
Abstract
Summary
The U.S. Trafficking Victims’ Protection Act of 2000 established specialized victims’ services and law enforcement directives to protect victims/survivors of sex trafficking through investigation and aftercare services. Yet, gaps remain in our understanding of services needed and the best approaches to improve outcomes. Using cross-sectional electronic survey data from 107 service providers to human trafficking victims across Missouri, this study examines (1) victims’ service needs, (2) agencies’ ability to provide services, (3) victim sub-populations that agencies are able to serve, and (4) the rural/urban availability of anti-trafficking services.
Findings
Service providers, including social workers, counselors, law enforcement, and medical professionals reported that the most needed services for victims included case management, counseling, crisis services, shelter, and medical assistance. However, out of 15 possible victim services, only two were provided in-house by the majority of agencies. Additionally, respondents identified populations they were frequently unable to serve including incarcerated victims, tribal victims of violence, and refugees and immigrants. Urban counties were served by a significantly higher mean number of respondents compared to rural counties.
Applications
Findings raise concerns that some of the most critical services needed for best practice response may not be easily accessible for victims, particularly in rural regions. In addition, many providers are tasked with addressing multiple service needs with limited resources. Efforts to increase cross-discipline training, interdisciplinary collaboration, and funding for basic services are needed to ensure adequate and accessible services for survivors. Recommendations for future research and coordination of an effective response are noted.
Keywords
Sex trafficking is the exploitation of a person for the purposes of sexual services (i.e. forced commercial sex) and is considered an affront to human rights across the globe. In 2000, the United Nations established a modern definition of human trafficking for the world in The United Nations Convention against Transnational Organized Crime, Protocol to Prevent, Suppress and Punish Trafficking in Persons (United Nations Office on Drugs and Crime, 2004). Article 3 paragraph (a) of the Protocol laid out an “Action, Means, Purpose” model, which was adapted to establish the United States (U.S.) legal definition (United Nations Office on Drugs and Crime, 2004). The Trafficking Victims’ Protection Act (TVPA) of 2000 established that the exploitation of a person for sexual or labor services was a unique crime and filled gaps in U.S. law.
Since its passage, nearly every state in the U.S. has formulated a state-level criminal code against human trafficking (National Counsel on State Legislatures, 2018). Further, the TVPA established specialized victims’ services and law enforcement directives, known as the “three Ps,” to prevent (often via public awareness and technical training), protect (through investigation and aftercare services), and prosecute (with adjudication) trafficking (U.S. Department of State, 2017). Though scholars and practitioners have produced and disseminated much scholarship related to this agenda over the past two decades, as an area of study, and regarding knowledge of evidenced-based practice, large gaps remain in our understanding of the breadth of services needed and the best approaches to improve outcomes for victims and survivors (the terms victim and survivor will be used interchangeably) (Davy, 2015; Futures Without Violence, 2007; OVCTTAC, 2019).
The field of social work is uniquely positioned to address human trafficking given the profession’s ethical code to advocate for human rights, to protect the most vulnerable in society, the ecological approach to understanding individuals’ situations, and holistic and strengths-based approaches to supporting individuals (Hodge, 2014; Okech et al., 2018). However, within the field of social work and human trafficking study, there is quite a breadth of understanding about the role of the practitioner working with this vulnerable population, the agency of those engaging in commercial sex (on their own volition or exploited), and approaches to service provision (Alvarez & Alessi, 2012; Sloan & Wahab, 2000; Weitzer, 2005). Much debate surrounding these conversations are influenced by ideology that may be best described as a continuum from empowerment to oppressive paradigms (Weitzer, 2005); from harm reduction (Rekart, 2005) on one hand to “carceral protectionism” (Musto, 2010) on the other. These understandings, in turn translate into vastly different approaches to service provision, policies impacting eligibility and kinds of services provided, and even the language used to describe the population(s) worked with (Nichols, Gerassi, et al., 2018; Wahab & Panichelli, 2013).
While social work literature has largely focused on sex trafficking (Okech et al., 2018), Alvarez and Alessi (2012) discuss the importance of social workers’ recognition of non-sexualized labor exploitation. Moreover, the illegal nature of sex work throughout much of the U.S., and the conflation of the distinct legal constructs of human trafficking and commercialized sex can put victims of human trafficking at risk for arrest (Farrell & Cronin, 2015). In turn, arrest and negative interactions with law enforcement can impede victims’ access to trauma-informed services (Rajaram & Tidball, 2018). Recent reactions to potentially coercive service provision for women engaged in commercial sex, and subsequent clarifications of the role of social work in service provision to sex workers are present throughout the literature (Wahab, 2002; Wahab & Panichelli, 2013).
Across the Midwest, various stakeholders have worked to reduce the harm of sex trafficking. In Missouri, the National Human Trafficking Hotline (2017) has seen a 25% increase in reports between 2012 and 2017; consequently, it is feasible that more victims are accessing services. Yet providers have expressed concern that a lack of service coordination may hinder response to victims in both urban and rural areas (Nichols & Heil, 2015). Therefore, it is essential to develop an understanding of existing and needed services to coordinate an effective response. The purpose of this research was to examine aspects of protection, specifically: (1) service needs of victims of sexual exploitation, (2) agencies’ ability to provide services in house or via referral, (3) the sub-populations of victims of sexual exploitation that agencies are able to serve, and (4) the availability of anti-trafficking services in urban and rural counties in the state.
Human trafficking victim services
Following the “three Ps” model, victim services fulfill the protection mandates by being the primary service mechanism to provide aftercare social services to identified survivors of trafficking. Once a survivor has been certified as a trafficking victim, they are eligible to receive specialized victims’ services (Rescue and Restore, 2012). Aftercare providers must address the complex symptomology of survivors, which may include loss of a sense of identity, security, and dignity; and the trauma, if unaddressed, may leave survivors vulnerable to revictimization (U.S. Department of State, 2012). To promote well-being, a variety of comprehensive services are recommended, including meeting basic needs; addressing physical health; screening and treatment for mental health, particularly trauma focused therapy; facilitating an empowering environment; and promoting skills development (U.S. Department of State, 2012).
Federally funded service providers typically have significant backgrounds working with international populations, such as refugee resettlement agencies, or in child welfare, such as youth shelters. As a requirement to receiving funding, these service providers must demonstrate adequate expertise working with the population, or similar population, and a high degree of interdisciplinary collaboration to ensure victims are afforded the services to which they are entitled (U.S. Department of Justice, 2017). Occasionally, agencies are established with the intention of providing aftercare services to trafficking victims but are largely unknown to existing organized anti-trafficking networks (Chuang, 2010; Zimmerman, 2010) limiting the ability of these agencies to offer coordinated and comprehensive aftercare for survivors. Moreover, because the established responses to assist trafficking survivors are typically concentrated in urban centers, the response coordination in less urbanized areas appears to be more nebulous across the nation (Nichols & Heil, 2015). Despite calls to examine aftercare services for survivors of sex trafficking, a paucity of scholarship exists (Dell et al., 2019; Macy & Johns, 2011; President’s Interagency Task Force to Monitor and Combat Trafficking in Persons, 2013). Sex trafficking survivors are often faced with extreme barriers to recovery and independence, including physical injuries, mental health needs, legal involvement, lack of housing, and a lack of overall safety (Macy & Johns, 2011).
Human trafficking victim services gaps
Rigorous evaluations of human trafficking programs and interdisciplinary taskforces are rare and badly needed (Davy, 2016; Dell et al., 2019). Anti-human trafficking service provision has been supported by the U.S. government since the earliest days of the TVPA, yet very few evaluations of supportive services exist in the literature. The U.S. Government Accountability Office (GAO, 2007) found during their 2007 review (the most recent the authors could find) that the majority of funded projects did not include functions to evaluate how funded activities achieved goals or examined long-term impacts of the projects.
However, a few recent studies have examined statewide anti-trafficking efforts to discover the needs for improvement and gaps in services experienced by survivors of trafficking (Jones & Lutze, 2016; Nichols & Heil, 2015). Based on their empirical finding that interagency collaboration was largely not formalized, Jones and Lutze (2016) recommend that efforts should create mechanisms to improve collaborative partnerships and a continuously updated contact list to help coordinate survivor services and expertise. Nichols and Heil (2015) and Jones and Lutze (2016) advocate for more training for providers steeped in evidenced-based materials as well as clear understandings about what is and is not human trafficking. Nichols and Heil (2015) also call for more survivor-centered approaches to service delivery to support the survivor’s safety and resource needs while valuing their input in collaborative service provision. Focusing our attention on identifying and addressing the gaps in services “may in turn assist the criminal justice system to pursue prosecutions as victims become empowered to fight back while moving forward” (Jones & Lutze, 2016, p. 170). Hence, the importance of mitigating deficits in trafficking response addresses the TVPA’s directive of ensuring empowering and effective prevention and protection to trafficking victims. Thus, this article seeks to map existing service provision within the state of Missouri and to identify geographic and/or demographic gaps in sex trafficking aftercare services.
Methods
Sample and data collection
This study used cross-sectional electronic survey data from a larger mixed-methods exploratory study. The survey was emailed to service providers across Missouri via four sex trafficking related membership listservs including a statewide domestic violence and sexual assault coalition listserv. The email that requested research participation included the option for participants to snowball the survey to other providers who would have sex trafficking knowledge. With snowball sampling, the authors attempted to control bias by offering the survey to knowledgeable professionals who were not signed up for listservs. This sampling strategy aimed to target those most likely to come into contact with survivors of sex trafficking from a variety of professions such as child protective services, medical providers, human trafficking response agencies, law enforcement, legal, and faith-based organizations. The survey was open for response between August and November 2017. Participation was voluntary and participants provided electronic informed consent before proceeding with the survey. Participants were not compensated for the time it took to fill out the survey, approximately 30 minutes. This study was confidential and approved by the Internal Review Board at the authors’ institution, number 2008437.
Instruments
All variables were self-reported. Participants were first asked information about themselves. There were three demographic questions: gender, age, and race/ethnicity. There were two professional questions with categorical response options: (1) the position they held in their agency (administrator, frontline staff, volunteer, Board of Directors Member, Other); and (2) their professional credential (social worker/counselor, certified law enforcement officer, licensed attorney, medical professional, other). There was a small amount of missing demographic data. One participant did not report their ethnicity, two participants did not report their age, and three participants did not report their professional credential.
The variables of interest in this study were responded to by participants filling out two electronic tables and one pictorial map. The first table asked participants to report both how often services were needed by victims/survivors of trafficking they served in the last 12 months and their agencies’ ability to provide each service. Both questions were side by side in one table, with 17 services listed, including “other” (with write in options). There were two response options for needed services. Participants could indicate that all or most victims need the service or that none of the victims needed services. There were three response options for agency ability to provide services. Participants could indicate: yes—(services were provided) in house; no—we refer (for these services); or no—(the services are) not available.
The second table asked, “What populations does your agency serve (check all that apply)?”. Respondents could select yes or no for each of the following sub-populations: victims/survivors of interpersonal violence, domestic violence, sexual violence; children who have experienced abuse or neglect; homeless adults and families; homeless youth; refugees and immigrants; English as a Second Language speakers; adult victims/survivors of human trafficking (sex or labor trafficking); campus survivors/victims of intimate partner violence; incarcerated survivors/victims of violence; male victims/survivors of intimate partner violence, domestic violence, or sexual violence; tribal victims/survivors of violence; veterans, spouses, and family survivors of violence; other (with a write in option).
Finally, there was a pictorial map of the state with every county drawn and labeled. Participants were first asked to fill in the number of “How many counties in (the state) does your agency serve?”. They were then asked, “which counties does your agency serve?” and to use their cursor to click on “all of your service counties on the map.” If they served every county, there was an option to select a box to indicate such rather than fill in a number and select counties from the map. For analysis purposes, we used the urban/rural classification system defined by the Missouri Department of Health and Senior Services (2017). Of 115 counties, 14 were classified as urban and 101 as rural.
Data analysis
A total of 129 individuals started the survey, and 125 individuals provided consent to participate. However, 18 individuals did not respond to any questions after providing consent, so they were dropped from the analysis. Responses from N = 107 participants were included in this analysis. Although only 66 (62%) of participants responded to every question in the full survey, we utilized all available data for this analysis to provide the most information on each variable relevant to the research questions. The survey did not require a response to every question. Given the use of tables to respond to questions (about service needs and provision and sub-populations able to be served) with multiple items that could be clicked on for response, it was possible for participants to skip irrelevant items.
The electronic survey data were exported into a spreadsheet. Descriptive analyses were conducted using the spreadsheet and Stata 13.1 (StataCorp, 2013). A t-test was conducted in Stata 13.1 to examine if there was a difference in the number of service providers available in rural compared to urban counties.
Results
The mean age of participants was 43.3 years with a range of 23–77 years. Most participants were women and Caucasian (Table 1). The majority was in administrative positions (n = 63) or were frontline staff (n = 35) at their agency. The most frequent professional credential was a social worker or counselor (n = 45) but there were also law enforcement officers (n = 17), medical professionals (n = 8), and other professionals (n = 30) who participated. “Other” professionals included participants who indicated a wide variety of professional backgrounds including accounting, public administration, office management, and non-specified MAs and PhDs, hence could not be categorized as a meaningful profession.
Electronic survey information for N = 107 participant providers to sexually exploited/trafficked persons in Missouri.
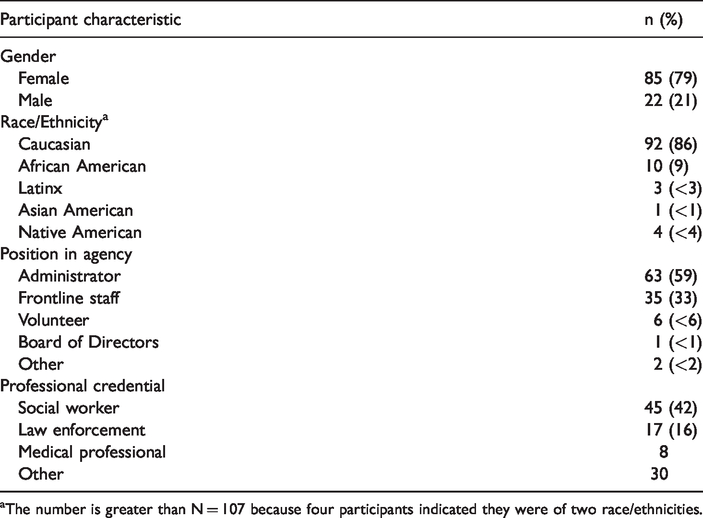
aThe number is greater than N = 107 because four participants indicated they were of two race/ethnicities.
Service needs and service provision
The majority of respondents indicated that all or most trafficking survivors needed 13 of the 15 services listed in the survey (Table 2). The most needed services included case management, counseling, crisis services, shelter, and medical assistance. The two services that only a few providers indicated that all or most survivors needed were interpretation services and childcare. Respondents also indicated needs for the “other” category, and one participant wrote in each of the following responses: “after care/safe home” (participant 57); “basic needs: transportation assistance, food, clothing, hygiene items” (participant 60); “forensic interview” (participant 37); “survivor support” (participant 20); and “specific LGBTQ services” (participant 89). Three respondents indicated that they had not directly served survivors.
Sex trafficking service needs and service provision identified by N = 107 providers in Missouri.
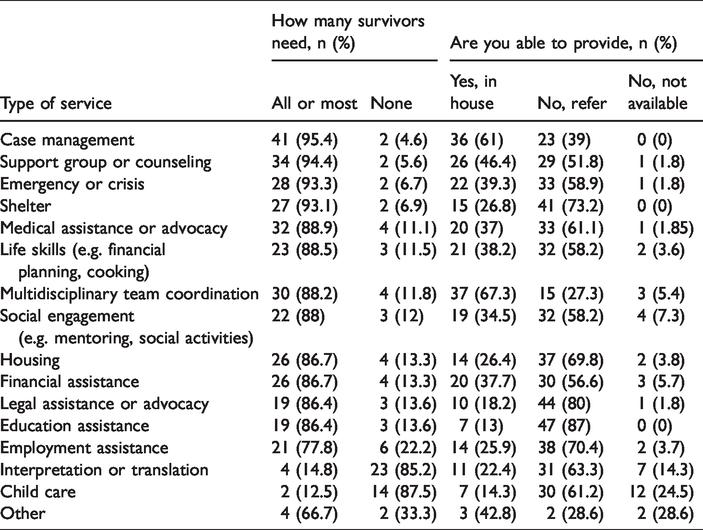
There were numerous gaps between reported victim service needs and the ability for agencies to provide the services needed by all or most survivors. Specifically, only 2 of 15 service options (case management and multidisciplinary coordination) were designated by over 50% of participants as a service the agency provided in house (see Table 1). Services that were needed but most frequently referred out to other agencies included education assistance, legal assistance, and housing or shelter assistance. Most survivors did not need interpretation nor childcare; however, these two services were the most frequently noted as unavailable, both at the respondent agency (14.3 and 24.5%, respectively) and for referral (63.3 and 61.2%).
Populations served by response agencies
The majority of respondents were able to serve a wide range of clients that may include human trafficking survivors (Table 3). The most widely served sub-populations among respondents were victims of interpersonal or sexual violence (90%), children who experienced abuse or neglect (86%), child victims of human trafficking (82%), LGBTQ victims of violence (82%), and male victims of interpersonal or sexual violence (81%). Respondent agencies were least able to serve incarcerated victims (59%), tribal victims of violence (62%), and refugees and immigrants (69%).
Populations that N = 107 respondents’ agencies were able to serve; n (%).

LBGTQ: Lesbian, bi-sexual, gay, transgender, queer or questioning.
Rural and urban service availability
Over a quarter of respondents (n = 37) were from agencies that provided human trafficking related services in all of the counties in the state. The mean number of respondents serving the state’s 14 urban counties was significantly more (M = 7.5, SD = 1.5) than the mean number of respondents indicating they served in the 101 rural counties (M = 2.9, SD = 0.1); t(13)=3.03, p = 0.009.
Discussion
Consistent with the literature, comprehensive services were a critical need. Shelter services appeared to be a critical need with 93% of clients requiring this service. However, among these providers, only 27% were able to provide shelter services in-house. We found similar discrepancies in crisis services, housing, and legal advocacy. It is heartening to see that there are a variety of services that exist within the state to handle the extensive needs of human trafficking survivors at the time of this study. However, it is concerning that some of the most critical services needed for best practice response (e.g. meeting basic needs; addressing physical health; screening and treatment for mental health, particularly trauma focused therapy; facilitating an empowering environment; and promoting skills development) may not be easily accessible. The need for referral adds a layer to service accessibility barriers. These concerns are shared by Macy and Johns (2011) and Nichols and Heil (2015).
Another important demonstration in the results is that agencies are serving many parallel populations, not just survivors of human trafficking (Jones & Lutze, 2016; Macy & Johns, 2011). The most widely served sub-populations among respondents were victims of interpersonal or sexual violence, children who experienced abuse or neglect, child victims of human trafficking, LGBTQ victims of violence, and male victims of interpersonal or sexual violence. This finding should be somewhat expected as there are few places, particularly in rural United States, that have dedicated anti-trafficking service providers. In the absence of dedicated service providers, anti-trafficking personnel are likely to reach out to the next best service avenue. Moreover, in areas with limited service capacity, providers are often tasked with addressing multiple service needs with limited resources (Randall & Tower, 2010). The ability to serve LGBTQ and male trafficking survivors (per Table 3) suggests a need for competent, basic service provision that is appropriate and culturally sensitive for these more marginalized trafficking populations.
Moreover, respondents indicated a gap in services available for survivors of trafficking among incarcerated populations, First Nations peoples, and refugees and immigrants. Noting a service gap among the incarcerated and First Nations peoples may not be particularly surprising, particularly since, at least among First Nations peoples, these populations are not particularly large in Missouri (Peace Studies, 2018). Additionally, across health and social services, there has been a dearth of funding and service provision for First Nations peoples (Olson & Wahab, 2006). This finding perhaps offers more support for some commentary that the anti-trafficking movement is not as inclusive as it should be (Andrijasevic & Anderson, 2009; Deckert et al., 2018; Srikantiah, 2007). Considering language interpretation services were not among the most difficult to provide, it is perplexing that providers would indicate that refugee and immigrant populations would be more difficult to serve. It could be that at the time these data were being collected one of the largest international service providers in the region was experiencing a gap in grant related human trafficking programming, hence weakening their ability to offer robust services. It could also be that these data were collected at the start of what has arguably become an era of heightened nationalism in the U.S. (Brands, 2017; Calvo, 2017; Deckert et al., 2018; De Vries et al., 2019; Erwin, 2017). This wave of anti-immigrant feeling may account for the lack of service responsivity in this study related to refugee and immigrant populations.
The results also showed very few providers were able to provide interpretation services and childcare in-house. Relatedly, the limitation of agencies’ ability to provide comprehensive services needed by all or most survivors in-house, rendering the survivor to seek these services in a variety of service settings which may or may not be trauma informed, culturally sensitive, or competent to serve trafficking survivors, which is a noted concern in extant literature (Dell et al., 2019). Hence, the continuity of care may be negatively impacted and is counter to the “victim centered approach” as it could involve sending a traumatized population all over a geographic area to get the services they need encountering more barriers to service access (Nichols & Heil, 2015). As Deckert et al. (2018) conclude, there appears to be a negotiation among providers about what trafficking means (e.g. oppression versus empowerment focused) and how policy (i.e. criminalization of sex work: Farrell & Cronin, 2015; coercive service provision: Wahab & Panichelli, 2013) treats the phenomenon, leading many providers to miss opportunities for identification and/or service engagement. “The ‘fuzzy’ lines related to defining trafficking make it difficult for service providers to connect trafficking risks with more commonly understood social problems” (Decker et al., 2018, p. 902); hence, survivors are left to navigate complex social and legal systems without assistance. More study is needed to explore these potential issues.
Very few examinations regarding gaps in services exist for general human trafficking response (see Jones & Lutze, 2016); however, there are several studies examining service gaps for victims of sex trafficking (see Gerassi & Nichols, 2018; Gerassi, Nichols, & Michelson, 2017) and more specifically, children who have been sex trafficked (see Gibbs et al., 2014; Goździak & MacDonnell, 2007; Hounmenou & O’Grady, 2019). The demographics of participants in these studies are largely white and female, as is this current study. Consistent with extant literature (Dell et al., 2019; Geraasi et al., 2018; Macy & Graham, 2012; Macy & Johns, 2011; U.S. Department of State, 2012), providers noted that the most needed services trafficking survivors required included case management, counseling, crisis services, shelter, and medical assistance. This is also consistent with best practices (Nichols & Heil, 2015) among anti-trafficking coalitions—to develop vetted referral networks to provide a variety of services for trafficking survivors and mitigate one agency having to be all to everyone. However, it should be noted that few if any studies have examined this issue closely.
That the majority of service providers appeared to be located in urban counties within the state is also unsurprising, as other scholarship has identified similar patterns (Nichols & Heil, 2015; Raphael et al., 2010; Wade, 2008; Wilson & Dalton, 2008). While there are many more rural (101) than urban (14) counties in the state, it is important to note that only 37% of the population is considered rural (Missouri Department of Health and Senior Services, 2017). However, it is interesting to note that despite the concentration of services in urban areas, rural providers in the same state have reported receiving more frequent and advanced human trafficking training than urban providers in this study (Preble et al., 2020). While this demonstrates that statewide agencies and rural providers are invested in learning about and responding to human trafficking, there is a clear need for more research around how to best address this service gap to meet the needs of identified survivors.
Limitations
The study’s findings should be interpreted in the context of its limitations. The sampling methodology may be a limitation for interpreting the findings regarding service gaps. As noted, there was no previously existing sampling frame from which to draw the study sample (i.e. no statewide coordinating body for human trafficking existed at the time of data collection). The responses come from a sample of individuals from a variety of agencies who self-selected into the study. It is not a census of all agencies; without a true sampling frame, it is not possible to know the extent to which the sample is representative of the total population of human trafficking serving agencies in the state.
As service providers representing agencies make up the survey sample, the findings represent the perspectives of service providers only and their opinions and assessments of potential gaps in services provided. Future studies to assess service gaps and the needs of service recipients would benefit from the inclusion of the perspectives of trafficking victims and survivors. Nevertheless, data from providers allow the research team to examine a phenomenon that is extremely sensitive and relatively rare with decreased risk for harm; soliciting provider perspectives on service to this hard-to-reach population takes advantage of their ability to report on experiences over their entire case load.
The findings may also be limited by some measurement error. For questions where providers were asked to indicate the extent to which they perceived each service was needed, the only response options were “all/most needed” or “none needed.” This question would have provided better data if the option “some needed” had been available, and some respondents may have skipped this question as a result if their desired answer choice was not an available option.
Conclusions and implications
The study contributes to the limited body of knowledge regarding existing and needed aftercare services for survivors of sex trafficking. We identified multiple gaps in services in the state of Missouri. Our findings suggest that respondents’ services for victims of sex trafficking may be more concentrated in the few urban areas in the state compared to the wider rural parts of the state. Although provider descriptions indicate that many services are being provided to a range of victims of sex trafficking, notable gaps remain in providers’ ability to provide adequate housing services, legal assistance, and education assistance. Additionally, although providers report that they are able to serve a number of particularly vulnerable sub-populations such as children, LGBTQ victims, or male victims, there are several groups, such as incarcerated or tribal populations, for whom services may only be available on a very limited basis. Policy makers, funders, and advocates should work to mitigate these shortcomings across the state as well as encourage culturally appropriate responses for these populations.
That most agencies had difficulty providing services in-house should not be surprising, especially in a field in which cross-disciplinary collaboration is seen as best practice. However, what should be concerning is that in a state with apparent concentrations of services in urban areas, interdisciplinary teams may be rare, making accessible and adequate service delivery difficult. This is supported in extant literature (Macy & Johns, 2011; Nichols & Heil, 2015) as well as in requests by these participants for more training in case coordination (Preble et al., 2020). Efforts to increase cross-discipline training, interdisciplinary collaboration, and funding for basic services are needed to ensure adequate and accessible services for survivors are available. In this state, since the collection of these data, organizations have expressed interest in developing streamlined resources and technical assistance across the state, which is a step in a positive direction. Additionally, there is still need for a statewide referral and response system, which may also point to a need for a centralized reporting system for trafficking data, to ensure accurate understandings of the scope of the issue, more accurately determine where gaps in services exist, and how best to steward available funds and resources. More research is needed to explore how systemic resources could be developed to help anti-trafficking professionals better respond to the trends in trafficking occurring throughout the state.
That service providers are serving multiple traumatized populations within the same agency requires further evaluation to ensure that the quality of care is standard and appropriate across all populations. Additional examination is needed to determine whether services that might seem appropriate for trafficked populations are, indeed, sufficient. More research should focus on examining the outcomes of services between parallel service populations to ensure that we are providing helpful, empowering services rather than a makeshift response to lack of services. Statewide, policy makers and advocates should work to ensure that service providers not only have enough resources to best serve these many populations, but also have the support they need to provide these necessary services. This means that agencies may need to advocate for increased funding to have dedicated personnel to handle trafficking cases with the understanding that they will not always have a significant case load. Funders should also be cognizant that lower case loads are preferable given the longevity and intensity these cases require (Futures Without Violence, 2007; Wisconsin Office of Justice Assistance, 2012).
The findings of this study could also suggest the need for a centralized mechanism to be developed as evidenced by (1) a lack of a sampling frame, (2) evidence that agencies experience needs for which they do not know how or where to refer, and (3) the limitation of not being able to do a census in order to truly assess differences in service availability by region. The development of this system would help to ensure current best practices (e.g. trauma-informed services) are adopted throughout the state, support a network of trust and collaboration between all providers, and to mentor new agencies wishing to provide assistance to survivors of trafficking. Future research should explore the efficacy of this claim. Additionally, future research should explore the quality of care across the state for survivors of trafficking. Without a nationally recognized minimum standard of care for serving trafficking survivors in the U.S., anti-trafficking professionals across the state of Missouri may find it difficult to hold accountable or identify areas for improvements among their peers for quality services. To better support these endeavors, more research to develop evidenced-based minimum standards of care in rural settings is needed.
Footnotes
Ethics
This research was approved by the University of Missouri Institutional Review Board #2008437.
Funding
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This research is funded by The University of Missouri Research Council Board. Grant number: URC-17-094-n.
Acknowledgements
The authors would like to thank the providers who contributed to this research, particularly for the work that they do to support the most vulnerable members of our community.