
Abstract
Background:
A substantial number of thyroid surgeries are performed annually, and most patients are of working age. Research on the impact of thyroid surgery on patient quality of life (QoL) remains limited. This study evaluated changes in QoL within 1 year after thyroid surgery and identified risk factors for poor postoperative QoL. The prevalence of depressive symptoms and their association with QoL outcomes were examined.
Methods:
A prospective cohort study including all consecutive patients (n = 314) who underwent lobectomy or total thyroidectomy at Oulu University Hospital in Finland between September 2021 and December 2022. QoL was assessed using the RAND-36 questionnaire, and depressive symptoms were measured with the Beck Depression Inventory (BDI) before surgery and at 6 and 12 months postoperatively. Poor QoL was defined as a RAND-36 score more than two standard deviations below the age-adjusted population mean.
Results:
Overall QoL improved, particularly in mental well-being, but remained below the Finnish population norms across all domains in patients with complete QoL data across all time points (n = 143). Preoperative depressive symptoms were present in 42% of patients who completed the baseline BDI questionnaire (n = 162). Among these patients, QoL improved in the same domains but remained below the baseline level of the overall cohort. At 12 months (n = 157), 64% of patients had good QoL and 36% had poor QoL. In multivariable analysis, female gender, poor baseline QoL, and preoperative depressive symptoms independently predicted poor QoL at 12 months.
Conclusion:
Thyroid surgery improves QoL over 12 months, especially in mental health, but remains below the general population. Depressive symptoms are common and predict worse recovery, indicating that patients may benefit from preoperative psychological assessment and support.
Clinical trial registration
N/A.
Context and Relevance
Previous studies have shown that thyroid surgery can improve quality of life (QoL), particularly in benign conditions, but evidence on long-term outcomes and the impact of depressive symptoms is limited. In this prospective study of Finnish patients, a significant improvement in QoL, especially in domains related to psychological well-being, was observed at 12-month follow-up, although overall QoL remained lower than in the general Finnish population. Depressive symptoms were highly prevalent among patients undergoing thyroid surgery, and their presence independently predicted poorer postoperative QoL, highlighting the importance of psychological assessment and support in optimizing recovery after thyroid surgery.
Introduction
In Finland, about 2500 thyroid surgeries are performed each year, 1 which is a relatively high number given the country’s population of about 5.6 million people. The primary causes for surgery include confirmed or suspected thyroid cancer, hyperthyroidism, and goiter. Out of these, the indication for surgery in goiter is relative, as the operation is primarily performed to alleviate symptoms and improve quality of life (QoL). Most patients undergoing surgery are of working age. Despite the high frequency of thyroid surgery, there is a paucity of research on how these procedures affect patient QoL, particularly among those with a relative indication for surgery.
Previous studies have indicated that overall QoL tends to improve after thyroid surgery. 2 In patients with goiter, disease-specific QoL seems to improve after surgery.3 –5 Among patients with hyperthyroidism who have been treated medically to achieve euthyroidism before surgery, QoL has also been reported to improve after surgery.6,7 For patients undergoing surgery for thyroid cancer, there is a temporary decline in QoL immediately after surgery. Long-term follow-up, however, shows that QoL eventually surpasses baseline levels within 5 years. 8 Patients who undergo a lobectomy instead of total thyroidectomy are reported to experience better postoperative QoL. This improvement is especially clear among those who do not need thyroid hormone replacement therapy after surgery, as their QoL surpasses that of patients who require lifelong hormone therapy. 9
In a previous study by the authors, it was found that patients undergoing thyroid surgery had a lower QoL compared with the general Finnish population. Factors associated with impaired QoL included age under 65 years, a Beck Depression Inventory (BDI) score above 9, regular shortness of breath, higher Voice Handicap Index (VHI) scores, and a higher body mass index (BMI). There was no difference in preoperative QoL between patients operated for cancer, goiter, or hyperthyroidism. 10
The aim of this study was to evaluate whether patient general QoL improves during a 12-month follow-up after thyroid surgery, including those operated on with lobectomy and total thyroidectomy. It was hypothesized that QoL would improve postoperatively. In addition, to identify potential risk factors associated with poor postoperative QoL at 12 months. The prevalence of depressive symptoms in this patient population was examined with the aim to assess whether changes in QoL over time differed between patients with and without preoperative depressive symptoms.
Methods
Patient cohort and QoL instruments
This prospective follow-up study was approved by the Ethical Committee of the Northern Ostrobothnia Hospital District (number 43/2021). Patients who underwent either total thyroidectomy or lobectomy at Oulu University Hospital in Finland between September 2021 and December 2022 were recruited. Participants provided written informed consent for the study. During this period, a total of 314 patients underwent surgery. Patient health-related data were collected from electronic medical records, including surgical and anesthetic reports, as well as laboratory information systems. The data were analyzed using SPSS software (IBM Corp., IBM SPSS Statistics for Windows, Version 27.0, Armonk, NY, USA). Sample sizes were not calculated due to the observational cohort study design.
General QoL was evaluated using the RAND-36 questionnaire, 11 which patients completed before surgery after their preoperative outpatient visit and again at 6 and 12 months after surgery. Depressive symptoms were measured with the BDI 12 also administered after the preoperative outpatient visit and at 6 and 12 months after surgery.
The RAND-36 is a widely used tool internationally for measuring general health-related quality of life (HRQoL). It includes 36 questions across eight domains: four assessing physical health (physical functioning, role limitations due to physical health issues, pain, and general health) and four assessing mental well-being (vitality, social functioning, emotional well-being, and role limitations caused by emotional health problems). Each domain is scored from 0 to 100, with 100 indicating the best possible QoL. 11 A validated Finnish version of the questionnaire and age-adjusted reference values for the Finnish population are available. 13 Consistent with previous research, poor QoL was defined as a score more than two standard deviations below the age-adjusted reference value in any domain.14 –16
The BDI is a commonly used 21-item questionnaire that measures the severity of depressive symptoms. For each item, patients choose one of four statements that best describe their experience. Scores of 10–16 indicate mild depression, 17–29 suggest moderate depression, and scores of 30 or above represent severe depression. 12
Analyses
In the first analysis, patient characteristics between responders and non-responders to the 12-month RAND-36 questionnaire were compared (Table 1). Next, changes in QoL at 6 and 12 months after surgery were assessed and compared with baseline. For this analysis, patients who had completed the RAND-36 at all three time points, that is, at baseline and 6 and 12 months after surgery, were included. In the third analysis, the subgroup of patients who completed the preoperative BDI questionnaire (Table 4) was examined. Changes in QoL 12 months after surgery among patients with preoperative depressive symptoms were then assessed. This analysis included patients with a baseline BDI score greater than 9 who had also completed the RAND-36 at both baseline and 12 months after surgery. Finally, the subgroup of patients who completed the RAND-36 QoL questionnaire at the 12-month follow-up (Table 6) was analyzed.
Characteristics of responders and non-responders at 12-month follow-up.
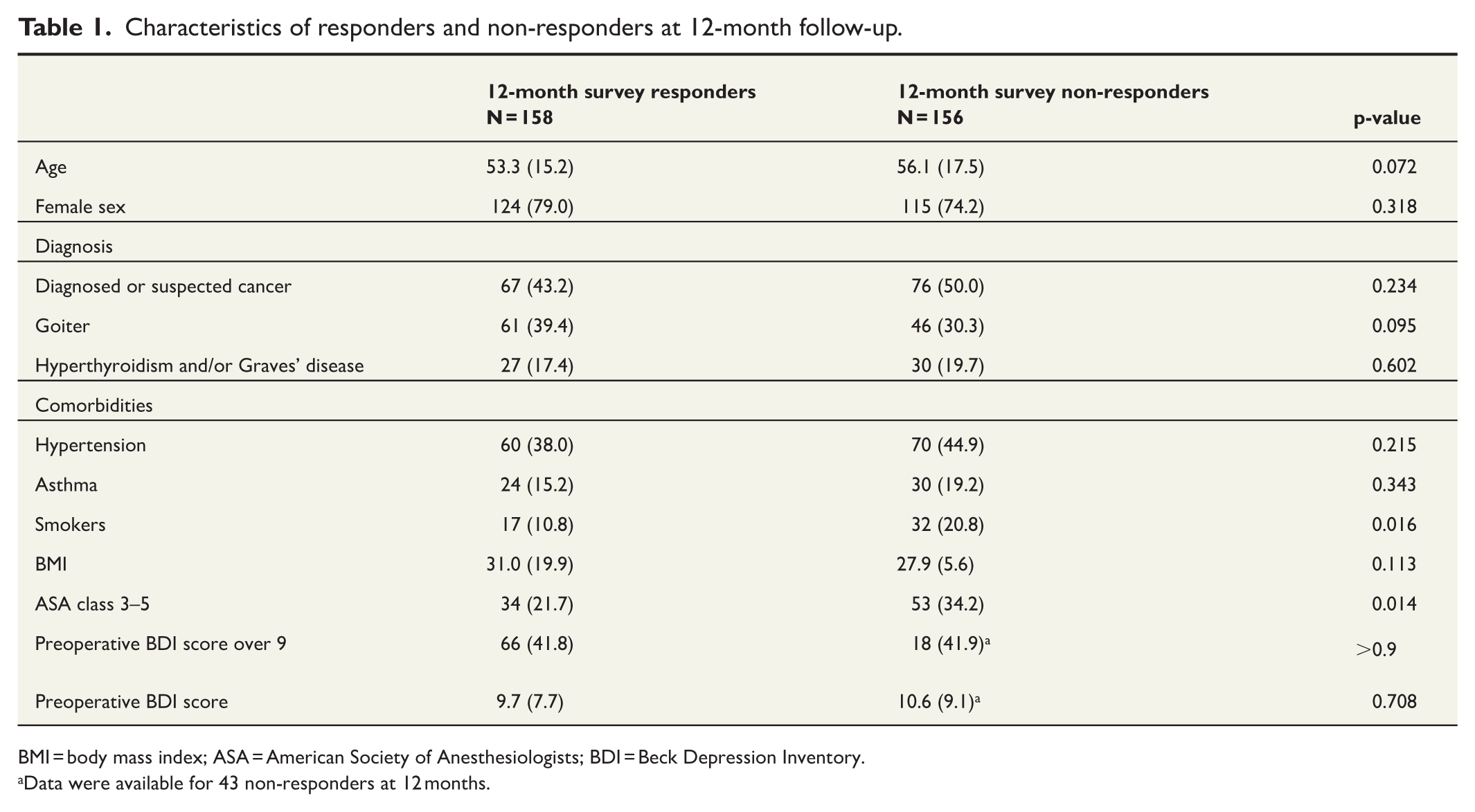
BMI = body mass index; ASA = American Society of Anesthesiologists; BDI = Beck Depression Inventory.
Data were available for 43 non-responders at 12 months.
Statistics
Continuous variables were analyzed using the non-parametric Mann–Whitney U test, and categorical variables using either the Pearson chi-square test or Fisher’s exact test, as appropriate. Differences in RAND-36 scores between baseline, 6-month, and 12-month surveys were analyzed using the paired samples t-test. Continuous variables are presented as means with standard deviations (SDs), and categorical variables are shown as counts (n) and percentages (%). All p-values are two-sided.
Logistic regression models were used to calculate odds ratios (ORs) and 95% confidence intervals (CIs) for poor QoL at 12 months. Variables considered clinically relevant and those with a univariable p-value < 0.1 were included in the multivariable model using the enter method. Only variables with a multivariable p-value < 0.05 or those that significantly influenced the log-likelihood function were retained in the final model (Table 7).
Results
Comparison of responders and non-responders
During the study period, a total of 314 patients underwent thyroid surgery. Of these, 204 patients (65%) completed the preoperative survey and 158 (50%) responded to the 12-month follow-up survey. Smokers and patients with an American Society of Anesthesiologists (ASA) class above 2 were less likely to respond to the 12-month survey. No other differences in patient characteristics were observed between respondents and non-respondents, including in the proportion of patients with preoperative depressive symptoms or based on preoperative BDI scores (Table 1).
QoL after thyroid surgery
Compared to baseline, patient QoL improved at 6 months after surgery in four RAND-36 subscales: Physical Functioning, Energy/Fatigue, Emotional Well-Being, and Social Functioning. At the 12-month follow-up, Physical Functioning was no longer significantly improved compared to baseline, but Role Limitations Due to Physical Health showed a statistically significant improvement. Energy/Fatigue, Emotional Well-Being, and Social Functioning remained significantly improved at 12 months. No significant postoperative improvements were observed in Role Limitations Due to Emotional Problems, Pain, or General Health. Even after surgery, patient QoL remained lower than that of the general Finnish population across all RAND-36 subscales (Tables 2 and 3, Fig. 1).
RAND-36 at baseline and the 6-month follow-up.
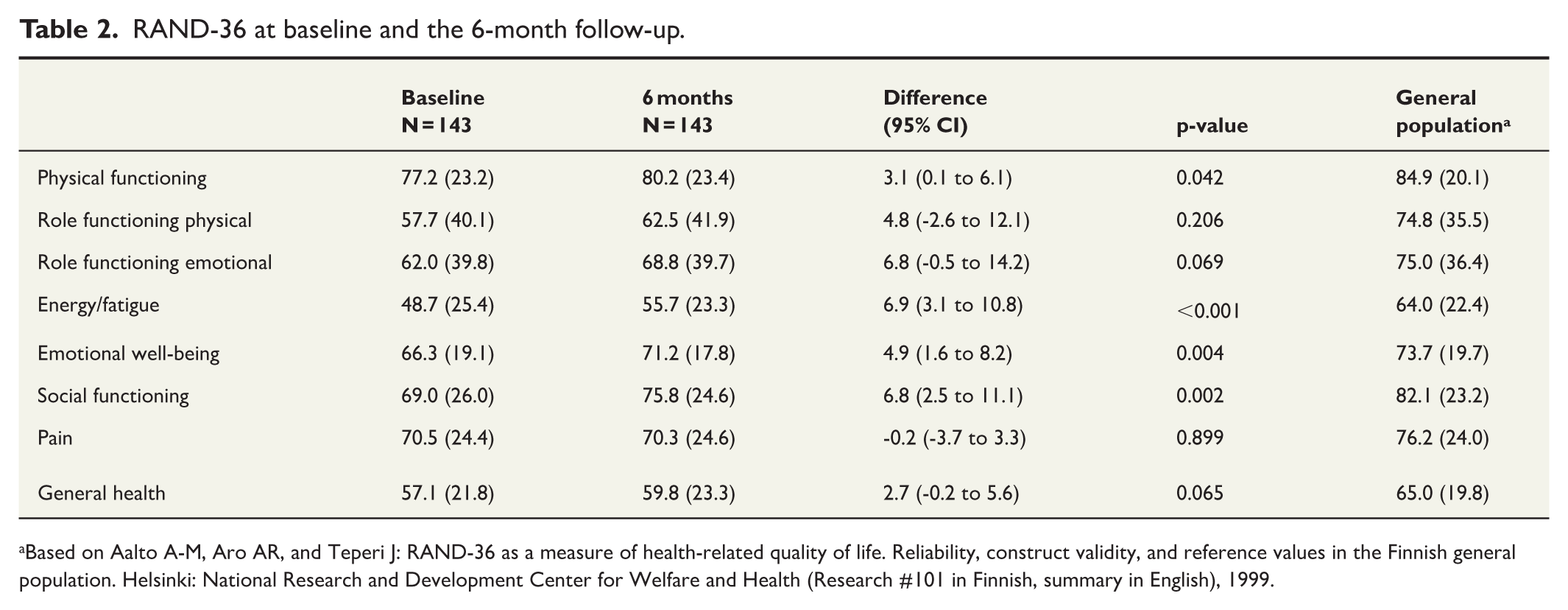
Based on Aalto A-M, Aro AR, and Teperi J: RAND-36 as a measure of health-related quality of life. Reliability, construct validity, and reference values in the Finnish general population. Helsinki: National Research and Development Center for Welfare and Health (Research #101 in Finnish, summary in English), 1999.
RAND-36 at baseline and the 12-month follow-up.
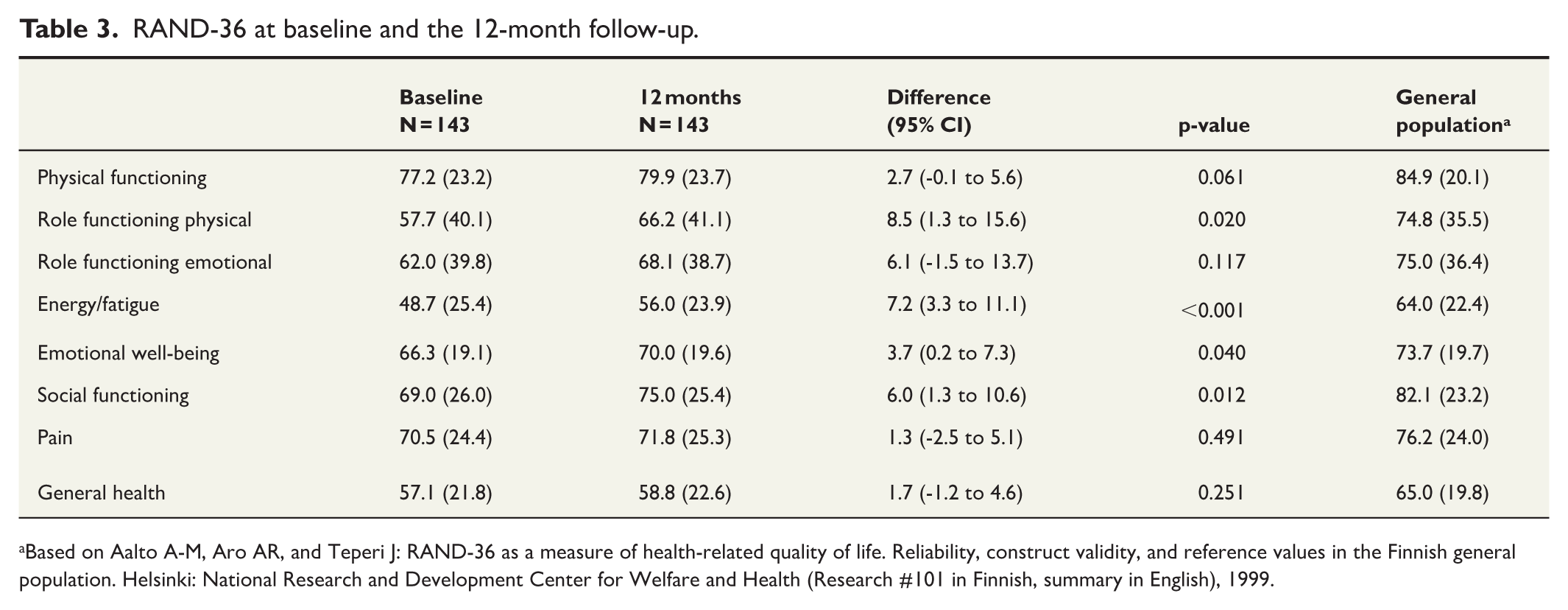
Based on Aalto A-M, Aro AR, and Teperi J: RAND-36 as a measure of health-related quality of life. Reliability, construct validity, and reference values in the Finnish general population. Helsinki: National Research and Development Center for Welfare and Health (Research #101 in Finnish, summary in English), 1999.
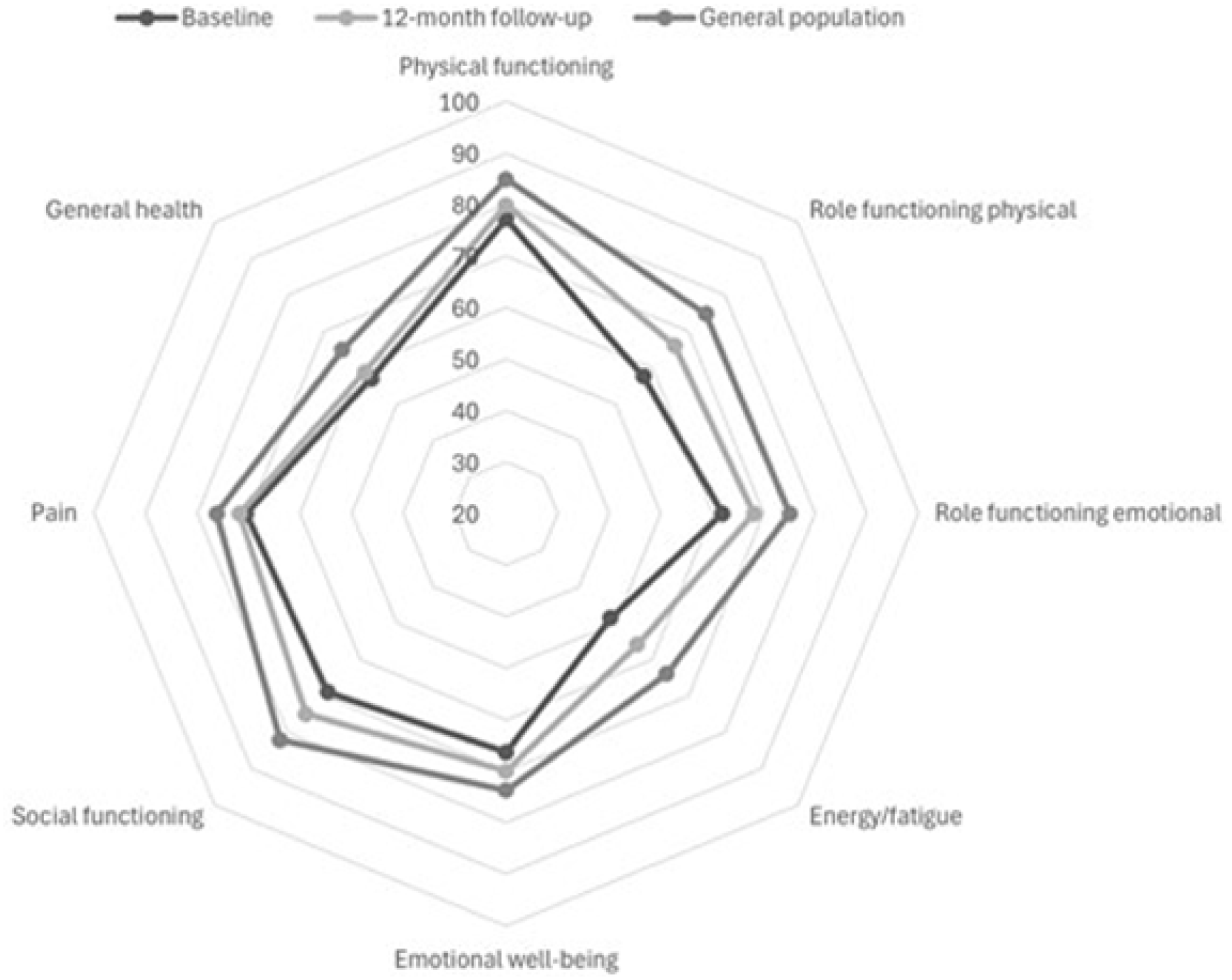
Radar chart of RAND-36 scores at baseline and at the 12-month follow-up, compared with the general Finnish population.
Depressive symptoms among patients undergoing thyroid surgery
At baseline, 68 patients (42%) exhibited depressive symptoms. There were no significant differences in age or sex distribution between patients with and without depressive symptoms. Similarly, the indication for surgery, whether being for cancer, goiter, or hyperthyroidism/Graves’ disease, was not associated with the prevalence of preoperative depressive symptoms. Patients with depressive symptoms, however, more often had other comorbidities, as reflected by a higher ASA class (ASA 3–5). Among those with depressive symptoms at baseline, 57% still reported such symptoms at 6 months and 66% at 12 months after surgery. Preoperative hypothyroidism was also associated with a higher prevalence of depressive symptoms (Table 4).
Characteristics of patients with and without depressive symptoms at baseline.
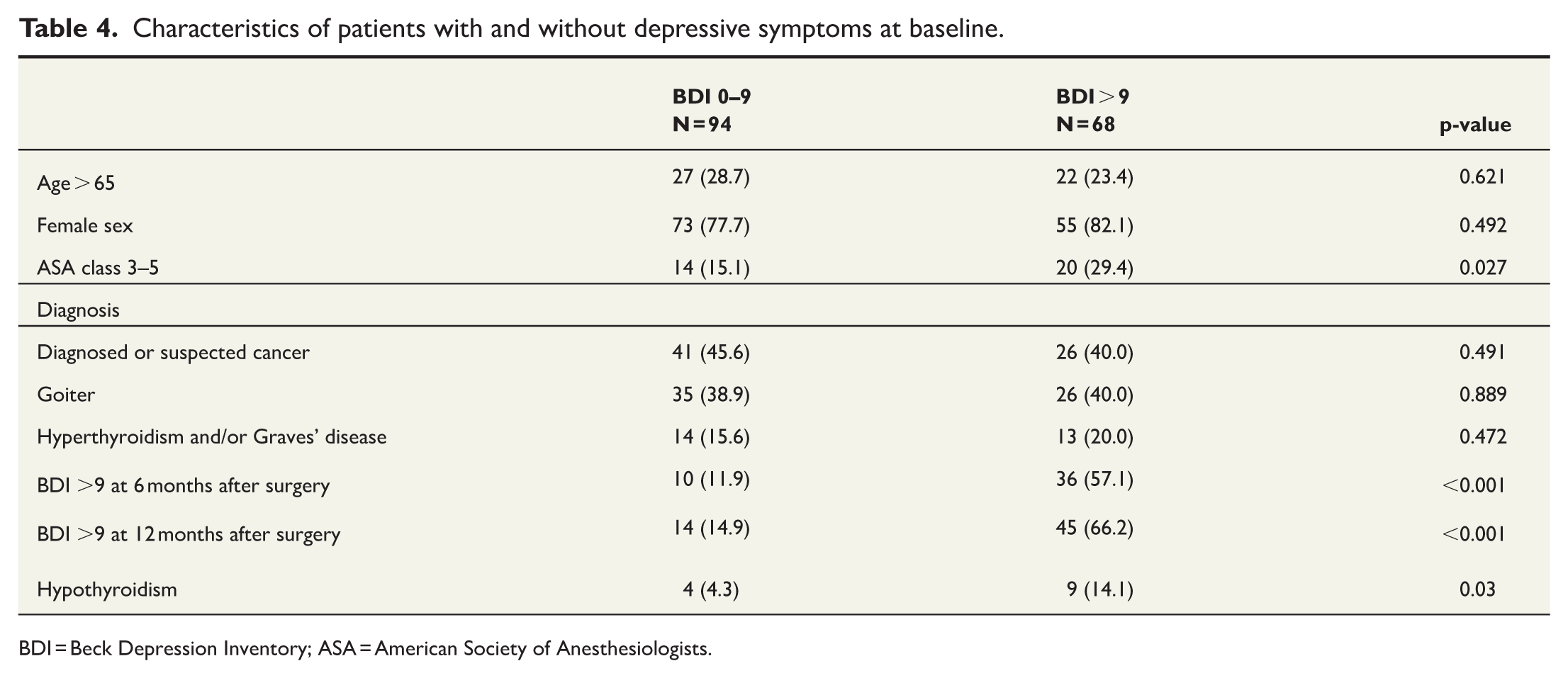
BDI = Beck Depression Inventory; ASA = American Society of Anesthesiologists.
When examining changes in QoL among patients with depressive symptoms at baseline, a statistically significant improvement at the 12-month follow-up was observed in the same four RAND-36 subscales as in the overall cohort: Role Limitations Due to Physical Health, Energy/Fatigue, Emotional Well-Being, and Social Functioning. Notably, patients who had depressive symptoms preoperatively scored significantly lower across all RAND-36 subscales compared to the overall cohort, and their QoL remained below the baseline level of the total cohort even at the 12-month follow-up (Table 5 and Fig. 2).
RAND-36 scores at baseline and the 12-month follow-up for patients with preoperative depressive symptoms.
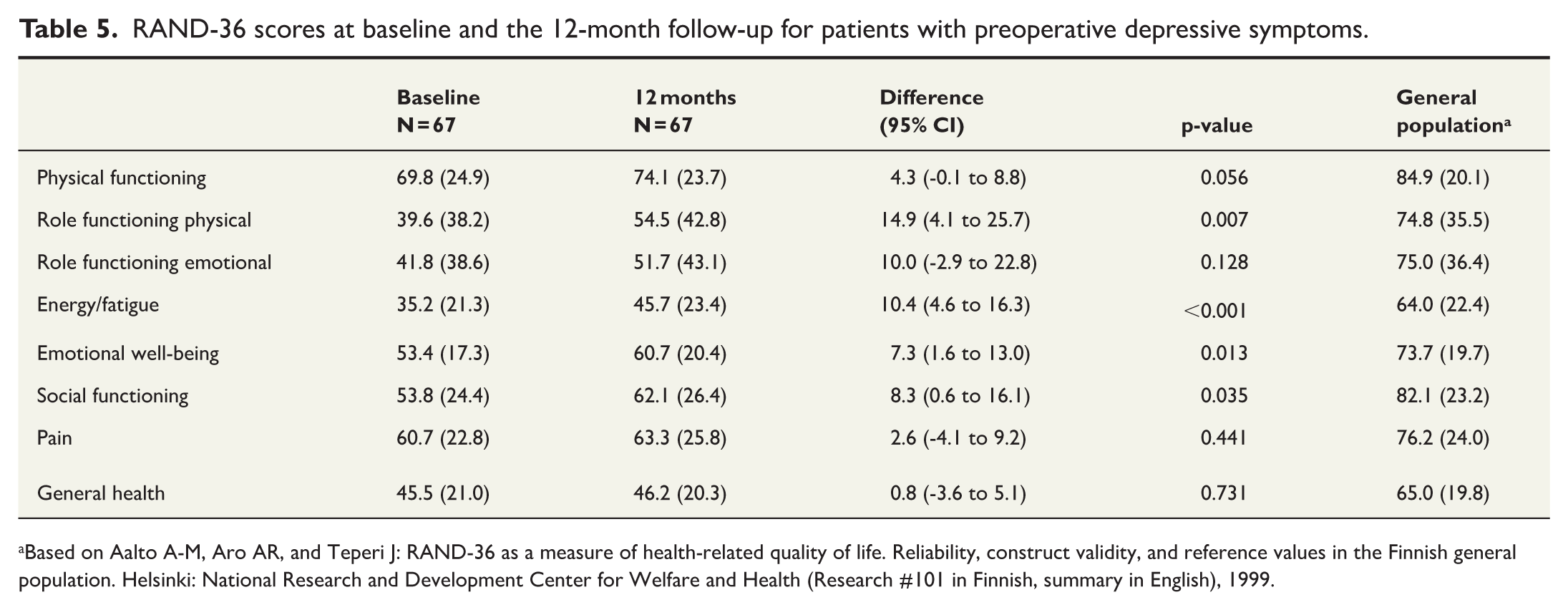
Based on Aalto A-M, Aro AR, and Teperi J: RAND-36 as a measure of health-related quality of life. Reliability, construct validity, and reference values in the Finnish general population. Helsinki: National Research and Development Center for Welfare and Health (Research #101 in Finnish, summary in English), 1999.
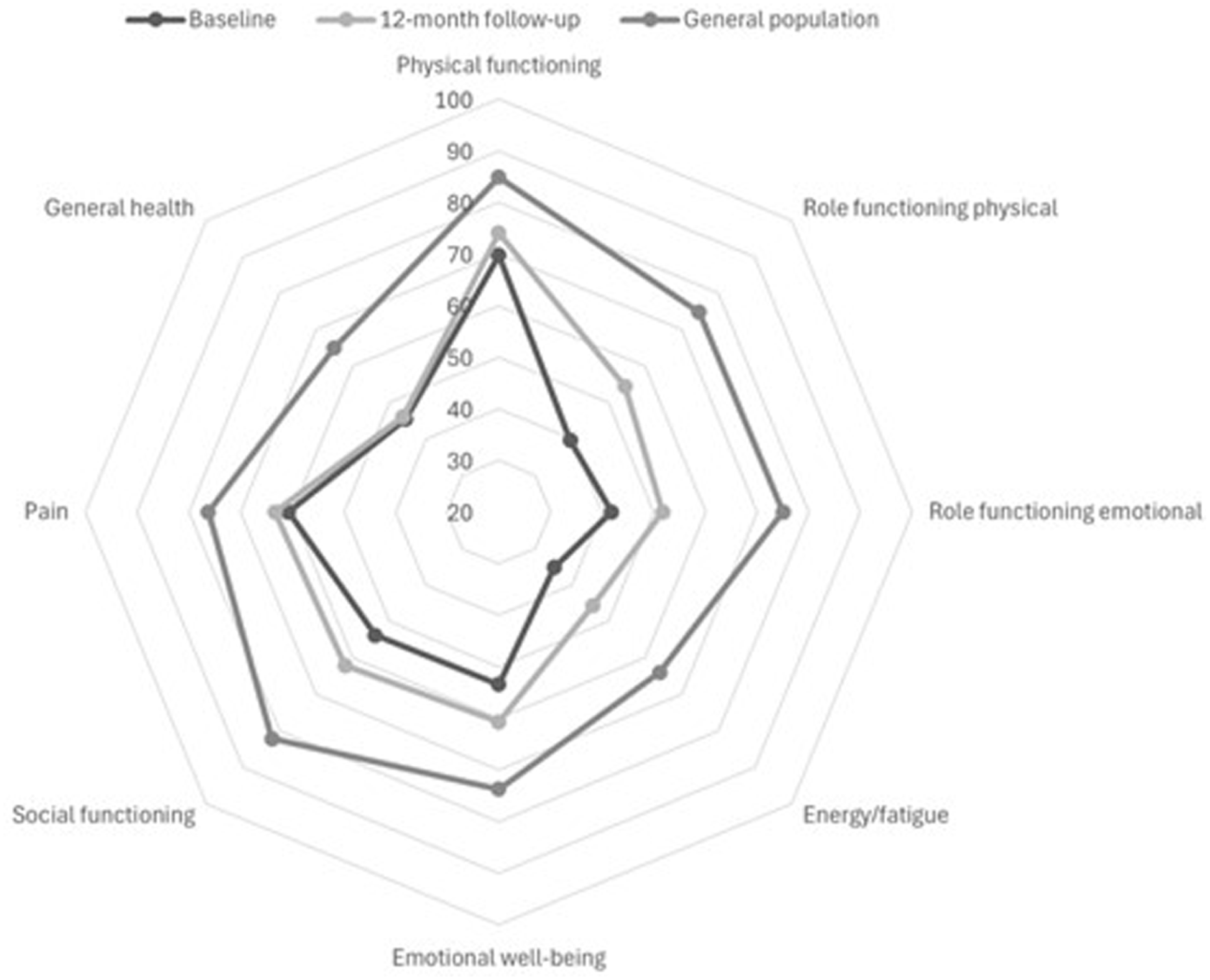
Radar chart of RAND-36 scores at baseline and at the 12-month follow-up for patients with depressive symptoms at study onset, compared with the general Finnish population.
QoL at 12 months after thyroid surgery
At 12 months after thyroid surgery, general QoL was rated as good in 100 patients (64%) and poor in 57 patients (36%). No significant differences in age or sex were observed between these groups. The indication for surgery, whether due to suspected malignancy or other indications, did not influence postoperative QoL. Among comorbidities, only asthma was associated with lower QoL at the 12-month follow-up, while other comorbid conditions showed no significant association (Table 6). In contrast, patients who reported poor QoL and symptoms of depression before surgery were significantly more likely to experience poor QoL at 12 months after surgery. A baseline BDI score over 9, suggestive of depression, was also associated with worse postoperative QoL. Similarly, patients with poor QoL at 12 months had higher BDI scores compared to those with good QoL (Table 6).
Characteristics of patients with good or poor QoL at the 12-month follow-up.
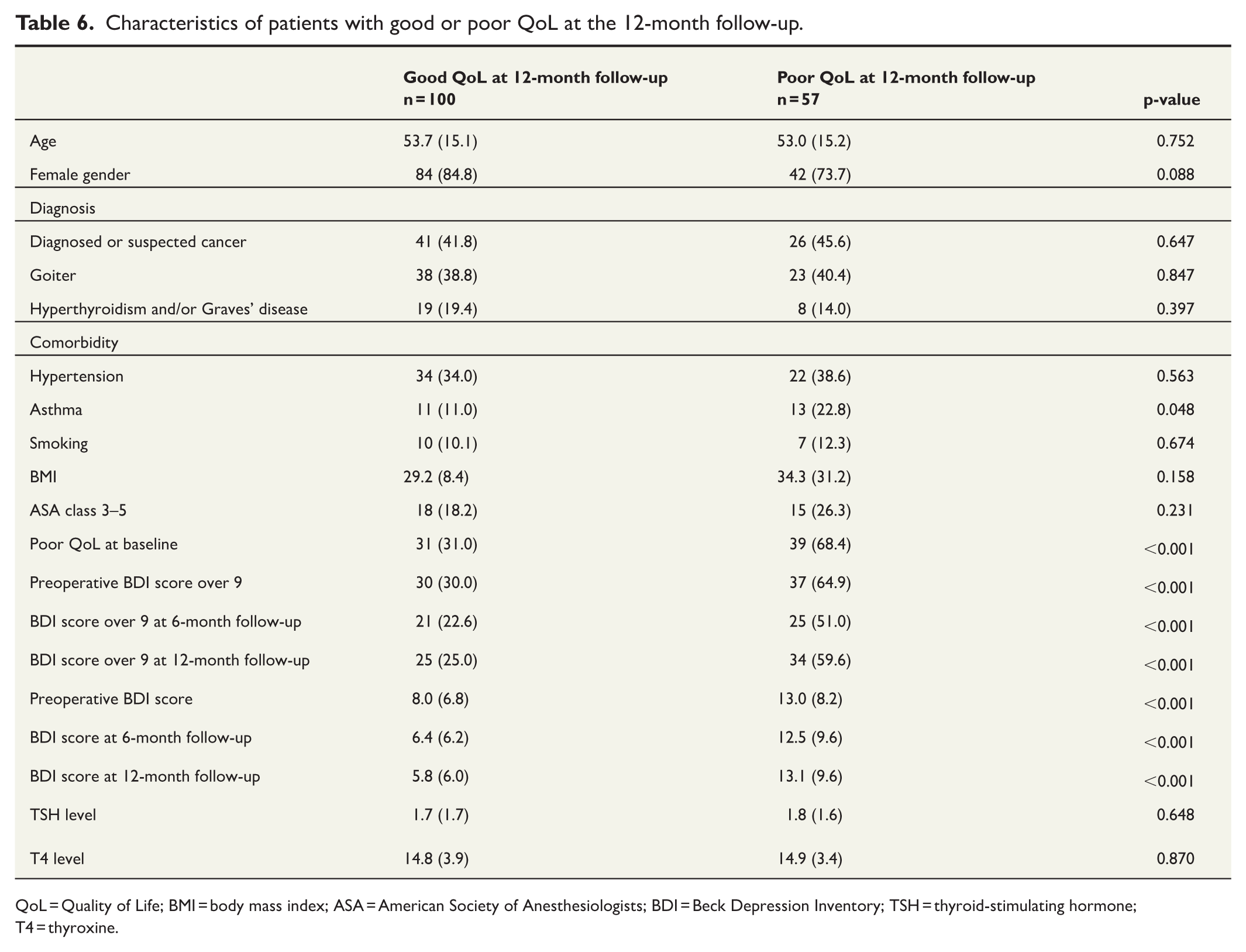
QoL = Quality of Life; BMI = body mass index; ASA = American Society of Anesthesiologists; BDI = Beck Depression Inventory; TSH = thyroid-stimulating hormone; T4 = thyroxine.
In the multivariable model, female sex, poor baseline QoL, and the presence of depressive symptoms at baseline were independently associated with poor QoL at 12 months after surgery (Table 7).
Poor QoL after 12-month follow-up.
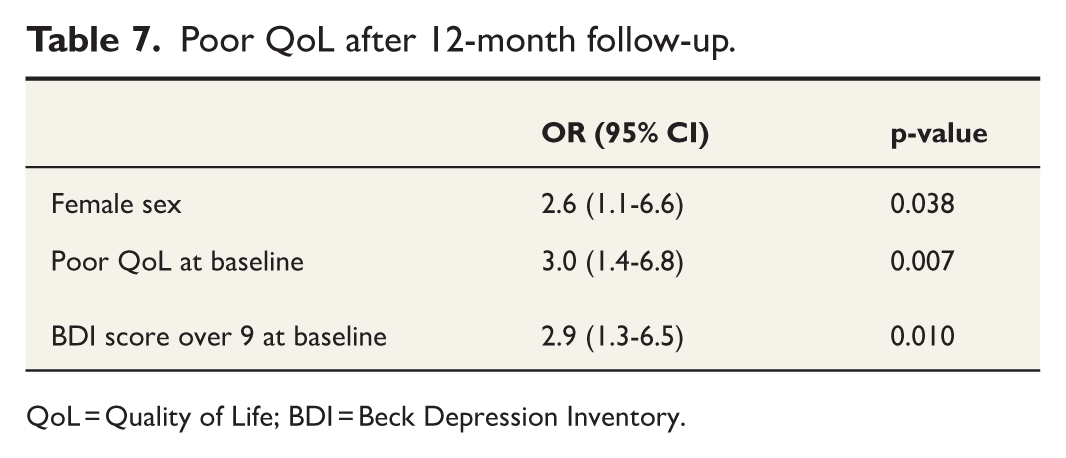
QoL = Quality of Life; BDI = Beck Depression Inventory.
Discussion
The main findings of this study show that general QoL improves during the 12-month follow-up after thyroid surgery, with the most notable improvements seen in areas related to psychological well-being. Among patients who had depressive symptoms at baseline, QoL improved more markedly in these same areas compared to other patients; however, their QoL still remained lower at 12 months than the initial level of the overall group.
Despite these improvements, patients who underwent thyroid surgery still reported lower QoL 12 months after the operation compared with the general Finnish population. Moreover, although the improvements were statistically significant, the absolute difference was rather small but nevertheless close to 5 points, which has been considered clinically meaningful. The largest numerical improvements were observed in role functioning physical scores, and this effect was further emphasized in patients who reported preoperative depressive symptoms.
Female sex, poor baseline QoL, and the presence of depressive symptoms at baseline were all associated with lower QoL at the 12-month follow-up. These findings may partly reflect underlying psychosocial factors rather than surgery-specific effects alone. In addition, the mean age of the study population was approximately 53 years, and thus, the observed differences may also be influenced by sex-related physiological changes occurring in midlife, including those related to the menopausal transition and the potential use of hormone replacement therapy. 17
Recent prospective cohorts have shown that QoL generally improves after thyroid surgery, but recovery is domain-specific: psychosocial dimensions (energy, emotional well-being, social functioning) tend to improve more consistently than pain, general health perceptions, or physical role limitations.18,19 This pattern closely matches the present RAND-36 results, where the most notable gains occurred in energy/fatigue, emotional well-being, and social functioning, while pain and general health changed little. Consistent with these findings, Winter et al. 18 reported that although QoL improved postoperatively, several domains remained below population reference norms, supporting the presence of persistent impairment relative to the Finnish reference population.
Thyroid-specific patient-reported outcome measure (PROM) and survivorship-focused studies similarly indicate postoperative improvements in symptom and psychosocial domains, yet a substantial subgroup reports an ongoing psychological burden.20 –22 Survivorship cohorts further emphasize persistent symptom distress and QoL deficits among thyroid cancer survivors despite a favorable prognosis.20,21 In this context, the high prevalence and persistence of depressive symptoms in this cohort (42% before surgery; 66% at 12 months among those symptomatic at baseline) are particularly important. By prospectively combining a generic QoL instrument, validated depression screening, and population-based reference comparisons, this study adds incremental evidence demonstrating that preoperative depressive symptoms independently predict poorer QoL at 12 months across domains.
In 2007, Miccoli et al. examined the effects of thyroidectomy on psychiatric symptoms and QoL. They showed that, regardless of the surgical indication, patients undergoing thyroid surgery reported lower QoL in the mental health and social functioning areas of the Short Form 36 (SF-36) questionnaire, which is similar to the RAND-36 used in this study, when compared to the general Italian population and to patients having non-thyroid surgery. Even long after reaching postoperative euthyroidism, patients showed notable improvement in mental health (except for social functioning), and psychiatric symptoms diminished. However, the perceived QoL of patients remained below that of the general Italian population. There were no significant differences in the physical health areas of the SF-36 when compared to the general population or non-thyroid surgery patients, and physical health did not improve after surgery. 23 The present findings largely align with those of Miccoli et al. with the most significant improvements in RAND-36 scores being observed in domains related to mental well-being. However, even after surgical treatment, patients’ QoL continued to be lower than that of the general Finnish population.
Dogan et al. examined changes in QoL after thyroid surgery. The study included 101 patients who completed a questionnaire based on the World Health Organization Quality of Life Scale (WHOQOL-BREF) before surgery, in the early postoperative period (<1 month after surgery), and in the late postoperative period (4–6 months after surgery). The authors observed a significant improvement in QoL related to general health, physical, and environmental aspects during the late postoperative period compared to both the preoperative and early postoperative periods. The improvement in QoL was not affected by whether the surgery was performed for benign or malignant thyroid disease. 2
Mirallié et al. conducted a large prospective multicenter trial involving 800 patients to evaluate the impact of thyroidectomy on QoL at 6-month follow-up. QoL was measured using the SF-36 questionnaire. The follow-up showed a significant improvement across all eight domains of the questionnaire, with the most notable change seen in mental health scores. Similar to the present study and that of Miccoli et al., QoL was also compared with that of the general French population and was found to be significantly lower in nearly all domains, both before and after surgery. In this study, thyroidectomy for Graves’ disease was associated with the most favorable improvement in QoL, while surgery for malignant tumors was associated with a decline in QoL at 6 months. 24
In the present cohort, a significant proportion of patients (42%) reported depressive symptoms prior to thyroid surgery, and these symptoms were associated with poorer QoL even 12 months after surgery. These findings indicate that preoperative assessment of depressive symptoms—by using tools like the BDI—may help identify individuals at risk of less favorable long-term outcomes. Early detection could allow for targeted psychosocial support, which might enhance postoperative recovery and QoL.
No studies have been conducted on the effects of preoperative depression screening and subsequent treatment of diagnosed depression on postoperative depressive symptoms and QoL in thyroid surgery patients. Some evidence exists from other surgical populations. In 2011, Dao et al. published a randomized controlled trial involving patients scheduled for coronary artery bypass graft (CABG) surgery who exhibited clinically significant symptoms of depression and/or anxiety. The study found that patients who underwent brief cognitive behavioral therapy had a shorter hospital stay than those receiving usual treatment, and their depressive symptoms decreased by the time of hospital discharge. In contrast, their symptoms increased in the comparison group. At the 3- to 4-week follow-up, both groups showed improvements in QoL and reductions in anxiety symptoms, but these improvements were more pronounced in the cognitive behavioral therapy group. 25
In 2025, Hall et al. reported similar results in a systematic review, meta-analysis, and meta-regression that evaluated the impact of psychological prehabilitation on surgical outcomes. The review assessed the effects of psychotherapy on four postoperative endpoints: length of hospital stay, pain, anxiety, and depression. The pooled analysis showed significant reductions in all these endpoints. Neither the psychotherapy modality nor the type of surgery significantly affected outcomes, except in the case of anxiety. 26
The response rate in the present study was relatively high compared with international QoL research, with 64% of patients completing the baseline survey. Moreover, 77% of those who responded to the QoL questionnaires remained in the study throughout the entire 12-month follow-up period, which strengthens the reliability of our findings. Because initial data found no differences in preoperative QoL according to the diagnosis leading to thyroid surgery, 10 all patients, regardless of surgical indication, were analyzed as a single group in the present study.
Limitations
QoL refers to an individual’s personal perception of their well-being and functional ability across different areas of life. As with most QoL research, this presents the challenge that no single universally accepted tool exists for its measurement. In this context, it is reasonable to question whether the RAND-36, despite its widespread use, is the best tool for assessing QoL in our study population.
Poor QoL was defined as a score more than −2 SD below the age-adjusted reference value in any RAND-36 domain. This threshold may be considered somewhat arbitrary and open to debate. It also combines clinically heterogeneous patients into a single category, as impairment in only one domain is sufficient for classification as poor overall QoL. Nevertheless, similar cutoffs have been used in previous QoL studies.14 –16 It is also possible that this definition may underestimate rather than overestimate the prevalence of poor QoL in our study population.
In this study, the postoperative RAND-36 questionnaire was administered at scheduled time points, that is, 6 and 12 months after surgery without requiring patients to be euthyroid when responding. Since both hypothyroidism and hyperthyroidism are known to affect QoL, this might have influenced the results. However, in a post hoc analysis, the proportion of patients who were euthyroid at 12 months after surgery was evaluated, and as many as 93% were euthyroid (data not shown); therefore, this is likely not a significant limitation.
During the study period, 314 patients underwent thyroid surgery at the authors’ hospital, of whom slightly less than half responded to the RAND-36 QoL questionnaire. Of those with depressive symptoms at baseline (n = 68), nearly all (n = 67) completed the RAND-36 both preoperatively and at the 12-month follow-up. It is possible that patients with depressive symptoms felt a stronger need to express their concerns, leading to their overrepresentation in the data. The results might have been different if the overall response rate had been higher.
Conclusion
In this cohort, overall QoL improved during the 12-month follow-up after thyroid surgery, although it remained lower than that of the general Finnish population. The most pronounced improvements were observed in domains related to mental well-being. While these changes were statistically significant, the absolute numerical improvements in scores were relatively small.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the regional medical research ethics committee of the Wellbeing Services County of North Ostrobothnia (number 43/2021).