
Abstract
Aim
The aim of this scoping review is to identify and describe patterns in personal narratives about the development of alcohol-related problems as presented in scientific health literature.
Methods
A systematic scoping review approach was applied to map and synthesize narrative patterns across the included studies. In total, 45 eligible studies were examined to capture how individuals describe the development of alcohol-related problems in health research.
Results
Across the studies, four major narrative categories were identified: (1) Drinking as a way of coping with difficult thoughts; (2) Drinking as rooted in the body, the genes and the personality; (3) Drinking as a reaction to a stressful situation; and (4) Drinking as a cultural practice or habit.
Conclusion
The findings illustrate the complexity and variability of reasons behind alcohol-related problems. They highlight the importance of interventions that are sensitive to personal narratives, subjective experiences, and the diverse pathways leading to alcohol-related problems.
Introduction
When asked to describe their drinking problems and their causes, individuals typically respond by narrating a personal story of how non-problematic drinking became problematic. Sickness, treatment seeking and healing are, in part, narrative acts (Charon, 2001) and so is suffering from drinking problems. We narrate ourselves when we try to make sense of what is happening, be it behavior, events or symptoms. Narratives involve plots. The notion of emplotment reflects a framework far from medical discourse, imported from literary theory, philosophy of history and phenomenology (Mattingly, 1994); it involves making a configuration in time and creating a whole out of a succession of events. When we narrate and tell stories, we intensify and clarify a plot structure of events as lived; eliminating events that, in retrospect, are not considered important or do not contribute to the potential ending of the narrative (Mattingly, 1994).
Locating ourselves within a story is essential to our sense that life is meaningful. As individuals, we have, so to speak, a narrative interest in constructing a story out of discrete episodes. We have a need to not only make sense (Goffman, 1974), but also to create sense of our life (Mattingly, 1994). We try to make certain things happen, to bring about desirable endings, to search for possibilities that lead in hopeful directions. In other words, we act in what may be called “a sense of ending” (Kermode, 1966).
Narratives about drinking and drinking problems frame self-conceptions of the individual who drinks, including whether the individual may, in fact, be characterized as suffering from an alcohol use disorder or not. Both the narratives and the value-laden language may, however, also influence what people in general perceive as leading to drinking, the consequences of drinking, the impact it has on the individual and what change is considered appropriate to the individual (Hydén, 1995).
In general, a personal narrative is characterized by a dimension of temporality (i.e., events occurring over time); by actors, of which the narrator is one; by references to context that particularize the individual narrative (Bruner, 1991) and, in some cases, an element of evaluation (Labov, 1972). By organizing these elements into a coherent personal narrative about drinking, be it short or long, an individual engages in an interpretation of the self (Ricœur, 1991) and may thus express what sense he or she makes of the drinking. Knowledge of what sense individuals make of their drinking, illustrated by the way they frame, understand and narrate their alcohol use may lay the foundation for gaining insight into how the individual considers change, including the individual's considerations about seeking – or not seeking – treatment, and what treatment he or she might consider acceptable and meaningful. For example, it may have an impact on what to expect from treatment if the individual considers excessive alcohol use to be explained as a “bad habit” or as a reaction on more profound problems.
Little is known about this subjective understanding of alcohol-related problems, and even less is known about whether there are recognizable patterns in the personal narratives by means of which individuals explain their own drinking problems; patterns that might be possible foundations for matching the right treatment to the right individual. A few studies have indicated that patterns may exist (Hammer et al., 2012; Nielsen, 2003), but, to our knowledge, no one has so far systematically searched the scientific literature for personal accounts describing the development of alcohol-related problems and thereby investigated whether there are recognizable patterns in those stories. This is a research gap compared with related research fields, such as Health Humanities, for example, where typologies of illness narratives (Frank, 2013; Hawkins, 1999) have been identified aiming to better understand how illness experiences as both highly subjective and culturally shaped.
Aim
By means of the standards for performing a scoping review, the aim of the present study is (1) to identify potential patterns in personal narratives about alcohol use and how it becomes problematic, as presented in health-scientific literature and (2) to categorize and describe recurring themes by analyzing the characteristics and concerns these narratives reveal.
Methods
Protocol and registration
The present study was reported according to the guidelines described by the PRISMA-ScR Checklist (Tricco et al., 2018) as was relevant for the present review. A protocol for this review was registered in advance in Open Science Framework on the 16 August 2022. The protocol can be accessed via the OSF website by searching for project CX8GQ.
Eligibility criteria
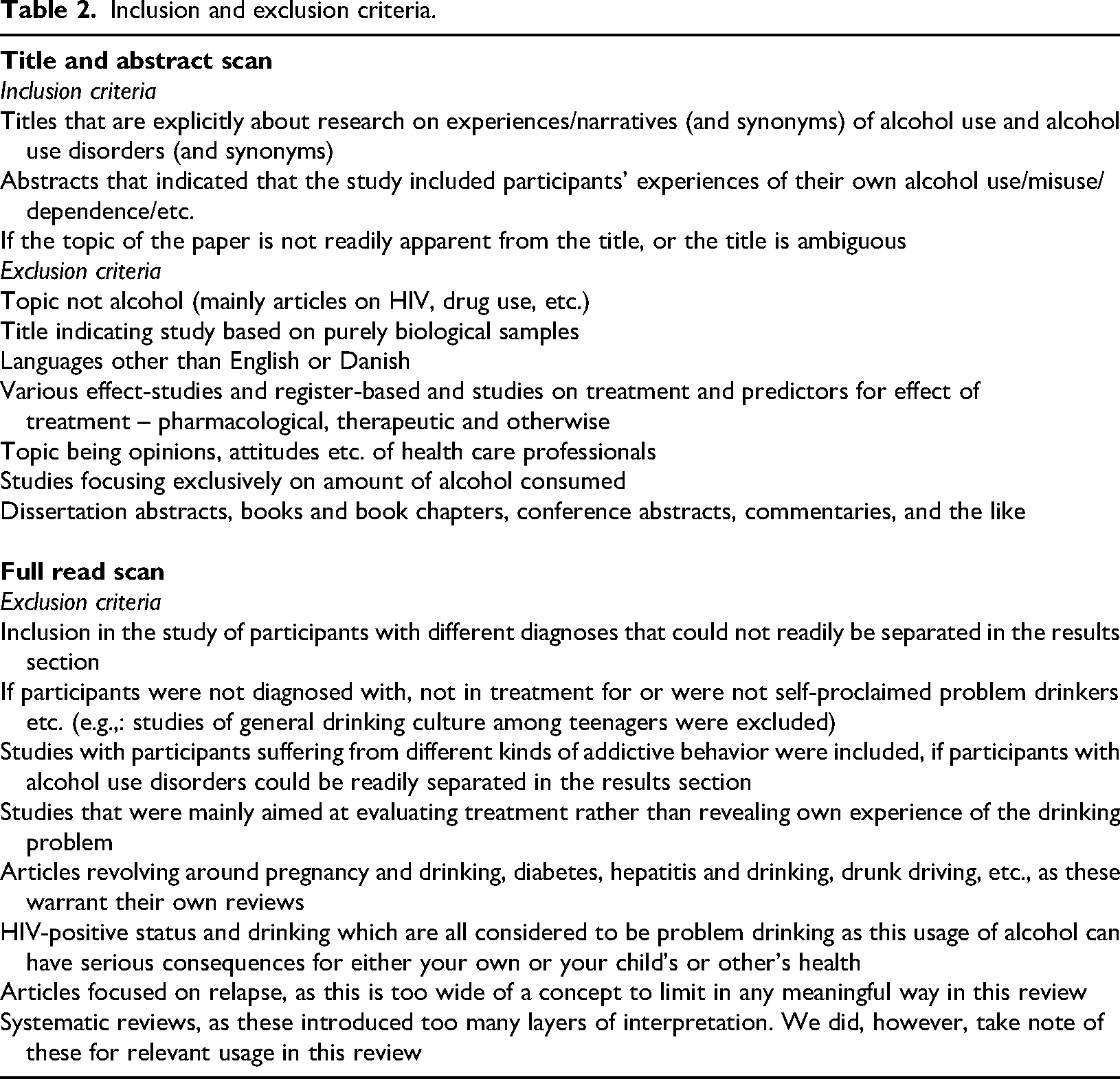
The search criteria were: (1) any study that cites either the patients’ or informants’ own descriptions of personal experiences of developing a problematic alcohol use in their own words (i.e., developing a state that was either diagnosed as an alcohol use disorder or probably might have been, had the informant sought treatment) or (2) their description of their own problematic alcohol use as a state (a state that was either diagnosed as an alcohol use disorder or probably might have been, had the informant sought treatment) would be eligible. As such, there is no limitation on study design, setting or time frame, if the above inclusion criteria is fulfilled. General exclusion criteria revolve around (1) narratives about problematic alcohol use presented by health professionals or treatment staff, and/or based on the staff's descriptions and explanations rather than on systematic information from the individuals suffering from problematic alcohol use; (2) surveys collecting only quantitative data; and (3) studies only presented in a language other than English or Danish. A more precise depiction of the exclusion and inclusion criteria, for both title and abstract scan and full read scan, is provided in Table 1.
Core articles.

Information sources
A systematic literature search was performed in the bibliographic databases of: PubMed, PsycINFO (via Ovid), Embase (via Ovid) and Cinahl (via EBSCO) to find relevant material among medical and psychological databases. The literature search was performed in sequences on the 12 September 2022 and again on the 23 January 2025 (see search strings in Appendix 1).
Search
When conceptualizing the search, we utilized the SPIDER tool because “the PICO tool is not an optimal working strategy for qualitative evidence synthesis” (Cooke et al., 2012). When developing the search strings, we first utilized experts in the study of alcohol use from the Unit for Clinical Alcohol Research (UCAR) to brainstorm relevant key words for narratives, alcohol use and qualitative studies, refining these in the process. These key words were used to find relevant MeSH Terms or Subject Headings in each database, ensuring more sensitivity in our search. These MeSH Terms and Subject Headings were then crosschecked between the four included databases and incorporated into the individual search strings for each database, resulting in an optimization of both the free text search and the subject heading-search. Throughout this process, an information expert from the University Library of Southern Denmark (SDUB) was consulted and helped ensure the quality of our search.
As the SPIDER tool has been criticized for having poor specificity (Methley et al., 2014), we attempted to heighten sensitivity by incorporating a core article (Table 1) for each of the databases. These were examples of articles we would like to find in our search, and, if they were found, would stand as a marker of the quality of our search, in our evaluation of our search strings. We found three of the four articles in Embase, Cinahl and PsycInfo, respectively, but we did not find the last core article (Nielsen, 2003) in Pubmed. This is discussed later in this review.
Study selection and data collection
Using the screening and data extraction tool Covidence, one of the researchers (JGN) screened titles and abstracts for relevance and obvious irrelevance. To heighten sensitivity, any doubts about relevance that were not fully answered in titles and abstracts, were included for a full read. Afterwards, two of the researchers (RC and JGN) both reviewed the full text of the remaining articles, excluding those that did not meet the inclusion criteria (a full overview of the process and excluded articles is provided in Appendix 2). Disagreements concerning eligibility were discussed, resolved and incorporated into Table 2 for inclusion and exclusion criteria in a meeting without the need for a third opinion from another researcher. Three of the researchers (JGN, RC and ASN) each extracted both descriptive information and information for analysis through covidence for insertion into NVivo (https://lumivero.com/products/nvivo) and usage for later analysis.
Inclusion and exclusion criteria.
Data items
To ensure transparency in the results of this review, descriptive data was extracted from the studies selected for inclusion concerning: Authors and year of publication; study country; participant characteristics; the methods with which data was collected; description of alcohol use in the given article, for example alcohol use disorder or problematic alcohol use, and the methods of analysis and/or theoretical approach used in the studies. This was carried out by JGN, RC and ASN.
As this review to a large extent is based on other researchers’ decisions about what patient or informant citations present and much of the data cited consists of brief and/or fragmentary responses from the original informants, two aspects of narratives have been necessary for us to delimit as an operationalization for our analysis. The first is narrative form. Narrative-based research studies are often based on oral narratives that are elicited in the contexts of interviews or treatment (DeFina & Georgakopoulou, 2012). These narratives will not be the full-blown and artfully rendered representations traditionally studied in classical narratology. Instead, oral responses tend toward the form of “small stories” (Bamberg & Georgakopoulou, 2008) that arise in human interaction. As characterized by Bamberg & Georgakopoulou (2008), these may be quite brief or fragmentary forms that vary in the degree to which they explicitly verbalize an actual plot, details or a clear point. The second is the fact that small stories possess the potential to awaken a narrative interpretation by alluding to sequences of events, characters or contexts beyond what is explicitly verbalized. The risk in this broad term is that any utterance may be argued to have narrative potential. To avoid this methodological pitfall, we have included in our working definition criteria that are generally considered characteristic of narrative:
A dimension of temporality – an event or events occurring over time, whether in the past or as a recurring activity, expressed through verbs, verb tense and/or adverbials of time (Nelson & Spence, 2020). One or more actors, of which the narrator is one (Jahn, 2025). References to context, including people and settings, that particularize the individual narrative (Bruner, 1991). In some cases, an element of reflection or evaluation with respect to something that has taken place – the sense that an event or occurrence is significant enough to warrant its telling (Labov, 1972). These criteria may appear even in abbreviated formulations and utterances.
Selection of sources of evidence
Through the literature search in 2022, we identified 4772 articles. In total, 42 articles (n = 42) were found to be eligible and included in the final study sample and three more were added in sequence in 2025. They are presented in Table 3. A PRISMA-flowchart of the study selection process is provided in Appendix 2.
Studies included in the review.

As can be seen from Table 3, most of the participants who delivered data for the included studies were recruited from institutions where they had enrolled in treatment. Eleven studies were based on narratives from men only, 17 studies had both male and female participants, and 11 studies were studies of women's experiences. For some included articles, the categories may have fit more than one of these categories. Each article was placed into one category that was determined to be the “best fit” based on the descriptive features in the researchers’ collective interpretation. For the sake of clarity, we have chosen to group the individual narratives in the category that the researchers thought best described the content.
Synthesis of results
The included articles were read in full by three of the researchers (RC, JGN and ASN). In accordance with the method of analysis for systematic reviews of qualitative data called “Thematic Synthesis” (Thomas & Harden, 2008, the process of data synthesis was conducted in three stages.
Stage 1 and 2
First, the extracted texts revolving around individuals narrating their alcohol use of all final included articles were inserted into NVivo, and two of the researchers (RC and JGN) both employed an inductive approach to thematize quotes, allowing their own interpretations to guide the thematic development rather than being constrained by pre-existing themes. In the realm of qualitative research, the pursuit of unbiased thematic analysis is paramount. The two researchers embarked on their study with a commitment to an inductive approach, allowing themes to emerge organically from the data. This method, known as open coding, ensured that their analysis was not confined by preconceived categories. Instead, they delved into the data with fresh eyes, letting the participants’ voices guide the thematic development.
Throughout the process, the researchers maintained a high level of reflexivity, constantly reflecting on their own potential biases and how these might influence their interpretations. This self-awareness was crucial in mitigating any inadvertent bias. Additionally, they employed triangulation, incorporating multiple data sources and methods to cross-verify the themes, thereby enhancing the credibility of their findings. To further ensure the integrity of their analysis, the researchers engaged in peer review, inviting colleagues to scrutinize their themes and provide feedback. This collaborative effort helped to confirm that the themes were truly reflective of the data and not unduly influenced by the researchers’ perspectives. Through these rigorous methodological practices, the researchers demonstrated a steadfast commitment to unbiased thematic analysis, allowing the richness of the data to shine through unimpeded by predefined themes.
Furthermore, to avoid bias from one of the researchers (ASN), who had already published an article on narratives of alcohol use, she did not partake in the process of coding but only in the discussion of the quotes the two researchers had extracted. After this, a meeting was held to discuss similarities and differences between the codes extracted by each researcher. Second, the descriptive statements were coded and grouped into four descriptive categories.
Stage 3
Lastly, the descriptive data synthesis was analyzed and prepared for presentation by characterizing the main narratives of the extracted literature. The characterization of the main narratives was conducted by keeping the purpose and the research question of the review in mind. Through this final process, we used decontextualized analysis to develop or retain the descriptive themes, so we had analytical categories and to answer our research question. This was achieved through a meeting with discussion, as Thomas and Harden (2008)) recommend in their process for a thematic synthesis.
Results
Drinking as a way to escape Thoughts
A substantial portion of the included articles (n = 18) contained narratives describing alcohol consumption as a way of coping with various troublesome thoughts that were difficult to articulate and get hold of.
A subset of the presented narratives (n = 12) explicitly pointed to alcohol use as a response to difficult intrusive thoughts. We found that these narratives described drinking as a strategy – whether conscious or unconscious – for managing complex or adverse thoughts that triggered a craving for alcohol (Hanpatchaiyakul et al., 2014; Hanpatchaiyakul et al., 2017).
In general, the narratives described that if something troublesome occupied the mind of the individual, a few drinks made it seem less bad (Orford et al., 2002). In a narrative presented by Inman & Kornegay (2004), the narrator that was quoted in the article reported being told by his/her GP that drinking was a kind of self-medication of problems. Smith (1998) found that feelings of guilt and shame were considered reasons for drinking alcohol as means to block one's mind. Three articles presented narratives where individuals struggled with ruminations that they would like to ease as they were considered as subject to worries. In such situations, alcohol was presented as a remedy. In one narrative a drink was used by the narrator to calm down (Choi et al., 2014); other studies introduced narrators who presented how drinking made the narrator stop thinking about a lot of things (Jennings, 2016; Orford et al., 2002; Jennings & Cronin-Davis, 2016). For example, an individual who was very self-conscious about his/her physical appearance, which was different to others (Inman & Kornegay, 2004), used the following words: Your main concern is getting that first drink, getting yourself sorted out. Without that drink you can’t face people, you can’t even speak. You shut yourself away… until you get this sort of Dutch courage to get you going. (Smith, 1998) […]Then I got out of the hospital after three days and swore I would never drink again. And within 2 weeks I was having wine again. I told myself it was just wine; it couldn't do any damage. So, yeah. And it just spiraled down, and I was very, very depressed, and constantly hopeless … I have emotional triggers that are problematic. (Hammer et al., 2012)
Similarly, in a narrative presented in Collins et al. (2018) the narrator described how alcohol was used to keep severe PTSD at a distance or aid for feeling depressed.
Other reasons for drinking covered “feeling out of place”, feeling worthless (Thurang & Bengtsson Tops, 2013) or isolated from social togetherness (McNair et al., 2016) and not being able to stand up for oneself (O'May et al., 2017), offering a “temporary fix” (Boyd & Mackey, 2000) and feeling lonely, as well as having no close friends to tell private matters to (Hanpatchaiyakul et al., 2014). In these conditions, alcohol served as a mitigating component for feeling comfortable with oneself. The individuals expressed how they felt more comfortable when drinking alcohol so as to have the power and openness to speak one's mind (Cunningham, 2012; Orford et al., 2002) adding to an individual’s self-confidence in the company of others (Emiliussen et al., 2017; Janes & Ames, 1989); Hammer et al., 2012). To some individuals, restrictive family traditions led them to drinking as to attain a more relaxed attitude (Kim et al., 2010) as opposed to being limited in words when sober (Choi et al., 2014).
Similarly, we identified narratives in the included studies, where the individual was aware of the negative influence alcohol had on him/her but nevertheless freely expressed how alcohol was used to disconnect from some situations: Although I can think a damn lot of thoughts and even though I know everything about how bad this is for me – I also know that I will always bring myself to situations where I need to disconnect. (Morck et al., 2020) The most important change, with supporting therapy, was the realization that all my self-destructive behavior from 14 on was associated with alcohol and that even if it was a result of other deep problems nothing would improve until I faced all of life without escape mechanisms. (Paris & Bradley, 2001) When my father died, I began to drink more; there's a saying, “alcohol makes you forget” and I would forget some of my suffering. (Puente et al., 2021) You can be in denial and can’t face what's going on, you just want to erase it. You don’t want to think about it. And the bottle just feels like it's your friend, that's what you’re coping with. That's your friend. You don’t want to face reality; you just want to be somewhere else. (Cook et al., 2016)
In some studies, periods of low mood were described by the informants to happen for no obvious reason, and alcohol was then an aid to feel better (Zakrzewski & Hector, 2004) or to unwind (Jennings, 2016). People may feel tired, sad (Christiansen et al., 2019), lack confidence, be frustrated, angry and worried, and sometimes all the feelings were tangled up, leaving the individual frustrated and in feelings of despair (Arai et al., 2014), and an urge may arise suddenly: Ohh yes, when I am tired or sad, anything really…not a lot of excuses…when you have that urge … just off with the cork. (Christiansen et al., 2019)
Similarly, in a study performed among people in the Peruvian highlands, the informants were reporting how problem drinking was linked to physical and psychological distress, life hardships and cultural practices. Collective drinking fostered social bonds, while alcohol was also used to cope with emotional pain and, in some cases, attributed to supernatural causes or interpersonal envy (Yamaguchi et al., 2023).
Drinking as rooted in the body, in the genes and in personality
A series of narratives that we identified in the studies, included descriptions of alcohol and alcohol problems as rooted in circumstances connected to somatic qualities. By utilizing the term “somatic”, we seek to separate statements that tangibly mention conditions related to the body even in figurative terms from statements that relate to the body in psychological terms.
In two papers, the individuals that was quoted, narrated alcohol as an appealing substance because they considered themselves predisposed to become addicts, just waiting for it to happen: It was like once I discovered that I felt different when I drank or used drugs, I wanted to feel that way all the time … but I was hooked on alcohol the minute I drank. It was always there
Or as expressed in another narrative: I was a chronic alcoholic from the time I took my first drink.
In some narratives, the alcohol problem was compared to a disease like heart failure and diabetes, and, since it was an illness, the narrator found it hard to overcome. The other side of the coin was that suffering from a disease was shameful; it was the disease that caused the trouble rather than the narrator's actions (Punzi & Tidefors, 2014). In another study, an individual was describing how it was the suffering from a disease that surprisingly explained his/her drinking behavior (Antunes de Campos & Narchi, 2022): … I had no idea that I was suffering from the disease of alcoholism; that because of this disease my life consisted only of trauma, only of defeat. I had blackouts; I couldn’t remember what I had done. (Antunes de Campos & Narchi, 2022).
Drinking as a reaction to a stressful situation
In eight of the included articles, the narrators described alcohol consumption as a response to specific and tangible life circumstances. These narratives pointed to identifiable external factors – such as work-related distress, physical pain, or states of exhaustion, and sexual abuse – that were perceived as directly triggering the drinking behavior. In these cases, alcohol was a reaction to concrete, situational pressures where alcohol served as an aid to the situation at hand.
In an article by Nielsen (2003), an individual explains his alcohol problem by describing drinking as a reaction partly to something psychological, partly to being divorced and fired, leading him, over time, to changing behavior (Nielsen, 2003). In the article, he described how he went from what he emphasizes as normal drinking behavior where he was able to cope with difficult or unpleasant challenges without the necessity to have a drink towards drinking excessively and in a needy way: I have never in my life needed a drink before going to work, neither when I was principal nor head, and no matter what problems that were in the air, even if they were unpleasant things. It was never a necessity, and it was never necessary. (Nielsen, 2003)
The identified narratives also included descriptions where the narrator focuses on his/her family relations or marriage problems as reasons for drinking (Arai et al., 2014; Choi et al., 2014), or the lack of parental attention during childhood. For example, Kim et al. (2010) present a narrative of an individual who explains how the lack of parents’ attention and love due to many siblings led to drinking to receive reactions from busy parents.
In another study, an individual expressed his/her marriage as a total disaster because of him/her having a hard time with feelings, another as having to marry a man because of pressure from surrounding family or because of being in a destructive relationship (Paris & Bradley, 2001), all the time thinking about how to escape from one's spouse and to turn to drinking (Hanpatchaiyakul et al., 2017).
Moreover, an article by Kim et al. (2010) contains a narrative where an individual uncovered how drinking full scale amplified feelings and allowed them to be released. The individual expressed idiosyncratic tendencies, considered to be stemming from unbearable life circumstances, when drinking alcohol: When I started drinking full scale, it seemed like my inside became at ease when I drank alcohol … I felt suffocated in my mind … and I liked it because I could cry out loud … cried by myself, talked by myself, when I was washing dishes in the sink … What are these for? … I broke dishes myself. I used to talk to myself a lot. With the power of alcohol, I poured out [the words], said things to my kids that I couldn’t before. Why am I getting this kind of treatment from my kids? … I got mad and lamented … cursing uncontrollably, saying; “Why did I even have [the kids]?” … like that … That makes me feel hurt … being ignored … I feel suffocated by my kids … That's why there's no satisfaction … I … getting married, ever since I got married I was insi-jip-sal-e (living with in-laws). My marriage, my husband, and my kids all fall below my expectations. Why is my fate like this? … When I find myself lamenting, that's when I look for alcohol. (Kim et al., 2010)
One study focused on individuals experiencing homelessness in Montreal and examined how alcohol use functioned as a coping mechanism for the challenges of street life. Participants described drinking in response to stressful life circumstances, including harsh environmental conditions, painful memories and experiences of social exclusion. Alcohol was used to manage both the physical and emotional burdens associated with their living conditions ( Motta-Ochoa et al., 2023).
Drinking as a cultural practice or habit
Twelve articles presented narratives describing how alcohol-related problems were culturally rooted. Note that we consider culture broadly in terms of cultural values such as tradition, norms, language, beliefs or symbolic character that belongs to a certain country or domain.
Eight articles presented narratives where the narrators found that their alcohol consumption intensified over time but for no specific reason. The individuals describe how their alcohol consumption initially might be considered a habit, but not a problem. It was merely part of fun moments feeling good and high (Nielsen, 2003), natural in the sense that the consumption was controllable and not a reason for worries (Hammer et al., 2012), or drinking as a natural part of daily life (Paris & Bradley, 2001). Over time, however, the individual became aware of the high level of drinking and how activities were planned around drinking; in one narrative, the escalation was related to when the individual began working by him/herself. Reasons for drinking habits were also described as rooted in cultural norms, originating in early life: I was raised in a family that at five o'clock it was cocktail hour – Every day – So, I didn't know it was weird to drink every day. I thought everyone did that, and all their friends, everybody […] Mm-hmm. And that was just normal – I really thought everyone had a cocktail at five. And when I think back, I think, well, [so and so]'s parents never did that – but all of my parents’ friends did. (Hammer et al., 2012)
Or as described in another narrative (Punzi & Tidefors, 2014), alcohol may have been part of the narrator's upbringing, something which marked celebration and always went with dinners and fine food. Or with the purpose of showing off: Serving alcohol at home, storing alcohol at home, and drinking alcohol is a way I show off. I want to let the world know that I have made it. (Nimmagadda, 1999) What am I going to do tonight? I don’t watch TV, there is only so much radio you can listen to, so many drawings you can do […] And the next minute, I’m getting together seven bucks to buy a cheap bottle. (Pienaar & Dilkes-Frayne, 2017) Something to look forward to … it cheers me up if I know I am going for a few pints, it cheers me up so it keeps me doing the chores better because I know … I suppose it's a reward if you like … And it gives me opportunity to talk to people … to get out as I live on my own, so it's nice to get out of the flat. (Puente et al., 2021)
In earlier days alcohol was to a greater extent than today part of everyday socializing at workplaces. In one article, we found narratives that date back in time yet may be relevant narratives to take into consideration for the purpose of understanding people's struggle of today. In an article from the late 1980s (Janes & Ames, 1989), individuals reveal how they had bottles of alcohol in their lockers, bottles in a box they sat on while working and going out at lunch and drinking. As one individual highlighted, they would come sober to work and get home drunk: I think it's the camaraderie that goes on in this type of atmosphere. You don't want to let go. There's safety in numbers. A lot of your buddies had problems drinking too, and it was something you always did together. (Janes & Ames, 1989) Oh yeah, I was thinking about changing my drinking, but then you hang around all these people, and it gives you the urge to drink. I got a lot of friends that drink. So, most of the people out there are just like me. (Clark et al., 2017)
Also, Eastern cultures were described as the foundation for developing drinking problems. In one study, an individual revealed how Thai tradition is known for offering employees alcohol for them to relax and be willing to work extra (Hanpatchaiyakul et al., 2017). Similarly, we found an example of how in Asian drinking culture it was perceived a man's right to drink alcohol as he pleased, because he worked hard every day: drinking was practiced after work with co-workers: Nu ambilai, enna venumanalum seiven [I am a man, and I can do whatever I want, drinking included] is society's sanction to drink. (Nimmagadda, 1999) Fate. Fate. Fate. That is what alcoholism is all about. Several of my friends also drink. It was meant to be me, and I am repaying some bad deeds I did in my previous life. Alcoholism means fate. (Nimmagadda, 1999).
Individuals narrated how pressure towards drinking often was established early in life because of societal expectations regarding drinking and socializing. Narratives about binge drinking and drinking until one cannot stand anymore were also found in Gray and Nosa (2009). In the same paper narratives revealed benefits from drinking were the ability to communicate more deeply, becoming much more flirtatious, loud, and boisterous (Gray & Nosa, 2009). The backside of the coin was how the social expectations might place pressure to the individual to fitting into the community or to gain acceptance by surrounding individuals (McNair et al., 2016).
The impact of social context was something that highly influenced the individual's prospect of failing to stay abstinent. Here expressed by an individual: What others around me are doing, of course it makes an impact … I wouldn’t feel comfortable sitting in a room … if they weren’t drinking and I was getting really drunk … so if people around me are drinking then I’m much, much more likely to drink. (Jennings, 2016)
Two narratives highlighted problematic circumstances faced by individuals associated with their sexual orientation. In one study, use of alcohol among bisexual individuals was studied and the narrators that were quoted in the study described how alcohol functioned as an aid in social situations, making the individual fit in in circumstances where anxiety is present, perhaps because of one's sexual orientation. Other themes covered in the narratives were social pressure, trying to keep up, staying out late and making the most of it, since there are relatively fewer gay and lesbian events, leading to higher expectation to participate and even get drunk: That was a really hard time, coming out at that age was difficult. I started drinking a lot and that, you know, I really got in full swing because it helped me with the difficulty, I felt in coming out … I didn’t come out in a very supportive situation … It [also] [ALCOHOL] helped me in social situations not to feel as anxious as I did, and it helped me to fit in. (McNair et al., 2016)
In a paper from Denmark, alcohol was associated with the term ‘hygge’ (coziness) when relaxing and enjoying oneself or together with friends (Emiliussen et al., 2017) and how this formed the starting point for developing alcohol problems. Three additional papers covered narratives where alcohol was a genuine pleasure and where individuals straightforwardly admitted how they love drinking and liked the feeling of being drunk and high (Cook et al., 2016). In the study by Eriksen and Hoeck (2022) Well, it is kind of … I won’t say disclaiming, but it really is very pleasant to be intoxicated – it really is […] and you sit on a bench in the sunshine and chat and – well, you can call it escapism, in a way that is what it really is. (Eriksen & Hoeck, 2022)
Discussion
The aim of present scoping review was to present personal narratives concerning alcohol-related alcohol problems identified and quoted in the health-scientific literature. The narratives found could be grouped under four headings or as illustrating four master narratives.
The first group was “Drinking as a way of coping with difficult thoughts” in which alcohol consumption was frequently portrayed as a way to cope with, complex or adverse thoughts. Many individuals described drinking not in relation to specific events, but as a response to difficult circumstances which they struggled to articulate. In the second group of narratives, named “Drinking as rooted in the body, in the genes and in the personality”, the identified narratives linked alcohol-related problems to somatic factors, such as genetic predisposition or addictive personality traits. In this group, the quoted individuals described their drinking as inevitable or disease-like, framing addiction as rooted in bodily conditions. By framing their drinking in terms of disease-like features, they could distance themselves from aspects of personal blame but we still found that feelings of shame were present in the narratives. In the third group of narratives identified in the literature, “Drinking as a reaction to a stressful situation”, drinking problems was described as a direct response to a certain external stressor – such as high workload, physical pain, or trauma – rather than to vague life circumstances as such. These narratives highlighted drinking as a reaction to tangible, situational challenges affecting the body or mind in immediate ways. Lastly in “Drinking as a cultural practice or habit”, drinking problems were described as culturally rooted, tied to norms, traditions and daily habits where individuals recount how drinking gradually intensified over time, initially seen as harmless or social, but later recognized as problematic and shaped by cultural expectations from early life.
Individual trajectories of illness or behavior change are not generated sui generis but constructed on the basis of existing narrative “maps” (Polner & Stein, 1996; Weegmann & Piwowoz-Hjort, 2009) and, beyond the uniqueness of the narratives presented by the individual, certain patterns can be discerned which represent more general styles of self-identification, a shared vocabulary and ways of talking about alcohol dependence and recovery. These patterns often draw on culturally available “master narratives” or “masterplots”, comprising dominant story structures within a culture that offer skeletal narrative frames for individuals’ sense-making, which are then fleshed out in particular storytelling instances (Abbot, 2008). While these frameworks can aid narrative coherence, they may also limit or constrain individual expression (Bamberg & Andrews, 2004).
Some of these patterns may stem from Alcoholics Anonymous (AA) story models (Steffen, 1997; Weegmann & Piwowoz-Hjort, 2009) and others may stem from treatment modalities such as cognitive behavioral therapy (Beck et al., 1993), and yet again others may stem from the literature or the media. Hence, individuals may be seen as “theorists of their own life” who use existing literature and other types of frameworks as a guide for understanding their problems in the same way as researchers, who test and modify existing theories or create new ones on the basis of their data (Hanninen & Koski-Jannes, 1999).
Experiences are the human conduit for affiliation, and the narratives presented in the present study may seem disorderly and in disagreement with one another. As noted by Hammer et al. (2012), this may be an important aspect of alcohol addiction that should not be glossed over in favour of a unified framework: “Addiction is not just the disease of one particular organ, not just the result of an unfortunate upbringing, or an unfortunate choice; addiction is not the affliction of, or, what is ‘the matter’ with the ill other, addiction is a matter with us”.
The diversity of addiction narratives is now and will always be myriad and infinite. They are told by individuals, and, when being told, they draw on the cultural structure, biases and storylines from the society in which the individual is brought up and lives. Treatment centres and self-help groups employ their own dominant narratives in explaining addiction and the individuals’ framework for understanding addiction is shaped by the language and ideology of their treatment and self-help milieu (Andersen, 2015; Hammer et al., 2012), just as it is shaped by the narratives presented in the literature (Warhol, 2002), films (Carota & Calabrese, 2013) and the mass media (Hellman & Room, 2015). Furthermore, in the present study, the identified narratives represent the subset of narratives that the original researchers chose to present in their published articles.
This discussion points to the tensions involved in navigating between the heterogeneity and unruliness of personal experiences and the commonalities that are grouped into recognizable patterns. For example, health professionals must constantly attend both to the individual story and to broader thematic consistency. This tension invites reflection on – and perhaps an explicit argument for – the value of identifying and understanding common patterns in addiction narratives.
While we often want doctors and professionals to listen carefully to everyone's story, listening for patterns can help them become more attuned to the kinds of cultural or social narratives, including stereotypes that patients may be drawing on to frame their own experiences. Being explicit about this dual responsibility – honoring individual stories while recognizing shared frameworks – may offer insight into how addiction is understood and treated across different contexts.
The understanding of the ways patients think and feel about their suffering and treatment is often missing from research in the field of addiction (Donovan & Blake, 1992). By combining research methods, we stand a better chance of unravelling the complex relationship between meaning and action. With this knowledge, we might stand in a better position to address substantive questions; for example, why some individuals change and why some individuals show better compliance in specific treatment modalities than others. Furthermore, since individuals draw on their cultural background when they narrate on their drinking habits, we may as researchers be in an even better position if we can manage not only to combine research methods, but also to build a bridge between studies in culture and fictional literature and clinical studies in the fields of addiction.
The present review focused on the patterns in the narratives presented and quoted in health-scientific literature. It became apparent from our research that most of the identified studies were based on narratives and accounts from participants enrolled in treatment for alcohol-related problems. Relatively few participants in the studies identified were recruited from the non-treatment seeking population. There were an equal number of studies that paid attention to female and male accounts respectively (11 exclusively with female and 11 exclusively with male informants out of the 42 studies).
Limitations and strengths
To our knowledge, the present review is the first attempt to systematically identify and describe patterns in personal narratives about alcohol use turning into problematic use that has been presented in scientific literature. It can be considered a limitation to the review that our search found all but one of our core articles, namely Nielsen (2003). This could indicate that our search string is not characterized by the degree of sensitivity we wished it to have. This may also be a matter of the following two issues.
The first issue is qualitative research status in bibliographic databases. As Shaw et al. (2004; p. 1) points out, “[…] qualitative research […] is often difficult to find”. Furthermore, according to Evans (2002; p. 22–26), “[…] there is little information on the accuracy of the indexing of qualitative research and that qualitative research has not to the same degree as quantitative research been a part of a larger systematization of index terms” (Shaw et al., 2004). It may be relevant to point out the large degree of heterogeneity in both theory, terms and methods used in qualitative research (Tracy, 2010), which may also represent a hindrance in the systematization of qualitative research in databases.
The second issue is that there may also have been a historical development in the specific set of terms used in the consideration of narratives. For example, Nielsen (2003) uses MeSH terms such as “Patient Compliance” and “Self-Assessment” that a qualitative article revolving around the stories that alcohol users tell perhaps would not use to index or describe their research today (Nielsen, 2003). This is a vital point about this review's searches and included articles to consider as this may point out that we may have missed relevant articles.
Because of these two issues, we point to the need for a larger discussion on how qualitative research in general – and more specifically, research into narratives and stories of individuals – can be indexed and systematically found through different types of reviews and perhaps argue that qualitative research needs to undergo the same rapid progress such as quantitative study designs have in bibliographic databases (Shaw et al., 2004).
Another limitation is that we have “sorted” all articles by hand, albeit through covidence, but it allows for human errors. For example, we did not get any articles about AA, and, although such studies may often be about recovery, they may have included parts or reasonings about why individuals drink. We conducted secondhand interpretations of quotes where the quotes were already subject to selection by the authors, respectively
Conclusions
In the scientific literature, we can identify four master stories about development of drinking problems: “Drinking as a way of coping with different emotions”, “Drinking as rooted in the body, in the genes and in the personality”, “Drinking as a reaction to a stressful life circumstances” and “Drinking as a cultural practice or habit”. Each narrative suggests a distinct therapeutic focus, from emotion regulation and trauma-informed care to psychoeducation, stress management and culturally sensitive interventions. By aligning treatment with how individuals understand their own drinking, practitioners can foster greater engagement and reduce stigma. These insights also support the education of healthcare professionals, enhancing their ability to respond empathetically to diverse experiences of addiction. Ultimately, integrating these perspectives can lead to more personalized and meaningful recovery pathways.
Footnotes
Ethical considerations
Due to the nature of the review, ethical clearing and patient consent for publication is not required.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Appendix 1
Appendix 2