
Abstract
Background:
The aim of breast reconstruction after mastectomy is to improve quality of life and patient satisfaction, but cost-effectiveness of different reconstruction techniques remains uncertain due to methodological limitations in existing studies. High-quality trial-based economic evaluations are therefore needed. This study aimed to compare the quality of life and cost outcomes of patients randomized to different delayed breast reconstruction techniques based on previous receipt of radiotherapy.
Methods:
A single-site randomized controlled trial (GoBreast; NCT03963427) including women aged 18–60 undergoing delayed breast reconstruction was conducted. Patients without previous radiotherapy were randomized to either thoracodorsal flap with implant (TD) or two-stage expander (EXP), while patients with previous receipt of radiotherapy were randomized to either latissimus dorsi with implant (LD) or deep inferior epigastric artery perforator (DIEP) flap. Outcomes included health-related quality of life (HRQoL) (by SF-6D utilities), re-operations, and direct/indirect costs over long-term follow-up.
Results:
Among patients without previous radiotherapy (n = 75), EXP had slightly lower direct healthcare costs, but higher indirect costs, and generated a statistically significant positive change in HRQoL utility value (0.06 (0.02;0.9)) and fewer re-operations (2.34 vs 4.73) during a mean follow-up of 12.9 years. Among patients who had received radiotherapy (n = 25), there were no statistically significant differences in HRQoL utility scores or total costs, but a higher re-operation rate for LD as compared to DIEP.
Conclusion:
Among patients without previous radiotherapy, EXP yielded superior HRQoL and fewer re-operations compared to TD. In patients with previous receipt of radiotherapy, DIEP reconstruction was associated with fewer re-operations and comparable costs compared to LD.
Keywords
Introduction
Several treatment options are available for breast reconstruction after mastectomy. Still, no clear consensus exists on the optimal approach, and both clinical guidelines and standards of care vary across healthcare settings. 1 Breast reconstruction after mastectomy is primarily performed to improve quality of life (QoL) and patient satisfaction with appearance and function. Alongside complications and re-operations, core outcomes for evaluating reconstructive techniques include patient-reported outcomes. 2 Increasingly, healthcare systems also explicitly consider economic consequences to control healthcare spending and devote resources to treatment options that help optimize patient outcomes, given limited budgets.3,4
A recent review of studies on cost-effectiveness in breast reconstruction included seven studies. 4 The available data indicate that, within the commonly accepted cost-effectiveness thresholds of $50,000 to $100,000 per quality-adjusted life year (QALY), deep inferior epigastric artery perforator (DIEP) flap procedures may be considered cost-effective compared with implant-based breast reconstruction. These findings, however, are undermined by significant methodological issues, making it difficult to draw definitive conclusions or provide firm guidance for clinical decision-making. Among others, there is a high risk of bias, unclear patient characteristics (such as radiation therapy status and cancer stage), inconsistent definitions of reconstruction timing, and short follow-up periods. The studies varied in modeling methods, utility measures, and health economic perspectives, limiting the directness and reliability of their conclusions. Overall, the certainty of evidence of current studies is low (GRADE ƟƟОО), and the reporting quality is inconsistent, making definitive conclusions regarding the cost-effectiveness of different methods difficult. 5 The search of the review 4 was performed again on 3 June 2025 for the period 10 May 2023 to 3 June 2025. This search retrieved 51 abstracts, none meeting the review’s inclusion. 4
The aim of this study was to evaluate whether the method of delayed breast reconstruction affects long-term outcomes in three key domains: (1) health-related quality of life utility scores, (2) the frequency of re-operations following the initial reconstruction, and (3) total direct healthcare and indirect costs accumulated during follow-up. The study is based on data from a randomized controlled trial (RCT), the Gothenburg Breast Reconstruction study (GoBreast).6,7 The GoBreast trial has two arms depending on previous receipt of radiotherapy or not. For previously non-radiated patients, the study compares outcomes between a one-stage lateral thoracodorsal flap (TD) with a permanent implant and 2-staged expander reconstruction (EXP). In previously radiated patients, the study compares the latissimus dorsi flap combined with a permanent implant (LD) with the DIEP.
Methods
Protocol
The data for this study come from a single-site, RCT stratified into two groups: non-radiated and radiated patients (The Go Breast Prospective study protocol, ClinicalTrials.Gov # NCT03963427). For GoBreast, short-term complications and quality-of-life outcomes, measured with BREAST-Q, Rand-36, EuroQoL 5D, and Beck’s Depression Inventory-21, have been published previously.6,7 The study is reported according to the CHEERS 8 and the CONSORT 9 guidelines.
Study population and comparators
All patients referred to the authors’ department for breast reconstruction were evaluated for potential inclusion in the study. Invitation letters were subsequently sent to all eligible individuals. Eligibility screening was conducted during the first consultation. Patients who fulfilled the inclusion criteria were invited to join the study. Patients were given sufficient time to consider the information and ask questions before providing written informed consent.
Eligible participants were women aged over 18 years who had undergone a unilateral mastectomy. Individuals were excluded if they were unable to give informed consent, were current smokers, or had a body mass index (BMI) exceeding 30 kg/m². For participants who had received radiation therapy, additional exclusion criteria included previous abdominal surgery or liposuction that made the DIEP flap unsuitable, as well as age greater than 60 years. For the non-radiated group, patients with extensive thoracic scarring that precluded the use of a lateral thoracodorsal flap were excluded.
The number of participants was determined using a power analysis outlined in the Go Breast Prospective study protocol (ClinicalTrials.gov Identifier: NCT03963427), based on expected differences in aesthetic outcomes. In the original protocol, the sample size was based on a 10% difference in aesthetic outcome, assessed by expert and lay panels using a 10-point Visual Analogue Scale, at 80% power. According to the calculation, a sample size of 70 participants in each group would be necessary. No sample size calculations for health economic analyses were performed.
In Sweden, national guidelines recommend autologous delayed reconstruction for patients who have undergone radiotherapy. 10 Accordingly, radiated patients were offered primarily autologous reconstructive options, while non-radiated patients were offered primarily implant-based methods. 10 Based on this, participants were divided into two study arms based on whether they had received radiotherapy. Each arm included two different reconstruction techniques: one-stage lateral thoracodorsal flap combined with a permanent implant (TD) 11 versus two-stage tissue expander reconstruction (EXP), 12 and latissimus dorsi flap with a permanent implant (LD) 13 versus the DIEP flap. 14 The study followed a parallel design, with a planned allocation ratio of 1:1:1:1 across the four groups. Allocation was concealed using a sealed-envelope system.
Setting and location
The study was performed at the Department of Plastic Surgery, Sahlgrenska University Hospital, Gothenburg, one of seven university hospitals in Sweden, with a catchment area of about 1.5 million inhabitants. The department of plastic surgery performs about 350–400 breast reconstructions yearly.
The health care and sickness insurance systems in Sweden are primarily publicly funded through taxes. The health care system is mainly financed by county and municipal taxes, with additional funding from national government grants. Patients pay small fees for services, but the majority of costs are covered by the state. 15 The sickness insurance system is also publicly funded. Employers cover the first 14 days of sick pay (except day 1, which is unpaid), after which the Swedish Social Insurance Agency (Försäkringskassan) provides income-related sickness benefits, funded by employer contributions and general taxation. 16
Ethics and funding
The study received ethical approval from the Regional Ethical Committee of Gothenburg (#043-08 and T948-17) and the Swedish Ethics Review Authority (#2021-06131-02 and 2022-06234-02). Study procedures were in accordance with the Helsinki Declaration, as coded in Swedish law, the “Ethics Review Act” SFS 2003:460, and the Good Clinical Practice guidelines. Data were treated according to the General Data Protection Regulation (GDPR) and the study’s data management plan. All participants gave their written informed consent to participate in the research and to the publication of the results.
The study was funded by grants from the Swedish Cancer Society (21 0279 SCIA) and the federal government under the ALF agreement (ALFGBG-1005048).
Outcomes and valuations, perspective, and time horizon
Benefits—health-related quality of life
Preference-based health-related quality of life (HRQoL) is based on data collected using the Rand 36-Item Short Form Health Survey, which measures HRQoL across eight domains. 17 The survey was administered pre- and postoperatively. The Short Form-6 Dimension (SF-6D) scoring algorithm, based on the UK version of the Brazier tariff, 18 was applied to the RAND-36 responses to derive preference-weighted health utility values from zero (equal to dead) to one (best possible health state). 19
Harms—complications and re-operations
The number of re-operations reflects the total number of surgical procedures each patient underwent during the follow-up period, based on data from the GoBreast study. Follow-up time was from the index surgery date to 30 June 2024. Nipple reconstruction was not considered a re-operation.
Economic costs
Economic costs are analyzed for total, direct, and indirect costs. Direct costs are the healthcare costs that include all medical costs, extracted from the university hospital accounting system, associated with the initial surgery and any potential re-operations during the follow-up period. Total procedure costs represent aggregated costs per surgical episode. These include operating room resources, staff, anesthesia, consumables, and postoperative inpatient care. This top-down costing approach was chosen to reflect real-world hospital expenditures and enhance comparability across procedures. Indirect costs are the value associated with production losses due to absence from work, estimated using the human capital approach. 20 Total costs are the sum of direct and indirect costs. All costs are expressed in 2024 price level with an assumed exchange rate of 1 SEK = 0.09 EUR. See online supplement for the unit costs associated with initial surgery and re-operations, and assumptions around absence from work per treatment options.
Statistical analysis
All outcomes are summarized descriptively using means and 95% confidence intervals (CIs) stratified by treatment group. To assess the difference between the treatments, for previously radiated and non-radiated patients, respectively, regression analyses were run on each of the three outcomes with the different treatments as a (binary dummy) explanatory variable. Confidence intervals are based on non-parametric bootstrapping. The difference in the HRQoL utility improvement was conducted using linear regressions, while re-operations (count data) were based on negative binomial models, and healthcare cost data were based on a generalized linear model (GLM) where the distributional and link functions were chosen based on the model with the best statistical fit, measured as the lowest AIC and BIC estimates. 21 All analyses were conducted using Stata (version 18, StataCorp), and a p-value < 0.05 is considered statistically significant.
Results
There were 25 patients with data on the 5 outcome variables among previously radiated patients and 75 patients among the non-radiated patients (Fig. 1). Reasons for dropouts are given in Supplementary Table 1. The mean follow-up time for re-operations and costs was 12.9 years (min 9.3 to max 15.3 years). The demographic characteristics of the patients across the groups are shown in Table 1.
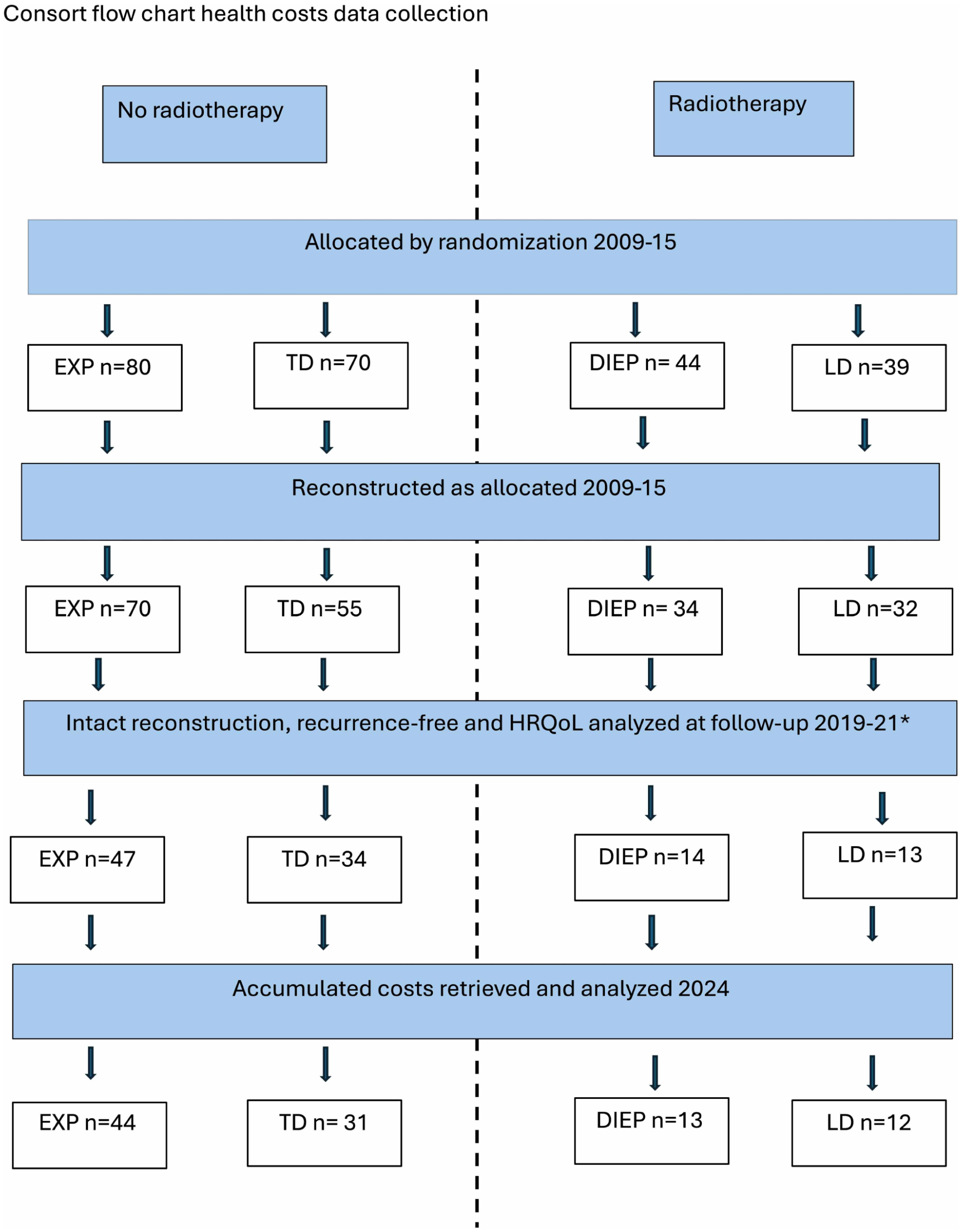
Consort flow chart.
Demography of included participants.
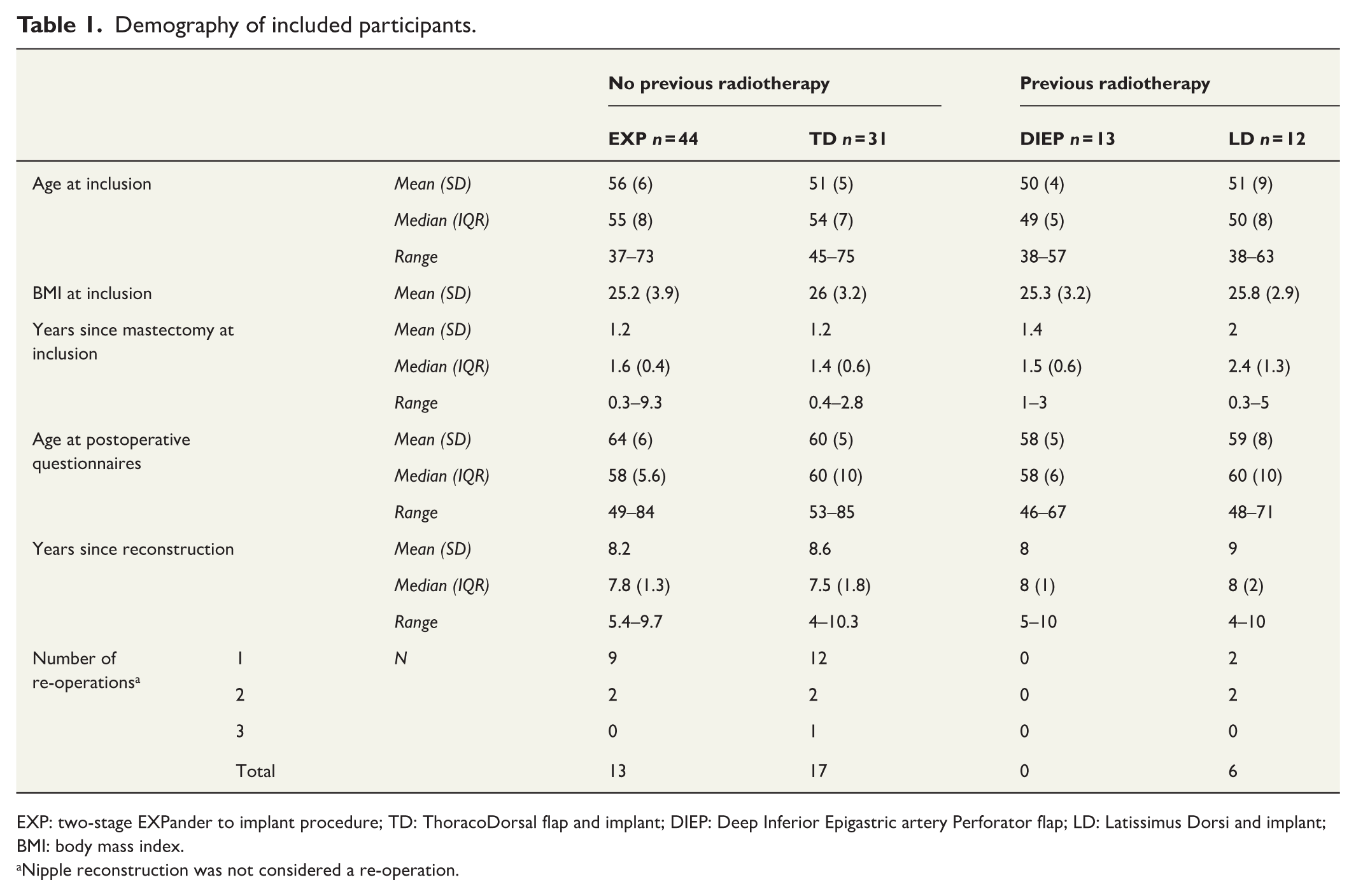
EXP: two-stage EXPander to implant procedure; TD: ThoracoDorsal flap and implant; DIEP: Deep Inferior Epigastric artery Perforator flap; LD: Latissimus Dorsi and implant; BMI: body mass index.
Nipple reconstruction was not considered a re-operation.
For previously radiated patients, Table 2 shows that patients randomized to LD had no meaningful change in the HRQoL utility value between the two measurements and 4.48 re-operations per 100 patient-years. Patients randomized to DIEP had a small improvement in HRQoL, which was not statistically significant, and no re-operations. The mean costs per patient were almost identical between the two groups. For patients not previously radiated, those randomized to EXP had a statistically significant increase in HRQoL and a lower rate of re-operations than those randomized to TD. Resource utilization and unit cost assumptions are given in Supplementary Tables 2 and 3.
Mean (95% CI) for HRQoL improvements, re-operations, and economic costs.
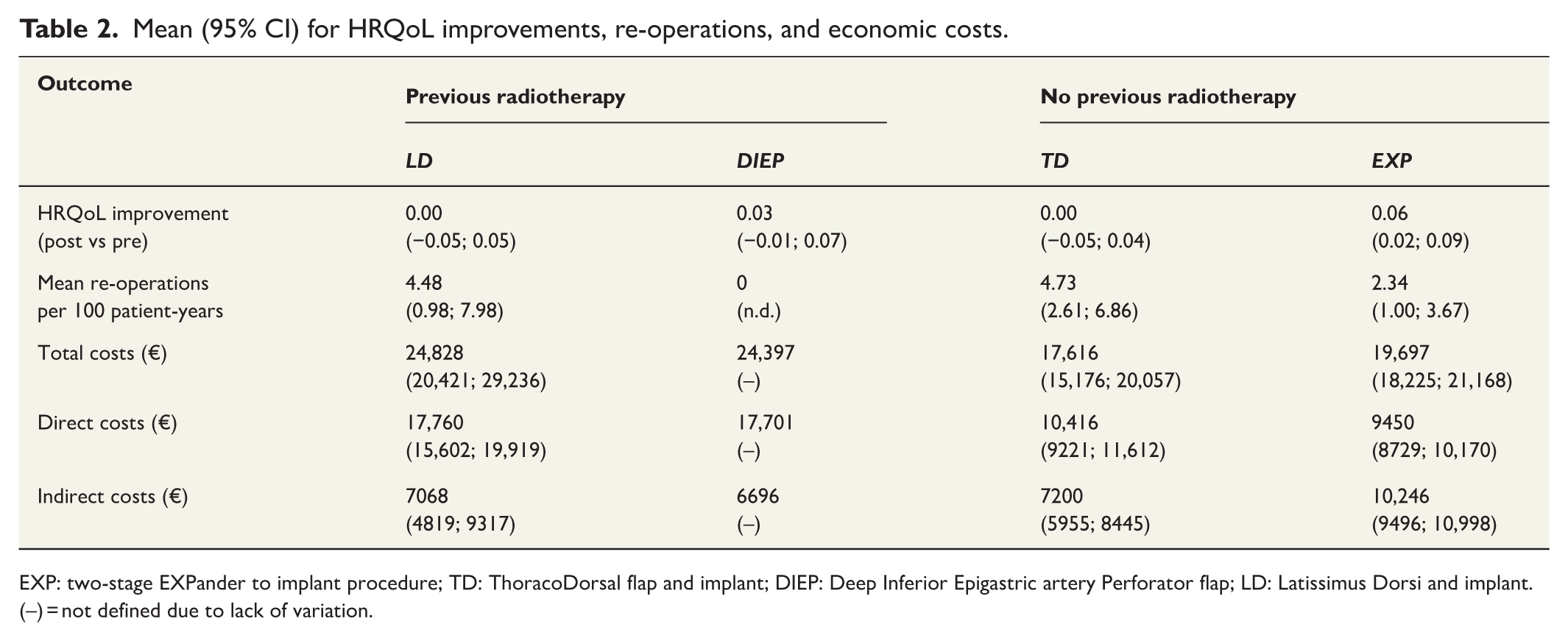
EXP: two-stage EXPander to implant procedure; TD: ThoracoDorsal flap and implant; DIEP: Deep Inferior Epigastric artery Perforator flap; LD: Latissimus Dorsi and implant. (–) = not defined due to lack of variation.
Table 3 shows the results from the regression analyses estimating the difference between the treatment options. For previously radiated patients, patients randomized to LD (vs DIEP) had slightly worse HRQoL development and somewhat lower costs, but the differences are not statistically significant. The difference in re-operations, expressed in Table 3 as the incidence rate ratio (IRR), has a substantial point estimate, but the confidence interval is not defined since there were no re-operations in the DIEP group during follow-up. For economic costs, there were no statistically significant differences between the groups, and the differences in point estimates were also modest.
Treatment effects on HRQoL improvements, re-operations, and economic cost.
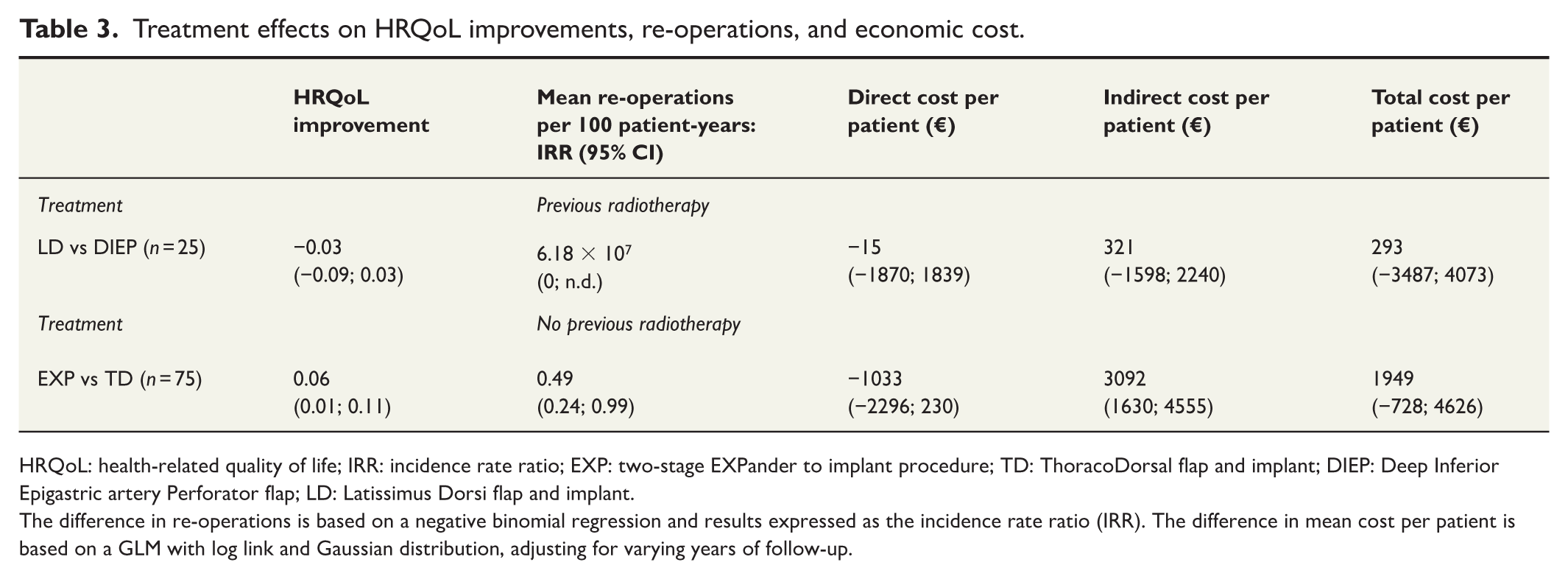
HRQoL: health-related quality of life; IRR: incidence rate ratio; EXP: two-stage EXPander to implant procedure; TD: ThoracoDorsal flap and implant; DIEP: Deep Inferior Epigastric artery Perforator flap; LD: Latissimus Dorsi flap and implant.
The difference in re-operations is based on a negative binomial regression and results expressed as the incidence rate ratio (IRR). The difference in mean cost per patient is based on a GLM with log link and Gaussian distribution, adjusting for varying years of follow-up.
For the not previously radiated group, patients randomized to EXP (vs TD) had a better HRQoL utility development and half the re-operation rate. Patients randomized to EXP had signs of lower direct economic costs but higher indirect costs, where the latter difference was statistically significant.
Discussion
This study compared HRQoL utility value improvements, re-operation rates, and economic costs between different delayed breast reconstruction techniques for previously radiated and non-radiated breast cancer patients, respectively. It is the first study to assess QoL and cost outcomes comparing breast reconstruction techniques, performed alongside an RCT.
For previously radiated patients, the results did not provide particularly clear results in comparing a latissimus dorsi flap (LD) with a permanent implant and a DIEP flap as HRQoL improvements, or lack thereof, and economic costs were similar between the two treatments. There was an implication that patients treated with LD had a higher rate of re-operations, as there were no re-operations in the DIEP group during the follow-up time. It should be noted, however, that the sample size in this comparison was small and only included 25 patients with data to analyze.
In the group of patients who had not received radiotherapy, patients randomized to a one-stage lateral thoracodorsal flap with a permanent implant (TD) had a worse HRQoL development and a higher rate of re-operations compared to patients randomized to a 2-staged expander reconstruction (EXP). The higher re-operation rate also led to slightly higher direct costs with TD, but the difference was not statistically significant, and in contrast, patients randomized to TD had lower indirect costs.
In the present study, patients were separated into groups based on previous receipt of radiotherapy and, based on this, into different reconstructive techniques. A previous study, comparing implant-based reconstruction and DIEP in radiated patients, 17 concluded that the rate of complications in implant-based breast reconstruction in an irradiated field is very high and that autologous reconstruction, therefore, is preferred. This is well known and therefore implant-based reconstruction was not included in the radiated arm in the present study. The use of implants implies a need for long-term revision, and indeed, re-operations and corrections made the LD option more expensive than a DIEP in the radiated arm (Table 2). In the non-radiated arm, an EXP had lower costs than a TD (Table 2). These findings align with previous research concluding that a high complication rate and need for further surgery drive cost. 22 In a previous study, DIEP reconstructions were more expensive as they had a high complication rate.22,23 In the present study, DIEP reconstructions, however, had no re-operations and thus did not drive any additional costs after initial reconstruction. Moreover, the follow-up was longer in the present study, leading to less emphasis on short-term complications and more on long-term revisions.
Previous studies comparing DIEP and implant-based reconstruction have suggested that DIEPs might be the most cost-effective option in patients with a long-life expectancy.24,25 Although the present study was not designed to compare DIEP with implant-based reconstruction, and the two methods were performed in different patient groups, the overall costs (Table 2) indicate that our results corroborate previous findings of the benefits of autologous reconstruction in patients with a long-life expectancy.
Using the point estimates in a simplified cost-effectiveness perspective, disregarding the varying follow-up time with QoL and costs and not adjusting for discounting, for previously radiated patients, LD is inferior to DIEP (due to higher costs and worse health outcomes), and would not be considered cost-effective. For non-radiated patients, the cost per gained QALY for EXP versus TD was €26,589. The threshold for acceptable costs per QALY generally varies between different healthcare systems, and many countries do not have a set threshold. The authors’ assessment of EXP versus TD (€26,589 per QALY) can be compared to US threshold of 50,000 to 150,000 dollars per QALY 26 and the British threshold of 20–30,000 GBP per QALY. 27 In Sweden, the informal threshold is about 500,000 SEK for an intervention in a typical patient population. 28
Strengths and weaknesses
A key strength of the present study is that it was conducted alongside an RCT, making it the first study to compare the quality of life and cost outcomes of breast reconstruction techniques in this way. In comparison, among the previous studies, five relied on modeling approaches using complication rates derived from a non-systematic selection of earlier studies, and two were based on non-randomized clinical cohort studies. 4 While a common limitation of cost-effectiveness studies embedded within RCTs is the typically short follow-up duration, this study has a minimum follow-up of 9.3 years, with an average of 12.9 years and a maximum of 15.3 years. This allowed the analysis to be based entirely on actual long-term data from randomized patients, reducing reliance on external sources and more accurately reflecting real-world outcomes of breast reconstruction. 29
Another strength of this study is the use of patient-reported data on both complications and health-related quality of life, collected from the same individuals. To date, only one previous study comparing the quality of life and cost outcomes of breast reconstruction techniques has incorporated both harms and benefits from the same patient group. 23 In addition, the patient population was relatively homogeneous regarding life expectancy and timing of reconstruction, and the analyses were stratified by radiation status, an important factor often neglected in earlier studies. 4 Several patient-reported outcomes were collected for the patients (BREAST-Q, Rand-36, EuroQoL 5D, and Beck’s Depression Inventory-21), and they have been published separately previously.6,7 In this study, only Rand-36 data were used, as there is a valid method to derive preference-weighted health utilities.18,19
The study also adopted a societal perspective, capturing the full spectrum of long-term costs in a publicly funded healthcare and social insurance system. Only one other study has used a similar approach in a comparable healthcare context. 23
Nonetheless, several methodological study limitations must be acknowledged. First, the inherent challenges of conducting RCTs in preference-sensitive surgical interventions, the relatively low response rate for patient-reported outcomes, 6 and potential variability in defining complications7,30 constitute methodological concerns. In this study, complication definitions were however standardized and applied consistently by the same research team. Furthermore, efforts were made to classify complications according to the Clavien-Dindo system, 7 thereby minimizing bias across study groups. This is an improvement over prior studies, where complication data were often drawn from heterogeneous and inconsistently defined sources. 4
Another methodological limitation is the use of a generic health-related quality of life (HRQoL) instrument to measure benefits. While this is the recommended approach for generating preference-based QALY estimates in cost-effectiveness analyses, 31 generic instruments may lack sensitivity to detect changes specific to breast reconstruction. 22 This limitation has been highlighted in a previous GoBreast study 5 and other cost-effectiveness research on breast reconstruction.22,23 Although some have proposed calculating “breast-QALYs” using disease-specific HRQoL instruments,22,32 this approach remains unvalidated. Such instruments would need to be mapped to generic preference-based measures like the EQ-5D or SF-6D to derive QALYs, 33 but no such mapping exists for breast-specific HRQoL instruments. In addition, the issue of how to discount HRQoL in breast reconstruction cost-effectiveness studies has been discussed. 4 In this study, HRQoL was measured on average 7–8 years postoperatively, 6 reducing the impact of discounting on the results.
Conclusion
Among previously radiated patients, those who underwent DIEP reconstruction experienced no re-operations and a slight, though not statistically significant, improvement in HRQoL. In contrast, patients who received LD reconstruction had no meaningful change in HRQoL and a relatively high re-operation rate. Despite these differences, the direct healthcare costs between the two procedures were similar.
For patients without prior radiation, those who received expander-based (EXP) reconstruction showed a statistically significant improvement in HRQoL and a lower rate of re-operations compared to those who received thoracodorsal flap (TD) reconstruction. Although the TD group showed signs of higher direct healthcare costs, these were not statistically significant, and they showed lower indirect costs. Overall, EXP appeared to provide better value in terms of both outcomes, and there were no statistically significant differences in total costs.
Although the study was not designed to compare implant-based and autologous reconstructions, our findings suggest that the public healthcare system could benefit from prioritizing DIEP reconstruction, due to its lower complication rates and better long-term outcomes. Fewer re-operations translate to reduced surgical burden and more efficient use of healthcare resources.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969261462051 – Supplemental material for Long-term study to assess quality of life and cost outcomes of different delayed breast reconstruction techniques
Supplemental material, sj-docx-1-sjs-10.1177_14574969261462051 for Long-term study to assess quality of life and cost outcomes of different delayed breast reconstruction techniques by Fredrik Brorson, Emma Hansson, Anna Paganini, Anna Elander and Mikael Svensson in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
Not applicable.
Author contributions
FB: Conceptualisation, Methodology, Investigation, Writing – Original draft, Visualisation. EH: Conceptualisation, Funding Acquisition, Methodology, Writing – Review & Editing, Resources, Supervision. AP: Methodology, Validation, Project Administration, Data Curation, Writing – Review & Editing. AE: Conceptualisation, Methodology, Writing – Review & Editing. MS: Methodology, Formal analysis, Writing – Original draft.
Data availability statement
The participants in this study did not provide written consent for their data to be shared publicly; therefore, due to the sensitive nature of the research, supporting data is not available.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by grants from the Swedish Cancer Society (21 0279 SCIA) and the federal government under the ALF agreement (ALFGBG-965161 and ALFGBG-1005048). The sources of funding had no role in the design of the study, data collection, analysis, interpretation, or writing of the manuscript. Open access publication was funded by Gothenburg University, the BIBSAM agreement.
Ethics approval
The study received ethical approval from the Regional Ethical Committee of Gothenburg (#043-08 and T948-17) and the Swedish Ethics Review Authority (#2021-06131-02 and 2022-06234-02). Study procedures were in accordance with the Helsinki Declaration and the Good Clinical Practice guidelines. Data were treated according to the General Data Protection Regulation (GDPR) and the study’s data management plan.
Consent to participate
All participants gave their written informed consent to participate in the study.
Consent for publication
All participants gave their written informed consent to the publication of the results.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.