
Abstract
Background and aims:
Over recent decades, the management of abdominal aortic aneurysms (AAAs) has undergone substantial transformation, influenced by the introduction of minimally invasive endovascular aneurysm repair (EVAR), advances in early detection, a reduction in disease prevalence, and aging. This study investigated long-term trends in AAA repair incidence, treatment modality, and mortality outcomes across Denmark, Finland, Norway, and Sweden—four neighboring countries with comparable healthcare systems and registry infrastructures.
Methods:
National registry data were used to identify intact (iAAA) and ruptured abdominal aortic aneurysm (rAAA) repairs from 1998 to 2017 (2008–2017 for Norway). Repair incidence, treatment modality (EVAR vs open repair (OAR)), and mortality (30-day and 1-year) were calculated and compared by country, age group, sex, and time period. Life-table analyses assessed long-term survival.
Results:
We identified 39,683 iAAA and 15,086 rAAA repairs. During the study, iAAA repair incidence rose markedly among octogenarians, while rAAA repair incidence declined across all countries. EVAR usage increased over time for both iAAA (11.0%–54.1%) and rAAA (2.5%–24.3%). Perioperative mortality declined throughout the study, with 30-day mortality after iAAA repair falling to 1.9% and after rAAA repair to 27.3%. One‑year mortality similarly improved: for iAAA, it reached 5.9%, and for rAAA, it reached 35.8%. Women had consistently higher 30-day and 1-year mortality than men across all procedure types. Outcomes and survival trends were largely similar between the four countries.
Conclusion:
In the Nordic countries, rAAA repair incidence decreased substantially between 1998 and 2017. EVAR adoption increased and was associated with a rising incidence of iAAA repair in octogenarians. Mortality rates were comparable across the four countries and declined over time for both iAAA and rAAA repair. However, females had consistently poorer perioperative survival than males.
Keywords
Context and relevance
Abdominal aortic aneurysm (AAA) treatment practices and outcomes are well studied in clinical trials, but international comparisons using real-world data remain limited outside of selective vascular registries. This study leverages high-quality national registries that capture the entire populations of Denmark, Finland, Norway, and Sweden to assess two decades of AAA repair trends. The analysis found that ruptured AAA repair has become increasingly rare, and that elective repair now involves older patients, accompanied by rising use of endovascular repair. Perioperative and long-term outcomes have improved, but sex-based disparities remain.
Introduction
Abdominal aortic aneurysms (AAAs) are the most common type of arterial aneurysm. 1 The only effective treatment is operative, with either open aortic repair (OAR) or endovascular aneurysm repair (EVAR).2,3 EVAR was introduced in the 1990s and gained widespread adoption in the early 2000s after trials demonstrated lower perioperative mortality in intact AAA (iAAA) repair.4 –7 Subsequent studies also showed low perioperative mortality in ruptured AAA (rAAA) repair. 8 While concerns remain about the long-term durability of EVAR, recent European Society for Vascular Surgery (ESVS) guidelines recommend it as first-line therapy for most patients. 2
Simultaneously, the epidemiology of AAA has changed. Improved early detection, declining prevalence, and an aging patient population have reshaped the disease landscape. In Sweden, AAA screening was introduced in 2006 and reached nationwide coverage in 2015, leading to earlier detection and fewer ruptures. 9 Contemporary screening cohorts report that AAA prevalence in 65-year-old men has fallen to under 1%, markedly lower than in previous decades, reflecting reduced smoking and better cardiovascular risk control.10,11 Despite this, repair rates among elderly patients continue to rise. 12
Denmark, Finland, Sweden, and Norway are neighboring countries with socioeconomically similar populations, publicly funded healthcare systems, and well-established nationwide patient registries, yet AAA repair centralization strategies differed during 1998–2017. Denmark implemented national centralization by law in 2007, leaving six hospitals performing AAA repair. 13 Three of these offered EVAR in 2017. Norway, Sweden, and Finland maintained more distributed systems. By 2015, Norway had 17 AAA centers, 12 of which offered EVAR. 14 Sweden, whose population is approximately double that of its neighbors, had around 30 AAA centers, all but two of which performed EVAR procedures in 2016. 15 Finland remained the least centralized country regarding OAR, utilizing approximately 20 hospitals for 5.5 million inhabitants. In contrast, EVAR was legally restricted to the five university hospitals during the study. 16
The Nordic countries provide a useful setting for studying changes in AAA repair over time, as they share many demographic and healthcare features but differ in screening, centralization, and EVAR adoption. Examining them together allows assessment of temporal trends in AAA repair. This study analyses national data from 1998 to 2017 to assess how iAAA and rAAA repair evolved across the Nordic countries, focusing on surgical approach, perioperative mortality, and long-term survival.
Methods
Patient-level data from national registries in Denmark, Finland, Norway, and Sweden were aggregated (Supplemental Table 1). EVAR and OAR procedures performed between January 1, 1998, and December 31, 2017 (Norway 2008–2017) were identified using the Nordic Medico-Statistical Committee (NOMESCO) Classification of Surgical Procedures. 17 Ruptured and intact AAAs were categorized based on ICD-10 codes I71.3 and I71.4, respectively. Mortality data were retrieved from national cause-of-death registries in each country.
The gathered variables included age, sex, possible iAAA diagnosis, possible rAAA diagnosis, the operation(s) performed and their date, and date of death. Perioperative mortality was defined as death within 30 days of the index operation. For each patient, only the primary procedure within the study period was included in the analysis. Unique personal identifiers were used for cross-matching between cause-of-death registries and surgical procedure registries. Analyses were based on available aggregated registry data for each variable, and no imputation of missing data was performed.
Data from each participating country were analyzed using consistent methods. The analyses included operation rates and mortality rates for iAAA and rAAA operations in three age groups (<65, 65–80, and >80 years) according to patient age at the date of operation. We calculated operation rates for each country by dividing the number of patients in an age group by the reported population in the same age bracket during the year(s) in question. For the lowest age group (<65-year-olds), the age bracket was chosen to be 40–64 years. Population data were obtained from Statistics Denmark, Statistics Finland, Statistics Norway, and Statistics Sweden.18 –21 Rates were calculated in 5-year intervals and are reported as per 100,000 person-years ⩾40 years.
Ten-year life tables for both iAAA and rAAA operations were constructed using the actuarial life-table method. This approach estimates survival probabilities by dividing follow-up time into fixed intervals and calculating survival rates within each period. Censored observations were accounted for by assuming that losses occurred uniformly within each interval. Confidence intervals (CIs) for operation rates were calculated assuming a Poisson distribution. CIs for mortality were calculated using the Clopper–Pearson exact method. Welch’s unequal variance t-test was used to compare patient ages. The chi-square tests were applied to determine p values for categorical variables. The log-rank test was used to compare groups in life-table analyses. p < 0.05 was considered significant. Python 3.8.8 with SciPy 1.9.3, Matplotlib 3.3.4, Pandas 1.5.3, and Microsoft Excel version 2501 were used for statistical analysis.
To comply with the General Data Protection Regulation (GDPR) of the European Union and national laws, data were pseudonymized and aggregated into broad strata before joint analysis. In Denmark, the study was conducted in accordance with national regulations for registry-based research, for which formal ethical approval was not required. In Sweden, ethical review board approval was obtained (2014/078), with individual consent waived for this retrospective registry study. In Norway, the Norwegian Directorate of Health approved the delivery of pseudonymous statistics (research permit 21/16490-5, 26 November 2021). In Finland, the Institutional Review Board of Helsinki University Hospital approved the study (permit §100/2023, 20 December 2023); no separate ethics committee approval or patient consent is required for registry-based research. This study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. 22
Results
Between 1998 and 2017, 39,683 iAAA repairs and 15,086 rAAA repairs were performed across the four participating countries, excluding reoperations. Women accounted for 16.1% and 16.3% of iAAA and rAAA repairs, respectively (p = 0.57) and were older than men (mean age, iAAA: 73.6 versus 71.8 years; rAAA: 76.4 versus 73.1 years; p < 0.001). Country-specific patient characteristics are presented in Table 1.
Patient characteristics for each country.
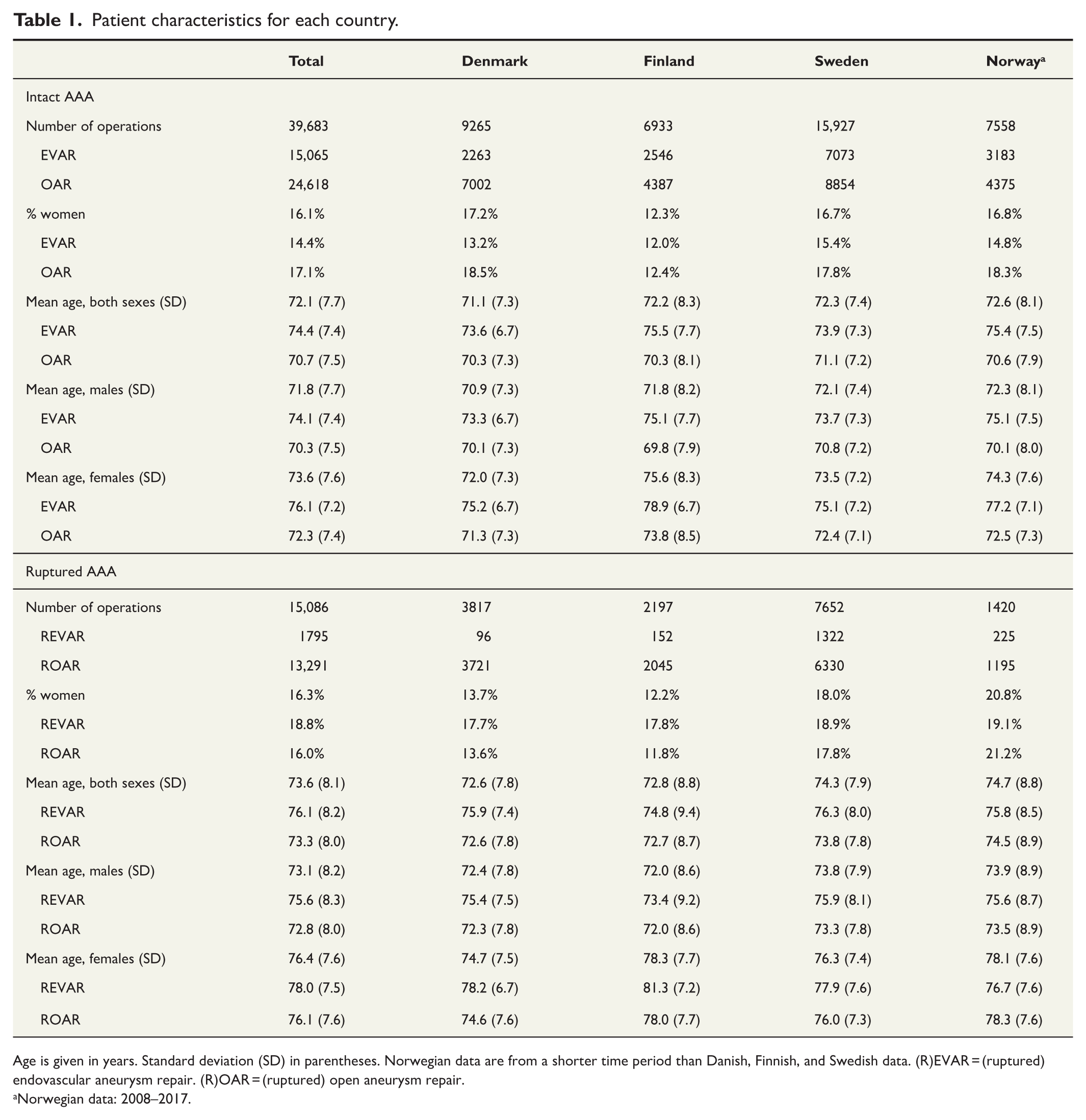
Age is given in years. Standard deviation (SD) in parentheses. Norwegian data are from a shorter time period than Danish, Finnish, and Swedish data. (R)EVAR = (ruptured) endovascular aneurysm repair. (R)OAR = (ruptured) open aneurysm repair.
Norwegian data: 2008–2017.
Mean iAAA operation incidence across the whole study period was 17.4 (95% CI = 17.3–17.6) per 100,000 person-years (males: 30.4 (30.1–30.8); females: 5.4 (5.3–5.5)). Mean iAAA operation incidence increased during the early study period and plateaued in later eras, while EVAR use increased substantially (Fig. 1).
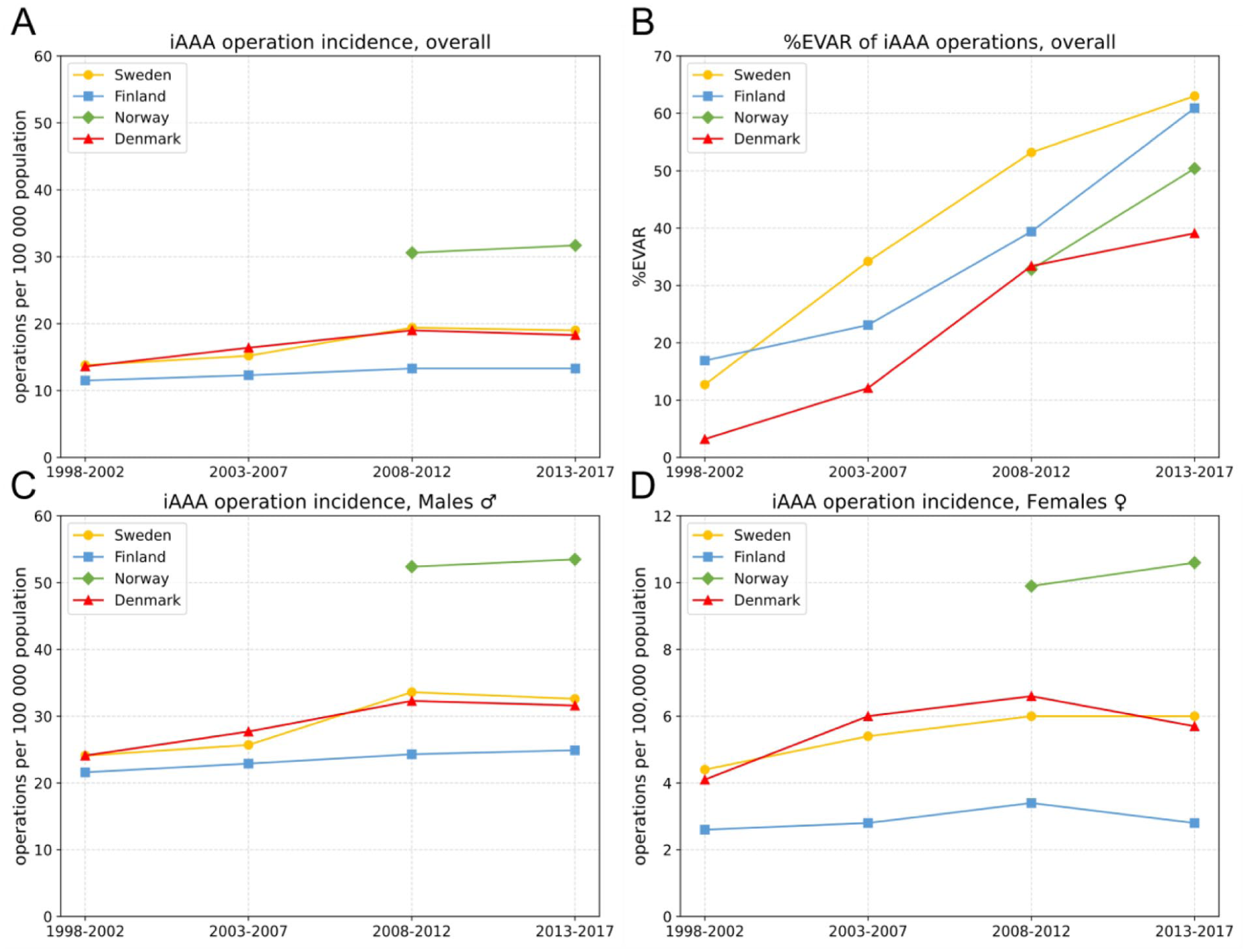
Incidence of intact abdominal aortic aneurysm (iAAA) repair in Sweden, Finland, Norway, and Denmark during four time periods (1998–2002, 2003–2007, 2008–2012, and 2013–2017). (A) Overall incidence. (B) Proportion of iAAA repairs performed with endovascular aneurysm repair (EVAR). (C) Incidence among males. (D) Incidence among females (note the different y-axis scale).
Mean iAAA operation incidence among patients over 80 years was 29.2 (95% CI = 28.4–29.9) per 100,000 person-years. Incidence and EVAR use increased throughout the study period in all four countries (Fig. 2).
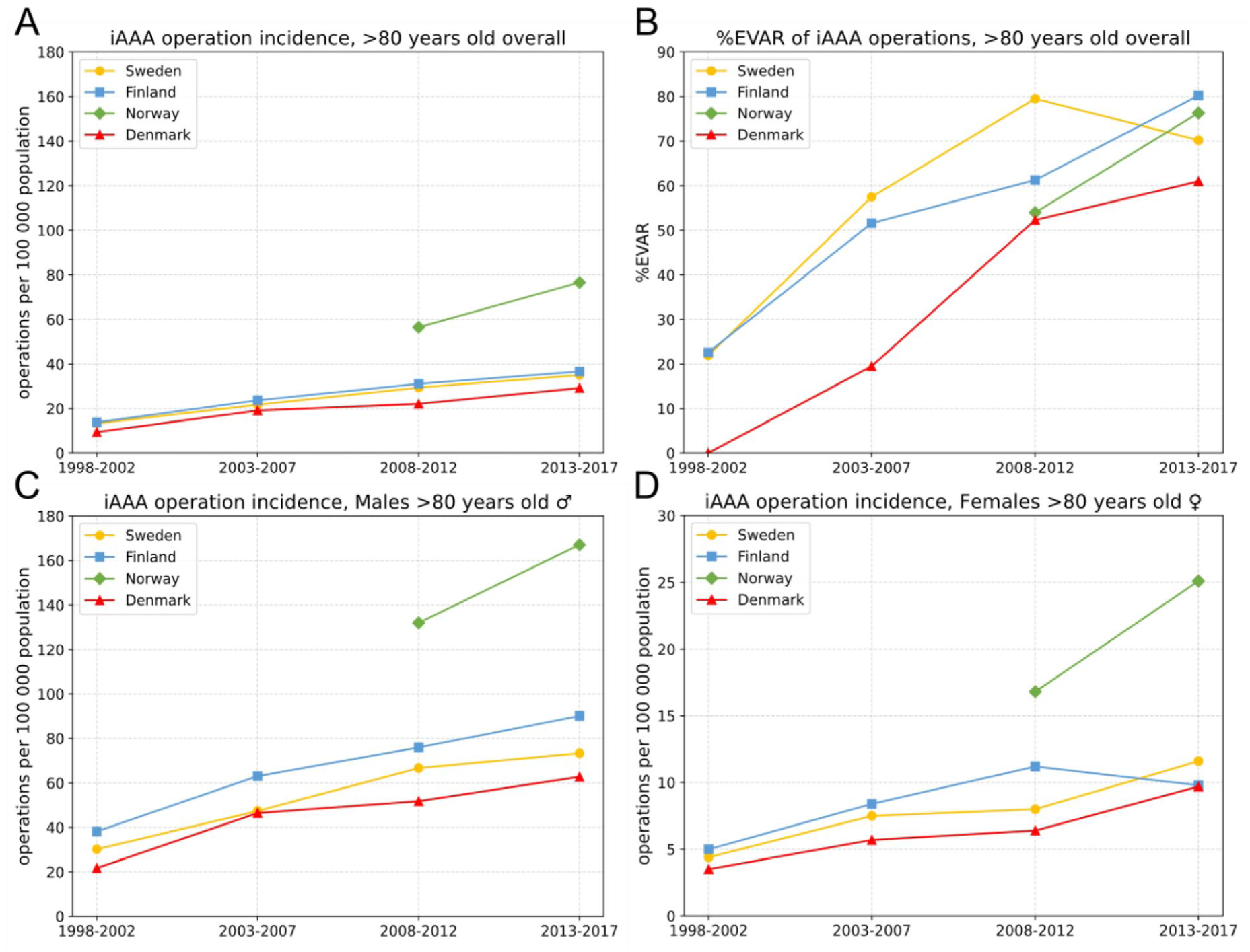
Incidence of intact abdominal aortic aneurysm (iAAA) repair among octogenarians in Sweden, Finland, Norway, and Denmark during four time periods (1998–2002, 2003–2007, 2008–2012, and 2013–2017). (A) Overall octogenarian incidence. (B) Proportion of iAAA repairs performed with endovascular aneurysm repair (EVAR). (C) Incidence among octogenarian males. (D) Incidence among octogenarian females (note the different y-axis scale).
Mean rAAA operation incidence across the whole study period was 6.7 (95% CI = 6.6–6.8) per 100,000 person-years (males: 11.7 (11.5–11.9); females: 2.0 (2.0–2.1)). Incidence declined throughout the study period in all four countries, while the use of EVAR in rAAA repair (REVAR) increased from 2.5% to 24.3% of operations (p < 0.001; Fig. 3).
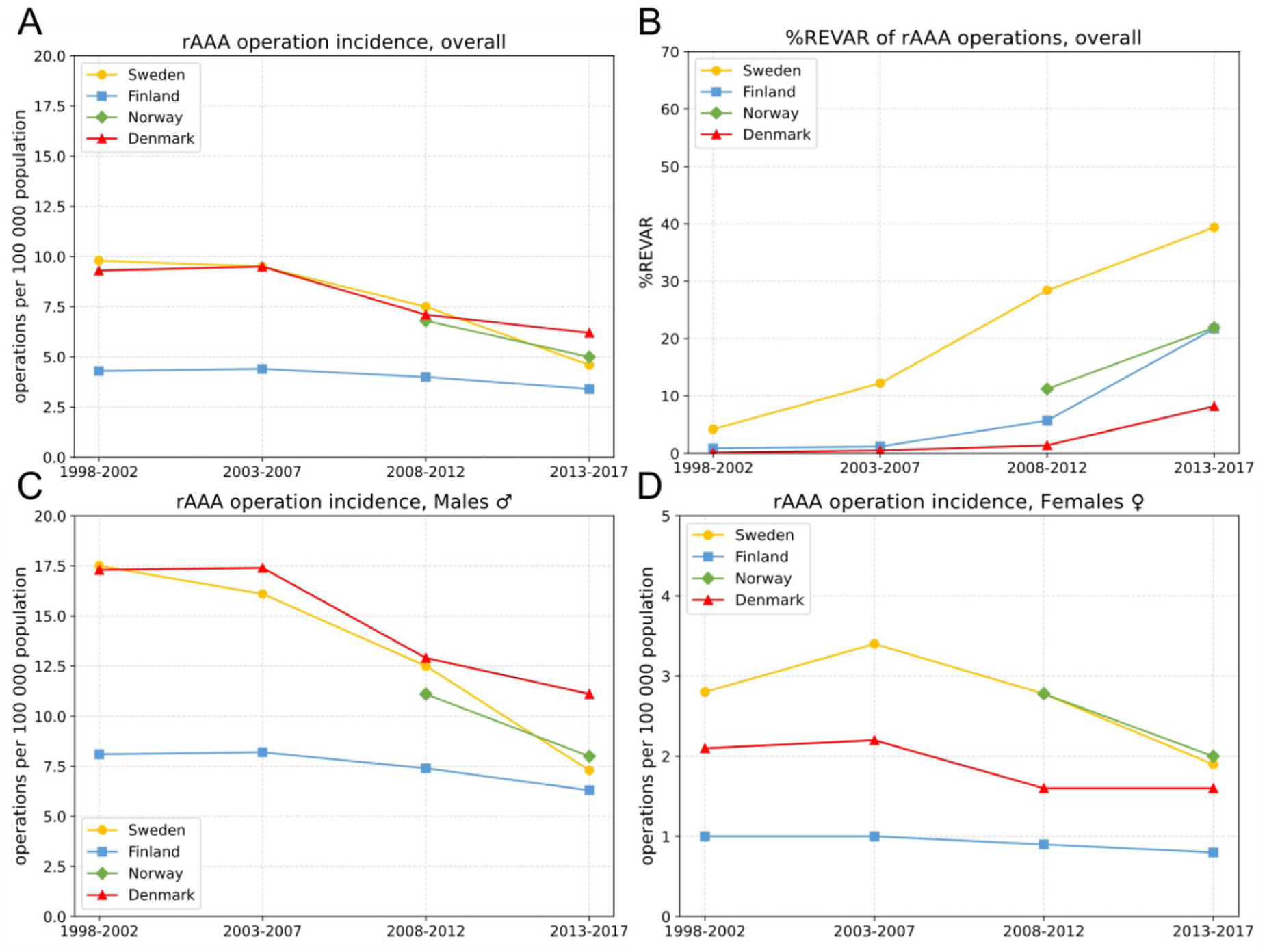
Incidence of ruptured abdominal aortic aneurysm (rAAA) repair in Sweden, Finland, Norway, and Denmark during four time periods (1998–2002, 2003–2007, 2008–2012, and 2013–2017). (A) Overall incidence. (B) Proportion of rAAA repairs performed with endovascular aneurysm repair (REVAR). (C) Incidence among males. (D) Incidence among females (note the different y-axis scale).
After iAAA repair, 30-day and 1-year mortality rates were 2.8% (95% CI = 2.7–3.0) and 7.6% (7.3%–7.9%), respectively, across both sexes in all countries, time periods, and age groups. Female patients had higher mortality than males: the 30-day mortality rate was 3.8% (3.4%–4.3%) for females compared to 2.7% (2.5%–2.8%) for males (p < 0.001), while the 1-year mortality rate was 9.0% (8.3%–9.7%) for females and 7.3% (7.1%–7.6%) for males (p < 0.001).
Mortality rates following iAAA repair were lower in younger patients and increased progressively with age. Thirty-day mortality was 1.5% (1.2%–1.8%) in patients under 65 years, 2.9% (2.7%–3.1%) in those aged 65–80 years, and 4.4% (3.9%–5.0%) in patients over 80 years. One-year mortality was 4.0% (3.5%–4.5%), 7.5% (7.2%–7.8%), and 12.3% (11.4%–13.2%) in the same age groups, respectively. Treatment-specific (EVAR versus OAR) 30-day and 1-year mortality across age groups is shown in Supplemental Fig. 1. Mortality rates following iAAA repair declined across all countries during the study period, with the most notable reduction observed in 30-day mortality (Fig. 4).
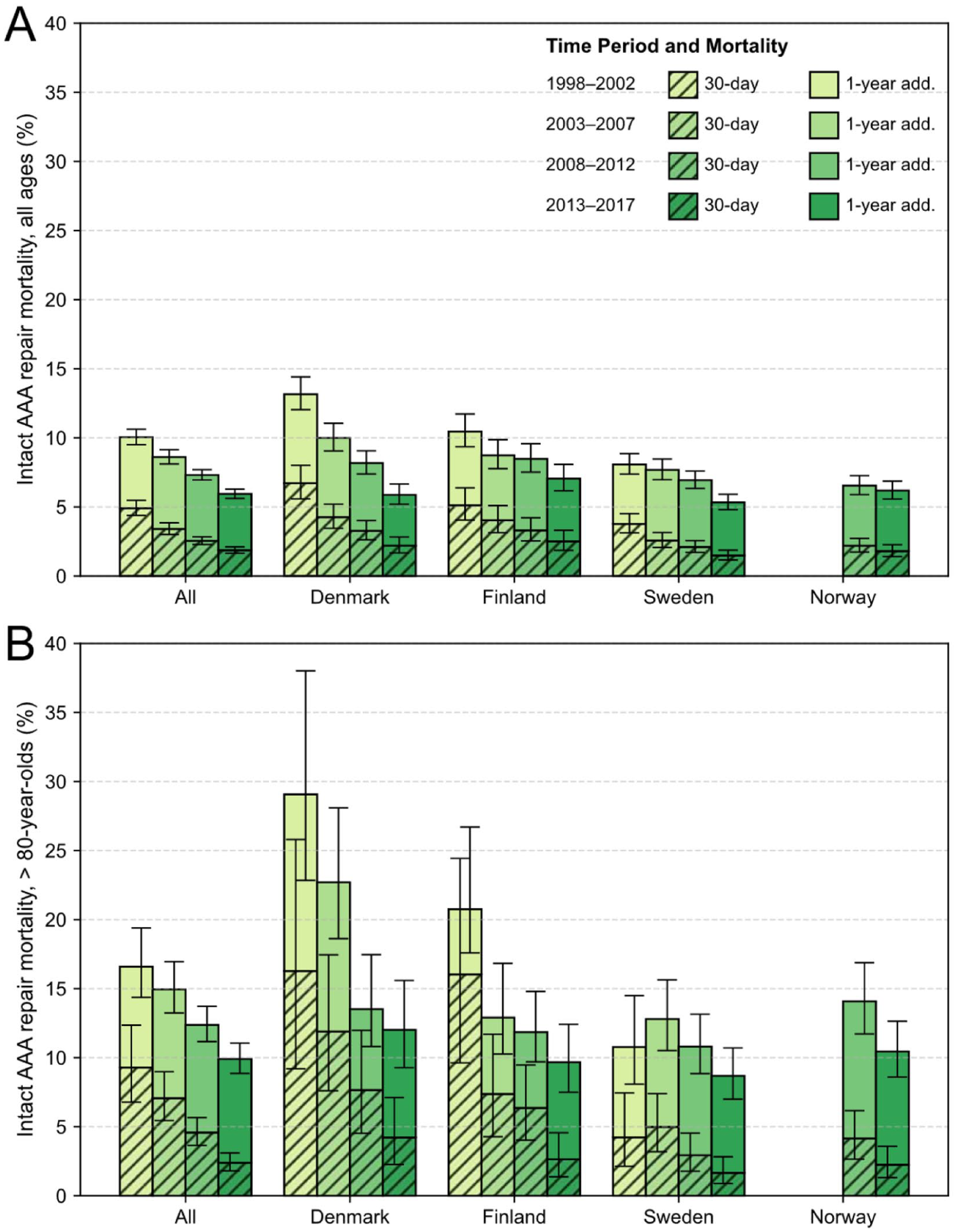
Thirty-day and 1-year mortality after intact abdominal aortic aneurysm (iAAA) repair in four Nordic countries during four consecutive time periods, shown for (A) all age groups and (B) patients aged >80 years.
Following rAAA repair, the mean 30-day and 1-year mortality rates were 34.9% (34.1%–35.6%) and 42.6% (41.8%–43.4%), respectively, across both sexes in all countries, time periods, and age groups. Similar to iAAA repair, female patients had higher mortality than males. The 30-day mortality rate was 40.5% (38.6%–42.5%) in females compared to 33.8% (32.9%–34.6%) in males (p < 0.001), while the 1-year mortality rate was 49.6% (47.6%–51.7%) in females versus 41.2% (40.3%–42.1%) in males (p < 0.001).
Younger patients had lower mortality than older patients after rAAA repair. Thirty-day mortality was 19.2% (17.5%–20.9%) in patients under 65 years, 33.1% (32.1%–34.1%) in those 65–80 years, and 50.5% (48.8%–52.3%) in those over 80 years. One-year mortality was 23.1% (21.3%–25.0%), 41.2% (40.2%–42.2%), and 59.7% (57.9%–61.4%) in the same age groups, respectively. Treatment-specific (REVAR versus ROAR) 30-day and 1-year mortality across age groups is shown in Supplemental Fig. 2.
Thirty-day and 1-year mortality rates after rAAA repair declined during the study period (Fig. 5). A statistically significant reduction in 30-day mortality between the first and last 5 years of the study was observed in all three countries with available data (p < 0.001). Similarly, 1-year mortality declined in all three countries (p < 0.001 in Denmark and Sweden, p < 0.01 in Finland). Between 2008–2012 and 2013–2017, 30-day mortality fell in Denmark (p < 0.001) and Sweden (p < 0.01). A statistically significant fall in 1-year mortality was observed only in Denmark (p < 0.001).
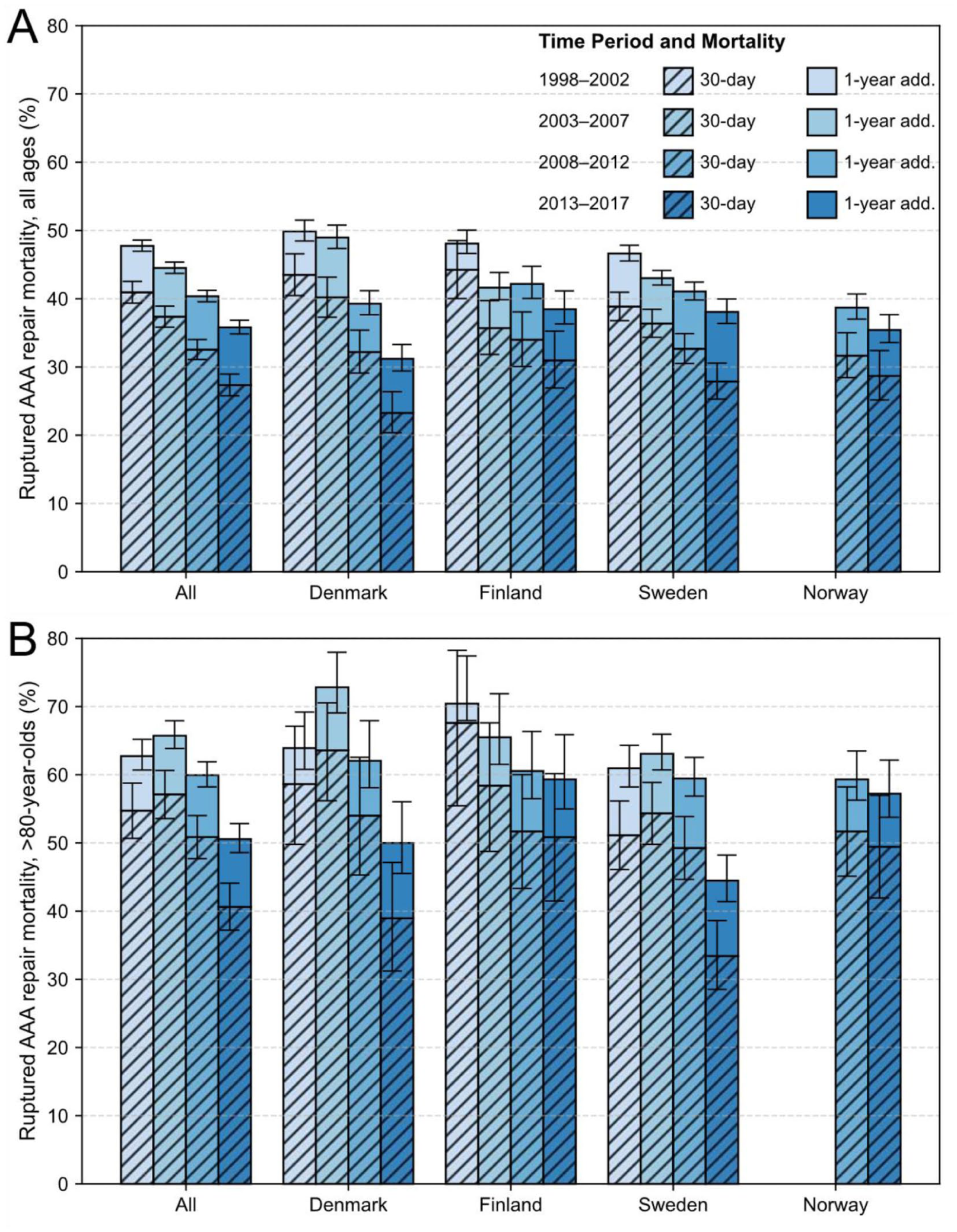
Thirty-day and 1-year mortality following ruptured abdominal aortic aneurysm (rAAA) repair in four Nordic countries during four consecutive time periods, shown for (A) all age groups and (B) patients aged >80 years.
Life-table analysis found a statistically significant difference in 10-year survival between males and females, with females showing poorer survival following iAAA and rAAA repair (log-rank p < 0.001; Fig. 6A, B). When both sexes were analyzed together, survival trends were similar in all countries, with Finnish iAAA patients and Swedish rAAA patients experiencing the lowest survival rates compared with their counterparts (Fig. 6C, D).
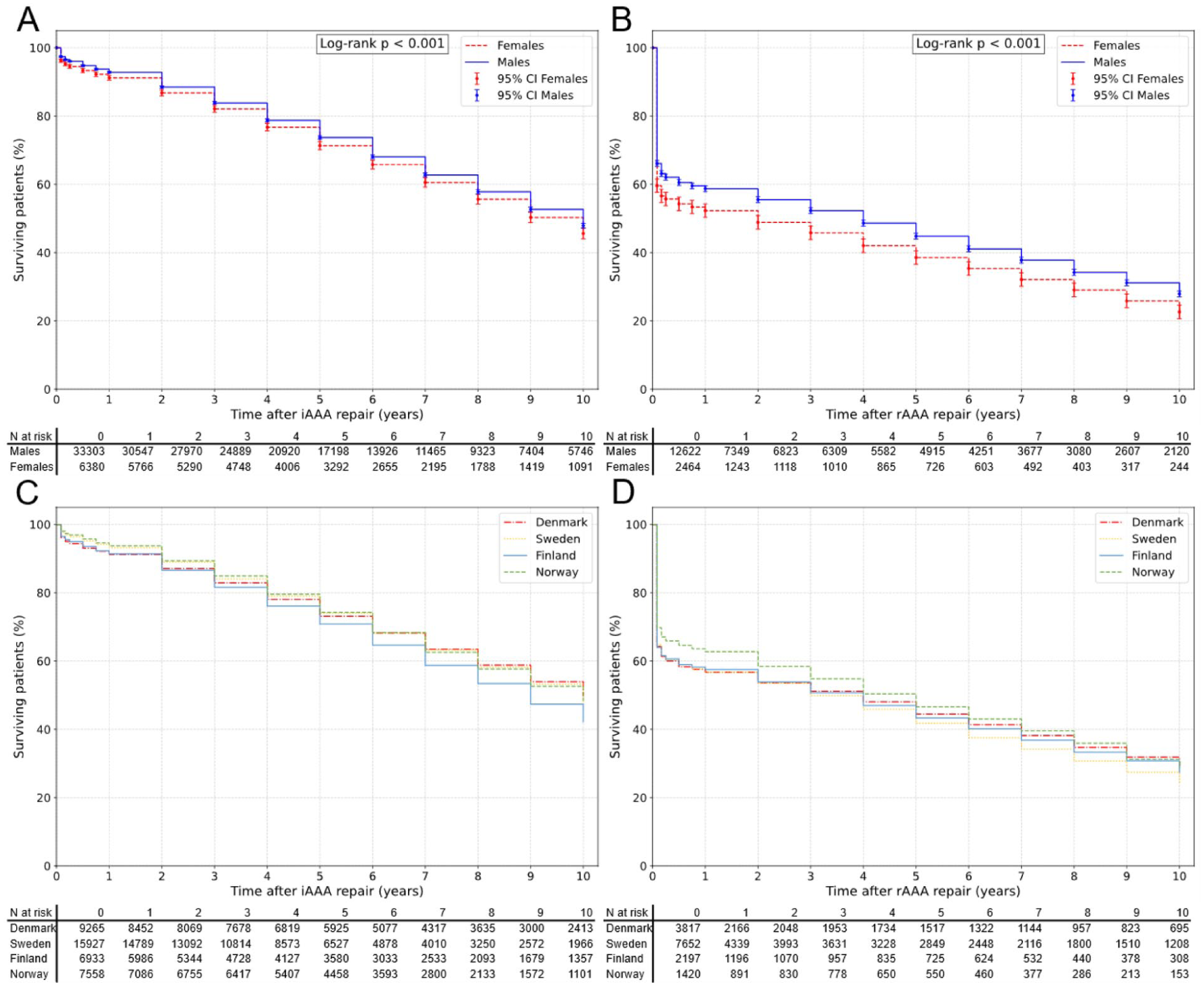
Life-table survival after intact (A) and ruptured (B) abdominal aortic aneurysm repair by sex, showing poorer survival in females (log-rank p < 0.001). Panels C and D show corresponding survival by country (DEN = Denmark, SWE = Sweden, FIN = Finland, and NOR = Norway).
Discussion
In this study, we analyzed two decades in the surgical management of iAAAs and rAAAs across four Nordic countries. Key findings include falling rAAA repair incidence, rising iAAA repair rates among octogenarians, increasing adoption of EVAR, decreasing perioperative mortality, and persistently worse outcomes for female patients.
The overall incidence of iAAA repair increased during the first 15 years of the study before plateauing in all countries. Among octogenarians, however, incidence continued to rise throughout the study, more than tripling in Denmark and more than doubling in Finland and Sweden. This likely reflects a previously recognized demographic shift in AAA patients, where reduced smoking and improved management of comorbidities allow AAAs to reach the surgical threshold at older ages.12,23 –25
Norway had a notably high iAAA repair incidence across all subgroups from 2008 to 2017. Its mean iAAA repair incidence (31.2 per 100,000) was 79.3% higher than the average of the other three countries. This marked difference may reflect variation in repair indications or referral practices. The high elective repair rate does not appear to translate into a correspondingly lower rAAA incidence, suggesting that some repairs may have been performed pre-emptively in patients at relatively low rupture risk. Similar figures have previously been reported from Norway: Wendt et al. 26 documented 8585 elective AAA or iliac artery aneurysm repairs in Norway between 2001 and 2013, corresponding to an average of 613 repairs per year compared with 756 in this study. The incidence rates are not directly comparable as Wendt et al. used a higher age threshold (⩾60 years versus ⩾40 years in this study).
In contrast, Finland had the lowest iAAA and rAAA repair rates, although the difference was less pronounced than in Norway. The underlying reasons for these disparities remain unclear and warrant further investigation into national differences in detection and treatment practices.
RAAA repair incidence declined in all countries. The largest drop occurred in Sweden, which launched a national AAA screening program for 65-year-old men in 2006. 9 Screening likely contributed to this decline by enabling early detection and elective repair, reducing emergency rAAA surgeries. Indeed, iAAA repairs increased by nearly one-third in Sweden between 2003–2007 and 2008–2013.
However, other factors must be contributing, as rAAA repair also declined in countries without screening. A major driver is the decline in smoking: between 2000 and 2015, smoking prevalence dropped from 44.9% to 21.2% in Norway, 37.8% to 20.5% in Denmark, 33.4% to 17.1% in Sweden, and 29.0% to 20.2% in Finland. 27 In addition to reducing AAA incidence, lower smoking rates decrease the risk of rupture. 3 Broader use of statins and improved cardiovascular prevention may also have contributed by slowing aneurysm growth and reducing rupture risk. 25 Meanwhile, the plateau in iAAA repair, despite declining AAA prevalence, 28 suggests better detection and elective treatment before rupture. This may be aided by increased incidental detection through abdominal imaging.29 –31
EVAR use rose steadily, eventually comprising around half of all iAAA and a quarter of rAAA repairs. The decrease observed in 30-day and 1-year mortality over time likely reflects this trend. Among octogenarians, the rising repair incidence was driven largely by EVAR adoption. Marked inter-country variation existed in EVAR and REVAR use. Sweden was the earliest and most extensive adopter of both, while Denmark lagged, with REVAR remaining minimal until after 2013.
Comparable international registry analyses, such as those from the VASCUNET collaboration, have shown similar but regionally heterogeneous trends in EVAR adoption. Boyle et al. 32 and Pherwani et al. 33 reported that while Western and Northern Europe, the United Kingdom, and Australia rapidly transitioned to EVAR-dominant practice, Eastern and Southern European countries have shown markedly lower uptake, often below 50%. In this context, the Nordic countries represent an intermediate pattern—ahead of Eastern Europe but still behind early adopters such as Australia.
Sweden consistently demonstrated lower-than-average 30-day and 1-year mortality rates for iAAA repair throughout the study period, while rAAA outcomes were near the four-country average. Sweden’s plummeting smoking prevalence and early EVAR adoption likely contributed to this. In contrast, Denmark exhibited the largest reduction in both 30-day and 1-year mortality following iAAA and rAAA repairs. During the study, these figures declined to become comparable with those of the other countries. This improvement likely reflects a significant decrease in smoking prevalence, along with Denmark’s delayed adoption of EVAR. It may also relate to Denmark’s centralization of vascular services initiated in 2007, which concentrated AAA surgery into fewer high-volume centers and standardized 24/7 coverage nationwide. 13 In octogenarians undergoing iAAA repair, Finland showed an even greater reduction in 30-day mortality, likely due to its high rate of EVAR utilization.
Long-term survival trends following iAAA and rAAA repairs were generally similar across all countries. Norway’s results may appear favorable due to shorter and more recent follow-up (2008–2017 only). In the extended follow-up, survival declined more steeply for Finnish iAAA patients and Swedish rAAA patients. The rAAA survival pattern may be partly explained by Sweden’s high REVAR usage, with more stent failures in extended follow-up,34,35, although this interpretation should be regarded as hypothesis-generating, as we did not have data on stent durability. Swedish rAAA patients were also slightly older than the mean. The causes behind worse long-term iAAA outcomes in Finland remain unclear. Despite high EVAR use, similar patterns were not observed in Sweden, suggesting other contributing factors.
Female patients had consistently worse outcomes following both iAAA and rAAA repair, with higher mortality at 30 days, 1 year, and long-term follow-up. Life-table analyses confirmed that this disadvantage emerged early and persisted. In our study, females were disproportionately more likely to undergo OAR for iAAAs. For rAAA, the trend was reversed, with females more frequently receiving REVAR. Nonetheless, females had worse 30-day and 1-year survival after all procedure types (OAR, EVAR, ROAR, and REVAR), indicating that treatment type alone does not explain the disparity.
On average, female patients were 2–3 years older than males, which could partially account for higher perioperative mortality. However, age-matched females in the general population live 2–4 years longer than males, suggesting that age alone is insufficient to explain the survival gap.14 –17
Prior studies have similar findings. A 2021 meta-analysis by Pouncey et al. 36 found that females experienced more perioperative complications following both OAR and EVAR for iAAA. For rAAA repair, several studies report higher in-hospital mortality in females despite similar or fewer perioperative complications. Stuntz et al. 37 and Leyba et al. 38 both reported this paradox in REVAR and ROAR outcomes.
A key limitation of this study is the lack of detailed patient demographic data, which prevented adjustments for comorbidities and aortic anatomy. We lacked patient-level follow-up and reintervention data, limiting longer-term subgroup analyses. In addition, Norwegian data were unavailable from 1998 to 2007, unlike the other three countries. Other limitations include questions about the reliability of registry data. 39 Since the registers used are not dedicated vascular registries, variations may exist in how different healthcare providers report their data. Reporting practices may also differ between countries. However, while mislabeling is possible, the large sample size in our study reduces its impact. In addition, as these are nationwide registries, the number of missed cases is likely minimal.
Our study has several strengths. It captures data from the entire populations of four neighboring countries over an extended period, providing a comprehensive overview of trends in aneurysm repair. The patient and death registries we utilized are mandatory for all healthcare providers in these countries. Given the genetic, cultural, and socioeconomic similarities among the populations, analyzing them as a single large cohort is both reasonable and informative.
Conclusion
The incidence of rAAA operations steadily declined in Denmark, Finland, Sweden, and Norway throughout the study period (1998–2017). In contrast, iAAA repair incidence increased among octogenarians, largely driven by the growing use of EVAR. The adoption of EVAR rose for both iAAA and rAAA repairs, contributing to improved perioperative outcomes. Mortality rates were comparable across all four countries and showed a decline over time for both iAAA and rAAA repair. However, females had consistently poorer survival than males, primarily due to higher perioperative mortality.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969261461395 – Supplemental material for Two decades of abdominal aortic aneurysm repair in the Nordic countries from 1998 to 2017: A population-based registry analysis
Supplemental material, sj-docx-1-sjs-10.1177_14574969261461395 for Two decades of abdominal aortic aneurysm repair in the Nordic countries from 1998 to 2017: A population-based registry analysis by Riku Pirinen, Matti Laine, Kim Gunnarsson, Martin Altreuther, Jacob Budtz-Lilly, Anders Wanhainen, Kevin Mani and Maarit Venermo in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-2-sjs-10.1177_14574969261461395 – Supplemental material for Two decades of abdominal aortic aneurysm repair in the Nordic countries from 1998 to 2017: A population-based registry analysis
Supplemental material, sj-docx-2-sjs-10.1177_14574969261461395 for Two decades of abdominal aortic aneurysm repair in the Nordic countries from 1998 to 2017: A population-based registry analysis by Riku Pirinen, Matti Laine, Kim Gunnarsson, Martin Altreuther, Jacob Budtz-Lilly, Anders Wanhainen, Kevin Mani and Maarit Venermo in Scandinavian Journal of Surgery
Supplemental Material
sj-docx-3-sjs-10.1177_14574969261461395 – Supplemental material for Two decades of abdominal aortic aneurysm repair in the Nordic countries from 1998 to 2017: A population-based registry analysis
Supplemental material, sj-docx-3-sjs-10.1177_14574969261461395 for Two decades of abdominal aortic aneurysm repair in the Nordic countries from 1998 to 2017: A population-based registry analysis by Riku Pirinen, Matti Laine, Kim Gunnarsson, Martin Altreuther, Jacob Budtz-Lilly, Anders Wanhainen, Kevin Mani and Maarit Venermo in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-4-sjs-10.1177_14574969261461395 – Supplemental material for Two decades of abdominal aortic aneurysm repair in the Nordic countries from 1998 to 2017: A population-based registry analysis
Supplemental material, sj-jpg-4-sjs-10.1177_14574969261461395 for Two decades of abdominal aortic aneurysm repair in the Nordic countries from 1998 to 2017: A population-based registry analysis by Riku Pirinen, Matti Laine, Kim Gunnarsson, Martin Altreuther, Jacob Budtz-Lilly, Anders Wanhainen, Kevin Mani and Maarit Venermo in Scandinavian Journal of Surgery
Supplemental Material
sj-jpg-5-sjs-10.1177_14574969261461395 – Supplemental material for Two decades of abdominal aortic aneurysm repair in the Nordic countries from 1998 to 2017: A population-based registry analysis
Supplemental material, sj-jpg-5-sjs-10.1177_14574969261461395 for Two decades of abdominal aortic aneurysm repair in the Nordic countries from 1998 to 2017: A population-based registry analysis by Riku Pirinen, Matti Laine, Kim Gunnarsson, Martin Altreuther, Jacob Budtz-Lilly, Anders Wanhainen, Kevin Mani and Maarit Venermo in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors thank the staff of the Biostatistics Unit, University of Helsinki, for providing methodological consultation; all analyses and their interpretation were performed independently by the authors.
Author contributions
Clinical trial registration
N/A.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: R.P. received personal research grants from The Finnish Foundation for Cardiovascular Research, The Aarne Koskelo Foundation, The Finnish Medical Foundation, and The Emil Aaltonen Foundation. These foundations are non-profit organizations and had no involvement in the study design or collection, analysis, and interpretation of data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.