
Abstract
Aims:
This study aimed to evaluate Norwegian elder abuse prevention policies using the Toronto Declaration’s framework, focusing on policy agenda configuration, development, and political processes. It sought to identify gaps and propose recommendations for enhancing policy coherence and effectiveness.
Methods:
The analysis employed John W. Kingdon’s Multiple Streams Framework and document analysis to assess the current state of elder abuse prevention policies. Stakeholder interviews provided insights into implementation challenges and opportunities for policy enhancement.
Results:
The study revealed that while Norwegian policies have progressed, significant gaps remain in public awareness, legal enforcement, service accessibility, and systematic data collection. Notably, there is an absence of specific elder abuse legislation. Stakeholder interviews highlighted challenges in policy implementation and suggested areas for improvement.
Conclusions:
Keywords
Background and aims
Elder abuse, defined as “a single or repeated act, or lack of appropriate action, occurring within any relationship where there is an expectation of trust which causes harm or distress to an older person” [1] is a critical issue worldwide. The Toronto Declaration on Elder Abuse provides a comprehensive framework for addressing this issue, emphasizing awareness, legal frameworks, support services, research, collaboration, and training for professionals. In Norway, efforts to prevent elder abuse have been in place since the Declaration, but significant gaps in delivery remain. A report shows that abuse against persons aged 65 and over living at home is between 6.8% and 9.2%, with no significant statistical differences reported between sexes [2]. These Norwegian findings mirror global trends, a meta-analysis estimated that 15.7% of community-dwelling older adults experience some form of abuse, with emotional abuse being most common [3]. In institutional settings, even higher prevalence is encountered, with two-thirds of nursing home staff reporting having committed at least one form of abuse [4]. A recent umbrella review, which synthesized findings across multiple meta-analyses, concluded that elder abuse remains pervasive in both formal and informal care environments, with detection and reporting systems still inadequate in many countries [5]. A new 2025 meta-analysis covering 151 studies across 37 countries estimated that the overall pooled prevalence of elder abuse is 24.3%, with emotional abuse (17.1%), neglect (13.8%), and financial abuse (8.6%) being the most frequently reported forms [6]. This study also highlighted major disparities in prevalence depending on region, care setting, and methodology, with institutional environments showing significantly higher risks and fewer safeguards. In the Norwegian context, a cross-sectional study revealed that over 60% of nursing home staff admitted to engaging in at least one episode of abuse or neglect toward a resident in the previous year [7]. A follow-up identified significant associations between staff-to-resident abuse and work-related stress, burnout, aggression from residents, and lack of support from management, pointing to systemic shortcomings in institutional elder care [8].
These findings are consistent with a systematic review about caregivers’ experiences in dementia care, which showed that aggression from residents, high workloads, and emotional fatigue contribute to an environment where abuse becomes more likely, especially when support systems are lacking [9]. In the literature, it was further confirmed that older adults with dementia are significantly more vulnerable to abuse and neglect in community settings, with prevalence rates ranging from 26% to 55% depending on the type of abuse [10]. In community settings, a study explored the role of informal carers in protecting older adults with dementia. Their findings reveal that family carers often act as frontline defenders against abuse but receive little formal support or guidance, raising concerns about caregiver burnout and safety [11]. Similarly, a study assessing the feasibility of preventive home visits in Norway found that proactive outreach through multidisciplinary health teams can detect risks early and reduce isolation, which is a known risk factor for abuse [12].
Another risk factor and system-level vulnerabilities are also portrayed in the literature: a study identified institutional weaknesses that elevate abuse risk [4]. An investigation into how nursing home leaders in Norway respond to abuse cases found a lack of standardized procedures and accountability structures. In addition, leaders often relied on informal discussions rather than formal investigations, reflecting a broader issue of fragmented leadership and unclear guidelines in elder care institutions [13]. In a complementary context, research examined how Norwegian police interact with victims of elder abuse in familial settings. The study showed that while police officers often expressed empathy, systemic challenges such as insufficient inter-agency collaboration and lack of targeted legal frameworks hampered effective protection [14].
Over the past two decades, elder abuse has gradually gained increased attention within Norwegian public discourse, policy development, and service design. One of the earliest national initiatives was the “Vern for Eldre” pilot project launched in Oslo in 1991, later extended nationwide with support from the Ministry of Health and Social Affairs. This project offered telephone helplines, case consultations, and counseling services, reflecting a growing institutional recognition of elder abuse as a distinct form of violence requiring a dedicated response [15]. In the mid-2010s, the TryggEst (SafEst) model was developed by the Norwegian Directorate for Children, Youth and Family Affairs (Bufdir), and piloted between 2017 and 2021. This model introduced a multisectoral framework for safeguarding vulnerable adults, with emphasis on improving inter-agency collaboration between healthcare services, social services, and law enforcement, alongside awareness campaigns and procedural guidance for municipalities [16]. Despite these efforts, however, elder abuse prevention in Norway remains inconsistently prioritized and fragmented. Many municipal action plans fail to explicitly include older adults in their violence prevention strategies, and no specific legislation or national safeguarding framework exists for the elderly, unlike the more robust systems for children or survivors of domestic violence [17, 18]. This absence of a legal mandate contributes to underreporting, uneven service implementation, and unclear lines of responsibility across sectors.
The literature review conducted also pointed to implications of health policies and praxis, as the body of research highlights the multifaceted nature of elder abuse, driven by a combination of individual, institutional, and systemic factors. Across all studies, one common theme emerges: the critical need for integrated, sustained, and evidence-based prevention strategies that operate across sectors—health, social services, and law enforcement [8, 13, 14]. While elder abuse is increasingly recognized as a public health issue, gaps persist between research, policy, and practice. In the Norwegian context, inconsistencies in implementation, underreporting, and the absence of a dedicated legal framework continue to undermine effective prevention [13, 15]. The World Health Organization’s (WHO) Tackling Abuse of Older People: Five Priorities for the United Nations Decade of Healthy Ageing (2021–2030) outlines key global priorities—combating ageism, improving data collection, developing effective interventions, making an investment case, and raising funds—that align closely with the Toronto Declaration’s framework [1]. This study contributes to the field by applying Kingdon’s Multiple Streams Framework (MSF) [19] to examine how elder abuse is framed as a policy issue in Norway, what responses have emerged, and what systemic barriers persist. Through qualitative document analysis and interviews with key stakeholders, this research explores the alignment—and misalignment—between international frameworks and national implementation.
Methodology
This study employed a qualitative research design using the triangulation method [20], combining document analysis and interviews with key informants [21]. The purpose was to explore how elder abuse is defined, prioritized, and addressed within national policies and institutional frameworks in Norway. This methodological approach allowed an in-depth examination of systemic responses at a structural governance level, rather than focusing on individual cases. The document analysis provided an understanding of the legal, political, and professional discourse surrounding elder abuse, while the interviews offered insights from individuals directly involved in policy development, oversight, and implementation. The section is organized as follows: first, the document analysis procedures are described, followed by the interview procedures, as the interviews were conducted after the document analysis to address identifiable gaps.
Document analysis
Document analysis followed Glenn Bowen’s [22] principles for reviewing and evaluating printed and electronic materials. The purpose was to convey the meaning, gain understanding, and develop empirical knowledge relevant to elder abuse prevention policy. A purposeful selection process guided the inclusion of documents, focusing on legal and policy documentation concerning elder abuse within the public health context for older people in Norway.
The final sample consisted of nine documents (N = 9), including municipal action plans (n = 1), project reports (n = 3), legal records (n = 1), and relevant public policy strategies and national guidelines (n = 4). These documents were selected to reflect the evolution of public health policy through historical, political, and institutional processes and to support a rights-based analysis of current elder abuse prevention efforts (see the Appendix for the full list).
The analysis followed Bowen’s approach to qualitative document analysis, beginning with skimming, reading, and interpretation of each document to determine its content, tone, function, intended audience, and contextual relevance [22]. The first stage of analysis focused on understanding each document’s purpose and its contribution to elder abuse prevention discourse. The second stage involved coding the documents to extract key concepts, identify policy gaps, and understand challenges in implementation. Kingdon’s MSF [19] was applied to understand the political processes involved in the formulation and implementation of elder abuse policies. This framework consists of three streams: problems, policies (government actions to face social problems), and politics (a set of activities related to the sphere of power in society, in the state, and its institutions and organizations). The analysis focuses on the convergence of these streams and the subsequent scenario.
Key actors in Norway’s elder abuse prevention scenario include: (a) non-profit organizations (such as the Norwegian Pensioners’ Association) that have played a role in lobbying for stronger protection and better resources for older persons, actively raising awareness among the public and policy makers about elder abuse; (b) academic institutions and researchers that contribute to understanding elder abuse, particularly in terms of its prevalence, causes, and impact on health and wellbeing; (c) public-sector initiatives, such as the Norwegian government pilot TryggEst—a safeguarding model for all vulnerable adults; (d) politicians at the Stortinget (National Assembly) that inquired about proposed national guidelines and a mandatory reporting system for elder abuse cases, which has still not been implemented, despite agreement being reached in the Norwegian parliament in Case 13/2021, Resolution 986 (national guidelines) and 987 (mandatory reporting).
To guide the thematic coding, the following analytic questions were applied to each document: (1) What function does this document serve (legal, political, educational)? (2) What assumptions does it make about elder abuse and its prevention? (3) How is elder abuse framed (as a health, legal, or social issue)? (4) Who is the document intended for (policy actors, practitioners, public)? (5) What contradictions or gaps appear across the documents? Based on this analysis, five core thematic categories were established: (1) awareness and education, (2) training and professional development, (3) legal frameworks, (4) cross-sector collaboration, and (5) systematic research and data collection. These categories formed the analytical backbone of the study’s results and discussion, illustrating the structural strengths and shortcomings of Norwegian elder abuse prevention policy.
Interview procedures
Following the document analysis, the study conducted 11 semi-structured interviews with 15 representatives from Norwegian authorities and stakeholder organizations involved in elder abuse prevention. The research was approved by the Norwegian Agency for Shared Services in Education and Research (SIKT—reference 910786) and followed national ethical research guidelines.
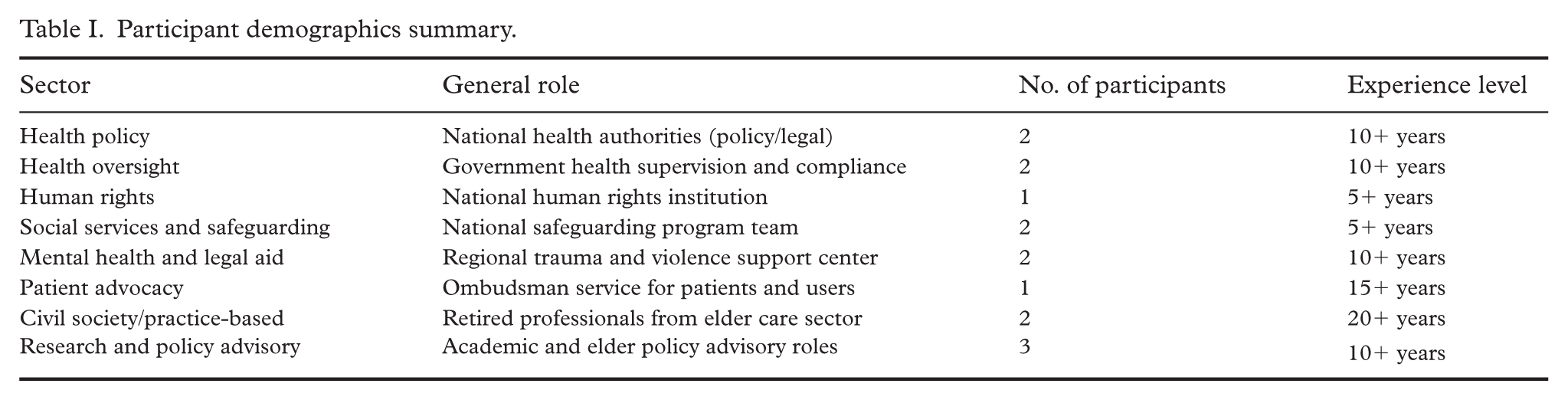
Participants were recruited through purposive and snowball sampling strategies to ensure representation from individuals with direct roles in developing, implementing, or overseeing elder abuse policy in Norway. The final sample included professionals from 11 institutions across health, legal, and advocacy sectors. Participants were selected based on their expertise with elder abuse either at the system level (e.g., policy implementation, legal oversight, human rights monitoring) or in applied program development. See Table I for a summary of the participants’ demographics. The research deliberately prioritized policy makers, program managers, legal specialists, and autonomous bureaucrats—those actively shaping or evaluating the public response to elder abuse. This participant focus reflected the core aim of the study: to investigate the governance and institutional dynamics of elder abuse prevention within the framework of Kingdon’s MSF.
Participant demographics summary.
Physicians, frontline care workers, and victims of abuse were not included in the sample. This exclusion was a deliberate methodological choice based on the study’s scope, which centered on how elder abuse is constructed, addressed, and governed at the national level. While such voices are essential to understanding the full picture, their inclusion would have shifted the focus toward clinical or experiential dimensions better suited for research on service delivery or lived experience.
Thematic analysis of the interview transcripts was conducted to identify patterns and perspectives aligned with the five analytical categories developed during document analysis: (1) awareness and education, (2) training and professional development, (3) legal frameworks, (4) cross-sector collaboration, and (5) systematic research and data collection.
All interviews were manually coded using a combination of deductive and inductive approaches. Deductively, Kingdon’s MSF guided the classification of participants’ reflections into the problem stream (issue recognition), policy stream (available solutions), and political stream (institutional dynamics). Inductively, new patterns were allowed to emerge from the data through close reading of participant narratives and meaning units.
The analysis focused on how participants framed elder abuse in their roles, identified institutional strengths and gaps, and interpreted policy developments. Stakeholders provided both operational and critical perspectives—some reflecting internal governmental challenges, others speaking from oversight or advocacy roles. The integration of these cross-sectoral views allowed the study to triangulate how policies are understood and applied in practice, and where structural weaknesses persist.
Analytical framework: application of Kingdon’s streams and thematic development
The analytical categories applied in the results section were developed through an iterative process combining both deductive and inductive approaches, grounded in established literature and guided by Kingdon’s MSF [19]. Deductively, categories such as legal frameworks, training, and cross-sector collaboration were informed by key international guidelines (e.g., the Toronto Declaration on the Global Prevention of Elder Abuse) [1], empirical studies on elder abuse in Norwegian institutions [2, 13, 15], and public health policy priorities as outlined in national strategies.
Inductively, themes such as awareness and education, as well as systematic data collection, emerged from repeated patterns observed during document and interview analysis. The research team systematically applied Bowen’s qualitative document analysis method (i.e., examining tone, content, function, and audience), and used thematic coding to identify meaning units within stakeholder interviews that revealed gaps in awareness efforts, legal ambiguities, and fragmented implementation [22].
Kingdon’s framework served not just as a theoretical lens, but as an organizing structure for interpreting how elder abuse is defined (problem stream), what policy responses have been proposed (policy stream), and how institutional and political actors prioritize or neglect the issue (politics stream) [19]. For instance, while legal obligations to avert abuse exist in general terms (e.g., Penal Code §196), they remain inconsistently enforced, which stakeholders frequently cited as a failure of both the problem and politics streams.
Thematic patterns across stakeholder interviews revealed cross-sectoral challenges that reinforced the analytical categories identified in the document analysis. For example, the pattern of fragmented service delivery and policy diffusion—echoed by participants from both health oversight and legal bodies—corresponds directly to the category of cross-sector collaboration, a known barrier to integrated elder abuse prevention systems internationally [1, 5]. Similarly, the repeated emphasis on insufficient professional preparedness from actors in frontline, regulatory, and advocacy positions reflected a shared concern over gaps in training and professional development—a category also supported by international meta-analyses that associate limited training with under-detection and poor response to abuse cases [10]. The theme of underreporting and ambiguity in legal mandates, particularly within health and care services, repeatedly surfaced in interviews and aligned with critiques in both Penal Code §196 and national parliamentary debates [5, 23]. Furthermore, emerging concerns about weak or ad hoc data systems reflected global literature highlighting the absence of sustained, national surveillance efforts as a critical policy blind spot [5, 15]. These patterns demonstrated the alignment between perceived field-level constraints and structural policy gaps, reinforcing the relevance of the categories developed and their connection to the broader dynamics of Kingdon’s problem, policy, and politics streams [19].
Results
The results are organized according to the five thematic categories from the document and interview analysis: (1) awareness and education, (2) training and professional development, (3) legal frameworks, (4) cross-sector collaboration, and (5) systematic research and data collection. These categories aligned with the Toronto Declaration [24] and were analyzed through Kingdon’s MSF to provide understanding about how elder abuse prevention policies have been formulated and implemented in Norway.
The Box 1 contains a summary of the document analysis.
Summary of the document analysis.
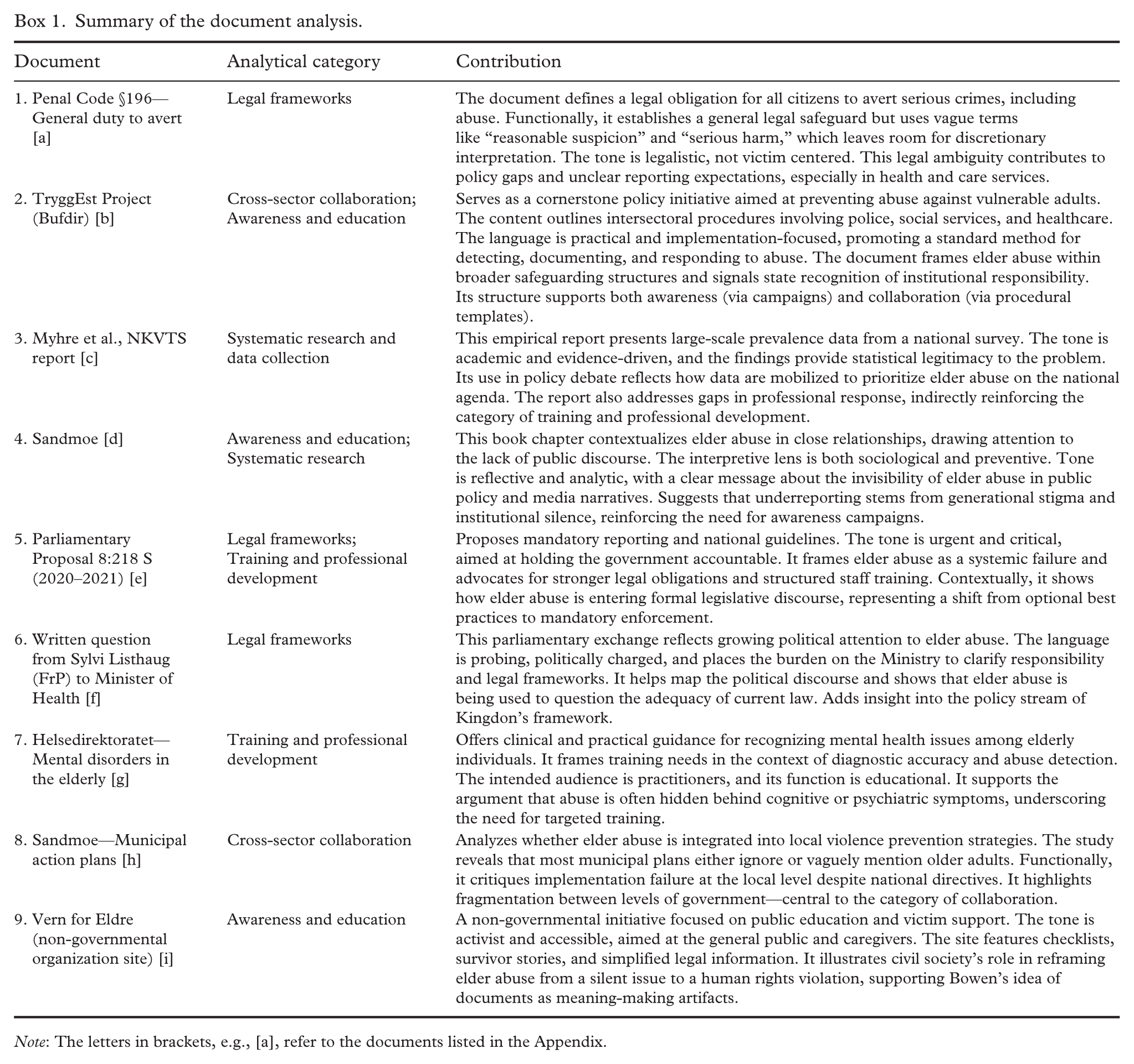
Note: The letters in brackets, e.g., [a], refer to the documents listed in the Appendix.
Three critical patterns emerged across the documents analyzed. First, Norway’s approach relies on general legal provisions rather than elder-specific legislation, creating ambiguity in application and enforcement. While multiple acts contain protective language, they address vulnerable groups broadly rather than targeting older adults’ specific needs. Second, policy responses remain fragmented and non-mandatory. TryggEst represents the primary governmental initiative, yet as of May 2025, it operates in only 51 municipalities with another 29 in implementation phases—leaving significant coverage gaps [16]. The government’s characterization of TryggEst guidelines as “national guidelines” contradicts their non-binding status and limited adoption. Third, a disconnect persists between research evidence and policy action. Studies document prevalence rates of 6.8% to 9.2% [2] in community settings and 60% staff-reported incidents in institutions, yet parliamentary resolutions on national guidelines (Resolution 986) and mandatory reporting (Resolution 987) from Case 13/2021 remain unimplemented.
Stakeholder interview analysis
The interview analysis revealed both convergence and divergence in how different institutional actors understand, respond, and suggest public policies to mitigate elder abuse. Box 2 maps the thematic insights from each participant/group using anonymized institutional descriptors that align with the sectors presented in Table I, to ensure informant confidentiality.
Interview themes mapped to analytical categories.
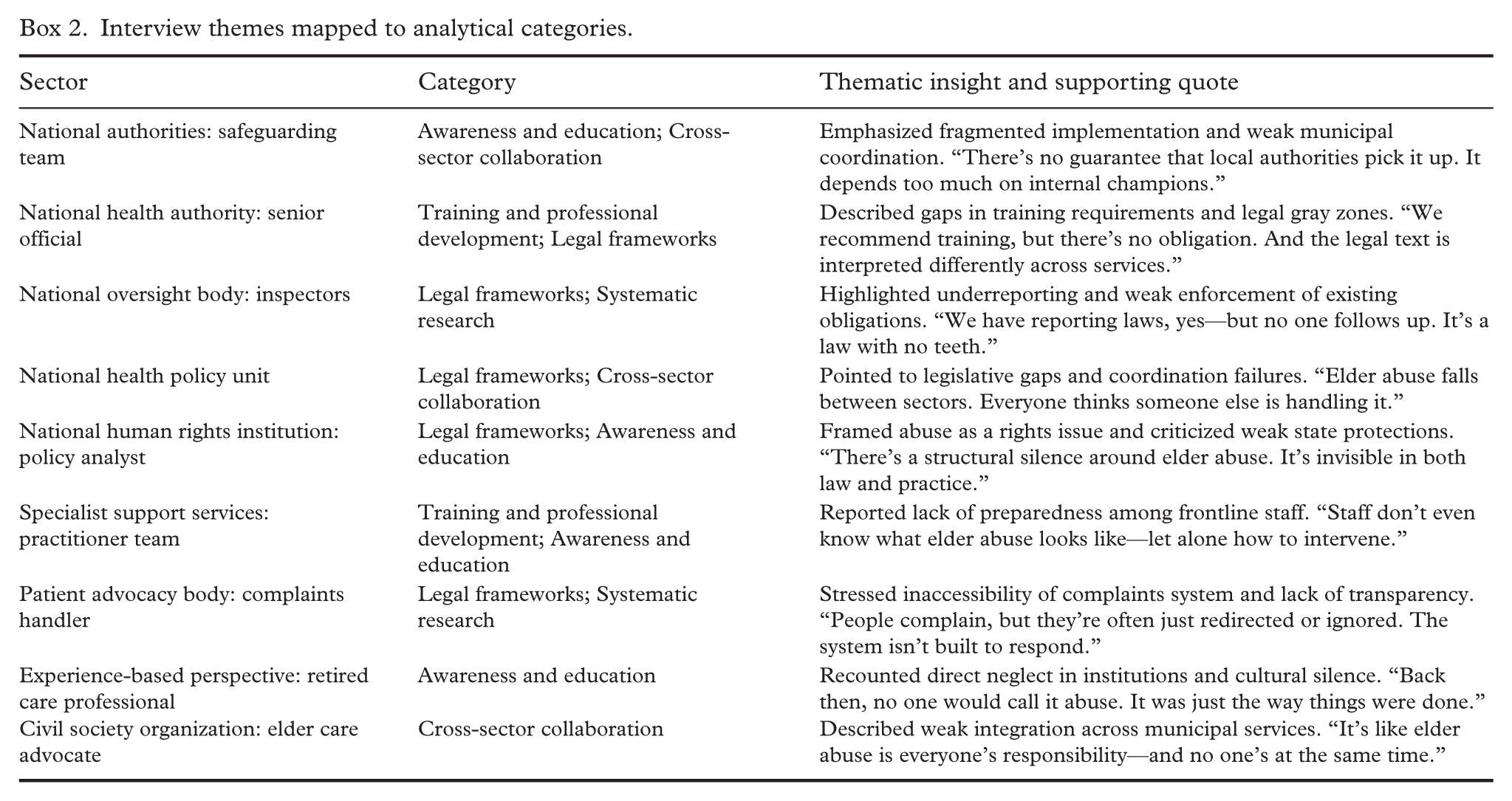
Across the interviews emerged recurring contradictions between policy intention and implementation. The disparities, exacerbated by compartmentalized duties, were most pronounced in intersectoral collaboration and legal enforcement. Systematic variations in perspectives according to institutional roles revealed not only gaps in implementation but also divergences concerning responsibility and accountability.
Awareness and education
Stakeholders reported that awareness campaigns exist but lack sustained impact and fail to reach rural and underserved areas. As one senior policy representative stated: “Public campaigns must be continuous and adapted to reach all parts of society, especially rural areas” (Interview, national health authority, 2024). A representative from a national safeguarding program noted fragmented implementation: “There’s no guarantee that local authorities pick it up. It depends too much on internal champions” (Interview, national safeguarding program, 2024). Generational stigma compounds these challenges, as a civil society representative with elder care experience recalled: “Back then, no one would call it abuse. It was just the way things were done” (Interview, civil society representative, 2024).
Training and professional development
While the national safeguarding program provides training materials covering approximately 47% of the population, stakeholders emphasized persistent gaps. A specialist health practitioner stated, “Staff don’t even know what elder abuse looks like—let alone how to intervene” (Interview, specialist health services, 2024). A senior policy representative described the non-mandatory nature: “We recommend training, but there’s no obligation. And the legal text is interpreted differently across services” (Interview, national health authority, 2024). Participants noted disparities for rural municipalities and emphasized, “Training must be continuous and address specific issues related to elder abuse” (Interview, national authority, 2024).
Legal frameworks
The absence of elder-specific legislation emerged as a critical gap across all participant groups. One policy and legal affairs representative noted, “There are many paragraphs in the Penal Code that can protect the elderly if one knows about them” (Interview, legal and policy affairs, 2024), while another stated, “We need specific regulations to protect the elderly, not just general ones” (Interview, national authority, 2024). Oversight officials highlighted enforcement failures: “We have reporting laws, yes—but no one follows up. It’s a law with no teeth” (Interview, national oversight body, 2024). A policy representative at national level described institutional confusion: “Elder abuse falls between sectors. Everyone thinks someone else is handling it” (Interview, health policy unit, 2024). A human rights expert characterized this as, “There’s a structural silence around elder abuse. It’s invisible in both law and practice” (Interview, human rights organization, 2024).
Cross-sector collaboration
Stakeholders emphasized resource constraints and coordination failures. One stated, “Resource problems are well-known; it’s very challenging to uncover and handle violence and abuse in institutions” (Interview, national authority, 2024). Another emphasized, “Coordination is crucial; it requires resources across sectors working together” (Interview, national level, 2024). A civil society participant described fragmented responsibility: “It’s like elder abuse is everyone’s responsibility—and no one’s at the same time” (Interview, civil society representative, 2024). A participant from a patient advocacy body stressed system inaccessibility: “People complain, but they’re often just redirected or ignored. The system isn’t built to respond” (Interview, patient advocacy office, 2024).
Systematic research and data collection
Participants emphasized gaps in continuous data collection despite existing research projects. One stated, “We need more knowledge about violence against elderly people, especially those with dementia or other vulnerabilities” (Interview, national level, 2024). Another highlighted, “It depends on who’s in charge locally. Some places don’t follow up at all” (Interview, safeguarding program, 2024), indicating that data collection, like other prevention efforts, varies by municipality. Stakeholders noted that implementing the national safeguarding model across all municipalities would create the comprehensive database that is currently lacking.
Discussion
This study analyzed Norwegian elder abuse prevention policies through Kingdon’s MSF [19], integrating document analysis with stakeholder interviews to assess alignment with the Toronto Declaration’s recommendations. Kingdon’s framework theorizes that significant policy change occurs when three streams converge: the problem stream (where issues gain recognition through data and focusing events), the policy stream (where solutions are developed and refined), and the politics stream (where political will, resources, and institutional commitment determine implementation) [19].
The findings revealed that while elder abuse is well-recognized in Norway’s problem stream, and policy solutions have been proposed, implementation stalls in the politics stream, where fluctuating priorities, weak intersectoral mandates, and limited visibility inhibit sustained action. This pattern of hindered convergence explains the persistent breaches across all five thematic areas examined below.
Awareness and education: fragmented campaigns and limited reach
Norway has initiated campaigns, including online courses recommended by the Norwegian Directorate of Health [25]. However, these campaigns lack sustained impact and fail to reach rural and underserved areas [15]. Vulnerable groups—people with dementia, isolated elders, and ethnic minorities—are particularly underserved. Generational stigma and silence compound the invisibility of abuse [2]. Research indicates that sustained and targeted campaigns are more effective in changing public attitudes and behaviors [26, 27], yet Norwegian efforts remain episodic. This gap suggests that awareness initiatives require not only policy recognition but sustained political commitment and resource allocation to ensure reach and continuity across geographic regions, population groups, and service sectors.
Training and professional development: non-mandatory and insufficient
Training programs exist for healthcare workers, social workers, and law enforcement officers [15, 28]. TryggEst provides open access training materials covering approximately 47% of the population [16]. However, programs are neither widespread nor specialized enough to address elder abuse’s unique aspects. The non-mandatory nature particularly weakens effectiveness, as disparities persist in rural municipalities and under-resourced institutions.
Research demonstrates that ongoing, specialized training is crucial for early detection and effective management [29, 30]. Norway requires mandatory, standardized training protocols to be embedded within professional certification and continuing education requirements, supported by adequate funding. Without binding requirements, training coverage remains dependent on local champions and institutional priorities rather than systematic professional preparation.
Development of legal frameworks: general provisions without elder-specific legislation
Norway lacks elder-specific abuse legislation, instead relying on general Criminal Code provisions (Sections 196 and 282) and health-related acts [23, 31]. This creates protection breaches, particularly for subgroups with complex needs such as those with dementia. Enforcement remains vague and inconsistent with limited monitoring mechanisms. Research shows that comprehensive legal frameworks tied with effective enforcement are critical for reducing elder abuse [32, 33]. The absence of targeted legislation reflects what stakeholders described as “structural silence”—elder abuse remains legally addressed through general provisions applicable to all citizens rather than protections recognizing older adults’ specific vulnerabilities. Comprehensive legal frameworks require not only statutory language but clear thresholds, documentation requirements, institutional responsibilities, and enforcement mechanisms—elements currently absent from Norway’s approach.
Support services and multidisciplinary collaboration: fragmented implementation
Support services exist through TryggEst and earlier Protective Services for the Elderly (PSE) initiatives [14], yet accessibility remains uneven across jurisdictions. Norway’s strong municipal autonomy means services vary widely in quality and availability, undermining national strategies. Service integration is complex, making navigation difficult for victims. Research indicates that collaborative approaches significantly enhance effectiveness of prevention and intervention programs [32, 34]. In addition bureaucratic obstacles and communication breaches delay cooperation despite existing frameworks [15, 35].
The government maintains that mandatory reporting is unnecessary given the existing regulations in the Health Personnel Act [36], Health and Care Services Act [37], and National Commission of Inquiry Act [38]. However, neglect, economic exploitation, and psychological abuse are not explicitly covered, creating enforcement openings. Fragmented services and collaboration reflect a systemic issue where policies exist but are not adequately operationalized, particularly given Norway’s decentralized governance structure. This suggests that national guidelines alone are insufficient without binding mandates and mechanisms for accountability and coordination across municipal boundaries.
Research and data collection needs: evidence without translation
Norway has funded significant research projects including national studies on violence against the elderly [15], abuse in long-term care settings [7, 39], and informal caregiver surveys [40]. More critically, research findings are not consistently translated into policy actions, resulting in missed opportunities for improving prevention strategies [15, 35]. Scientific publications, especially in the Norwegian context, lack longitudinal perspectives, limiting the ability to track change over time and thereby impacting informed policy decision-making [3, 33]. This disconnection between the problem stream (where research establishes the scope and nature of elder abuse) and the policy stream (where evidence should inform concrete interventions) reflects insufficient political commitment to evidence-based policy making.
Comprehensive data collection is fundamental for informed policy development and effective intervention strategies [3, 33]. Norway’s current approach, however, remains project-based and episodic rather than systematic and continuous. Establishing mandatory reporting mechanisms coupled with centralized data collection systems would enable longitudinal tracking, trend analysis, and evidence-based policy adjustments—elements currently absent from Norway’s elder abuse prevention infrastructure.
Conclusion
Through the frame of the Toronto Declaration and Kingdon’s MSF, the analysis revealed that although elder abuse is recognized in Norway’s problem and policy streams, measures to mitigate it are not recognized in the politics stream. The results that emerged from the document and interview analysis revealed that it occurs due to fluctuating priorities, weak intersectional mandates, and insufficient public visibility, that is, political stagnation prevents the translation of policy proposals into effective implementation.
Significant breaches in policy coherence and effectiveness were identified, which confirmed the study’s initial concerns. Norway lacks specific elder abuse legislation comparable to child protection laws. This creates legal ambiguity that produces inconsistent municipal responses and inadequate follow-through on reported cases. Additional deficiencies include insufficient public awareness, inconsistent application of preventive measures, systematic underreporting, and limited service accessibility.
To improve policy and political effectiveness, Norway must establish dedicated elder abuse legislation. This legislation should include enforceable mandates and clear protocols that integrate health-, legal-, and social services. Municipalities should be required to implement functioning adult welfare systems. These must be supported by national guidelines and mandatory reporting mechanisms. Strengthening public awareness campaigns, ensuring systematic data collection, providing trauma-informed training, and enhancing multisectoral coordination are crucial steps. These recommendations address the identified gaps. They provide a pathway for Norway to align with WHO guidelines and the Toronto Declaration. Ultimately, this will improve protection for older adults.
Footnotes
Appendix. Public health documents analyzed
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.