
Abstract
Aims:
To explore perceived work ability after sickness absences of varying durations.
Methods:
Questionnaire data from the Healthy Finland survey in 2022–2023, which included self-rated work ability (SRWA), were linked with registry data of the Social Insurance Institution of Finland on sickness allowance for the period 2021–2022. The association between the number of disability days on sickness allowance over a period of 2 years and SRWA were analysed among sickness allowance recipients (N = 2398) by cross-tabulation and multinomial logistic regression taking potential confounding factors into account.
Results:
The number of days on sickness allowance (p < .001) was associated with subsequent perceived work inability: the probability of perceived work inability increased with more sickness allowance days. Among individuals who received sickness allowance for more than 300 days over 2 years, the relative risk ratio was 174.5 for perceived work inability and 13.6 for perceived partial work inability, compared with those who received sickness allowance for 1–30 days. Nonetheless, only 44% of those with over 300 sickness allowance days perceived themselves to be completely unable to work. Individuals who did not believe they could work until normal retirement age were more likely to perceive themselves as completely or partially unable to work.
Conclusions:
Background
Identifying individuals at risk of permanent disability is crucial for targeting timely support and rehabilitation interventions [1]. Work ability is not a binary state: it is not simply present or absent. Even with reduced functional capacity, partial work ability may exist, which can be utilised to enable continued participation in the workforce.
Most individuals experience temporary inability to perform their usual work at some point, for example when illness impairs their functioning and requires rest and medical care. However, absences due to illness are typically short, lasting no more than a few days [2]. In Finland, the Social Insurance Institution (Kela) compensates for income losses due to illness-related disability through sickness allowance if the disability lasts more than 10 days. Such absences are less common. In 2023, 8.5% of the Finnish population aged 16–67 received sickness allowance [3].
Perceived work ability has been shown to be a good predictor of subsequent work ability [4–14]. Poorer perceived work ability has been shown to predict greater sickness absence [7–9], slower return to work following absence [10,11], fewer days of employment [12] and an increased likelihood of transition to disability pension [4–8,14]. Studies have been conducted across various populations using a range of methodologies. Self-assessment of work ability has employed multiple measurement tools, most notably the Work Ability Index (WAI), which is based on a series of questions across seven domains, and the Work Ability Score (WAS), which is derived from the first question of the WAI [15]. In addition, a direct question about an individual’s own experience of their work ability, that is, self-rated work ability (SRWA), has demonstrated usefulness in population studies [4,15]. In SRWA, the respondents estimate their current work ability as completely fit for work, partially unable to work, or completely unable to work.
Both recurrent short-term and prolonged sickness absence are associated with permanent work disability and the transition to disability pensions [16,17]. Perceptions of work ability are shaped not only by health status but also by the demands and conditions of the work environment [18]. Furthermore, prior experiences of sickness absence may contribute to how individuals perceive their work ability. From the perspective of preventing work disability, it is essential to gain a more detailed understanding of how individuals who have received sickness allowance for varying durations perceive their work ability, particularly regarding partial work ability. However, to the best of our knowledge, perceived work ability after sickness absences of varying durations has not been previously studied. Therefore, we aimed to examine the perceived work ability of individuals receiving sickness allowance for varying durations, with a particular focus on also taking into account partial work ability.
Methods
This study is based on the nationally representative Healthy Finland survey, which provides information on the health and well-being of adults living in Finland [19]. In total, 61,600 randomly selected permanent residents of Finland over the age of 20 were asked to participate in the survey. Work-related questions were asked of participants under the age of 75. The sample was restricted to participants aged 67 years or younger, the age range eligible for sickness allowance. Of individuals within this age range, 37,966 were invited to participate in the study, and 14,688 (38.7%) of them responded between September 2022 and March 2023. These data were linked to Kela’s registries on paid sickness allowances from 2021 to 2022. For the purposes of our analyses, we only included individuals who had received sickness allowance in 2021–2022, resulting in a study population of 2398 participants.
For the Healthy Finland survey, the ethical review was conducted by the Institutional Review Board of the Finnish Institute for Health and Welfare. Participants were informed via an invitation letter, an information leaflet, and study website, which included the Privacy Notice for the Healthy Finland survey and details on linking data to Kela’s registries. Filling out the questionnaire was considered to indicate consent to participate in the survey.
In the questionnaires, the participants evaluated their work ability using SRWA, a three-level self-assessment tool with a strong association to the WAI and WAS, both of which have been shown to predict work disability in earlier population studies [4,15].
This SRWA is a single-item measure with verbal response options, unlike the numerically rated WAS or the multi-item WAI. It is intended for use in population studies that include participants who are not employed. It assesses current work ability irrespective of the participant’s employment status and is completed by selecting one of three verbal response options: completely fit for work, partially unable to work, or completely unable to work [15].
The participants were asked to assess their current health status with five response options: 1) good, 2) fairly good, 3) average, 4) fairly poor, or 5) poor. They were also asked whether they believed, based on their health, that they would be able to continue working in their occupation until the statutory retirement age. The response options ranged from 1) no, 2) probably not, 3) probably yes, 4) yes, and 5) I am retired. In the analyses, we combined these options into two categories: no (including no and probably not) and yes (including yes and probably yes). The retired were excluded from these analyses.
Employment status was determined through a multiple-choice question with the following options: 1) full-time employment, 2) part-time employment, 3) retired due to age, 4) disability pension or rehabilitation allowance, 5) partial pension, 6) unemployed or laid off, 7) parental leave, stay-at-home parent, or 8) other. Participants working part-time while receiving a partial pension may have selected either response option 2 or 5, and they were analysed according to the option they chose. In the analyses, we combined these groups into three categories: working population (1–2), retired (3–5), and other (6–8). The participants were asked to report their household income for the previous year, categorised into five levels: 1) less than €15,000, 2) €15,000–35,000, 3) €35,001–55,000, 4) €55,001–75,000, and 5) more than €75,000.
Data on sickness benefits paid from 2021 to 2022 were obtained from Kela’s sickness allowance registries. Participants who received sickness allowance during 2021–2022 were classified into seven categories based on the number of days on sickness allowance during the 2-year period: 1) 1–30 days, 2) 31–60 days, 3) 61–90 days, 4) 91–150 days, 5) 151–230 days, 6) 231–300 days, and 7) over 300 days. This classification is based on Kela’s reference points for work ability and assessment of rehabilitation needs in collaboration with occupational health services [20]. We counted calendar days for sickness allowance recipiency, as sickness allowance is not paid for Sundays or public holidays. Sickness allowance is paid for a maximum of 300 days, except if the incapacity for work is caused by a new illness. Additional days may also be granted if the person has worked for at least 30 days in between. If the incapacity for work continues after the maximum period of sickness allowance, one can apply for disability pension.
Statistical analyses
We cross-tabulated the association between SRWA and other variables. Pearson’s chi-squared test was used to analyse statistical significance. SRWA was analysed across different age groups using cross-tabulation, separately for both sexes. The association between SRWA and perceived ability to continue working in one’s occupation until retirement age, based on health, was also analysed using cross-tabulation across distinct age groups: 1) under 30 years, 2) 30–49 years, and 3) 50–67 years.
A multinomial logistic regression analysis was performed to study the association between disability days on sickness allowance and SRWA, taking sex, age group, employment status, education years, and annual household income into account as confounding factors. The outcome variable was SRWA. Accounting for household size and the number of minors and adults did not affect the results. Therefore, these factors were not taken into account.
Finally, inverse probability weights were used (except for characteristics of study population presented in Table I) to adjust for differences in selection probability, to correct the effects of non-participation, and to improve the generalisability of the results to the Finnish population [19,21]. Analyses were made by using Stata software.
Characteristics of study population cross-tabulated by perceived work ability.
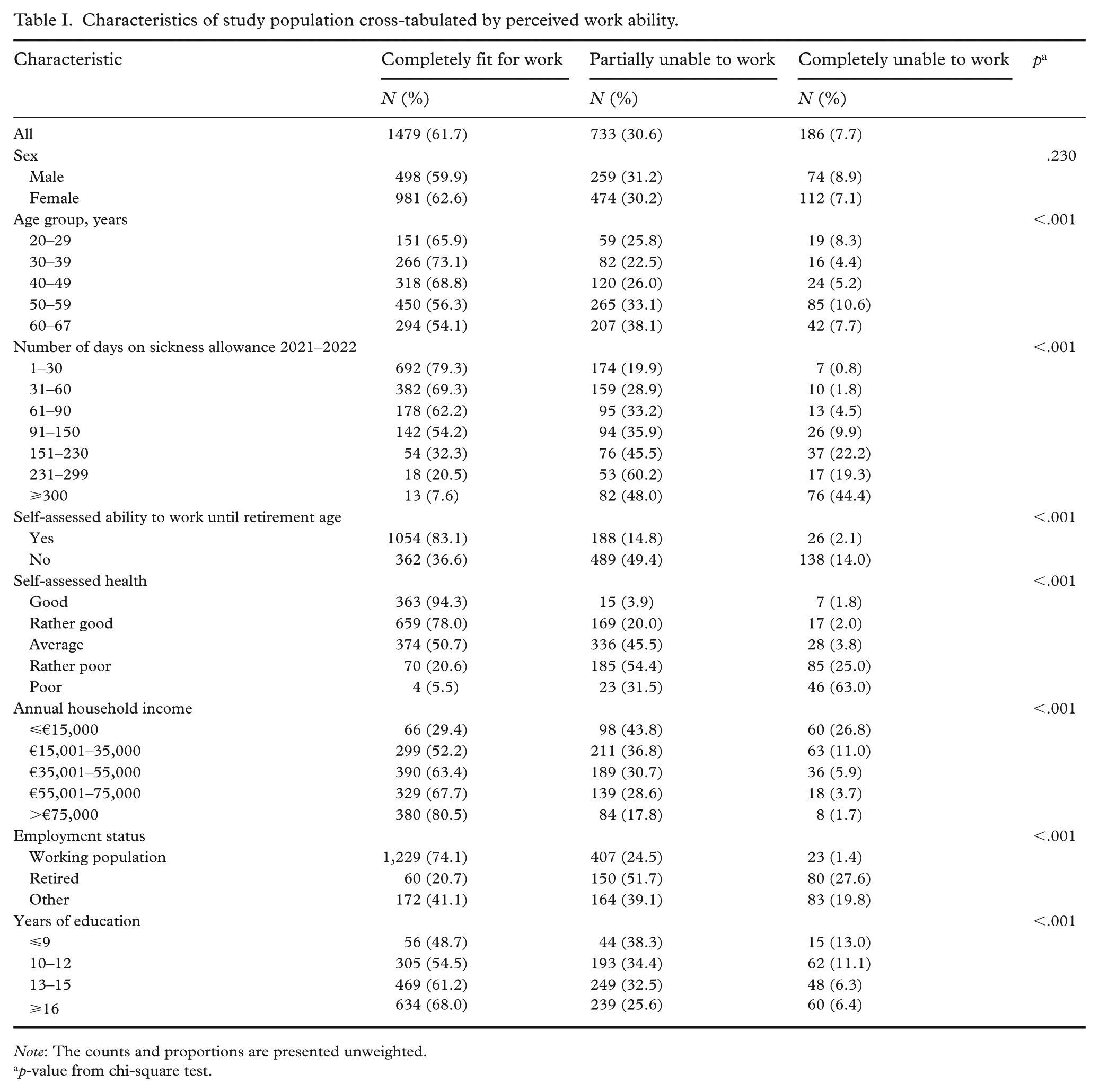
Note: The counts and proportions are presented unweighted.
p-value from chi-square test.
Results
The study population comprised 2398 persons receiving sickness allowance between 2021 and 2022. In the 2022–2023 survey, 1479 (61.7%) reported being completely fit for work, 733 (30.6%) partially unable to work, and 186 (7.8%) completely unable to work. Table I presents the characteristics of the study population cross-tabulated by SRWA.
A statistically significant difference in the number of days on sickness allowance, age distribution, estimated ability to continue working until retirement age, self-assessed health, annual household income, employment status, and education years was observed between groups categorised by perceived work ability. However, there was no statistically significant difference between sexes. Experiences of partial work inability were particularly common among older age groups, individuals with poor self-rated health, those who doubted their ability to continue working until retirement age, recipients of long-term sickness allowance, and those with low income.
Table II presents SRWA separately for males and females by age group. Among those who received sickness allowance in 2021–2022, the highest share of individuals who perceived themselves as completely fit for work was found in the mid-career age groups (ages 30–39 and 40–49) for both males and females. At the start of a career (ages 20–29) and towards the end of a career (ages 50–59 and 60–67) the proportion of those who perceived themselves as partially or completely unable to work increased. There was a statistically significant difference between males and females only in the 50–59 age group, where more males than females assessed themselves completely unable to work.
Self-rated work ability across age groups by sex.
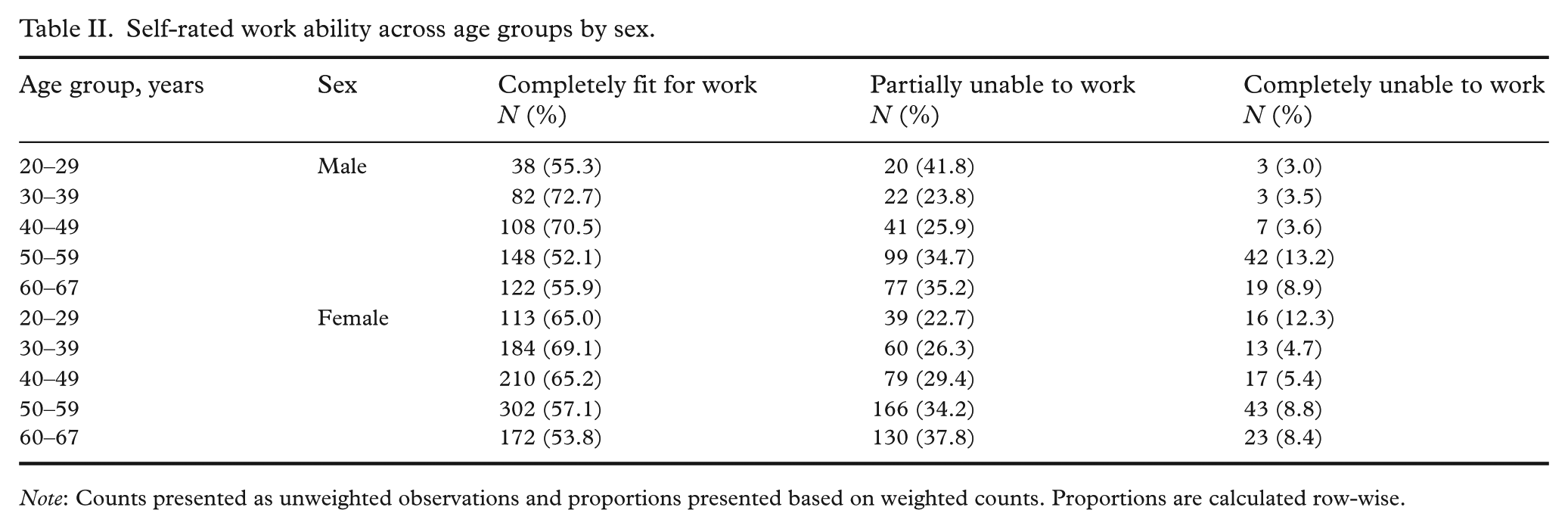
Note: Counts presented as unweighted observations and proportions presented based on weighted counts. Proportions are calculated row-wise.
Table III shows SRWA across different age groups based on whether the individuals believed they were able to continue working until retirement age. Among those who did not believe they were able to continue working until retirement age, a significantly larger proportion perceived themselves as completely or partially unable to work compared to those who believed they were able to continue working until retirement age. This difference was greater in the age group closer to retirement age (50–67 years), where a higher percentage perceived themselves as completely or partially unable to work compared to younger age groups.
The association between self-rated work ability and self-assessed ability to work until retirement age in different age groups.
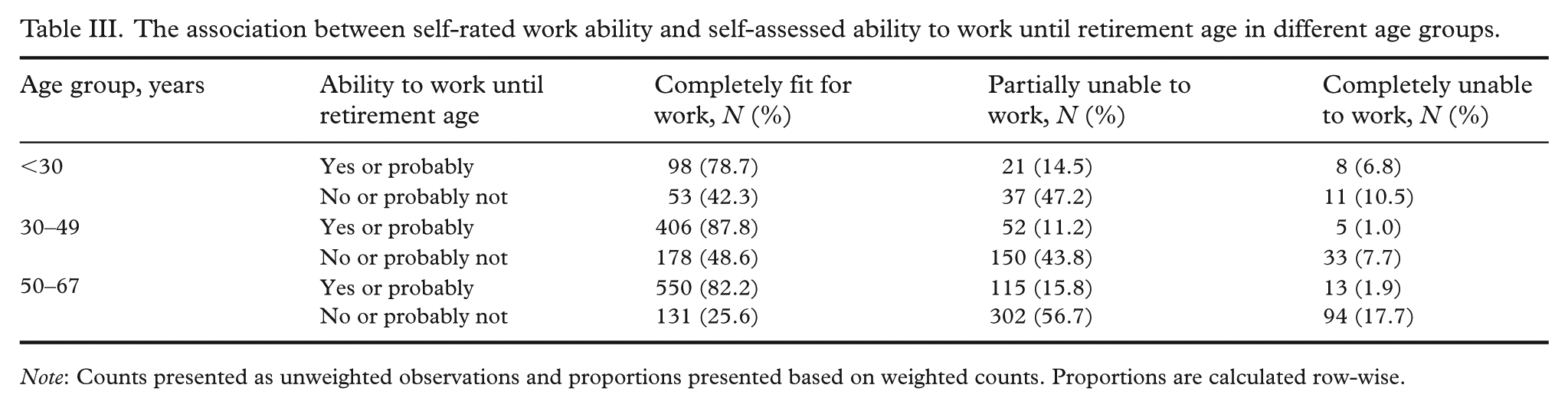
Note: Counts presented as unweighted observations and proportions presented based on weighted counts. Proportions are calculated row-wise.
Table IV presents the results of the multinomial logistic regression analysis on the association between sickness allowance days and self-assessed partial or complete inability to work among those who received sickness allowance in 2021–2022. There was a statistically significant association between these variables even when controlling for age group, sex, employment status, education years, and income level as confounding factors. Those who received sickness allowance for a longer period were more likely to perceive themselves as either completely or partially unable to work compared to those with shorter benefit periods. This association was stronger among individuals who perceived themselves as completely unable to work than among those who perceived themselves as partially unable to work, relative to those who considered themselves completely fit for work. Compared with individuals who had 1–30 days of sickness absence, those with more than 300 days had a 175-times higher relative risk of perceiving themselves as completely unable to work and a 14-times higher relative risk of perceiving themselves as partially unable to work, rather than completely fit for work.
Multinomial logistic regression analysis of the association between days on sickness allowance during 2021–2022 and perceived inability to work, adjusting for confounding variables.
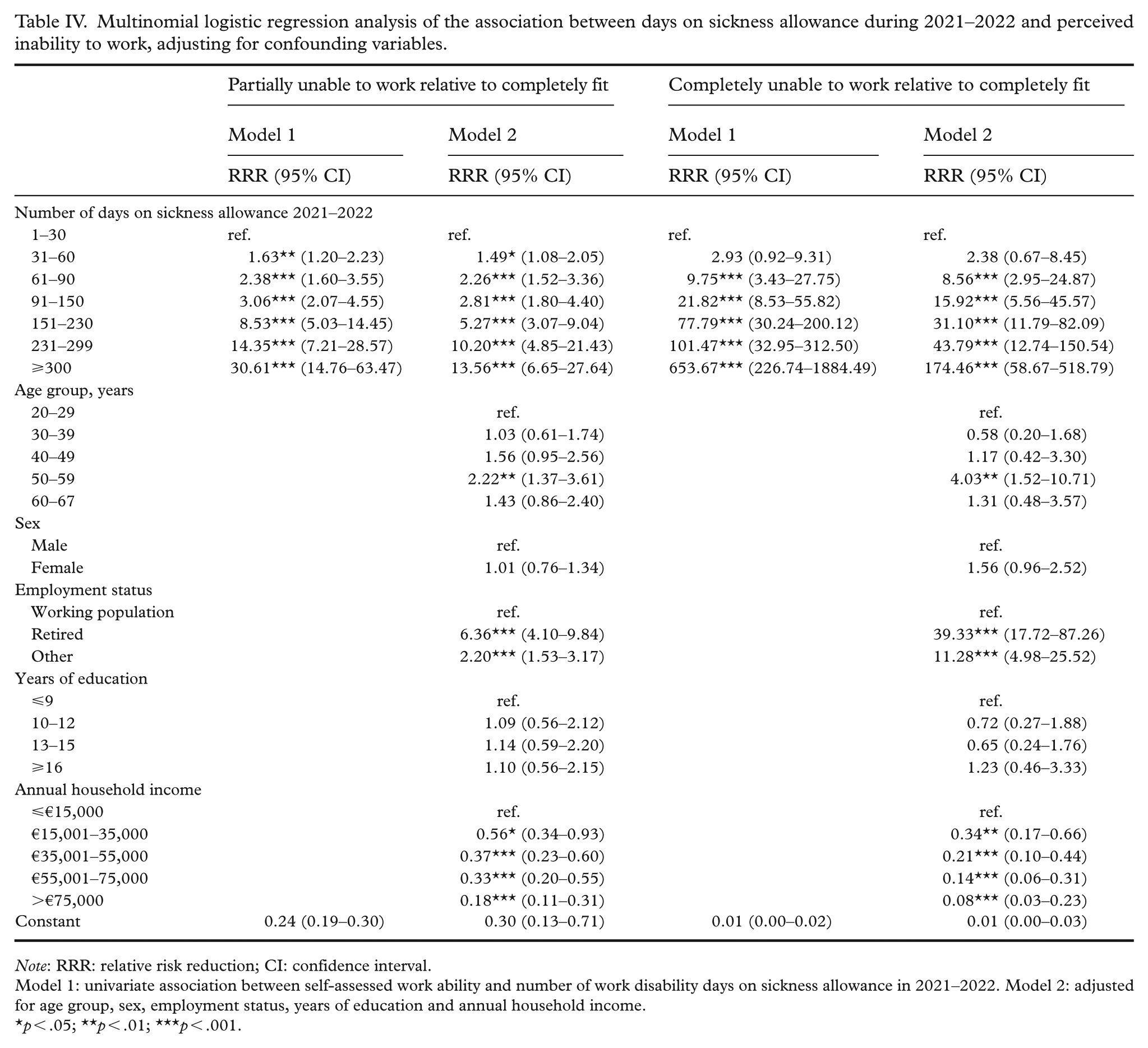
Note: RRR: relative risk reduction; CI: confidence interval.
Model 1: univariate association between self-assessed work ability and number of work disability days on sickness allowance in 2021–2022. Model 2: adjusted for age group, sex, employment status, years of education and annual household income.
p < .05; **p < .01; ***p < .001.
Discussion
The number of days on sickness allowance was strongly associated with individuals’ perceived work ability, even when controlling for confounding factors. The longer an individual had received sickness allowance, the more likely they were to perceive themselves as partially or fully unable to work. Notably, perceptions of partial work inability were particularly common among long-term recipients of sickness allowance, with a majority of individuals with more than 150 allowance days perceiving themselves partially unable to work. Of those with more than 300 days of sickness allowance over the previous 2 years, less than half (44%) perceived themselves as completely unable to work, suggesting substantial potential for rehabilitation and reintegration into the workforce. Nonetheless, most people apply for disability pension after 300 days on sickness allowance. According to an earlier study, only 14% of people did not apply for disability pension, 18% were not granted disability pension, and 68% transitioned to disability pension after 300 days of sickness allowance [22].
Perceived work ability did not differ significantly between sexes. This finding is consistent with previous reports among Finnish municipal employees [5] and German recipients of sickness absence benefits [6]. Although females receive sickness allowance more often than males, sickness allowance periods are on average longer among males [3].
The differences in perceived work ability across age groups were noteworthy among those who had received sickness allowance in the past 2 years. A higher proportion of those aged 20–29 perceived themselves as partially or completely unable to work compared with those in the mid-career age groups. These findings suggest that perceived work ability may vary across different disease groups. For example, sickness absences related to mental health are known to be more prevalent among young people [3].
Among individuals over the age of 50, those who did not believe they could work until retirement age were more likely to perceive themselves as partially or completely unable to work than those in younger age groups. This aligns with findings from a previous study of Finnish municipal employees, which showed the lowest proportion of employees confident about continuing to work until retirement age in the youngest age group (under 30 years) and a clear decline from 2016 to 2022 [23]. Naturally, a longer time until retirement may increase uncertainty about being able to continue working until retirement age, even among those who are currently able to work. These differences may also reflect the varying attitudes and experiences of working life across age groups and generations [24].
In the multinomial regression analysis, the number of disability days on sickness allowance was strongly associated with experiencing partial or full work disability. Among the age groups, individuals aged 50–59 had a higher relative risk of perceiving themselves as partially or completely unable to work, which may be related to diseases affecting work ability that are prevalent in this age group. The association between lower income and a higher relative risk of perceiving oneself as partially or completely unable to work may reflect a reduced capacity to earn income.
The observed association between education years and perceived work ability was statistically significant but relatively modest compared with the previously reported stronger association between education and the risk of disability retirement [25]. When employment status and annual income were additionally accounted for in the same multinomial regression model, the association between education years and perceived work ability was no longer statistically significant. In a previous study examining disability retirement risk, the association with education was also shaped by income and social class [26]. Our study population covered a broad range of working-aged adults, from younger to older adults near retirement age, while the association between years of education and disability retirement risk has been stronger in younger cohorts [25]. Individuals with longer educational backgrounds may also have better opportunities to continue working regardless of impaired perceived work ability, which may contribute to differences in the association of education with perceived work ability and disability retirement risk.
In previous research on the link between perceived work ability and disability benefits, the most commonly used measure has been the WAI or some of its components, such as the WAS, while a direct SRWA has been less frequently used. Nevertheless, even SRWA has previously shown an association with the risk of disability retirement in the general population [4] as well as with employment outcomes among psychiatric patients [27]. This study also demonstrated an association between SRWA and previous periods of sickness allowance.
A notable strength of this study lies in the extensive sample of individuals representing the Finnish adult population and the linkage between reliable registry data on sickness allowance periods and survey responses. However, short disability spells of less than 10 days are not included in these data, as they do not qualify for sickness allowance and are therefore not recorded in the register.
Societal norms shape individuals’ experiences of sickness absence and its role in their personal narratives [28]. Unrealistic expectations and subsequent disappointments may lead to self-stigmatisation, complicating the return to work. Such narratives can influence perceptions of work ability after the sickness allowance period, where the experience of inability may serve as a justification for the often-stigmatised absence. Therefore, efforts to support return to work should also take into account individuals’ self-concept and perceived work ability.
Of those who had received sickness allowance over the past 2 years, 92.2% perceived themselves as completely fit for work or only partially unable to work. From the perspective of perceived work ability, the purpose of sickness allowance, that is, to compensate for short-term income loss, appears to be fulfilled. The high proportion of individuals who perceive themselves as partially unable to work, especially among those with extensive days on sickness allowance, highlights the importance of work-related support measures and timely rehabilitation efforts for work ability. This is particularly relevant, as previous research has shown that individuals’ belief in the benefits of work-related interventions is associated with reduced disability [29]. Further research is needed on the relationship between rehabilitation measures and perceived work ability, as well as the differences in perceived work ability between diagnostic groups.
Conclusions
Even after a long period of sickness absence, only a minority perceive themselves as completely unable to work. However, perceived partial inability to work is common among those who have previously received sickness allowance. Most of those who consider themselves partially unable to work do not believe they will be able to continue working until retirement age. Therefore, it is essential to make use of the remaining work ability to facilitate a return to the labour market and to promote longer work careers, which are essential to ageing populations and sustainable pension systems.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.