonstrated a higher risk of ARIA-E with Donanemab compared with lecanemab. 31 Collectively, these data support a biologically plausible risk gradient aligned with amyloid-binding characteristics and plaque-clearing kinetics, reinforcing that ARIA-E risk is not a uniform class effect but rather varies meaningfully by molecular target profile and therapeutic potency.
Overall risk of ARIA-H
Consistent with prior literature, ARIA-H occurred more frequently than ARIA-E, with a pooled prevalence exceeding 15% across anti–Aβ monoclonal antibody trials. Among approved therapies, aducanumab and donanemab demonstrated higher ARIA-H prevalence than lecanemab, whereas the low estimate for bapineuzumab (∼1%) should be interpreted cautiously given its derivation from a single study.
Subtype analyses showed that cerebral microhemorrhages (∼19%) were more common than superficial siderosis (∼10%), a distribution that aligns with the proposed mechanism of transient vascular fragility during amyloid clearance. Higher microhemorrhage rates observed with solanezumab and donanemab suggest that hemorrhagic changes may occur even without prominent ARIA-E, although these findings are based on limited data.
Despite the high prevalence, the relative risk compared with placebo was more modest (pooled OR ≈ 1.9). Consistent with prior work by Jeremic et al., our analysis demonstrated that donanemab and aducanumab exhibited the highest odds, followed by lecanemab, whereas crenezumab, solanezumab, ponezumab, and bapineuzumab showed weaker or non-significant associations, often constrained by sparse-event data. 32 Network meta-analysis reinforced this hierarchy, with smaller effect sizes for ARIA-H than ARIA-E, indicating overlapping but quantitatively distinct safety profiles. Observed heterogeneity likely reflects variability in MRI protocols, radiologic adjudication, dosing strategies, and baseline vascular vulnerability, underscoring the need for standardized imaging and harmonized safety reporting.
Clinically, although most ARIA-H events are asymptomatic and incidentally detected on MRI, their cumulative burden may increase long-term intracerebral hemorrhage risk, particularly in individuals with cerebral amyloid angiopathy or those receiving antithrombotic therapy. Importantly, ARIA-H can occasionally present with seizures or focal neurological deficits that mimic acute ischemic stroke. Case reports have documented instances in which ARIA was misdiagnosed as stroke, leading to thrombolytic administration and subsequent catastrophic intracerebral hemorrhage. 33 As anti–Aβ therapies become more widely implemented, emergency and stroke teams must recognize ARIA as a critical stroke mimic in this population to avoid inappropriate reperfusion therapy.
Translational implications of APOE ε4–associated ARIA risk
A consistent finding across the included studies mirroring prior literature was the strong association between APOE ε4 carriage and increased risk of ARIA. For ARIA-E, APOE ε4 carriers had more than double the odds compared with non-carriers (OR, 2.28; 95% CI, 2.01–2.60), with minimal between-study heterogeneity. A clear gene-dose effect was observed, with ε4 homozygotes demonstrating the highest risk (OR, 3.84), followed by heterozygotes (OR, 1.84). A similar pattern was evident for ARIA-H, with increased risk among ε4 carriers overall (OR, 2.07), particularly among homozygotes (OR, 3.18). However, genotype-stratified estimates especially for homozygotes were derived from a limited number of studies and should therefore be interpreted with caution. 34
The biological plausibility of this association is well supported. APOE ε4 is strongly linked to cerebral amyloid angiopathy and promotes vascular amyloid deposition, leading to increased vessel fragility.35–37 Because ARIA pathogenesis is closely related to vascular amyloid burden, ε4-mediated vascular vulnerability likely amplifies treatment-emergent injury, particularly during rapid amyloid clearance. Supporting this mechanism, machine-learning analyses presented at the 16th Clinical Trials on Alzheimer's Disease Conference (Boston, USA) using pooled data from phase 2 and phase 3 donanemab studies identified APOE ε4 homozygosity as the strongest baseline predictor of ARIA-E (OR, 4.6; 95% CI, 3.3–6.4) among multiple candidate risk factors. 38
Clinically, these findings have direct translational relevance. In the United States, the U.S. Food and Drug Administration includes boxed warnings for anti–Aβ monoclonal antibodies, highlighting the increased incidence of ARIA particularly symptomatic and serious events among APOE ε4 homozygotes compared with heterozygotes and non-carriers. 39 In contrast, the UK Medicines and Healthcare products Regulatory Agency and the European Medicines Agency's Committee for Medical Products for Human Use, have adopted a more cautious position, citing uncertainty regarding the benefit–risk balance of lecanemab in APOE ε4 homozygotes and restricting routine clinical use accordingly. 40
Overall, APOE ε4 emerges as a dominant host-level determinant of ARIA risk. These findings support genotype-informed patient selection, risk counseling, and MRI surveillance strategies when initiating amyloid-clearing therapies, particularly in individuals with genetically elevated vascular vulnerability.
Clinical implications
Although the ARIA risk hierarchy identified in this meta-analysis with donanemab and aducanumab carrying the highest burden is broadly consistent with data reflected in regulatory labeling and prior systematic reviews, the present synthesis meaningfully advances the clinical evidence base in several concrete ways. First, by quantifying relative risk across all approved and investigational anti-amyloid agents within a unified penalized likelihood network framework, this analysis enables direct, statistically principled agent-to-agent comparisons that individual trials or pairwise reviews cannot provide. The approximately twofold difference in ARIA-E odds between lecanemab and donanemab, for instance, is now expressed with greater precision and anchored to a common reference, offering clinicians and formulary committees a quantitative foundation for comparative benefit–risk assessment that goes beyond qualitative labeling statements.
Second, the APOE ε4-stratified analyses have direct implications for patient selection protocols. Current prescribing practice often involves a binary carrier/non-carrier screen, yet our gene-dose data demonstrating that APOE ε4 homozygotes face nearly fourfold elevated ARIA-E odds compared with non-carriers, versus approximately twofold for heterozygotes argue for a more granular genotyping and counseling framework. Clinicians could use these stratified estimates to structure individualized risk discussions: heterozygotes may reasonably proceed with standard MRI monitoring intervals, whereas homozygotes warrant pre-treatment counseling that explicitly quantifies their substantially higher risk and, in line with EMA and MHRA guidance, may appropriately inform a decision to defer or decline treatment. This genotype-guided tiering is not yet codified in most institutional prescribing protocols and represents a specific, actionable refinement that extends beyond current regulatory labeling language.
Third, the symptomatic ARIA-E prevalence estimates stratified by agent reaching 6.1% for donanemab and 2.8% for lecanemab are clinically relevant for designing post-marketing surveillance and MRI monitoring schedules. Trials have employed heterogeneous MRI intervals, and no consensus surveillance protocol currently exists across prescribing centers. The pooled symptomatic rates derived here provide an empirical basis for risk-stratified monitoring frameworks: agents with higher symptomatic ARIA-E rates may warrant more frequent early surveillance MRI (e.g., at weeks 4, 8, and 12 of induction), whereas agents with lower symptomatic rates could support less intensive but still structured protocols. Similarly, the documented risk of ARIA mimicking acute ischemic stroke with case reports of catastrophic outcomes following thrombolytic administration highlights the need for institutional pathways that prompt ARIA consideration before reperfusion therapy in any patient receiving anti-amyloid immunotherapy who presents with acute neurological change. These are specific, implementable protocol adjustments that the quantitative data from this meta-analysis can directly inform.
Volumetric brain changes as a complication of anti–Aβ therapy
Beyond ARIA, our volumetric analyses demonstrate that anti–Aβ immunotherapy is associated with measurable structural brain changes. Whole brain atrophy reached statistical significance across 22 studies (MD −1.12%; 95% CI, −1.92% to −0.31%; p = 0.007), and lateral ventricular enlargement was robustly detected across 20 studies (MD +1.30%; 95% CI, 0.80% to 1.80%; p < 0.0001), with both outcomes driven predominantly by lecanemab, donanemab, and aducanumab. These findings suggest that potent amyloid-clearing therapies may induce treatment-emergent volumetric changes, potentially reflecting a combination of rapid amyloid plaque clearance, inflammatory microglial activation, and resolution of vasogenic edema leading to apparent parenchymal contraction. Hippocampal atrophy, while not reaching pooled significance (MD −5.11%; p = 0.168), showed a numerically large reduction with lecanemab (MD −24.00%), warranting cautious interpretation given the hippocampus's central role in memory consolidation and its particular vulnerability in AD. Complementing structural MRI-based volumetric assessment, [18F]fluorodeoxyglucose positron emission tomography (FDG-PET) provides a well-validated measure of cerebral glucose metabolism and neuronal function in AD. Unlike volumetric MRI, which reflects structural tissue loss, FDG-PET can detect metabolic dysfunction that may precede visible atrophy, offering a functionally complementary perspective on treatment-related brain changes. Several anti–Aβ trials have reported reductions in cerebral glucose metabolism following therapy, suggesting that amyloid clearance may be accompanied by transient or sustained metabolic disruption in vulnerable cortical regions. Accelerated atrophy beyond the expected disease trajectory could theoretically contribute to, rather than ameliorate, cognitive decline—a critical concern given the modest benefit margins observed in pivotal trials. Although FDG-PET outcomes were not included in the present meta-analysis due to inconsistent reporting across trials, future studies should prospectively incorporate FDG-PET alongside ARIA and volumetric MRI measures, with longer follow-up, standardized imaging protocols, and independent imaging adjudication, to enable a more comprehensive assessment of the functional and structural consequences of anti–Aβ immunotherapy.
Strengths and limitations
This study has several important strengths. It represents one of the largest comparative safety syntheses of anti–Aβ monoclonal antibodies to date, incorporating 22 randomized controlled trials. Multiple complementary analytic approaches including pooled prevalence estimation, pairwise meta-analysis, genotype-stratified models, and PL-NMA were applied, enabling both absolute and comparative risk assessment across agents and strengthening the robustness of the findings.
Several limitations should be acknowledged. Substantial heterogeneity was observed in prevalence analyses (I2 > 90% in some models), likely reflecting differences in MRI protocols, ARIA adjudication methods, dosing regimens, and trial populations. Variations in APOE ε4 enrichment, vascular risk profiles, and background antithrombotic use may have further influenced event rates. For certain agents, estimates were based on sparse events or single trials, limiting precision. Although penalized likelihood modeling reduced sparse-event bias, network meta-analysis relies on indirect comparisons and assumptions of transitivity, leaving potential residual confounding. Finally, relatively short follow-up durations (typically 18–24 months) restrict conclusions regarding long-term hemorrhagic risk and cumulative ARIA burden.
Future directions
Future research should prioritize standardized MRI surveillance protocols and harmonized ARIA reporting to improve cross-trial comparability. Genotype-informed trials are needed to refine dosing and monitoring strategies in APOE ε4 carriers, particularly homozygotes. A major gap in the current evidence base is the underrepresentation of racial and ethnic minority populations, including Black/African American and Hispanic individuals, despite their disproportionate burden of AD. Dedicated studies assessing the efficacy and safety of monoclonal antibody therapies in these groups are essential to ensure equitable therapeutic translation. Real-world pharmacovigilance studies will be critical to evaluate ARIA risk in broader clinical populations, especially those with vascular comorbidity or receiving antithrombotic therapy. Finally, mechanistic and therapeutic research should aim to balance amyloid clearance potency with vascular safety through optimized targeting and dosing strategies.
Conclusion
In this meta-analysis of randomized controlled trials, anti–Aβ monoclonal antibodies significantly increased the risk of ARIA, with substantial variability across agents. Donanemab and aducanumab carried the highest risk, lecanemab showed intermediate risk, and other agents demonstrated lower or non-significant associations.
APOE ε4 carriage was a strong determinant of ARIA susceptibility, with a clear gene–dose effect. Overall, ARIA risk is not a uniform class effect but varies by molecular profile and genetic vulnerability. As these therapies enter routine practice, balancing clinical benefit with vascular safety will be essential.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261466097 - Supplemental material for Comparative risk of amyloid-related imaging abnormalities with anti–amyloid-β monoclonal antibodies: A systematic review and penalized likelihood network meta-analysis of randomized trials
Supplemental material, sj-docx-1-alz-10.1177_13872877261466097 for Comparative risk of amyloid-related imaging abnormalities with anti–amyloid-β monoclonal antibodies: A systematic review and penalized likelihood network meta-analysis of randomized trials by Arkansh Sharma, Vinay Suresh, Pavan Raju Kola, Rishu Raj, Fnu Javairia, Allimuthu Nithyanandam, Anmol Kaur, Himanshu Arora, Olivier Uwishema, Dhanya Gorty, Nitya Beriwal, Amogh Verma, Khalid Qidwai, Hardeep Singh Malhotra and Ravindra Kumar Garg in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We acknowledge the use of ChatGPT, a large language model-based AI tool for refining the writing and language quality of this manuscript. The tool was utilized exclusively for enhancing the clarity and coherence of the text, with no influence on the scientific content, analysis, or interpretation of the data.
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets analyzed during this network meta-analysis are derived from the included RCTs, all publicly available in their original published form. Extracted data are available from the corresponding author on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.