
Abstract
This article analyzes the viability of utilizing a new performance-based development financing model related to funding medical equipment technology (MET) transfers to developing countries. In such an innovative model utilizing market-based incentives and public–private partnerships (PPPs or P3), social bond investors fund MET by receiving a social development ‘bond’ in exchange for a predetermined and agreed-upon amount of principal and interest to be paid only if the related MET project is deemed to satisfy certain predetermined, agreed-upon success metrics (as determined by a third party). Thus, the public sector only funds MET projects that are deemed successful based on the agreed success metric by all related stakeholders, with the MET transfer project being funded no matter what the circumstance. This performance-based model can complement existing funding models, which improves the transparency, coordination and efficacy of such MET development assistance projects in developing countries.
Keywords
Introduction
Individuals in economically disadvantaged countries and regions often experience shortages of essential medical equipment technology (MET) to meet health care needs—due to lack of funding and funding models—leading to a non-optimal equilibrium.
Insufficient MET is deemed as a main contributor to the poor quality of health care in developing countries. Recent statistics suggest that many people are disadvantaged due to the MET discrepancy between developed and developing countries. According to the Baseline Country Survey on Medical Devices, eight out of 134 countries do not have at least one computer tomography (CT) scanner per million inhabitants (WHO, 2011a).
Ineffective use and subsequent poor operational performance of MET is another related issue affecting health care quality in developing regions. Despite recent progress, numerous segments of the population in developing regions do not have access to adequate health care. The economic consequences of poor health, directly and indirectly, contribute to the economic burden carried by many in developing regions (Remmeizwaal, 1997). Dr Margaret Chan (the World Health Organization (WHO) Director General) stated that the medical device industry holds great promise for public health, sometimes spectacular promise and sometimes seductive promise (WHO, 2010).
Medical or health technology generally ‘refers to the application of organized knowledge and skills in the form of devices, medicines, vaccines, procedures and systems developed to solve a health problem and improve quality of lives’ (WHO, 2015), which includes ‘pharmaceuticals, devices, procedures and organizational systems used in healthcare’ (INAHTA, 2015). Brown et al. described medical equipment simply as being ‘…the equipment which may be found in hospitals, medical research and teaching institutions’ (Brown, 1986: i, cited by Gedel and Gablah, 2014). Remmeizwaal also noted that ‘the term “medical equipment” can be interpreted as including a wide range of instruments, equipment, machinery or apparatus used for medical and para-medical purposes’ (Remmeizwaal, 1997: 4). These definitions include the entire range of mechanical, electrical and electronic devices used, directly or indirectly, for the delivery of health care. Such technologies could also include devices that improve millions of peoples’ lives, such as wheelchairs, hearing aids, eyeglasses, pacemakers and prostheses (WHO, 2010b).
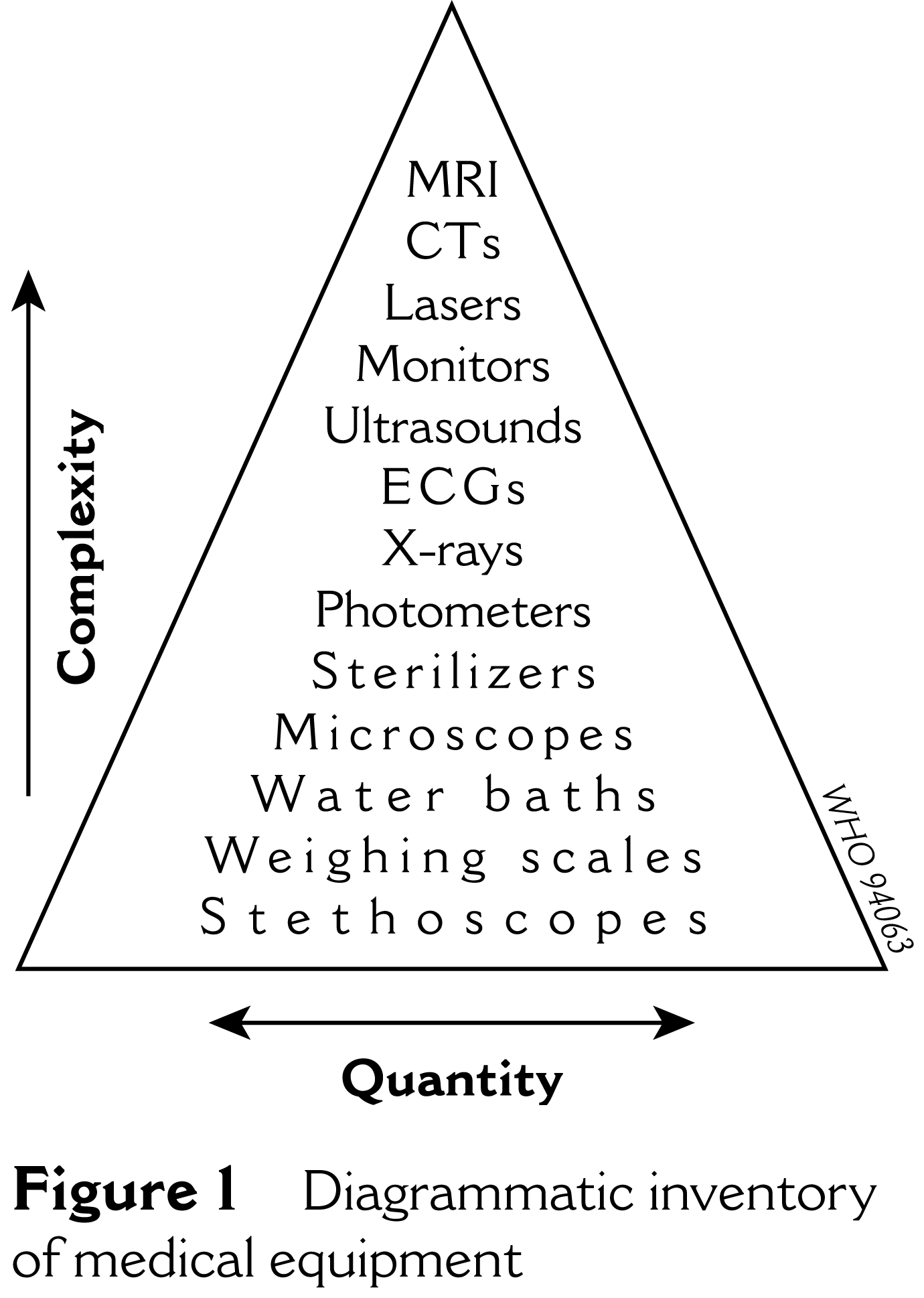
According to Cheng (1994), MET of simple equipment greatly outnumbers complicated items (which the pyramid schematic below denotes (Figure 1)).
Diagrammatic inventory of medical equipment
Thus, if lack of much-needed MET funding exists, what is a creative alternative funding model to resolve such a problem?
This article, composed of four main parts, attempts to provide a creative market-based solution in the form of social impact bond (SIB) funding. The article’s first section describes the current medical equipment ecosystem as it relates to developing countries. The second section overviews the specific funding challenges to importing MET to developing countries. The third section analyzes the existing traditional conceptual frameworks related to MET funding for developing countries focusing on simple donations and project financing models. The article’s fourth section proposes a new performance-based development financing model utilizing SIB funding that leverages market-based incentives and public–private partnerships (PPPs or P3) to fund the needed METs to developing countries.
This article asks two important research questions. First, what are the current existing funding structures for MET transfers to developing countries? And second, how can such existing funding structures be complemented through the use of social finance utilizing SIB funding? The article argues that, although still in its early stages, performance-based development funding for MET utilizing SIB models can represent a viable, transparent, sustainable and highly optimal financing model to assist developing countries in receiving MET. In doing so, this article creates an interlinkage between MET funding needs (i.e., the demand for MET and funding to secure MET by developing countries) and SIB structural models (i.e., the supply of scarce funding utilizing a performance-based PPP framework to secure MET for developing countries). Such interlinkage constitutes a unique contribution to the existing literature that will be beneficial for both scholars and practitioners.
Medical equipment technology transfer challenges to developing countries
Funding and transferring MET to developing regions have led to the specific problem of suboptimal MET outputs. The common problems are as follows.
Insufficient volume of medical equipment: The main issue is that the total stock of MET is inadequate for developing countries or regions in comparison with high-income, developed countries and regions (Remmeizwaal, 1997: 7). Donors are at times reluctant to provide MET to developing countries and regions due to poor infrastructure while recipient countries are often not able to purchase such MET due to the recipient’s relatively low government expenditure on health care (WHO, 2010b). According to Nimunkar et al. (2009), 86 per cent of the world’s population spends $6 per capita on MET as compared to $290 per capita spent by developed countries.
Improper maintenance of medical equipment: MET equipment received by developing countries are not always fully optimized due to poor infrastructure including a shortage of power supply, roads, purified water, facilities, spare parts, health workers and limited training capacities (Bonair et al., 1989; WHO, 2010b). For example, 20–40 per cent of the MET equipment stock is not operational, and 60 per cent of the equipment in medical units in developing countries is unusable (Remmeizwaal, 1997: 7). According to Perry and Malkin (2011), an average of 38.3 per cent of MET equipment in developing countries is out of service due to lack of training, health technology management and related infrastructure.
Unequal distribution of medical equipment: MET equipment received in developing countries is often focused on urban areas where health care facilities are more readily available. About 40–60 per cent of the health budget in Africa is spent on a select group of hospitals located in (non-rural) capital cities (Remmeizwaal, 1997: 7).
Maladoption of medical equipment: Many MET devices in low-resource settings, which were imported or donated from industrialized countries, do not function properly due, in part, to the importation and transfer of Western medical paradigms (Bonair et al., 1989; Salicrup and Fedorkova, 2006; WHO, 2010b). As such, the health care needs of developing countries and the allocation of related MET equipment cannot bring about its full intended effect since donors fail to fully consider the relevant local environment, such as cultural, social, economic and institutional factors.
When considering the design aspects of MET equipment, Nimunkar et al. (2009) suggested cost-effective and local-friendly MET with some conditions – namely, accuracy, reliability, durability, portable size and weight, available materials, power requirements, ease of manufacture, language issue, facilities available and population dynamics (Nimunkar et al., 2009). Examples of MET that could be effectively used for developing countries include: (1) Jaundice treatment (jaundice afflicts more than 13 million babies every year, with more than 9 million living in developing countries.), (2) Jairpurknee (high-tech prosthetic limbs that in many ways represent a technology upgrade over previous prosthetic alternatives in the market now (Popular Mechanics, n.d.)), (3) Leveraged wheelchair (wheelchair users in developing countries often need chairs that can function on rough terrain, with field tests conducted in Kenya, Uganda and Tanzania in 2009, and second-generation designs in Guatemala (Popular Mechanics, n.d.)) and (4) Mobile phone and/or PC-linked medical diagnostic devices (by having greater access to a mobile phone, patients and medical professionals can benefit from greater connectivity without travelling long distances (National Science Foundation, March 27, 2012)).
Pre-SIB funding frameworks for funding to developing countries
Donations
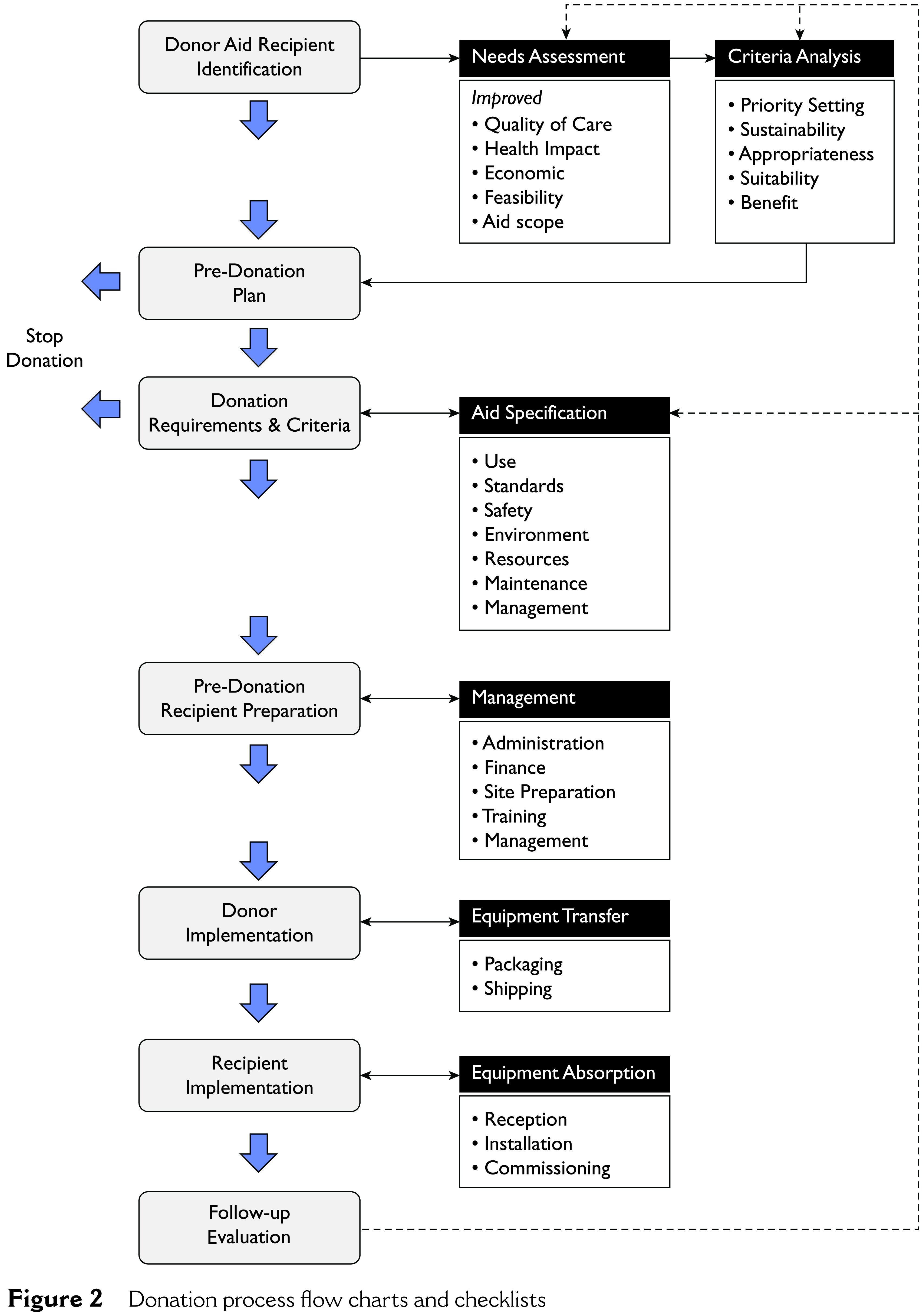
MET has traditionally been provided through donations to developing countries and regions. The WHO has produced a guideline on this, which notes that: (1) health care equipment donations should benefit the recipient to the maximum extent possible, (2) donations should be given with due respect to the wishes and authority of the recipient, and in conformity with government policies and administrative arrangements of the recipient country, (3) differences should not exist in terms of equipment quality and (4) effective communication should exist between the donor and the recipient, with all donations made according to a plan formulated by both parties (WHO, 2000: 1).
Below is the donation process of medical equipment presented in the WHO guideline (Figure 2).
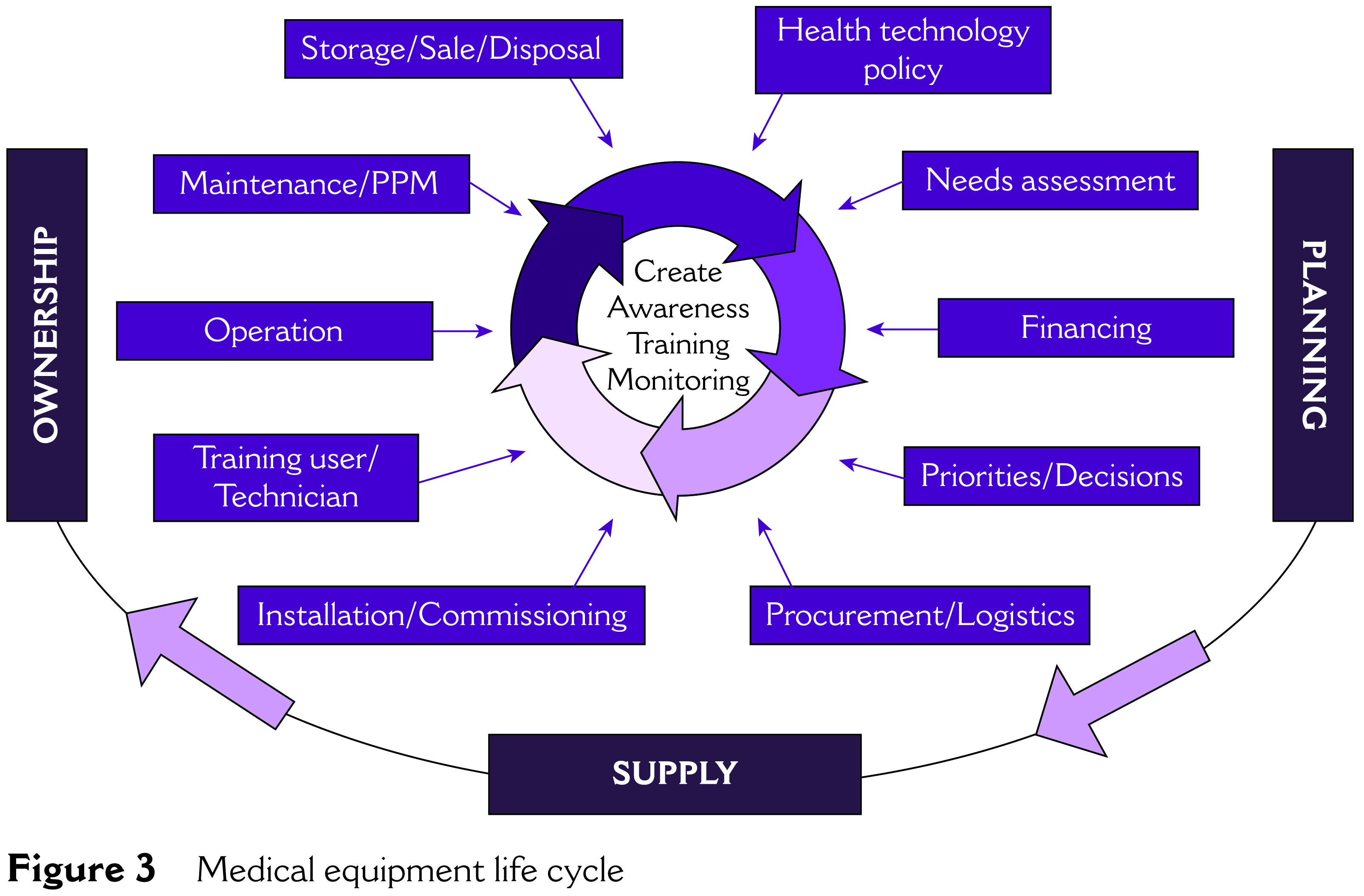
As one framework used in a developing country in Asia, the Bangladesh Medical Equipment Survey provided a ‘Medical Equipment Lifecycle’ related to effective MET management (See Figure 3) (Simed International, 2008).
Another example of donations to developing countries is from the World Bank, which provided MET to the developing country of Croatia (see Table 1).
Project financing
Separate but related to MET donations, project financing has represented a recent traditional financing model for some donors to achieve certain stated objectives for MET equipment transfers to developing countries. According to the International Finance Corporation (IFC), project finance helps finance new investments by structuring financing around the project’s own operating cash flow and assets, without additional sponsor guarantees. The technique is able to alleviate investment risk and raise finance at a relatively low cost, to the benefit of both the sponsor and investor. Thus, the advantages of project finance are (1) increasing the availability of finance and (2) reducing the overall risk for major project participants (IFC, 1999).
Bond (2012) proposed the use of project finance as a means to attract financing from domestic banks and institutional investors. Project financing focuses on the problem of fiscal autonomy and insufficient fiscal transfers from the central government that have left local governments with few resources to finance MET development projects. The project finance MET framework involves local governments (as well as other locally based entities) that work with donors and private sector companies in a PPP to identify and put together bankable infrastructure projects that can be financed by local banks and capital markets on a non-recourse basis.
Donation process flow charts and checklists
Medical equipment life cycle
The World Bank MET Project overview
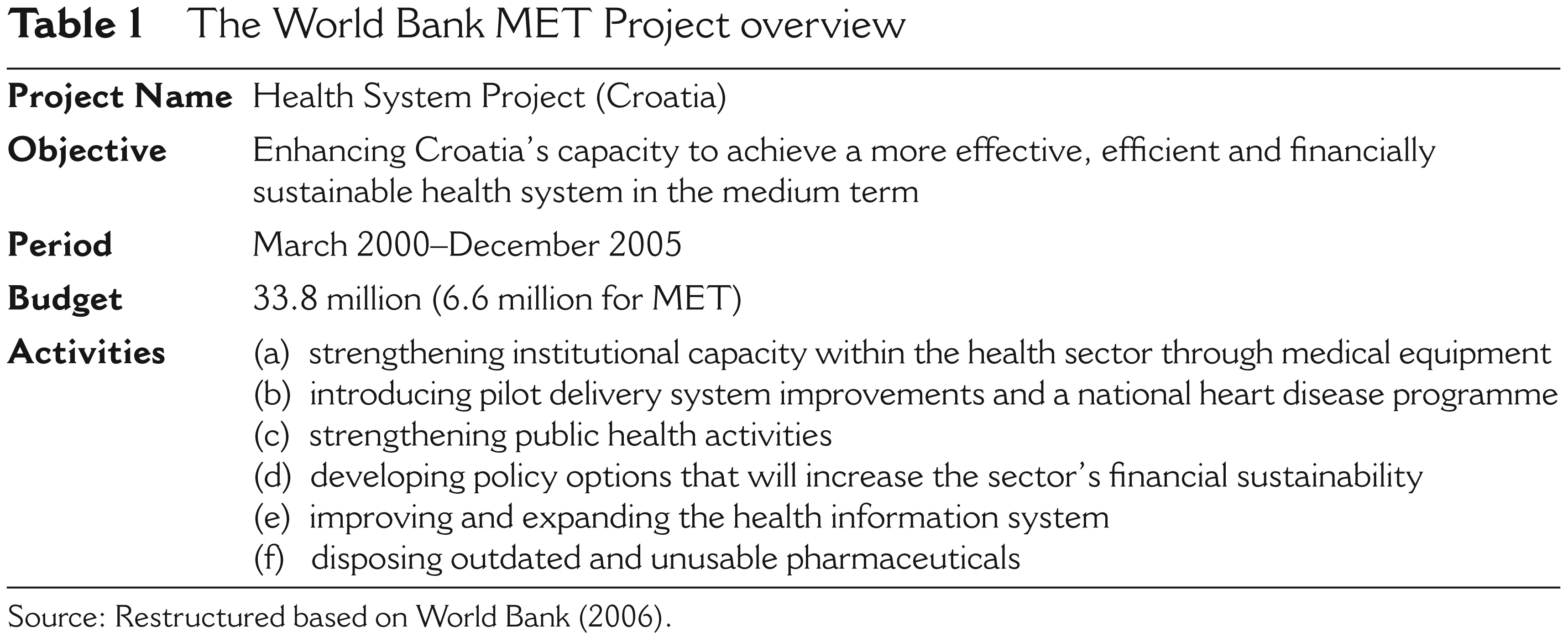
Source: Restructured based on World Bank (2006).
Despite some of the benefits of project financing, Schieber et al. (2007) analyzed the basic financing challenges facing low- and middle-income countries (LMICs) as a result of revenue generation and collection constraints, increasing flows of development assistance for health, donors’ concerns regarding aid effectiveness and the economic difficulties facing many LMICs as a result of globalization and poor economic management. Meanwhile, other new and relatively large global funding sources’ players have also entered as potential new players in MET transfers, such as the Bill and Melinda Gates Foundation; the Global Fund to Fight AIDS, Tuberculosis and Malaria; and the Global Alliance for Vaccines and Immunization (GAVI) vaccine fund. However, notwithstanding the rise of such new players, a lack of effectiveness, optimal results and harmonization still exists within the global community because of the different accountabilities of the various multilateral and bilateral organizations, global funds and alliances as well as private foundations.
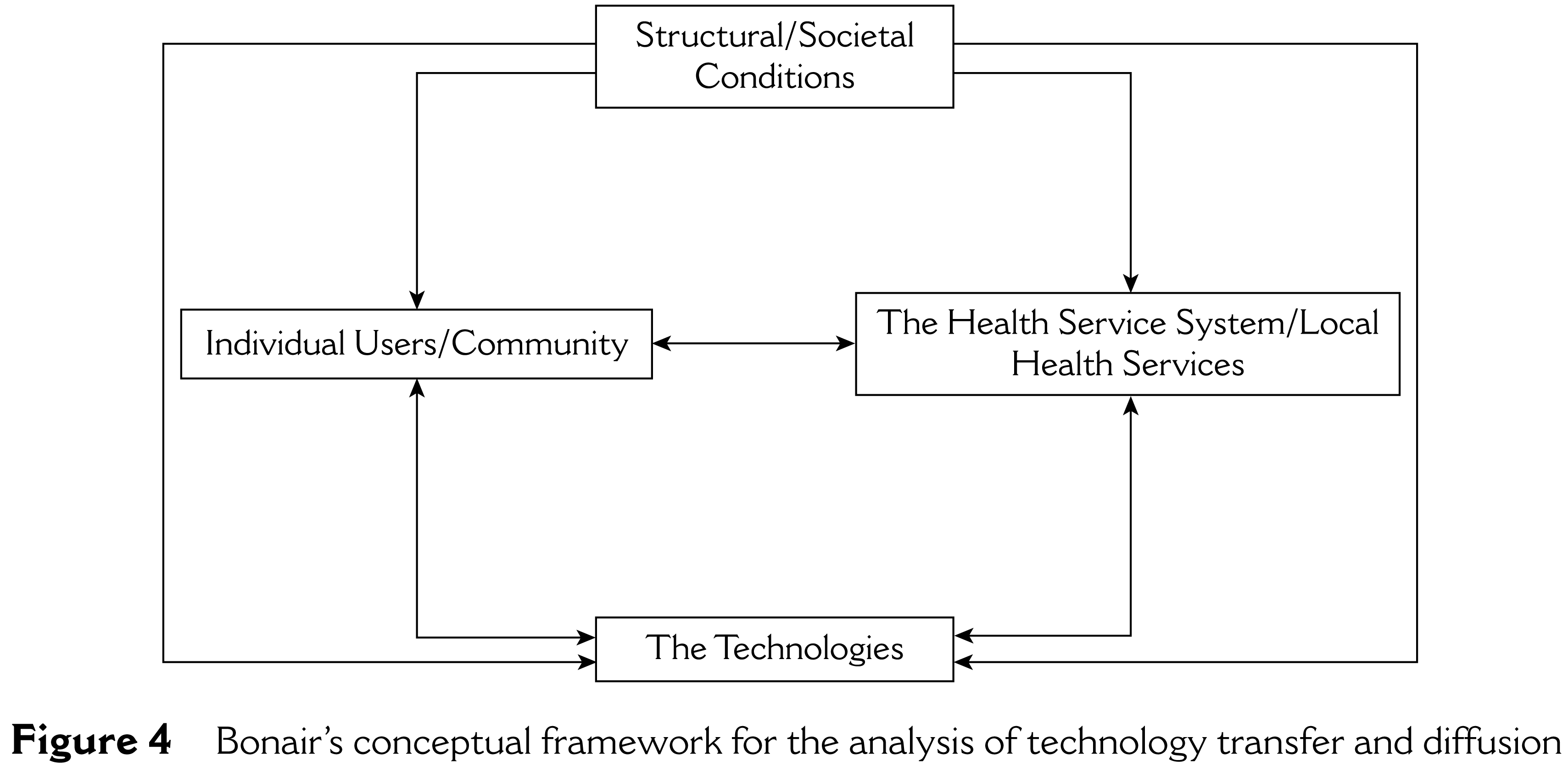
As possible remedies, Lee and Eom (1989) suggested three criteria for successful project financing: (1) minimization of political risks, (2) minimization of market risks and (3) maintenance of an acceptable range of debt–equity ratios. Bonair et al. (1989) also sought a more comprehensive approach involving a conceptual framework for the analysis of technology transfer and diffusion—incorporating cultural, social, economic and institutional factors in the developmental phases of technology transfer—which could include MET transfers to developing regions (See Figure 4).
To mitigate and improve on some of the limitations related to MET financing models for developing regions described thus far, the next section argues that the use of ‘social impact bonds’—a subset in the field of social finance—could serve as a form of innovative market-based mechanism and conceptual MET funding framework. The specific structure and explanation of SIBs is explained in the next section below.
Bonair’s conceptual framework for the analysis of technology transfer and diffusion
Performance-based financing for medical equipment technology: Applying social finance and the social impact bond conceptual framework
Because a lack of funding for MET transfers represents a major problem facing MET funding and transfers to developing regions, this article proposes that the SIB conceptual framework can represent a viable alternative that aims to be more transparent, efficient and optimal than previous and existing MET funding frameworks.
At the conceptual level, social finance techniques offer a unique performance- and incentive-based method in which the relevant stakeholders to one or more particular social assistance projects are several actors unified as one cohesive unit, which represents a new type of performance-based PPP (‘Performance-based PPP’ or ‘P4’). This is accomplished through the shared interests of the various stakeholders involved, which have verification elements embedded in to ensure that assistance gains are verifiable, transparent and sustainable (Kim and Kang, 2012).
At the micro-level perspective, SIB is implemented for a particular project or group of persons (‘constituency’, which represents one of the structure’s stakeholders) (Evans, 2012; McKinsey & Co., 2012). Such constituency typically would require the need for a specified improvement in an effort to rectify a particular social objective, and one that has traditionally needed and been served by public funds (or non-governmental organizations (NGOs)), such as to improve designated health levels, equipment for persons with disabilities, medical education and training, as well as the building of MET infrastructure (such as hospitals and related medical and MET facilities) (Evans, 2012). However, in theory, a much broader constituency and/or assistance projects could exist. Another SIB component is the (social) ‘service provider’ that would provide the assistance, programme or other related effort on behalf of the constituents. Often, but not always, the service provider is a civil society organization (CSO) or the state, acting separately or collectively (Kim and Kang, 2012).
Similar to traditional medical financing methods, the social-finance-driven SIB structure requires the need for investors. However, unlike traditional finance investors—which focus primarily on maximizing economic returns—in the social finance SIB structure, the typical social finance SIB investor would be a ‘social impact investor’ (an investor that takes into consideration social as well as financial impacts related to the investment made for a particular assistance programme). Although not much transactional history in the SIB market exists, the impact investor may include, but not be limited to, private sector entities, state actors, non-profits, philanthropic organizations and/or charitable entities (Evans, 2012).
The next stakeholder in the medical technology transfer and equipment SIB structure is the ‘intermediary’ that serves as the hub that connects the various stakeholders involved (McKinsey & Co., 2012). The intermediary would most likely be a private sector financial institution (although public sector entities with relevant expertise would also be possible) that has the requisite experience in dealing with similar (but not necessarily identical) legal and financial structures and issues. For instance, a financial institution that has had experience dealing with structure products involving asset-backed securities (ABS) or special purpose vehicles (SPVs) may already have some broad familiarity with those existing already related to SIBs (Kim and Kang, 2012). In a typical ABS structure, somewhat similar to the SIB structure, a financial intermediary sets up an entity that issues structured bonds to investors (Jobst, 2007).
External evaluation ‘advisors’ are also part of the SIB-based medical technology transfer and equipment funding structure, which provide guidance and advice relating to setting and implementing the SIB’s performance criteria (metrics), particularly between the service provider(s) and impact investors. An independent ‘evaluator’ is also employed in the process. It is the evaluators’ mandate, as objective independent evaluator on an arms-length basis, to determine whether or not the SIB has met its stated objectives. If the independent evaluator’s conclusion is ‘yes’ to the stated objectives—based on predetermined and contractually agreed-upon terms, conditions and verifiable success metrics by all involved stakeholders—the social impact investors are paid principal plus interest. Unlike the evaluation advisors, who play a relatively active, hands-on, day-to-day-management-type role, the independent evaluator’s purpose is to be at an arms-length such that its decisions are objective, fair and reliable (Kim and Kang, 2012; McKinsey & Co., 2012).
The final stakeholder is arguably the most important—the local community and greater society relating to the particular programme, project or persons. While the constituents benefit directly from the funding provided by the SIB programme, the local community and greater society can also benefit, directly and/or indirectly, from the outcome of the funded constituents.
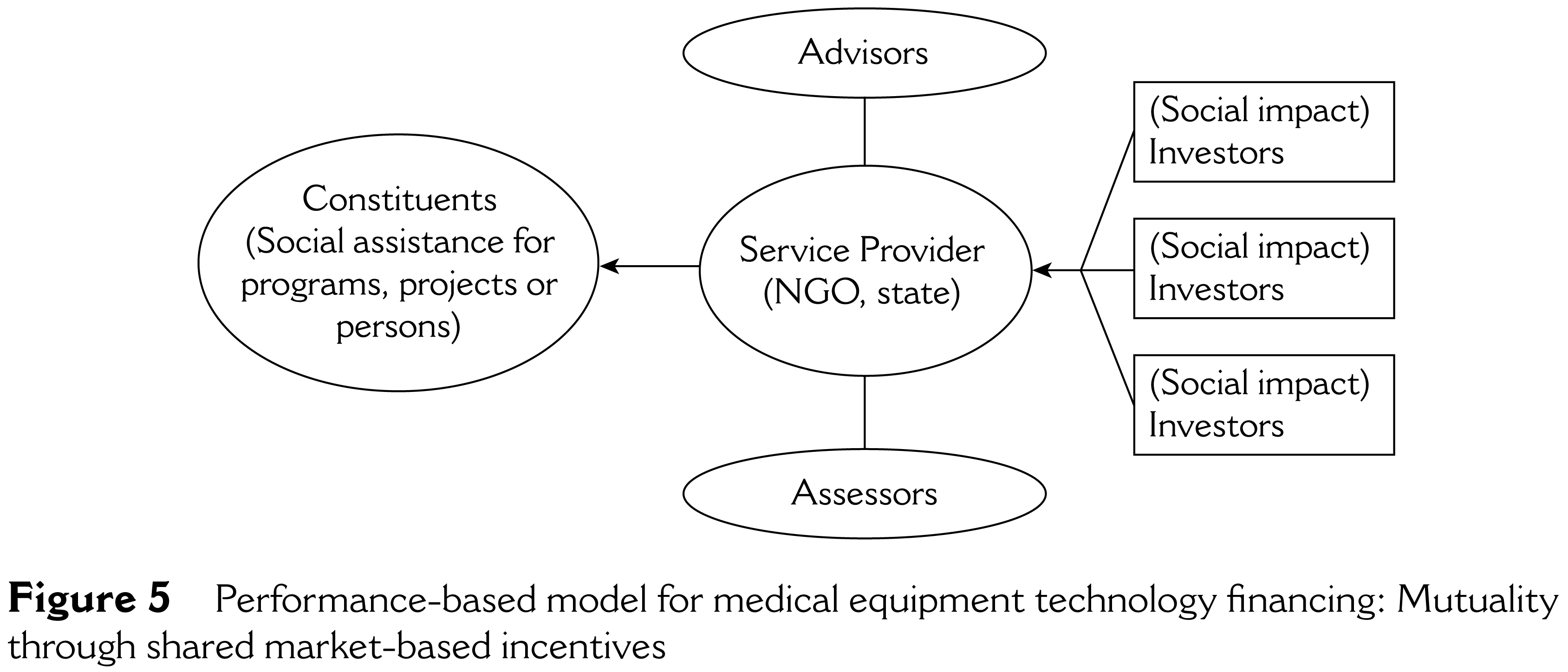
Performance-based model for medical equipment technology financing: Mutuality through shared market-based incentives
In broad terms, the main legal SIB stakeholders (social and financial networks) include:
constituents (assistance project, programme or persons) service providers (social) impact investors intermediary advisors assessors community/society (community)
Encouraging and creating more effective medical technology transfer and equipment-related incentives vis-à-vis specific roles, shared stakeholder agreement, trust and independent post-project verification—all features present with social finance and SIB-based assistance projects and related funding efforts—is in the authors’ view, a viable approach that can complement existing traditional financing models, applicable to funding for MET transfers into developing regions (Kim and Kang, 2012). Such interlinkage between MET and SIB models, which is the scope of this article, would thus constitute a unique contribution to the existing literature.
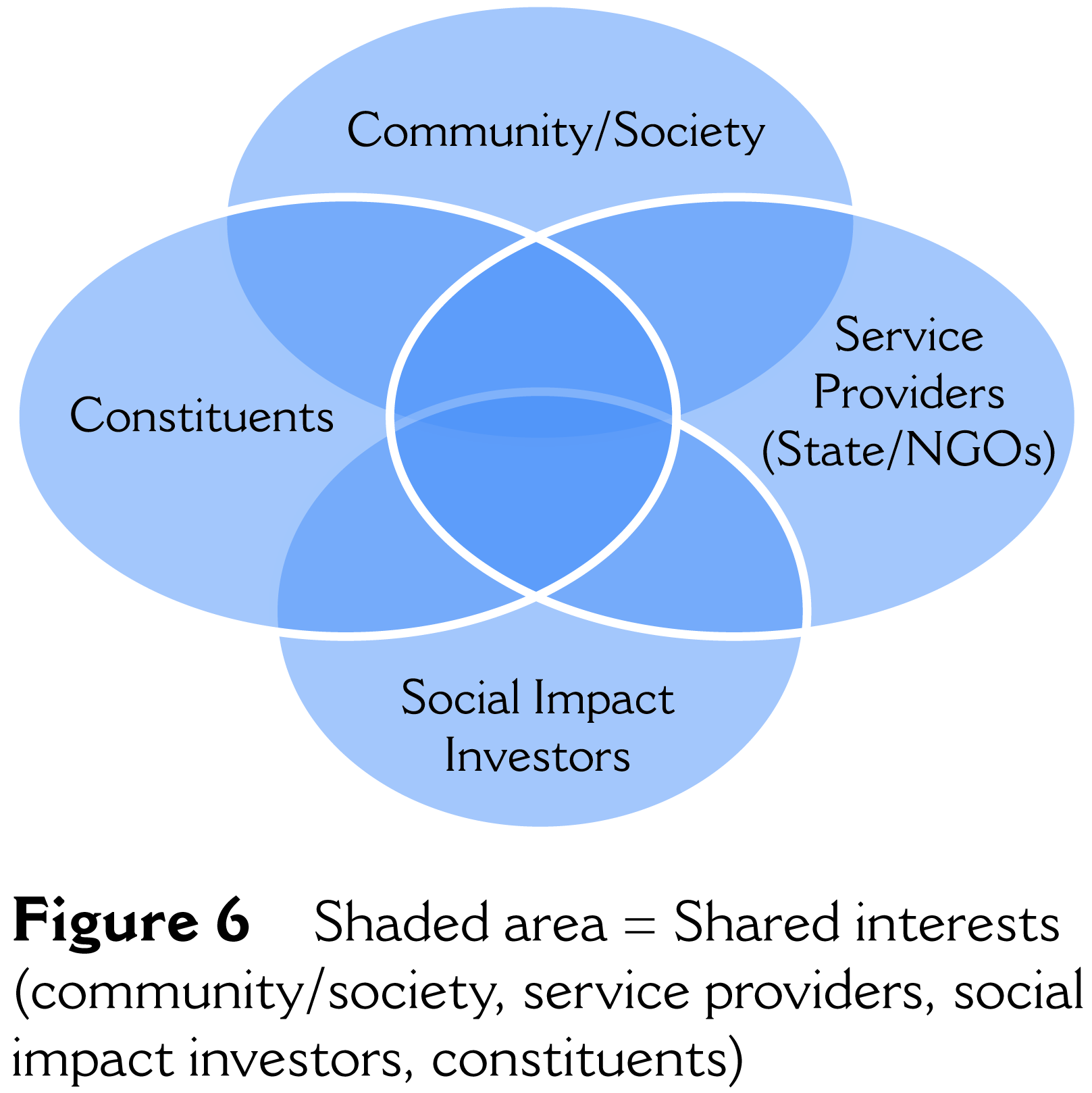
Shaded area = Shared interests (community/society, service providers, social impact investors, constituents)
Unique features
The unique financial feature of the SIB conceptual framework is that, first, the services provided for the constituents are initially funded by the impact investors (rather than the service provider, which would typically be the state and/or CSO) vis-à-vis the SIB purchase by the impact investors. That is, the service provider—albeit the federal/local government and/or NGO—is not obligated to pay any funding amount upfront. Second, the service provider only provides funding (for the particular service to the constituents) if and only if certain pre-designated post-social assistance project metrics are achieved. If not, then the impact investors bear the loss (up to a certain level).
Summary of benefits
From the perspective of shared incentives with respect to each related stakeholder, the benefits of social finance and SIBs include (Kim and Kang, 2012):
Target transparency: Service providers, such as government (public) organizations, only need to fund projects (services) that are deemed successful. In the past, such hortatory terms as objectives were difficult to measure. However, under the SIB social finance structure, clear pre-designated targets are set, which will typically include quantitative targets (to mitigate the implicit ambiguity of hortatory language found in qualitative language). This provides a very clear aspirational target for all parties involved—impact investors, intermediaries, service providers, advisors, outside assessors and the constituents—upon which to make the relevant analysis and conclude whether the particular project relating to the SIB investment was successful or not. Throughout the SIB transaction tenor (life cycle), the internal advisor provides the necessary due diligence to ensure transparency, while the external assessor calculates and determines whether the project (transaction) has met its stated target levels or not. Economically efficient use of resources: With the SIB structure, the relevant resources are allocated by the related parties and social networks to the transaction in a relatively efficient manner. The service providers—most likely public entities and/or NGOs only pay for services that are efficient (i.e., have met their pre-designated success target levels). The social finance impact investors provide (invest) the original funding amount in exchange for the possible (but not guaranteed) economic benefit of a return on investment greater than its original investment amount. According to scholars such as Lynn Stout, this would be the focus of those with a homo economicus approach (Stout, 2012). Ethical standards: Traditional finance is predicated on ‘rational’ behaviour, which is another way of saying to maximize one’s own benefit through risk-taking in investments (products and/or services) that provide the opportunity to receive profit in exchange for such risk-taking behaviour. In the SIB model, ethical considerations, including moral considerations (linked to ‘moral capital’) are also driving incentive forces for SIB impact investors, which represent a new approach in terms of deciding how to allocate (invest) capital.
Summary of stakeholders
From the perspective of shared incentives from the perspective of each related stakeholder, the benefits of social finance and SIBs include:
Social impact investors: Much like investors in traditional MET funding frameworks, investors in social finance transactions would seek to maximize profit. In slight contrast, however, social finance investors would consider not only factors related to maximizing profit but also positive externalities, such as societal contribution of the investment capital. CSOs/NGOs: The incentive for CSOs/NGOs in social finance transactions is that such groups only fund those projects that are successful in terms of meeting certain pre-designated metrics. If such metrics are not met, then the end social impact investors fund the transaction. Constituents/project: The constituents benefit since funding will be provided, which is clearly a better scenario than if funding is not provided. An additional benefit is that specific ‘success metrics’ are established, such that sustainable and verifiable measures for success are instituted. Greater society/community: The resources for the social project, such as with MET transfers, combined with the incentive structure of the social finance transaction provide a more efficient way to allocate capital and ensure long-term measurable results that can benefit the local community. Less taxpayer resources may also be utilized since only those projects that do not meet certain pre-designated standards related to the project are funded by the government (or NGO, as the case may be).
Future challenges and opportunities using the SIB funding model
What could constitute some of the challenges to this new innovative funding model? One challenge is that the SIB market is new. Schieber et al. (2007) evaluated health financing in developing countries from global- and country-level perspectives and described several fundamental problems that exist within the current aid architecture as a result of sectoral complexities and governance factors. Although the social finance SIB conceptual framework was not referenced directly by Schieber, the same constraints could apply to the given social finance/SIB conceptual framework.
Assuming that a limited global policy coherence does not yet exist, the SIB conceptual framework may also face further challenges when it comes to cross-border funding efforts. For instance, a lack of predictability of funding may arise, in which large differences between donor commitments and disbursements may also exist, whereby the short-term and volatile nature of such funding at both the micro- and macro-levels can generate problems of macroeconomic management and planning. Another related concern may be the level of debt-to-equity levels by both the donor and recipient entities involved in the SIB MET funding transaction.
As Lee and Eom noted related to project financing earlier (but also not specifically to the social finance SIB conceptual framework), which may also apply to SIBs, it is important that SIB MET financing from non-traditional arrangements is undertaken by a separate entity (i.e., by a new company or by a subsidiary of an existing company), and that the debt of the project is differentiated, at least for balance sheet purposes, from the parent company’s direct obligations. Other challenges include how to effectively coordinate the relevant public and private sector entities (especially given that the two sectors operate in somewhat different ways), capacity building (in terms of gathering personnel who have the depth and breadth of relevant experience in such a new area), availability of relevant administrative data (to determine whether the success metric has been met or not by the assessor) and of course finding a market of potential SIB investors for such MET projects.
An evaluation of the first SIB social development project in Peterborough, UK was released in 2014, and with it (along with the release of other evaluations related to subsequent SIB funding social development projects), an even closer examination of the benefits and costs can be conducted of such performance-based development projects. Despite such outlined challenges, the potential benefits of the related stakeholders seem to outweigh its potential costs and challenges, thus warranting serious consideration of such performance-based MET funding development assistance models for future related projects.
Conclusion
This article suggests—drawing upon and expanding upon previous related literature—that the use of social finance generally, and SIBs specifically, represents one possible solution leveraging performance-based market mechanisms, inter alia, to meet such challenges as it relates to MET funding mechanisms. With the SIB funding model, the end social impact investors provide the initial funding relating to a particular project and/or constituency (rather than the government and/or CSO, which would be the typical case without the advantage of a social finance mechanism), resolving some (but clearly not all) of the funding challenges for the needed public work projects that benefit society. Here, the relevant CSOs/NGOs and government body(ies) involved need only to provide MET development financing if and only if a specific target is met, else the social impact investors bear all or a proportion of the loss. Thus, CSOs and/or the government only fund those projects that are deemed ‘successful’ as measured by certain predetermined metrics agreed upon by all the stakeholders to a particular MET project—including the service providers (NGOs, government), constituent (project to receive funding) and end investors (who are willing to forsake a certain portion of financial gain in exchange for adding to funding a MET project that may, but is not guaranteed to, result in some form of societal benefit).
The SIB framework would also further transparency relative to previous frameworks since the relevant stakeholders would be fully aware of what money is used for what service. It also helps to bring the public sector and CSOs into greater alignment with clearly defined stakeholder roles and responsibilities in which such a structure could complement and serve as an additional possible funding option (rather than one that is aimed to completely replace the currently existing MET funding structures). The social finance structure also incentivizes other stakeholders to invest in SIBs, which in turn, helps society’s interests (in a unique overlap of individual and societal shared interests and incentives). Although certain challenges exist with the SIB structure as a conceptual framework, by utilizing the proposed performance-based MET funding model for assistance to developing countries, relatively greater transparency, efficiency and sustainability can be achieved to maximize societal contribution benefits related to funding MET for developing countries.
Footnotes
Acknowledgements
This work was supported by the Ewha Womans University Research Grant of 2012, Global Top 5 Project (Grant No.: 2012-1777-1). The author would also like to express appreciation to professors EunMee Kim, Pil Ho Kim, Jean Kang, Minah Kang, Pilwha Chang and Jinwhan Oh, for their invaluable feedback and comments on earlier versions of this article. This article was also immensely furthered by the invaluable medical equipment technology (MET) research of Yeon-Joo Oh (Researcher at Re-shaping Development Institute; Ewha MIS).