
Abstract
Medical tourism is an extensively researched sub-sector of the tourism industry because of its acknowledged role as an important catalyst for economic growth. Nevertheless, the impact of medical tourism on economic growth remains contentious due to associated negative externalities. This paper assesses medical tourism’s role in Malaysia’s long-term economic growth using a neoclassical growth model as its framework and a set of time series econometric approaches, namely cointegration, Granger causality and variance decomposition analysis as core instruments. The results indicate that medical tourism has significant positive impact on Malaysia’s economic growth in the long run.
Introduction
Key drivers for long-term economic growth are manifold and have often been researched upon extensively as their contributions are vital for ensuring sustainable economic growth and socio-economic well-being (Fellner, 1960; Tobin, 1964). Tourism has long been noted for its capacity to accelerate economic growth, a phenomena termed as the tourism-led growth (TLG) hypothesis. The TLG hypothesis has been the subject of numerous studies to evaluate its validity in both developed and developing economies (e.g. Balaguer and Cantavella-Jordà, 2002; Narayan and Prasad, 2003; Tang and Abosedra, 2016; Tang and Tan, 2015a; Tang et al., 2016). Tang and Tan (2013) noted that, despite its lack of universal validation, the TLG hypothesis was valid in the Malaysian context.
Tourism is a vital component of the Malaysian economy because of its important role in income generation and job creation. A major factor for tourism’s growth in the country is due to tourism’s widely acknowledged capacity to generate multiplier effects through the synergy of forward and backward linkages within the tourism value chain (United Nations Conference on Trade and Development, 2013) which in turn contributes to higher employment, poverty alleviation (Overseas Development Institute, 2007) and narrowing income disparities (Ashley et al., 2007) as well as balance of payment realignments (Malik et al., 2010; Thano, 2015). This multiplier effect is particularly evident in the Malaysian tourism narrative as growth in this sector accelerated in the 1980s subsequent to a policy reconfiguration designed to offset diminishing revenues derivable from the export sector due to a collapse in the price of primary commodities particularly rubber and tin. These policy realignments sought to market Malaysia’s natural attractions, cultural heritage and culinary delights as tourism products with the simultaneous objective of leveraging on the anticipated returns to drive socio-economic growth and poverty reduction initiatives (Mosbah and Al Khuja, 2014; Nanthakumar et al., 2008). A key component of this realignment was the formulation of three tourism master plans, namely the National Tourism Policy in 1992, the National Ecotourism Plan in 1996 and the Malaysian Tourism Transformation Programme in 2010. The net result of the implementation of these plans allied to the earlier reconstitution of the old Tourism Development Corporation of Malaysia as the Malaysian Tourism Promotion Board or more popularly known as Tourism Malaysia in 1992 has been significant growth in both income and job opportunities in the tourism sector. For instance, tourism contributed approximately MYR 161 billion or 14.9% of the nation’s gross domestic product (GDP), raking in MYR 72 billion in tourism receipts on the back of 27.44 million tourist arrivals whilst bringing in MYR 19.4 billion worth of investment and contributing 1.77 million jobs (13% of total employment) in 2014 alone (Mohsen, 2015). These gains resulted in Malaysia being ranked 26 out of 184 countries in the world with regard to Travel and Tourism’s contribution to GDP (World Travel and Tourism Council, 2015).
One of the emerging sub-sectors of tourism in Malaysia is medical tourism. Due to astute policy realignments in the healthcare sector to exploit latent demand both in the ASEAN region and beyond and coupled with a convergence of pull factors (Connell, 2013; Fetscherin and Stephano, 2016), medical tourism has witnessed an exponential growth in both arrivals, receipts and facilities. In terms of arrivals, the figures peaked in 2014 when 882,000 medical tourists sought treatment in Malaysia while gross receipts totalled MYR 900 million in 2015 (International Medical Travel Journal, 2016). Additionally, the number of facilities has more than doubled from 35 in 2009 to 78 in 2014. All these achievements were recorded within a short time frame of approximately 16 years commencing 1998 when Malaysia embarked on imbricating medical tourism as a key sub-sector of tourism.
The example of Malaysia substantiates the postulation that medical tourism has emerged as one of the key sub-sectors that have thus far generated substantial revenue for numerous economies (Chaynee, 2003). Hence, it is unsurprising that policy-makers in both developed and developing economies have been assiduously promoting medical tourism in efforts to boost economic growth. However, a review of current literature reveals that the actual impact of medical tourism on economic growth is debatable. This is because while medical tourism spurs economic growth via its positive impact on foreign currency earnings, investments in infrastructure, tax revenues and employment opportunities, it may also generate negative externalities as evidenced by the New Delhi metallo-β-lactamase superbug scare in the United Kingdom (Kumarasamy et al., 2010) and infectious diseases afflicting Third World medical destinations (Cuddington, 1993; Cuddington and Hancock, 1994), the increase in healthcare costs (Gupta, 2008; Hazarika, 2010; NaRanong and NaRanong, 2011; Ramírez de Arellano, 2007) that either directly or indirectly impinge upon the process of economic growth and development. 1
In light of these contradicting outcomes, it is essential to ascertain medical tourism’s role in boosting long-term economic growth. Thus, we chose Malaysia for case study since there is a dearth of empirical research on the role of medical tourism in Malaysia’s economic growth. We utilised co-integration, Granger causality and variance decomposition tests to evaluate both the validity of the medical TLG hypothesis and ascertain its sustainability as a long-term catalyst for economic growth.
Following this introduction, the next section provides a general overview of medical tourism in Malaysia. The subsequent section discusses methodology and results while conclusions and policy implications derived is presented in the final section.
Overview of medical tourism in Malaysia
The Malaysian medical tourism narrative is a testament of public–private sector synergies that have yielded impressive results within a short span of time. These two sectors have often worked in tandem to propel the medical tourism agenda through a variety of strategic policy formulations and investment initiatives.
The role of the private sector in foregrounding medical tourism is essentially predicated on corporate mergers and acquisitions initiatives that have served to create global health service corporations through the establishment and the consolidation of medical centres under mega private healthcare groups such as the Parkway Group in 2010 and the Integrated Healthcare Holding Groups in 2013. The subsequent economies of scale accrued have lowered costs via the provision of a technology-based, human expertise helmed and quality delivery-oriented private medical service sector which has attracted medical tourists seeking affordable, safe and quality treatment. Consequently, these capex have led to the birth of Joint Commission International (JCI) – the gold standard for international accreditation – accredited medical centres, which as of 2015 totalled seven.
In the public sector context, the evolution of Malaysia’s medical tourism sector accelerated from 1998 onwards when a series of tax incentives were instituted in order to promote the medical tourism sub-sector. This led to private medical institutions investing in facility upgrades and expertise enhancements in order to gain international accreditation. Chee (2010) noted that Malaysia was among the first in the Asian region to promote medical tourism as a growth industry. Poon (2008) highlighted that the Malaysian government has thus far allocated at least MYR 110 billion to build new public hospitals to develop the medical tourism sector in Malaysia. Amongst the other direct support measures rendered by the government include the provision of visas for foreign visitors seeking health treatment and tax incentives (International Medical Travel Journal, 2011). In addition, the Ministry of Health has created the Malaysia Healthcare Travel Council to promote medical tourism. Finally, the government has identified medical tourism as one sub-sector of Healthcare, which was designated as one of the 12 National Key Economic Areas (NKEA).
The net result of these initiatives was an exponential growth in both medical tourist arrivals and gross receipts amounting to 341,288 and MYR 254 million, respectively, as of 2008 (Pocock and Phua, 2011). This linear exponential growth was further accelerated with the designation of Healthcare in 2010 as one of the country’s 12 NKEAs deemed to have the potential to spur growth. As part of the Healthcare NKEA, medical tourism is targeted to generate MYR 9.6 billion (Musa et al., 2012) in revenue and MYR 4.3 billion in gross national income and to employ 5300 more medical professionals by 2020 (PEMANDU, 2010). As of 2015, total hospital receipts alone amounted to MYR 900 million which is projected to reach MYR 1.3 billion in 2016. Additionally, medical tourist arrivals have also increased from 641,000 in 2011 to more than 880,000 in 2015 (International Medical Travel Journal, 2016) with arrivals being mainly from Indonesia (72%), Singapore (10%), Japan (5%) and West Asia (2%) (United Nations Economic and Social Commission for Asia and the Pacific, 2007). In terms of destinations, a majority of medical tourists travelled to Penang (61%) (Ormond, 2011).
Finally, other extrinsic factors have also coalesced to propel Medical tourism to the forefront of the tourism and healthcare sector. In fact, Malaysia’s emergence as a medical tourism hub resides in its fulfilment of what Connell (2013) defines as the five essentials of medical tourism, namely attraction, amenities, accessibility, accommodation and awareness. From the attraction perspective, cost is one of the key reasons for Malaysia’s emergence as a major medical tourism destination in Asia. With its relatively low exchange rate (USD 1.00 = MYR 4.00), Malaysia offers excellent medical care at affordable rates when compared with its competitors in both the developed and developing world (Smith et al., 2009). In relation to accessibility, Aigbogun et al. (2013) note that easy availability to air transport as provided by low cost carriers like AirAsia, Malindo and Firefly has enabled more medical tourists to seek treatment in the country. This plus the existence of good transport infrastructure in the major cities of Kuala Lumpur, Georgetown and Johor Bahru means that travel costs are minimal. As for accommodation, both Hilmi and Ngo (2011) and Kelly (2010) highlight how hoteliers and wellness resort operators have optimally refined their offerings to cater to the needs of a specific niche market and thus attract more medical tourists to the country. In other words, the availability of suitable accommodation is another pull factor that has abetted the medical tourism sector’s robust growth. In terms of amenities, most private hospitals that are the main purveyors of medical tourism possess not only sophisticated treatment and recuperation facilities but also contemporary communication facilities such as easy internet and telephony access. These facilities are further augmented by ancillary facilities within hospitals such as pharmacies, retail outlets and cafeterias. Medical tourism arrivals in Malaysia have to a large extent boosted by awareness about the excellent treatment and care services provided by Malaysian hospitals. In this regard, word of mouth is a key factor as delineated by Yeoh et al. (2013) while well-structured and informative websites of medical facilities play a key role in drawing in medical tourists (Anvekar, 2012)
In short, the Malaysian medical tourism sector has witnessed phenomenal growth since its evolution from an ancillary income generating sector of the local Healthcare industry to one of the key sub-sectors of the Malaysian tourism industry due to the convergence of crucial pull factors that were carefully modulated both by public sector policy makers and private sector health service providers.
Despite these developments, the Malaysian medical tourism sector is not immune to problems that plague the medical tourism industry in the region. Most of these problems are associated with the issues of equity and accessibility to quality healthcare (Blouin, 2010). Inequality in healthcare arises when only high- and middle-income earners can access healthcare services due to the high costs of treatment attributable to increased demand for finite resources and expertise (Ramesh and Xun, 2006). Consequently, Medical and Health Insurance (MHI) policies have become tools to mitigate rising healthcare costs. As of 2003, data from Bank Negara Malaysia (BNM) revealed that MHI-based premiums totalled almost MYR 1.0 billion in 2002 or 5.5% of all premiums paid (Bank Negara Malaysia, 2002). A decade later, the quantum of these premiums constituted approximately 20% due to inflation (Chin, 2014).
These negative externalities pertaining to equity and costs of quality healthcare raise the question as to how sustainable and viable is medical tourism for Malaysia’s long-term economic growth.
Methodology and results
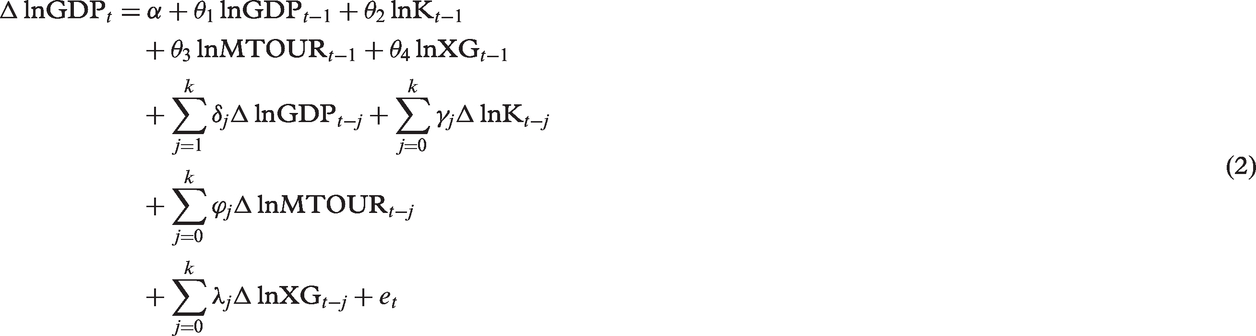
Since the aim of this study was to examine the effects of medical tourism on economic growth in Malaysia, we applied the following two sectors: Feder (1983) growth model extended by Tang and Tan (2015b)

This study used quarterly data from 1998:Q1 to 2013:Q4. The data were extracted from the International Financial Statistics published by the International Monetary Fund, Monthly Statistical Bulletin published by BNM and Tourism Satellite Account published by the Department of Statistics, Malaysia. 2 Additionally, the GDP deflator (2005 = 100) was used to compute the real values of each variable.
Results of ADF DF-GLS unit root tests.
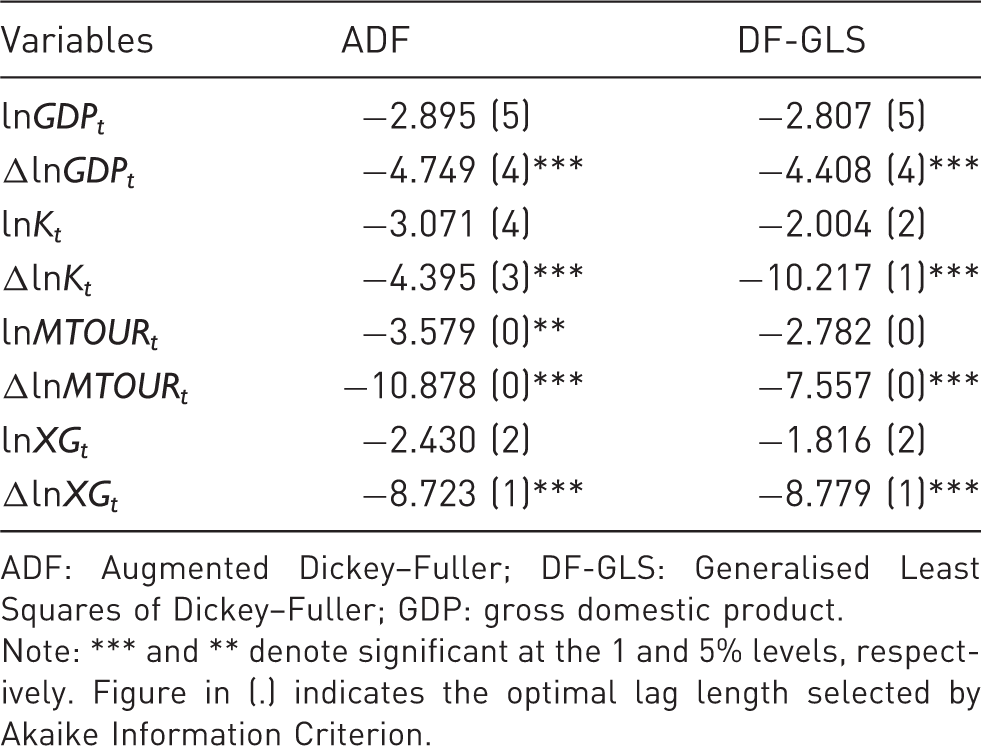
ADF: Augmented Dickey–Fuller; DF-GLS: Generalised Least Squares of Dickey–Fuller; GDP: gross domestic product.
Note: *** and ** denote significant at the 1 and 5% levels, respectively. Figure in (.) indicates the optimal lag length selected by Akaike Information Criterion.
Results of bounds test for co-integration.
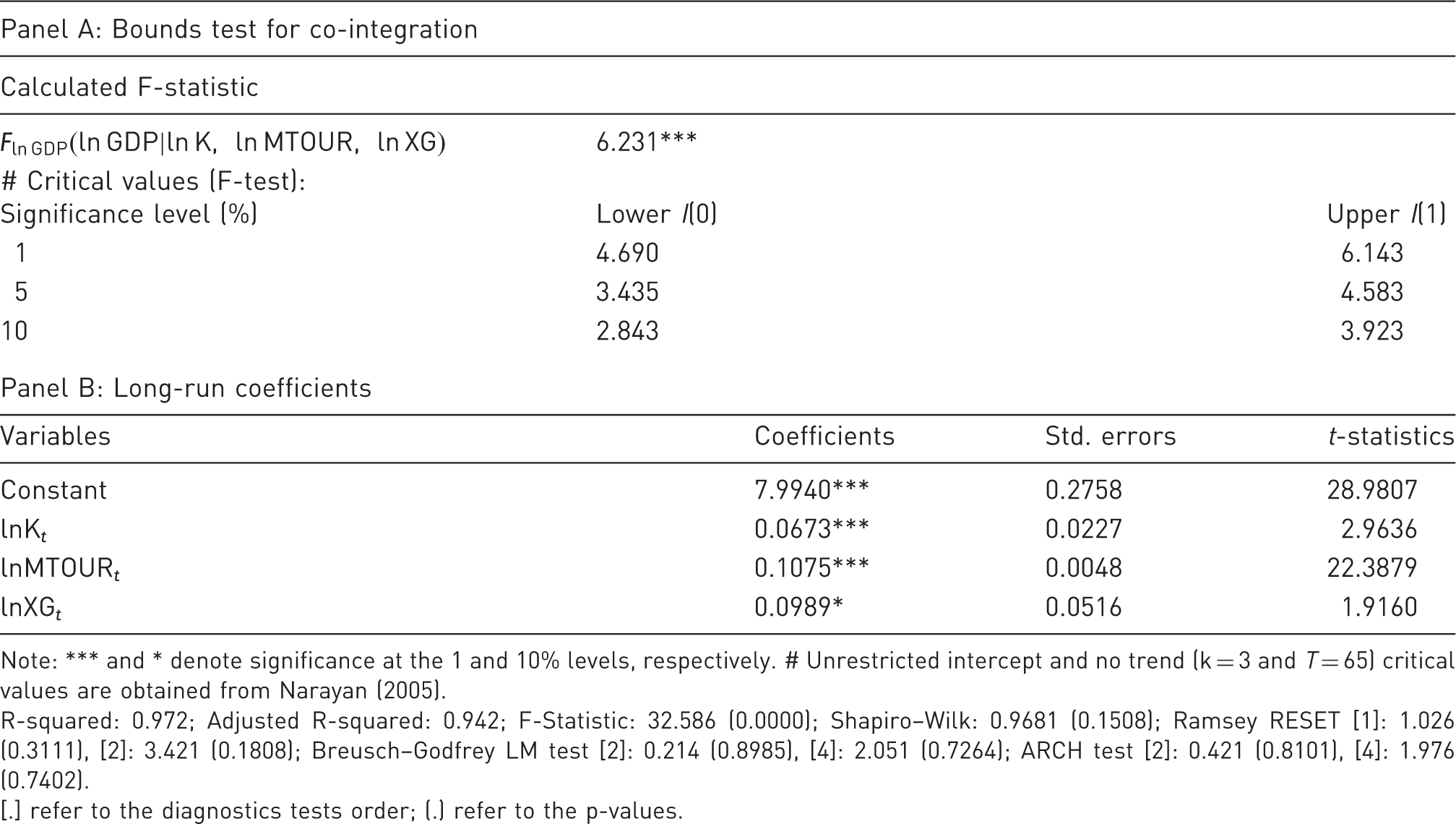
Note: *** and * denote significance at the 1 and 10% levels, respectively. # Unrestricted intercept and no trend (k = 3 and T = 65) critical values are obtained from Narayan (2005).
R-squared: 0.972; Adjusted R-squared: 0.942; F-Statistic: 32.586 (0.0000); Shapiro–Wilk: 0.9681 (0.1508); Ramsey RESET [1]: 1.026 (0.3111), [2]: 3.421 (0.1808); Breusch–Godfrey LM test [2]: 0.214 (0.8985), [4]: 2.051 (0.7264); ARCH test [2]: 0.421 (0.8101), [4]: 1.976 (0.7402).
[.] refer to the diagnostics tests order; (.) refer to the p-values.
The calculated F-statistic for bounds test was 6.231 and greater than the 1% upper bound critical values as proposed by Narayan (2005). This implies that there is a long-run equilibrium relationship between real GDP, real capital, real medical tourism and real export of goods in Malaysia from 1998:Q1 to 2013:Q4. We then proceeded to estimate the long-run coefficients by setting real GDP as the dependent variable since our key interest was to assess the response of economic growth to medical tourism, capital and export of goods in Malaysia. The estimated co-integrating equation is illustrated in Panel B of Table 2 with all variables being statistically significant at the 10% level or better. Specifically, a 10% increase in medical tourism will entail a real GDP increase of approximately 1.1% in the long run. In contrast, economic growth increases by approximately 0.67 and 0.98% for every 10% increase in real capital and real export of goods, respectively.
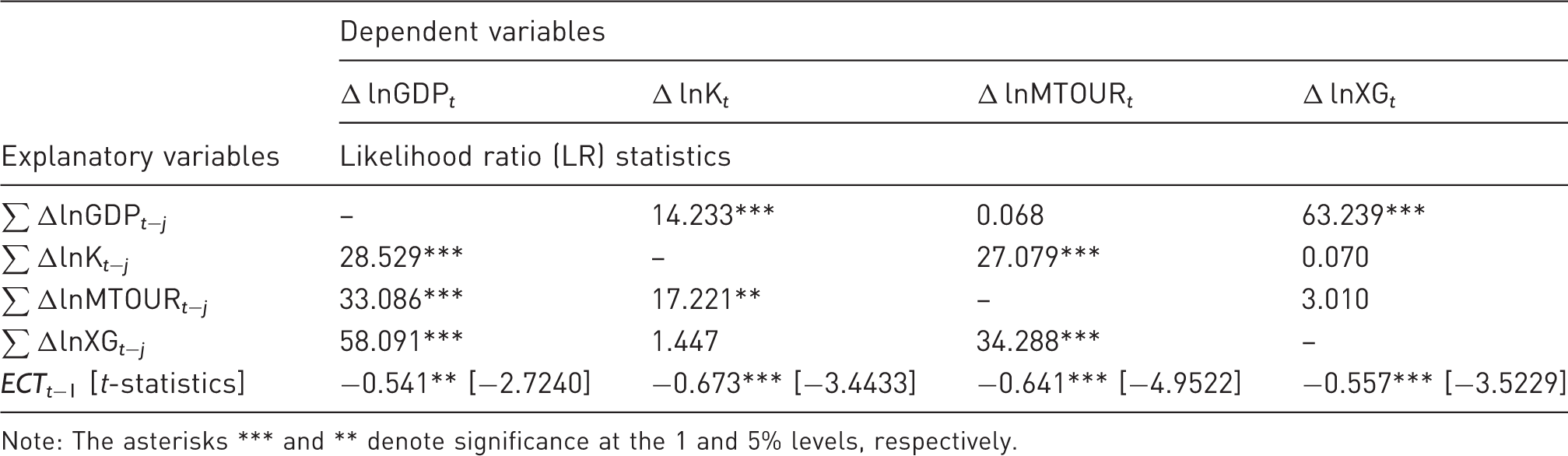
Next, we examined the Granger causality between economic growth and its determinants by estimating the following vector error-correction model (VECM):
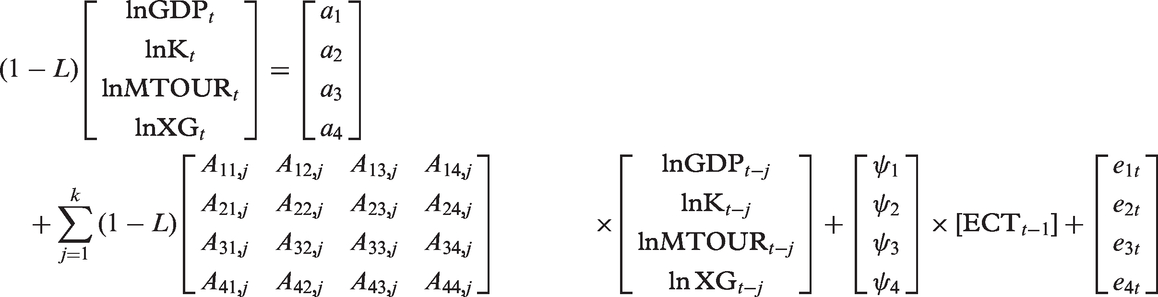
Table 3 indicates that the coefficients of Summary of the short- and long-run Granger causalities. The results of the Granger causality test – VECM. Note: The asterisks *** and ** denote significance at the 1 and 5% levels, respectively.
Generalised variance decomposition analysis of lnGDP.
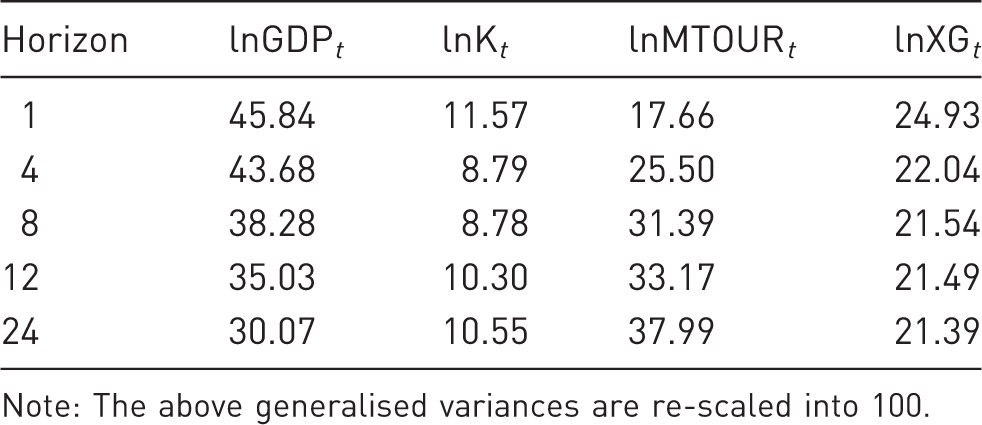
Note: The above generalised variances are re-scaled into 100.
In the short run (i.e. four quarters), 43.7% of the variations in economic growth was explained by its own innovation. In contrast, a shock in real capital, real medical tourism and real export only explained about 8.8, 25.5 and 22%, respectively, of variations in economic growth. Over the long run (i.e. 24 quarters), real medical tourism explained approximately 38% of variations in economic growth. On the other hand, real exports of goods and real capital, respectively, explained about 21.4 and 10.6% of all variations. Thus, it can be concluded that medical tourism is a key determinant of Malaysia’s economic growth in both the short and long run.
Conclusions and policy implications
This paper sought to determine the extent of medical tourism’s role in Malaysia’s long-run economic growth. To answer this research question, we employed a series of parametric tests, namely the co-integration, Granger causality and the generalised variance decomposition tests. We found that economic growth, medical tourism and other determinants in Malaysia were co-integrated and that the response of economic growth to medical tourism was slightly higher than that to capital and export of goods. The generalised variance decomposition analysis also identified medical tourism as the most important factor in explaining the variations in economic growth in both the short and long run. Finally, we found that medical tourism Granger-causes economic growth in Malaysia, regardless of short or long run.
Several policy implications arise from these findings. First, medical tourism’s function as an effective catalyst can be further augmented through the provision of Goods and Service Tax (GST) exemption on medical supplies and equipment. This will help reduce treatment, medication and hospitalisation costs that will consequently attract medical tourists in search of affordable treatment. Alternatively, a GST refund mechanism can be made available for genuine medical tourists. Second, the private sector should be incentivised to open more medical facilities that cater to tourists in our economic corridors. For example, investing in medical facilities in the Iskandar Region of Johor would enable healthcare providers to tap into the Singaporean clientele base seeking quality yet affordable medical services abroad to offset high medical costs at home. In this regard, Malaysia is eminently placed to fulfil that demand as exchange rate differentials are currently skewed in its favour. Third, local medical tourism purveyors should seek international accreditation from renowned organisations like the JCI in the United States, the Australian Council for Healthcare Standards International in Australia and quality healthcare advice (QHA) Trent in the United Kingdom in order to gain the confidence of medical tourists from Europe, the Americas and Australasia. Furthermore, accreditation has the winnowing effect of filtering out low-quality healthcare providers thus indirectly foregrounding Malaysia as a provider of safe and quality healthcare. Finally, legal protection for patients, easier facilitation of litigation and prompt disposal of claims arising from malpractice would engender trust in foreign tourists seeking medical treatment while simultaneously functioning as a quality control mechanism that ensures the highest standards of service are adhered to. All these efforts will emplace Malaysia as a destination that provides affordable, safe and quality medical services, thus optimising the impact of medical tourism on economic growth in Malaysia.
Footnotes
Acknowledgement
We would like to thank the two anonymous reviewers for their critical and valuable suggestion on the earlier draft of this research paper. Any flaws that remain in this paper are our own responsibility.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author would like to acknowledge Universiti Sains Malaysia Short-Term Research Grant No. 304/CDASAR/6313179.