
Abstract
Using 20 video recordings of Emergency Room treatment and over 5 years of Emergency Room fieldwork data, this study elucidates how interactional processes serve as resources for generating a cultural script of death in Japan called ‘Mitori’. A sudden death at a hospital, in which a patient is removed from their social network, is often considered as the opposite of a ‘good home death’. This study shows how hospital deaths in Japan are strongly interrelated with family participation. After showing the point where medical professionals decide to terminate resuscitation attempts, the analysis depicts interactional steps that shift the definition of environment from a place for treatment toward a place where ‘Mitori’ occurs; that is, a family encounter occurs with a dying patient. Conversation between a doctor and a family member consists of a step-by-step evidence- building story. The final section displays both conversational and physical resources used to establish ‘Mitori’.
Keywords
Introduction
Most deaths in many developed countries including Japan and the United States occur in hospitals. Over 80% of adults die in hospitals in Japan and the United States (Field and Cassel, 1997; Statistics and Information Department,2008). In America, 20 to 30% of adults receive intensive care before they die (Timmermans, 1999). In Japan, 60% of ambulances are dispatched for sudden illnesses including brain and cardiovascular diseases (FDMA (2010), 2009). In 2009 in Japan, among over 11,000 cases of patients with a cardiopulmonary arrest (CPA) condition, the survival rate after a month was 11.4% (FDMA (2010), 2009). Taken altogether, death often occurs in a hospital under crisis circumstances. This may especially occur when a patient arrives with a condition that is no longer manageable by in-home care.
Regardless of this general trend of death, most discussion on death, dying, and end-of-life care presupposes a relatively slow dying process when concerning a ‘good death’ (Ariès, 1974; Kübler-Ross, 1969; Seale, 1998). Within the rather romanticized view of good death, home is viewed as both an ideal place for it to occur and one of the choices that a patient should be given when he or she has time to consider their options (Ariès, 1974, 1981; Kübler-Ross, 1969). Another choice is a hospice, where a patient’s illness is managed without excessive medical treatment (Lofland, 1978). In any case, the good death movement (Ariès, 1974, 1981; Kübler-Ross, 1969) often considers an individual as a choice-maker within the process of death and cherishes a willful decision-making process (Hart et al., 1998). In such discussion, a hospital death is often viewed as a polar opposite and left unspecified (Seymour, 2000; Timmermans, 2005).
This article depicts how death occurs as a process in a Japanese Emergency Room (ER) where family participation is an important component. By uncovering the practices through which death becomes apparent among medical staff and family members, this study attempts to elucidate how interactional processes serve as resources for generating a cultural script of death called ‘Mitori’ in Japan. The ‘Mitori’ cultural script is carefully prepared by the medical staff for the family members of the terminally ill patient in order to create the conditions of a ‘good death’ at the moment of death within the hospital setting in a collaborative, sensitive, and inclusive manner.
Family involvement in a hospital death
Along with emphasizing individualized choice-making, good death and dying is often associated with active family involvement (Hudson et al., 2004; Kristjanson and Aoun, 2004). In the domain of palliative care, the family’s opinion is an important element in the decision-making process (Beder, 2009; Craigie and Meyer, 1990; Fineberg et al., 2011). In other words, family is often considered a key agent for making a decision, especially when a patient is facing his or her death.
A sudden death at a hospital is often considered the opposite of a ‘good home death’ because patients are removed from their social network and family members are isolated during the resuscitation process (Elias, 1985; Seymour, 2000; Timmermans, 1999). Excessive use of medical technology and professionalized practices during the resuscitation process are considered the most medicalized form of human ending (Illich, 1974; Kearl, 1989). In the classic work on emergency departments of county hospitals by David Sudnow (1967), Passing On, the most remarkable finding is the process through which medical professionals ‘create’ a death depending on their perception of patients’ social and moral status such as age. Sudnow’s work is striking, as he reveals the process of how ‘social death’ takes place in a hospital, which was originally suggested by Goffman (1961): professionals treat a patient as dead even though he or she is still clinically alive. Within the process of social death, professionals keep family members removed from a patient (Sudnow, 1967).
Some researchers point out that hospital death is oversimplified and has even been mystified by the critiques in the medicalization, professionalization, and bureaucratization literature, as well as among the good death and dying movements (Seymour, 1999; Timmermans, 1998, 1999). Timmermans (1998, 1999) has done extensive work on emergency medicine and described processes of social death in modern hospitals. He also found a moral hierarchy deployed by medical staff to determine the amount of resuscitation effort. For example, a patient rises in the moral hierarchy when family members are known to or are familiar to medical staff. However, rather than oversimplifying the resuscitation process with critiques against medical professionals, Timmermans (1998) stated that resuscitation technology is used in order to help family members make sense of a sudden death and to convert a sudden death into a more dignified dying process: ‘The resuscitative effort sustains a period of liminality which allows the relatives and friends to prepare for the transition to death if the reviving attempts fails to restore life’ (Timmermans, 1999: 162). Resuscitation technology and its usage among medical professionals creates a more socially appropriate meaning for family members of a sudden death.
Similar to Sudnow (1967) and Glaser and Strauss (1964), Timmermans (1998) claimed that family members are still isolated from the process because the staff consider that ‘it is better for the relatives not to know that their loved one is dying’ (p.468). Timmermans (1998) suggested more active involvement of patients’ relatives during the resuscitation process since it promotes awareness among medical professionals that they are actually dealing with a person who is embedded in a social network. Such suggestions are also made by medical professionals (Chan et al., 2012) and they encourage development of systematic programs for family involvement in the resuscitation process, particularly because some research shows that family involvement assists family members’ bereavement process.
The previous discussion of family involvement in the death process elucidates what are considered appropriate cultural scripts of death. The negativity associated with hospital death often stems from the absence of two things: (1) individual autonomy and (2) family involvement. Family involvement here is treated as one key determinant for constructing a socially and culturally appropriate death. The practices of resuscitation or end-of-life treatment are often explained by using cultural scripts of death (Seymour, 1999; Timmermans, 1998). By considering hospital death as the opposite of a good home death, hospital death itself has been taken for granted and not examined very carefully. This article will discuss how a death becomes accountable and appropriate among medical professionals with the participation of family members in a Japanese ER. The purpose of this study is to describe concrete interactional steps through which family members are involved in the process of death.
Mitori as a practice
The concept of ‘good death and dying’, which became popular in the 1980s in Western countries such as the United States (Kübler-Ross, 1969), has also been adopted in Japan (Hirai et al., 2006; Kimura, 1991; Long, 2004). Some researchers have specified cultural aspects of a good death in Japan (Hirai et al., 2006; Long, 2004; Morita et al., 2004), and family involvement is considered a key factor of good death in Japan due to strong family relationships (Hirai et al., 2006). According to a large-scale survey using a universal scale comparing Japan and the United States (Saito et al., 1996), Japanese families are considered to have high cohesiveness and control over family members’ decisions. In clinical situations, family members play quite active roles in deciding a patient’s treatment plan (Ishikawa et al., 2005; Ruhnke et al., 2000; Voltz et al., 1998). Long (2004) claimed from her cross-cultural description of a good death that ‘family responsibility for care and social continuity was a more dominant theme in Japan’ (p. 926).
Recently, increased emphasis has been placed on home care and home death for patients with terminal conditions in Japan (Long and Chihara, 2000; Okabe et al., 2009). Some use the term ‘Mitori’ as an ideal form of death and dying. ‘Mitori’ literally means taking care of a family member until the end of life and/or being present at one’s death. It signifies an image of a good home death surrounded by family members (Okabe et al., 2009). In addition, it is highly important for a family member to be present at the moment of death. This resembles the Victorian deathbed in Western culture, where a death occurred at home surrounded by family members within a small community (Timmermans, 1998). Okabe et al. (2009) pointed out that this concept of ‘Mitori’ is viewed as ideal but has not quite transformed current practice in modern Japanese society since most deaths occur in hospitals.
In my observations, medical professionals use the word ‘Mitori’ quite differently. Specifically, it refers to a practice of death announcement meaning a medical examination of three signs of life: pupil, breath, and heartbeat. The medical examination is often practiced in front of a family member if he or she can be present, and the medical staff attempt to wait for the family members’ arrival during resuscitation. The term ‘Mitori’ does not necessarily imply home death in its practice, but family involvement in the process of death. This study describes how family members are involved in the process of death interactionally. Applying an interactional approach, the study attempts to capture how participants (medical staff and family members) collaboratively generate the process, which serves as a basis for cultural phenomenon such as ‘Mitori’ in a hospital.
Data and method
My data set consists of 20 video recordings of resuscitation attempts and family encounters in a Japanese emergency department. Over 30 medical staff and 25 family members participated in this research. This research was approved by the human subject committee of the university hospital with which the emergency department is associated. All participants provided written consent to be involved in video recordings. 1
This emergency department is a traumatic care center, so it only accepts patients with life-threatening conditions. It accepts over 2000 patients a year. Among the recordings, 10 cases included death announcements in front of family members and in other cases doctors discussed serious situations with family members at the bedside of patients during resuscitation. All recordings were transcribed for analysis.
This study used a conversation analysis (Sacks et al., 1974) as its primary methodology along with ethnographic observations. Conversation analysis offers an array of analytical concepts that are useful in clarifying what is being achieved through talk (Heritage and Atkinson, 1984; Heritage and Maynard, 2006b, 2006c) and other interactional components such as gestures and bodily arrangements (Goodwin and Duranti, 1992). As Maynard and Clayman (1991) suggested, ethnographic observations allow researchers to have more background knowledge to understand interactions occurring at a research site. Since the emergency department is a highly specialized section, my field observations which lasted for over 5 years from 2006 to 2011, are necessary to make sense of what occurs during resuscitation attempts.
There is an array of research on medical interactions using conversation analysis (Heritage and Maynard, 2006a). Giving bad news, which is especially relevant in this article, is a major research area in conversation analysis of primary care, pediatrics, oncology, palliative care, HIV counseling, developmental consultations, and other healthcare areas (Lutfey and Maynard, 1998; Maynard, 1997, 2003; Peräkylä, 1989). Such studies have identified many interactional phenomena that have both theoretical and practical contributions. This study resides within the same stream of research, focusing on the worst case of providing bad news, in which a doctor has to tell family members about the death of a patient. Death is strongly associated with cultural rituals. By attempting to analyze cultural and interactional practices, this study aims to shed light on how we understand medical practices and specific cultural concepts that are associated with forms of interaction.
In order to depict the continuity of these steps clearly, the following analysis sections deploy the examples from one single case. As will become clear later, the continuity among these steps plays a significant role in establishing a whole process. Even though these examples are from a single case, similar interactional patterns occur quite frequently during each step throughout my data set. The data provided below pertained to the case of a terminal patient who was in her 60s and was volunteering at an elementary school where she suddenly lost consciousness, as she had an aortic dissection (a sudden rupture of an artery). Her daughter accompanied her in the ambulance.
Analysis
To capture the entire process through which a death becomes actualized among participants in a Japanese ER, the analysis shows four steps. The first section shows the point at which medical professionals decide to terminate resuscitation attempts. The second section shows some interactional steps that medical staff take to shift the definition of environment from a place for treatment toward a place where ‘Mitori’ occurs, that is, a family encounter with a dying patient. The third section presents the analysis of a talk between a doctor and a family member at their first encounter. The final section displays interactional steps through which a last examination at the ER occurred.
Decision point to terminate resuscitation
After the arrival of patients with CPA, it is usual that the medical team conducts a resuscitation attempt for about 15 minutes at least. During the resuscitation attempt, medical staff members usually evaluate a patient’s condition every 2 minutes by following a resuscitation protocol. In this case they had already opened an airway with a ventilator and performed chest compression with auto-pulse and a heart stimulant via an IV (intravenous drip), and done the evaluations several times, but the patient did not show any reaction. This is the last point of evaluation they did on this patient, which happened around 15 minutes after the patient’s arrival.
Excerpt 1 6-2-10-1030-A decision made D=Doc, F=Family member, N1=Nurse 1, N2=Nurse 2, P1=Paramedics 1, P2=Paramedics 2, R=Researcher 44 ((alarm sounds, indicating the two minutes have passed since last evaluation of patient condition)) 45 N1: 2分 たち ました::. Nifun tachi mashia::. two minutes pass-PST-POL 46 (8.0) 47 P1: 失礼しま::す. Shitsurei shima::su. impolite do-POL 48 (3.0) 49 P1: (脈)ふれまっせん. (Myaku) fure massen. pulse feel-NEG-POL 50 (0.2) 51 D: まっせん. Massen. NEG-POL 52 P1: (PEA) [で::す. (PEA) [de::su. PEA COP 53 D: [うん, <いいよ, 止めましょう . [Un, <Ii yo, yame mashoo. yes fine IP stop COP-REC 54 (1.0) 55 P2: はい. Hai.
When the alarm goes off, the nurse announces the time, implying it is time to re-check the patient’s condition at line 45. Then she goes to stop the heart compression machine, and about the same time, the paramedic goes to the other side of the bed to check the pulse of the patient at her neck at line 47, while saying ‘excuse me’ to the patient. The paramedic reports at line 49 that he does not feel any pulse. This online commentary (Heritage and Stivers, 1999) announces a sensatory account of the patient’s current condition of no pulse. At line 51, the doctor partially repeats the turn only with the negation ‘cannot’. This partial repeat works to request re-confirmation.
In response, the paramedic adds another description of the patient’s current status as ‘PEA’ (pulseless electrical activity), meaning the heart monitor is showing some electrical activity but without pulse, at line 52. (This PEA condition often happens before the heartbeat becomes completely flat, i.e. a-systole.) At line 53, the doctor gives confirmation, ‘Okay, that’s fine’, and advises other staff that they should stop the treatment. As he mentions this, he also touches the patient’s neck to make sure there is no pulse. After the doctor stops touching the patient’s neck, a staff member goes to turn off the machine alarm, not resuming heart compression.
Within this interactional process the doctor positions himself to confirm the other staff member’s evaluation of the patient’s current condition. In addition, by announcing the end of treatment with directives, the doctor presents himself as a legitimate interpreter of the patient’s bodily signs. This can be read as the doctor being a gatekeeper of life and death (Pelligrino, 1986). Moreover, this is the point at which it became apparent that the patient’s condition was non-reversible and non-treatable; therefore, the death of the patient became a common understanding among the medical professionals.
Transformation of environment: From treatment to ‘Mitori’
This section shows the gradual transformation of the definition of this context from a life-saving one to ‘Mitori’ (family encounter). As Goodwin and Goodwin (1992) suggest, the spatial and temporal arrangement is organized by the participants’ concerted interactional movements, which cumulatively contribute to the shift of context. The shift has to do with the level of mutual involvement and focused interaction that the medical staff demonstrate during interactions (Goffman, 1963). There are seven significant steps through which such a transformation occurs.
1. Shortly after the events of Excerpt 1, the senior doctor picked up a small piece of trash (Figure 1) and threw it into a bin (Figure 2), which was left by the bed by a resident when he was drawing the patient’s blood. During the treatment, the staff usually do not care about these small pieces of trash. This senior doctor’s movement is the first one to signal that now they are in the preparation stage for clearing the place up for a family encounter. Thus, even though it is a small gesture by the doctor, it interactionally marks the beginning of the transformation of the definition of the environment.
Picking up a trash.
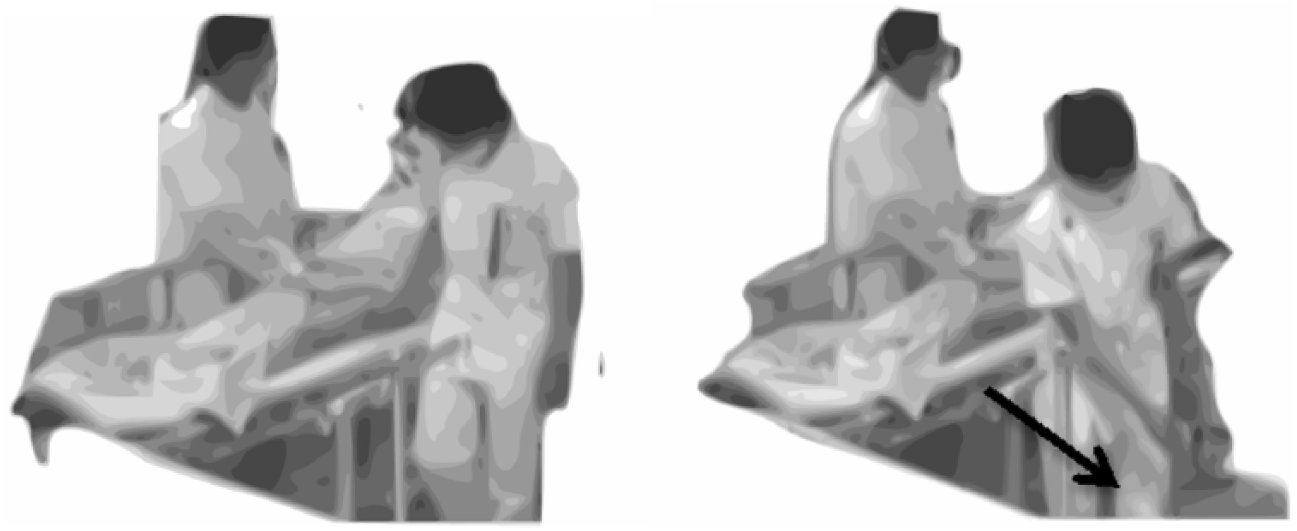
2. Immediately after picking up the trash, the doctor starts asking questions of other staff about details surrounding how the daughter came to the hospital with the patient. While they are discussing the details, the doctor moves the patient’s hand toward her body on the bed (Figure 3). Then he pulls up a sidebar of the bed (Figure 4). This sidebar is usually down during the treatment. Thus, by pulling this up and setting it at the upper position, it clearly marks that they are no longer engaged in treatment.
Sliding the patient’s hand toward her body.
3. Shortly after the doctor finishes discussing with the other staff, he moves away from the bed to write up a medical chart on a desk. At that point, the nurse comes close to the bed (Figure 5) and stops the flow of IV (Figure 6). This movement follows the doctor’s decision to stop the treatment.
Coming close to the bed.
4. After writing up the chart, the doctor comes to examine the patient’s eyes. As he checks the eyes, he announces ‘Doukou wa sandai shiteru tto’ (Her pupils are dilated) and tells other staff that he is going to invite family members to come in, by saying ‘Yonde kimasu ne’ (I will call her in). As he announces that the family encounter is approaching, the doctor closes the patient’s eyes. This is also part of the sign that the examination/treatment is done and the body is being prepared appropriately, here by closing the patient’s eyes, to meet with the patient’s family.
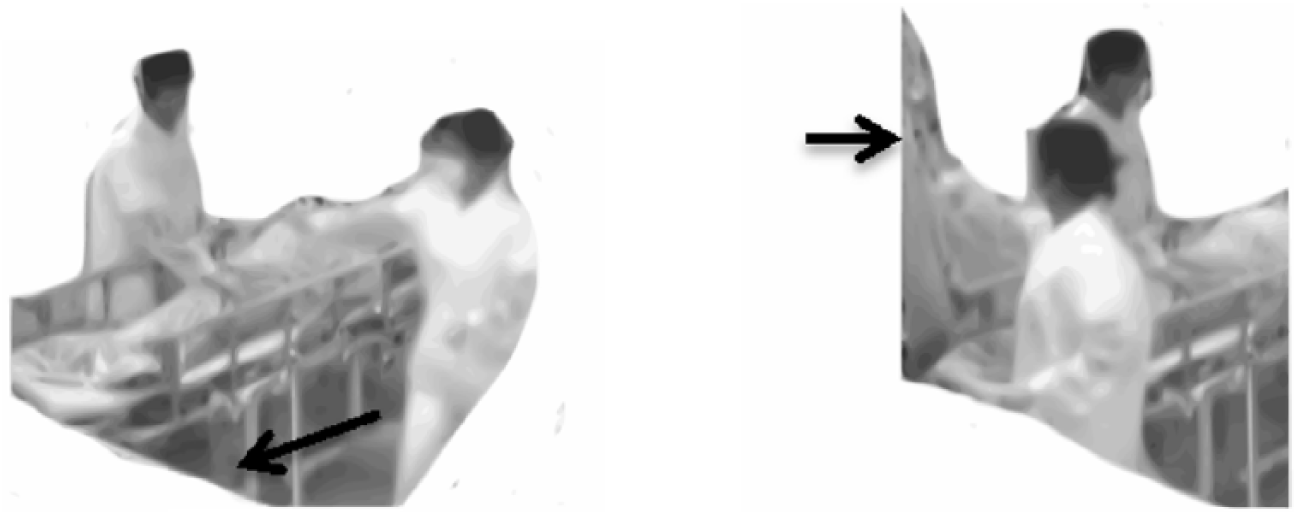
5. After the doctor leaves the ER to talk to the patient’s family, the paramedic approaches the patient’s head and straightens her face (Figure 7) because it was tilted toward the ventilator. Since the treatment with the ventilator has ended, it is no longer necessary for the patient’s face to lean toward it. The straightened angle of the face is thus more appropriate for the family encounter.
Straightening the patient’s face.
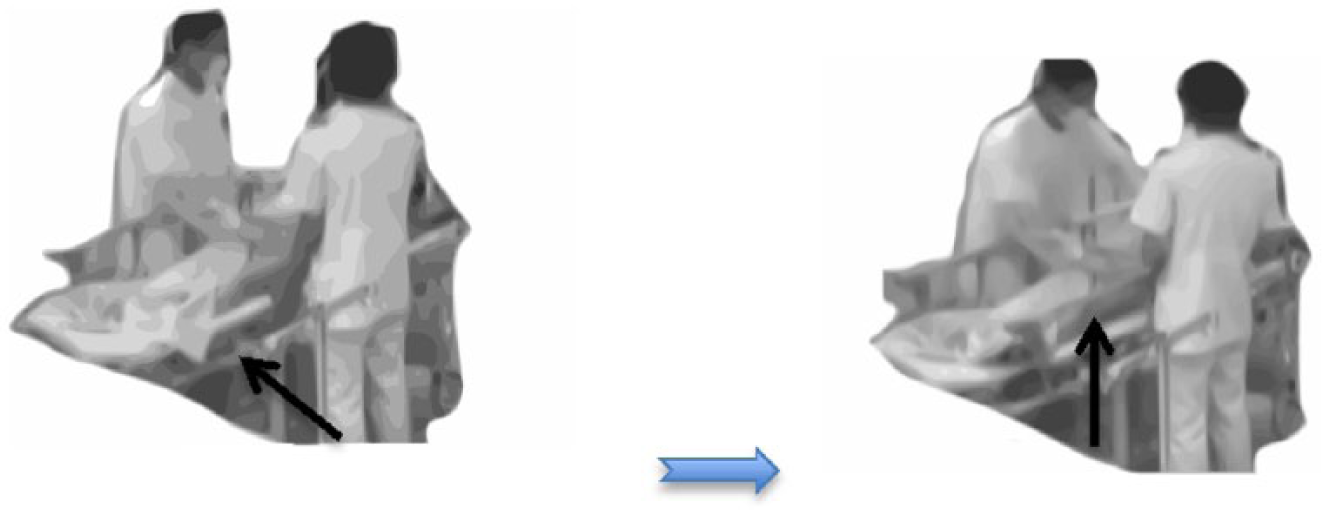
6. Right after the paramedic finishes re-arranging the patient’s head, the nurse approaches the bed (Figure 8) and uncovers the patient’s hand from a blanket (Figure 9). This has a significant meaning because this arrangement allows a patient’s family member to hold the patient’s hand during ‘Mitori’.
Approaching to the bed.
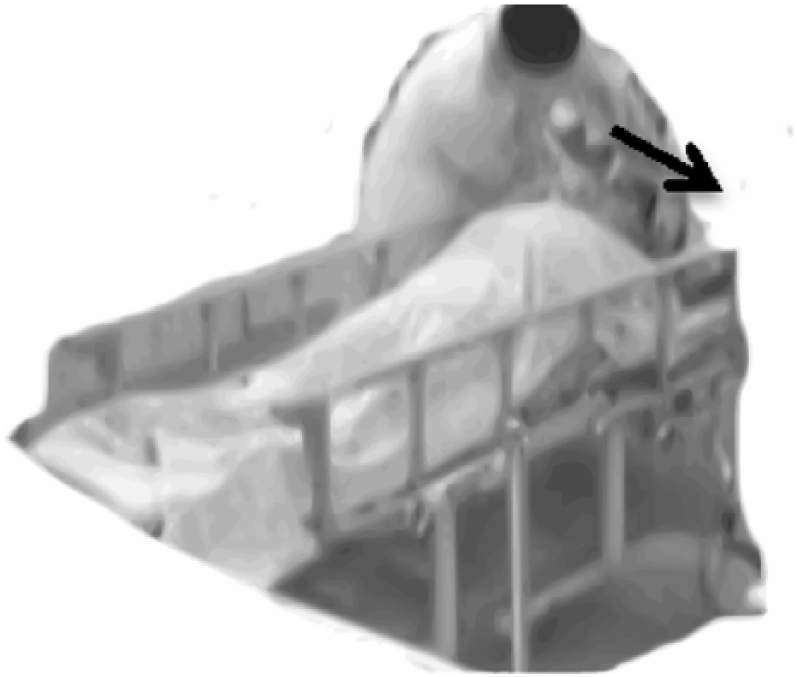
7. Finally, the staff start to move away from the bed and keep the bedside area isolated (Figure 10) – the area is almost reserved for the later family and doctor interaction, that is, making space for the family encounter. This isolation gives the patient a special position. In addition, the staff members hold their hands behind their backs, signaling non-engagement in any activity except waiting for the family encounter.

Moving away from the bed.
These steps are observed quite frequently in my data set, even though the order is not always in this sequence. These arrangements are done step by step to signal the shift in the definition of the environment, from a place of treatment to a place of family encounter. Furthermore, the staff coordinate their movements without explicit verbal exchanges to direct these movements. These spatiotemporal arrangements are done with the participants’ shared anticipation of the family’s involvement in the last examination. In other words, the medical staff are re-arranging the space to make it relevant to the family’s participation in the process of the patient’s death during ‘Mitori.’
Initial explanation to family members
When the ER doctors initiate explanation for family members, it usually takes the form of storytelling (Sacks, 1974; Schegloff, 2000), which was previously described in detail by Kawashima (2017). In the following excerpt, the doctor begins with the description of a past situation when the ambulance arrived at the site (lines 9–13) and then describes with increasing detail what has happened since then and what the staff have done since the patient came to the hospital (lines 15–19).
Excerpt 2 10_06_02_1030_B First encounter (This data was partially presented in Kawashima, 2017) D=Doc, F=Family member(daughter), N1=Nurse 1, N2=Nurse 2, P1=Paramedics 1, P2=Paramedics 2, (Lines 1–8 were omitted while the doctor introduced himself to the family member.) 09 D: あの:: ま:: きゅ- 救急隊 が ね, [00:06:56] ano:: ma:: kyu- kyūkyūtai ga ne, H well rescue crew S IP 10 F: は[い. ha[i 11 D: [あの: 現場 に 到着したときは: 心拍 停止した 状態で[::, [ano: genba ni tōchakushita toki wa: shimpaku teishishita jōtai[de:: H site TP arrive-PST when TP heartbeat stop-PST state CP-and 12 F: [はい, [hai, Yes, 13 D: ま 心臓マッサージ [とか ね そういうこと を され[て:, ma shinzō massāji [toka ne sōyū koto o sare[te:, P heart massage etc IP such thing O do-PAS-and 14 F: [はい. [はい. [hai. [hai. Yes. Yes. 15 D: こちら に 搬送されて [きて, え:: こちら に 来た とき も です ね kochira ni hansōsarete [kite eh:: kochira ni kita toki mo desu ne here to admit-PAS-C come-PL H here to come-PST when also CP IP 16 F: [はい. [hai. Yes. 17 D: やっぱり 心臓 は [動いてない 状態 で, え:- こんすi-= yappari shinzō wa [ugoitenai jyōtai de, eh:- konsui-= as expected heart TP work-NG state and H coma- 18 F: [はい. [hai. Yes. 19 D: =い- 意識 も ない ような 状態 だった ん です ね. =i- ishiki mo nai yōna jyōtai datta n desu ne. consciousness also exist-NG like state CP-PLN-PST N CP-POL IP 20 D: .hh で, 出来る かぎり の そ-蘇生処置 は 行った ん です けれども, .hh de, dekiru kagiri no so-soseesyochi wa okonatta n desu keredomo, and possible utmost LK resuscitation TP implement-PST N CP but 21 心臓 は まったく 動かない ような 状態 で, Sinzoo wa mattaku ugoka nai yoona jyootai de, heart TP absolutely work-NEG such state CP-and 22 今後 これ 以上 処置 を 続けて も, 身体 に, kongo kore ijyoo shochi wo tsudukete mo, karada ni, from.now.on this more treatment O continue even body to 23 F: はい. Hai. 24 D: え:: 傷 を 付ける だけ [に なって しまう ん です ね.= Eh:: kizu wo tsukeru dake [ni natte shimau n desu ne. Uhm hurt O give only to become:TE N CP IP 25 F: [はい. Hai. 26 F: =はい. Hai. 27 D: で, ちょっと⎕ これから⎕ ⎕最後⎕の⎕⎕診察⎕ ⎕を⎕⎕ します⎕⎕ ので[:: De, chotto korekara saigo no shinsatsu wo shimasu node[:: and a.little from.now.on last LK examination O do-POL because 28 F: [はい. Hai. Yes. 29 D: 大変 つらい ん です けども, ちょっと, 最後に ね, taihen tsurai n desu kedomo, chotto, saigoni ne, hard paiful N CP but a.little lastly IP 30 D: 付き合って いただけます か? Tsukiatte itadakemasu ka accompany do-PAS-POL Q 31 (1.0) 32 F: すいません.((泣き声?)) Suimasen.((sobbing?)) (0.8) 34 F: 診察. [00:07:34] Shinsatsu. (0.8) (a few lines are omitted, which discuss paper work) 39 F: それ は 家族 が やっぱり 見てた ほう が いい ん です か. Sore wa kazoku ga yappari miteta hoo ga ii n desu ka. that TP family S as.expected seeing-PST side S good N CP Q 40 D: そうですね. Soo desu ne. so CP IP
Within the doctor’s storytelling, there are some ‘flags’ (Goffman, 1981) that display the doctor’s understanding of the situation. For example, at line 17, the doctor uses a word ‘yappari’ (as expected) to describe the non-responsiveness of the patient regardless of their treatment. This word conveys his supposition of the patient’s condition and helps the family member to recognize the hopeless nature of the situation. In addition, at line 21, as the doctor describes the current heart condition of the patient, he uses extreme case formulation (Pomerantz, 1986) with ‘mattaku ugokanai’ (not working at all). This also signals the doctor’s understanding of the irreversible condition of the patient.
During the first part of the doctor’s explanation, the family member gives the continuer ‘Yes’ quite frequently (at lines 10, 12, 14, 16). However, after line 18 the family member withholds the continuer even at points where it is relevant to do so, such as after the doctor’s turn at lines 19 and 20. These points are not Transition Relevant Places (TRP), since the doctor is engaged in the multiple turn unit (i.e. storytelling). Yet the continuers from the family member (at lines 10, 12, 14, 16) show her active engagement in the telling. By contrast, the family member shows her resistance toward moving forward in the storytelling by withholding these continuers after line 18. In other words, the family member shows her understanding of this irreversible condition of the patient through this change in her reaction.
After the doctor mentions the patient’s prognosis, indicating at line 22 there is no positive future for the patient, the family members respond with ‘yes’ at line 26. Then the doctor extends the invitation for a ‘last examination’ to the family member at line 27. The family member hesitates to join the examination by questioning the necessity of participating at line 39, yet the doctor encourages it at line 40. The phrase ‘last examination’ is used here in place of the ‘death announcement’ and it conveys the definite, non-negotiable situation of the patient for the family members. By extending the invitation and confirming the necessity of the family member participating, the doctor displays the relevance of family participation to finalize the process for the patient.
As a whole, this first encounter has the conversational form of storytelling. By doing so, the doctor gradually brings the family into the course of events that occurred concerning the patient (Maynard, 2003). This storytelling functions in a similar manner to a perspective display sequence (Maynard, 2003), which is also reported to be an effective technique for eliciting decision-making discussion during life-sustaining treatment in the United States (Pecanac, 2016). In this case, the end of the story is not something negotiable. Hence, by taking the family member through the whole process as a story, the doctor not only explains the inevitability of the situation but also legitimizes his decision-making process.
Last examination
The final part of the ‘Mitori’ process can end with family participation at the site of the death announcement. Let me first focus on the conversational aspects of this last examination before describing some features of bodily arrangement.
Excerpt 3 10_06_02_1030_C Last Examination D=Doc, F=Family member, N1=Nurse 1, N2=Nurse 2, P1=Paramedics 1, P2=Paramedics 2, [00:06:49] 51 D: じゃ, これから 最後 の 診察 を します. Jya, kore kara saigo no shinsatsu wo shimasu. INJ this from last LK exam TP do-POL 52 F: はい. Hai. 53 (44.0) ((Doc first removes a respirator, examines her chest, and then checks her pupil.)) 54 D: あの::生命兆候 で ある 対光反射 が ない と いう こと と, Ano::seemeichookoo de aru taikoohansha ga nai to iu koto to, that life sign CP exist light.reflex S not QT say thing and 55 F: はい. Hai. 56 D: 自分 で 呼吸 を して ない と いう こと と, Jibun de kokyuu wo shite nai to iyuu koto to, herself by breath TP do-NEG QT say thing and 57 D: 自分 で 心臓 が 動いて ない って こと です ね. jibun de shinzoo ga ugoite nai tte koto desu ne. herself by heart S work NEG QT thing CP IP 58 F: はい. Hai. 59 D: で, こちらの時計で10時51分ですね. De, kochira no tokee de jyuuji gojyuu ippun desu ne. Then this LK clock by ten fifty-one CP IP 60 F: はい. Hai. 61 D: 死亡⎕⎕を⎕確認⎕⎕ しました. ((Doc bows to her daughter)) Shiboo wo kakunin⎕shimashita. death TP confirm⎕do-PST 62 F: お世話になりました.((頭を下げながら)) Osewaninarimashita. ((bowing)) thank.you.very.much-PST 63 F: 色々ありがとうございました.((一歩下がって向きを変え頭を下げながら)) Iroiro arigatoo gozaimashita. ((One step down)) in many ways thank you very much-PST (0.8) ((Daughter moves one step to her left)) 65 F: お手数をお掛けいたしました.((頭を下げながら)) Otesuu wo okakeitashimashita. ((bowing)) trouble TP impose-POL-PST
The doctor first examines three points – the patient’s heartbeat, breath, and pupils – right in front of the family member. Then he tells the family member the result of each examination at lines 54, 56, and 57. Then the family member registers each description. It can be heard as a diagnosis when he announces the patient’s death at line 61. These descriptions move almost like syllogisms, which Gill and Maynard (1995) suggest as part of syllogism diagnosis. The doctor conveys a list of evidence and shows the conclusion drawn therefrom. In addition, each description functions almost like an online commentary (Heritage and Stivers, 1999) by describing what the doctor is seeing/hearing, which shapes the recipient’s expectations during the physical exam by increasing the demonstrative nature of evidence. Overall, it enhances the legitimacy of the conclusion, which is the announcement of the patient’s death through the arrangement.
Furthermore, instead of a purely verbal and more clinical report of the patient’s death, these reports are done in front of the family member. The doctor suggests looking at the clock as he announces the time of death, and the family member also follows his gaze. This also encourages performative mutual engagement in the event. These arrangements add further demonstrative proof, and the family member here is treated as a very relevant part of establishing the whole process.
Let me also point out that during the last examination the family member begins to hold the patient’s hand, which was uncovered from under a blanket by the nurse as shown in Figures 8 and 9. The family member shakes her hand a little bit while the doctor was performing the above examination. Thus, the patient’s body is divided into different social fields (Goodwin, 2003) in a way that a patient is treated not only as an object of examination by the doctor but also as a beloved mother by the family member. This poses very different social statuses of the patient’s body. The last examination with the family member’s participation allows the patient to embody multiple social meanings during the event.
Finally, as the doctor pronounces the patient’s death, all medical staff bow together toward the patient and the family member. This is done almost as a demonstrative apology for not having been able to save the patient’s life and as an expression of sorrow for the patient’s death. It is very rare for medical professionals to verbally express such emotions, but this physical expression is done as a default ritual during the ‘Mitori’.
In response, the family member bows back and says ‘Thank you very much’ twice – almost bowing toward each staff member. The family member’s appreciation shows that she accepts the death of the patient as demonstrated by the doctor. Although bowing has various meanings in Japanese culture (Morsbach, 1988), this participation of family member and hospital staff member strongly demonstrates their mutual engagement in finalizing the process.
More importantly, this shows that the whole process of establishing a patient’s death is now complete and registered by all participants. Moreover, the completion of death is presented along with the appropriate social expression of emotions associated with the patient’s death. Even though the patient’s death poses different social and emotional meanings for different participants, the emotions are here demonstrated in a restricted manner as the ‘Mitori’ participants bow to each other. This set of actions is done ritualistically and constructs this scene as one of collective mourning of the patient’s death.
Conclusion
As we have seen, family participation is a crucial part of the interactional process of constructing a patient’s death in the Japanese ‘Mitori’ process. Within my data, after the hospital staff decides to cease resuscitation efforts they start re-arranging the spatiotemporal organization of the ER to prepare for the family’s encounter with the patient in a way that allows appropriate interactions between the medical professionals, family members, and the patient. In addition, the doctor tells the family member the bad news in the form of a story that enhances the legitimacy both of treatment and of the patient’s death itself. More importantly, the last examination with the family member offers undeniable proof of the patient’s death for the family member, since the death is effectively completed as well as confirmed by mutual engagement among medical staff and family members.
According to Timmermans (2005), Health care provides relatives with a cultural script of how to behave and what to expect in the dying process. The script socializes patients and relatives to die well: with dignity, naturally, quickly without realization or slowly with time to say good-byes, or while everything medically has been done to keep patients viable but not so much that suffering ensued. (p. 1006)
Such a cultural script is apparently present in my analysis. The medical staff are oriented to forming a place for ‘Mitori’, which creates a culturally appropriate moment for family members to meet their loved one.
However, the cultural script of death is established, managed, and re-organized through a conversational structure and locally managed spatiotemporal organization at the place of death. The interactional establishment of a death in the ER provides a basis for the cultural appropriateness of the death, and family involvement is a relevant and crucial aspect of the whole process. As suggested by Peräkylä (1998) and others (Heritage, 2005; Lutfey and Maynard, 1998), the interactional organization of medical practices provides foundations for medicine’s cultural authority (Freidson, 1970), which apparently has a powerful presence in the realm of death and dying (Timmermans, 2005). Instead of explaining such family involvement with a simple reference to Japanese death culture, this article has suggested that interactional arrangements in the process of death at a hospital create resources for generating culturally appropriate scripts for encountering and coping with a death.
Footnotes
Appendix 1
In this article, the transcription notation is based on the commonly used Jefferson system. For the abbreviation used in word-by-word gloss of Japanese transcripts, please refer to the following notations:
Acknowledgements
I would like to express my sincere appreciation to all participants in this study, especially the families who lost their loved ones and still agreed to participate. I would also like to devote this paper to Dr. Candy Goodwin and Dr Charles Goodwin who continually supported me in completing this paper. Part of this paper was presented at International Conference of Ethnomethodology and Conversation Analysis, in Manchester, England, in 2011.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by JSPS KAKENHI grant numbers 16H03090 and 16K04133.