
Abstract
Summary
Social workers’ eating disorder mental health literacy (ED-MHL) is essential to the detection, assessment, and treatment of eating disorders (EDs) and disordered eating (DE) in clinical practice. This study explored social workers’ ED-MHL, particularly the assessment practices of EDs on intake forms, and within the first two therapy sessions. Participants in this national survey were N = 316 outpatient masters-level social workers in the United States. Participants completed an online survey measuring ED assessment practices in clinical practice.
Findings
Results showed that 42.4% (n = 133) of respondents did not routinely assess for EDs/DE on clinical intake forms, and 53.2% (n = 165) did not assess within the first two therapy sessions. However, those with recent training related to EDs were more likely to assess. Participants reported low to moderate perceived comfort levels with the assessment of EDs, and training and education were identified as needed resources. Social workers reported deficits in their own assessment practices of EDs. Barriers included: lack of training about EDs/DE; uncertainty about process questions to ask; and perceptions that EDs/DE are rarely the client's primary presenting problem.
Applications
Difficulties with detection and screening practices appeared contingent on gaps in existing education and training related to EDs/DE. These findings suggest that future research may serve to increase social workers’ ED-MHL, as underscored by the noteworthy finding that 86.1% (n = 229) of the sample reported that they would make proactive changes in their clinical practice, as a direct result of participating in this study.
Introduction
Eating disorders (EDs) are biologically based, serious mental illnesses (Klump, Bulik, Kaye, Treasure, & Tyson, 2009). Common feeding and EDs are binge ED, anorexia nervosa, and bulimia nervosa (American Psychiatric Association [APA], 2013). A recent worldwide review about the prevalence rates of EDs between 2000 and 2018 found the weighted means of lifetime EDs were 8.4% and 2.2% for women and men, respectively; and, the means of 12-month prevalence were 2.2% for women and 0.7% for men (Galmiche et al., 2019). The most common ED worldwide is binge ED with global mean lifetime prevalence of 2.8% in women and 1.0% in men (Galmiche et al., 2019). For anorexia nervosa, the global mean lifetime prevalence rate is 1.4% and 0.2% for women and men, respectively; for bulimia nervosa, the rates are 1.9% and 0.6% for women and men, respectively (Galmiche et al., 2019).
Background
Anorexia nervosa is characterized by body image disturbance, intense fear of gaining weight, and dietary restriction that leads to significantly low body weight (APA, 2013). Individuals with anorexia nervosa also may engage in periodic binge eating (i.e., consuming large amounts of food while feeling out of control) or purging (i.e., self-induced vomiting or the misuse of laxatives, diuretics, or enemas) (APA, 2013). Bulimia nervosa is characterized by body image disturbance, and recurrent episodes of binge eating accompanied by compensatory behaviors (e.g., self-induced vomiting, diuretics, laxatives, over-exercise) in order to prevent weight gain often associated with binge eating (APA, 2013). Binge ED is characterized by episodes of binge eating without the presence of compensatory behaviors (APA, 2013). Problematic eating behaviors (i.e., restrictive dieting, binging, purging, emotional eating) that occur less frequently and/or, are less severe are often labeled as disordered eating (DE) (Jacobi et al., 2012; Yager et al., 2014). Thus, DE refers to behaviors associated with distress that may be related to, but do not meet, criteria for a clinically significant ED (Vela et al., 2021; Yager et al., 2014).
Eating disorders are rarely stand-alone diagnoses and occur in conjunction with other psychiatric illnesses; rates of comorbidity can vary based on ED diagnosis and subtype (Godart et al., 2007). For example, in a review of the literature on comorbidity studies of EDs and mood disorders, Godart et al. (2007) found that comorbidity rates for bulimia nervosa and depressive disorders ranged from 24% to 90%, and for anorexia nervosa, comorbidity rates ranged from 31% to 89%. Obsessive-compulsive disorder is more frequent in anorexia nervosa than bulimia nervosa (Mandelli et al., 2020), while substance use disorders are more prevalent in bulimia nervosa and binge ED than anorexia nervosa (Bahji et al., 2019). Post-traumatic stress disorder is common in individuals with EDs, regardless of ED subtype (Ferrell et al., 2022). Overall, EDs are highly comorbid with a range of anxiety, mood, trauma, substance use, and personality disorders (APA, 2013).
Regardless of such prevalence and severity, EDs often go undetected, which renders them as a public health issue (Austin, 2012; Worsfold & Sheffield, 2018). Unfortunately, most individuals suffering from EDs never receive treatment, even though some research has shown that individuals often consult their health care practitioners about them (Mond, Myers, et al., 2010). Even when visiting general health care practitioners, only one-third reported directly being asked about their eating problems (Mond, Myers, et al., 2010). In a systematic review of ED-specific treatment seeking among community cases, Hart et al. (2011) found that, on average, 23% of individuals with diagnosable EDs seek outpatient ED-specific treatment, as it is more common for individuals to utilize health services and primary care for weight loss, anxiety, depression, and comorbid physical illnesses instead (Mond et al., 2007; Mond, Myers, et al., 2010; Van Son et al., 2012). Despite individuals seeking treatment or primary health care for other problems (Hart et al., 2011), this does not preclude health care and mental health providers from inquiring about and assessing for co-occurring problems with EDs.
Research has shown that individuals with EDs often seek services for anxiety, depression, and/or other mental health concerns from generalist, outpatient mental health providers (Fursland & Watson, 2014). Despite the rising prevalence rates of EDs (Galmiche et al., 2019; Hudson et al., 2007), elevated mortality and morbidity rates of EDs (Chesney et al., 2014; Mehler & Brown, 2015), and health care costs associated with EDs (Agras, 2001; Mitchell et al., 2009), there is room for growth in the awareness of the seriousness and complexities of EDs among many medical and mental health professionals, including clinical social workers (Ali et al., 2017).
Regardless of the fact that EDs may be masked in their clinical presentation, they have devastating financial, educational, and medical consequences, and costs for the individual, family, and health care systems are substantial (Agras, 2001; Mitchell et al., 2009). Early detection and prevention are essential, as individuals with more severe EDs report stronger barriers to seeking treatment, including fear of change, fear of losing control, and lower motivation to change (Griffiths et al., 2018). Given that social workers provide the majority of mental health services in the United States (National Association of Social Workers [NASW], n.d.), they become essential gatekeepers to this subpopulation. Outpatient social workers need a basic working knowledge of EDs in order to adequately identify and assess their presence in outpatient practice. Evaluating outpatient social workers’ eating disorder mental health literacy (ED-MHL), particularly within their assessment practices, or lack thereof, is critical for timely and appropriate care for clients with EDs.
Mental health literacy
Mental health literacy (MHL) is defined as “knowledge and beliefs about mental disorders which aid their recognition, management, or prevention” (Jorm et al., 1997, p. 182). Jorm and colleagues coined this term as an extension of health literacy, in order to address the lack of action and research related to public knowledge of mental disorders and mental health. They also frequently noted multiple components of MHL, namely: recognition of when a mental health disorder is developing; knowledge of how to prevent mental disorders; knowledge of risk factors, causes, and available treatment options; knowledge of self-help strategies for milder problems; and possession of skills to help others who are experiencing mental health crises or who are developing a mental disorder (Jorm et al., 1997; Jorm, 2012). Often, mental health providers cannot recognize when EDs are developing or exist if they do not screen and assess this neglected population (Fursland & Watson, 2014).
In the past two decades, extant studies have explored allied health and medical professionals’ self-perceived knowledge of EDs and skills, as well as their screening and assessment practices (Currin et al., 2009; Hay et al., 2005, 2007; Jones et al., 2013; Linville et al., 2012, 2010; Mond et al., 2007; Worsfold & Sheffield, 2018, 2019). Taken together, these studies often noted poor screening, and/or assessments practices. In a study of N = 260 individuals at an Australian outpatient mental health clinic, Fursland and Watson (2014) incorporated a five-item screening questionnaire (i.e., the SCOFF; Morgan et al., 1999) and found that 7.3% of participants met criteria for an ED, yet all had been clinically undetected by the referring psychiatrist, psychologist, or referring general practitioner. A study by Linville et al. (2012) found that 68% of medical providers (e.g., nurse practitioners and general practitioners) “did not think to screen for an eating disorder” since it was not the presenting problem. In a study of N = 153 primary care physicians and psychologists in Canada, Lafrance Robinson et al. (2012) found that only 16% reported that they “always” assessed for EDs among children and adolescents. Overall, such studies have focused predominantly on medical professionals. However, understanding the knowledge and assessment practices of other health care and mental health professionals is also necessary, as individuals with EDs are more likely to seek services for a variety of other co-occurring presenting concerns (Hart et al., 2011; Mond et al., 2007; Mond, Myers, et al., 2010; Van Son et al., 2012). Universal screening among mental health professionals, particularly social workers, may also contribute to earlier detection, diagnosis, and intervention.
Eating disorder mental health literacy
Inadequate, and/or nonexistent ED-MHL among practitioners can negatively affect early detection, intervention, management of medical risk, and/or utilization of evidence-based treatments (Jones et al., 2013). Practitioners’ perceived knowledge of EDs and skills also impacts their clinical practice behaviors. Australian researchers (Worsfold and Sheffield, 2019) assessed ED-MHL using a fictional vignette of a female experiencing a subthreshold variant (e.g., bulimia without purging). They reported that almost two-thirds of the sampled practitioners, consisting of psychologists, naturopaths, and fitness instructors, believed the issue was not an ED. Studies investigating the ED-MHL of individuals suffering with EDs and of various practitioners often have utilized a fictional case vignette to examine participants’ abilities to detect EDs along with the corresponding knowledge, perceptions, and/or attitudes about the etiology and treatment of EDs (Hay et al., 2005; 2007; Jones et al., 2013; Mond, Hay, et al., 2010; Morgan et al., 1999; Worsfold & Sheffield, 2019). Other research has highlighted components of ED-MHL that focus more on specific clinical practice behaviors and knowledge, such as assessment practices, referral practices, interventions, and/or provision of evidence-based treatments (Worsfold & Sheffield, 2018).
To date, there are no known or published studies that have focused specifically on understanding the assessment practices of EDs among outpatient clinical social workers. This study extended the concept of ED-MHL to licensed professionals and investigated the ED-MHL of licensed clinical social workers, specifically related to the area of ED assessment. The current study had two related aims. First, it sought to explore, identify, and describe assessment practices relevant to EDs/DE, including barriers encountered on intake forms, and within the first two therapy sessions among practicing outpatient social workers. Second, it examined social workers’ perceived comfort levels with such assessment practices.
Methods
Participants
Participants in this online, exploratory descriptive survey study were N = 316 outpatient social workers in the United States who: a) had a master's degree in social work; b) had at least two years of clinical experience; c) worked at least part-time in private practice or with a group practice; and, d) did not currently identify themselves as ED specialists. Their mean age was 51.13 (SD = 13.74) and 85.7% (n = 269) were female. The sample majority was Caucasian (90.8%, n = 286); practicing in a city/urban community (61.3%, n = 192); and living primarily in the northeast United States (37.8%, n = 119). The average number of years in clinical practice was 17.22 (SD = 12.58), and the average number of training hours specifically related to EDs in the last five years was 3.78 (SD = 7.10).
Procedures
This research was part of a larger doctoral dissertation study conducted in 2015–2016 by the author. All participants gave written permission for their anonymous and confidential data to be used in this study. Ethical approval was obtained by the Human Subjects Review Committee at Smith College School for Social Work (Reference number 2015–820). Data were collected variously by: a snowball method; using web-based recruitment advertising via social media (e.g., Facebook, LinkedIn); and, email recruitment, and/or newsletter advertising through various state branches of the National Association of Social Workers or other state clinical social work societies. Due to the recruitment methods used that incorporated advertisements via various social media sites as well as emails to state societies for clinical social work, an overall and more precise response rate was unable to be determined. The recruitment advertisement identified an aim to understand more about outpatient clinical social workers’ assessment practices of and comfort levels with EDs. Participants were then invited to complete an anonymous, confidential online survey via Survey Monkey. A thank you page that included a list of resources related to EDs was provided to participants after 30 questions were completed. Once participants clicked “done” at the end, they were automatically redirected to a separate form which could not, in any way, be linked to their responses in the survey. On a separate form, participants were able to enter their contact information and select incentives in which they were interested. Participants could opt for any or all of the following three incentives: 1) registering for an online draw for one of five $40.00 Amazon gift cards, 2) access to a free one-hour webinar/PowerPoint on EDs developed by the researcher, and/or, 3) obtaining study results. Individuals who did not meet eligibility criteria were directed to an exclusion page that thanked them for their interest in the study, informed them that they were ineligible, and provided a list of resources related to EDs.
Measures
In order to explore social workers’ clinical practice behaviors and experiences related to EDs, this study explored: a) assessment practices relevant to and knowledge of EDs; b) the extent of ED training among a group of non-ED specialist social workers; and c) professional, personal, and demographic factors impacting the assessment process. Participants completed the 30-item survey assessing assessment practices, knowledge, and perceived comfort levels with EDs/DE in their clinical practice. It was compiled from items developed in a previous study by Linville et al. (2012) who demonstrated a resultant three-factor solution (knowledge, skills, resources) via confirmatory factor analyses and items assessing self-perceived knowledge. Then, items developed by the author that examined personal and professional variables were added and pretested. Overall, the survey included: 5 items about demographics; 13 items related to assessment processes and perceived knowledge of EDs in clinical practice; 4 items related to professional background and training; 5 items related to practitioners’ specific personal experiences of weight loss and DE; 2 items related to consultation practices and theoretical orientations; and 1 item that asked participants what they may choose to change in their practices, as a result of participating in the survey. There were also four open-ended questions included in the total 30 items; responses were coded by the author. A content analysis was conducted on the responses to the open-ended questions in order to code, quantify, and then tabulate the occurrences of certain forms of content (i.e., words/phrases).
Items used to analyze assessment practices included questions that asked if participants saw clients with EDs/DE in their own practice, and assessed them on intake forms, and/or within the first two therapy sessions. Additional items addressed how social workers assessed; reasons for not assessing; an open-ended question about resources needed to better assess; how they intervened; other providers to whom they refer; and, their perceived, present comfort levels with assessment. Response formats were dichotomous (yes/no) and multiple-response options (select all that apply). Using a six-point Likert scale, participants also were asked to rate how strongly they agreed or disagreed with the statement: “initial screening and assessment for EDs is important and clinically appropriate, even when the ED or DE is not the client's reported primary presenting problem or concern.” Perceived comfort was assessed using a five-point Likert scale of 1 (very low) to 5 (very high). Lastly, the survey included one item that specifically inquired about other common presenting problems (e.g., depression, trauma) that social workers assess via their intake forms.
Descriptive data were analyzed using IBM SPSS Statistics version 20 (Chicago, IL). Univariate analyses initially were used to determine significant associations between demographic data and item responses using Chi-square tests. Logistic regression assessed what variables predicted whether or not a social worker assessed for EDs on intake forms, and/or within the first two therapy sessions. Content analyses were conducted on the responses to the open-ended questions in order to code, quantify, and then tabulate the occurrences of certain forms of content (i.e., words/phrases). Open-ended responses were categorized based on content, content analyses based on frequencies were calculated, and each response was assigned only one category. A power analysis was conducted prior to data collection to determine the minimum sample size needed (MacCaughelty, 2017).
Results
Of the sample of US social workers (N = 316), 71.3% (n = 221) indicated they saw clients with EDs, and 82.9% (n = 261) saw clients with DE at their places of employment. Even though the majority of practitioners reported they saw clients with EDs/DE in their practices, 42.4% (n = 133) of respondents did not routinely assess for EDs/DE via specific questions on clinical intake forms. Further, 29.3% (n = 92) reported not using any intake forms in their clinical practice, while only 28.3% (n = 89) reported including EDs/DE on their intake forms. Similar to the initial inquiry on intake forms, more participants (53.2%, n = 165) reported not assessing for and inquiring about comorbid EDs/DE within the first two therapy sessions, compared to those (46.8%, n = 145,) who did. In addition, six participants did not answer this item.
Rationale for lack of eating disorders/disordered eating assessment
The sample indicated a variety of reasons that they did not assess for EDs/DE on their intake forms and/or within the first two therapy sessions. Survey participants were asked to select all items that applied. Table 1 presents the frequency of rank-ordered reasons why they did not assess for EDs/DE on intake forms. Similarly, Table 2 shows the frequency of reasons why they did not assess within the first two therapy sessions. In addition, when asked in a separate question to select the top two reasons for not assessing within the first two therapy sessions, “it is often not the primary presenting problem” (43.0%, n = 136) was most common, followed by “there are other co-morbid diagnoses that require more immediate attention” (24.4%, n = 77). Table 3 shows the frequency of common presenting problems for which social workers indicated they assessed via their intake forms.
Most frequently reported reasons by social workers for not assessing eating disorders/disordered eating on intake formsa (N = 316).
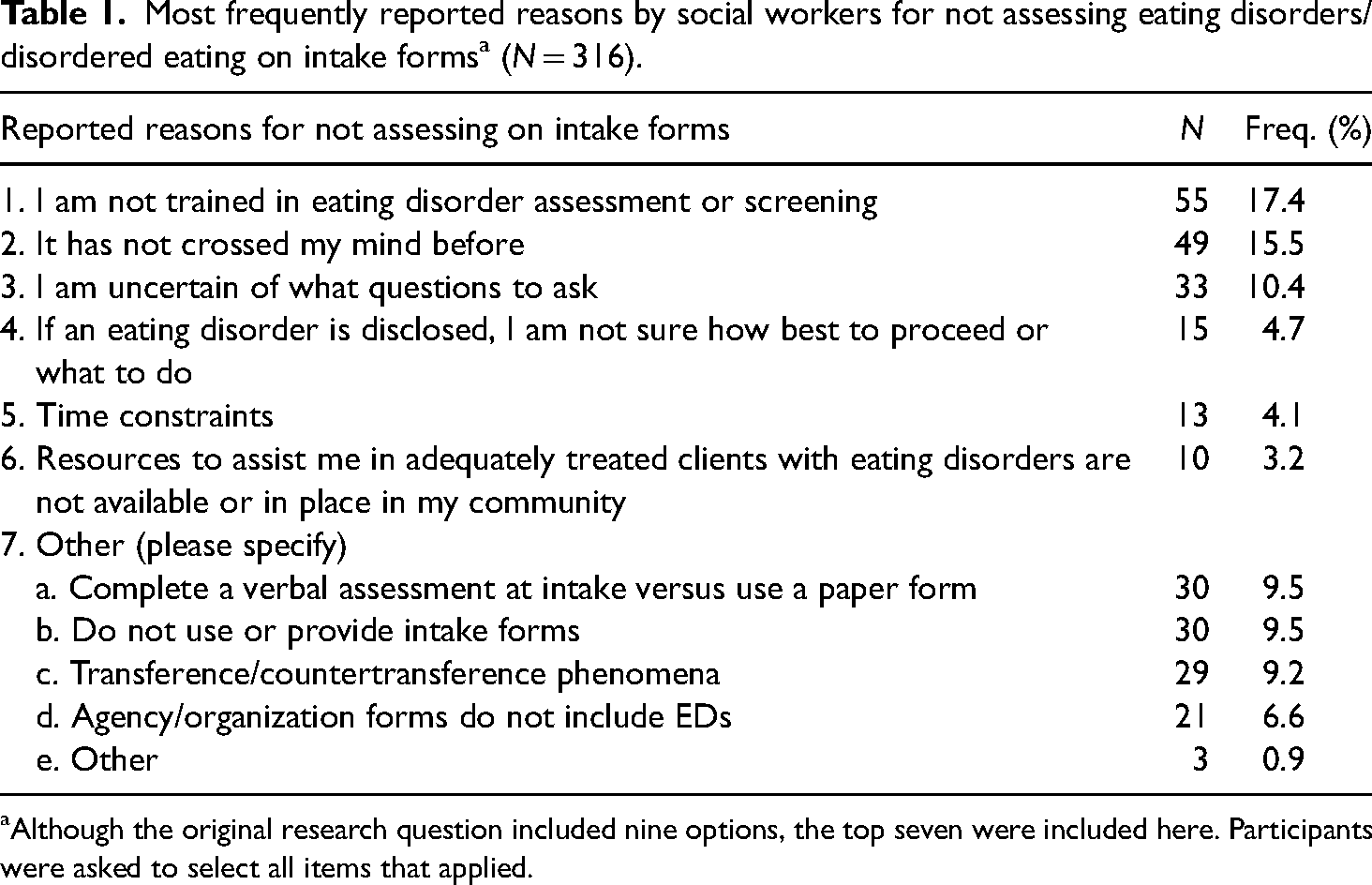
Although the original research question included nine options, the top seven were included here. Participants were asked to select all items that applied.
Most frequently cited reasons for not assessing eating disorders/disordered eating within the initial therapy sessionsa (N = 316).
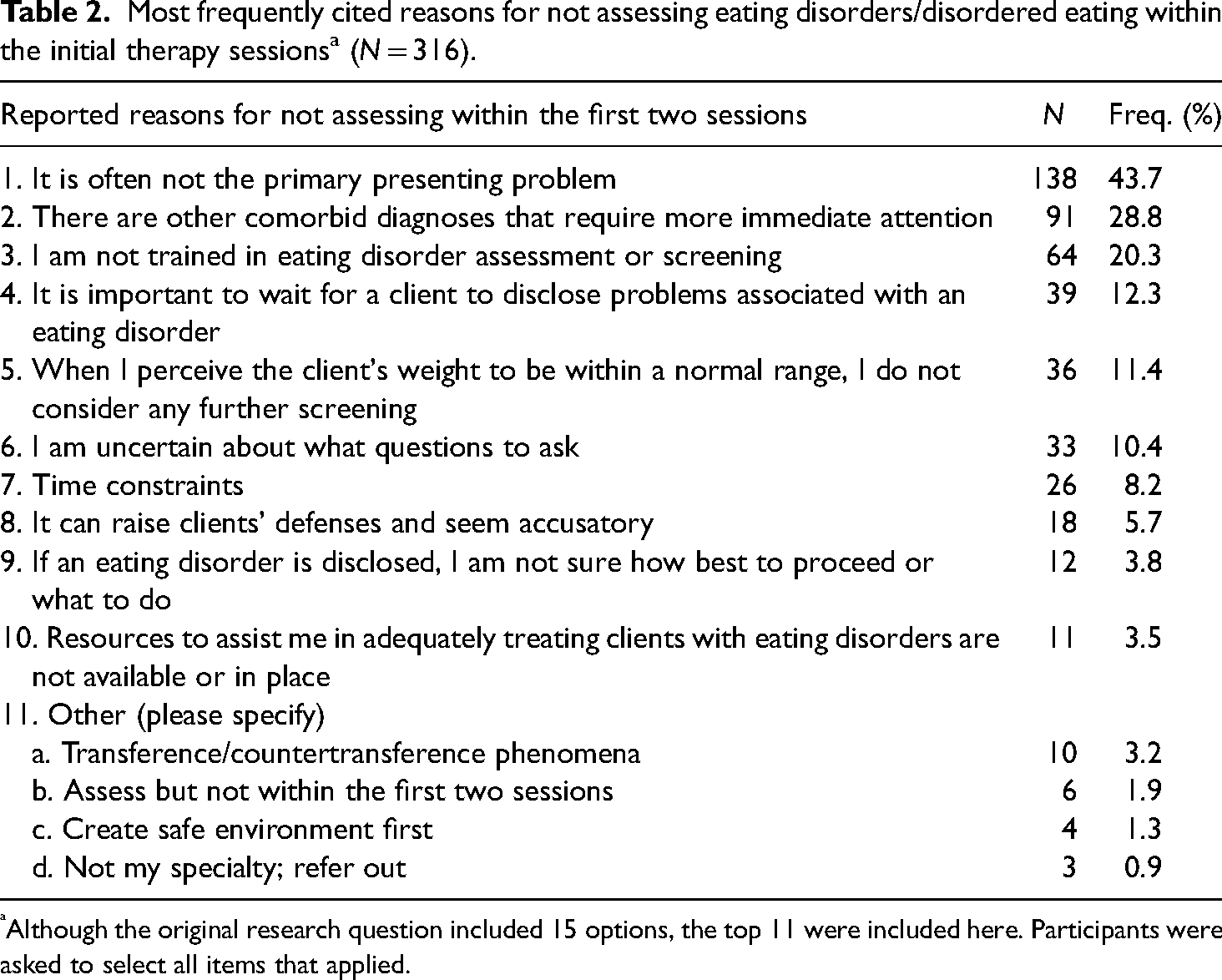
Although the original research question included 15 options, the top 11 were included here. Participants were asked to select all items that applied.
Frequency of most common presenting problems assessed for via intake formsa (N = 316).
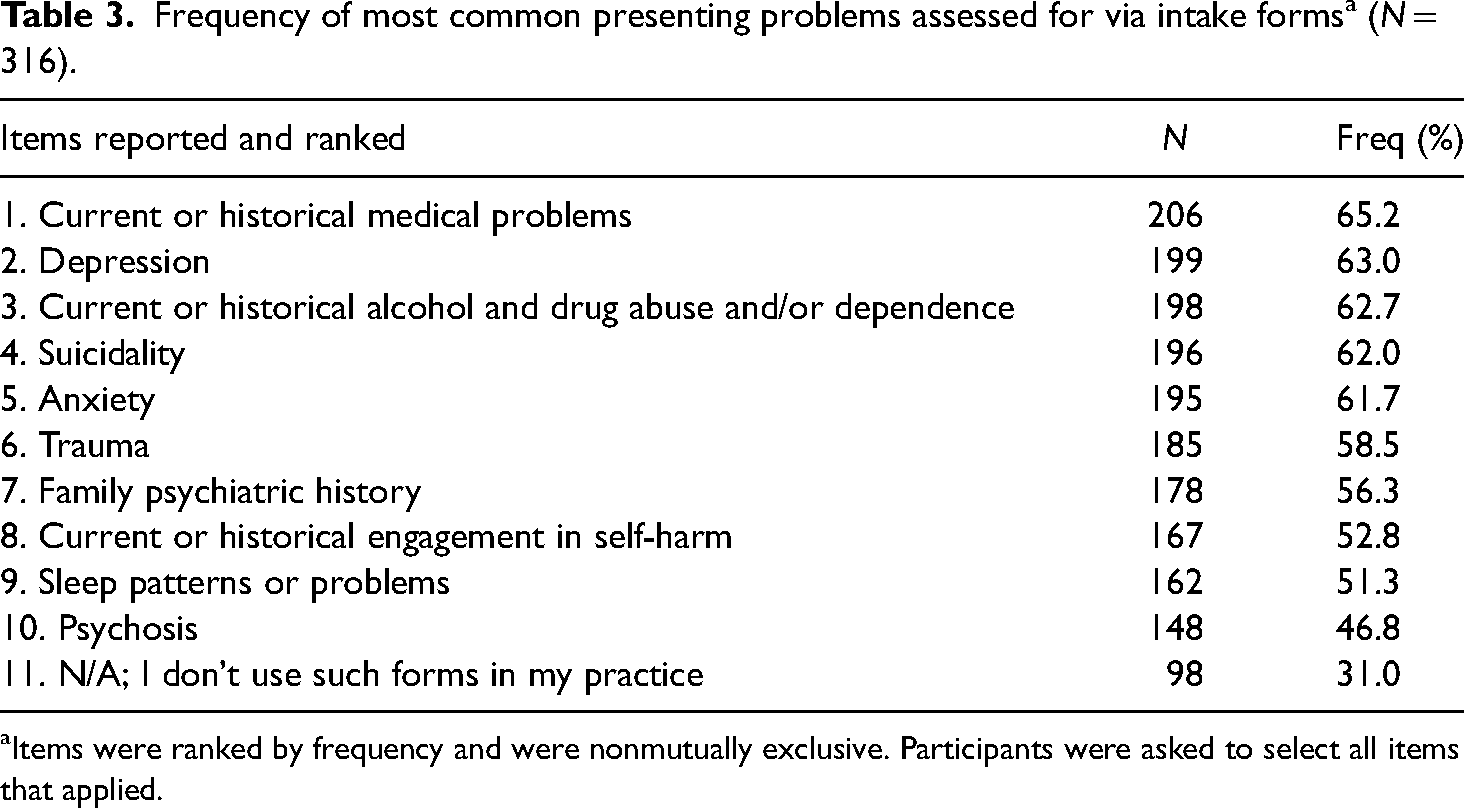
Items were ranked by frequency and were nonmutually exclusive. Participants were asked to select all items that applied.
Despite the fact that 42.4% (n = 133) of participants indicated they did not specifically assess, and/or, inquire about EDs/DE on their clinical intake forms, 53.2% (n = 165) indicated they did not assess them within the first two therapy sessions, and that the verbatim most frequent rationale noted was “it is often not the primary presenting problem,” 85.2% (n = 264) of participants mildly to strongly agreed that initial screening and assessment for EDs is important, even when it is not the client's primary presenting problem (Figure 1). Using a Likert scale of 1 (strongly disagree) to 6 (strongly agree), the mean response was 4.58 (SD = 1.21).
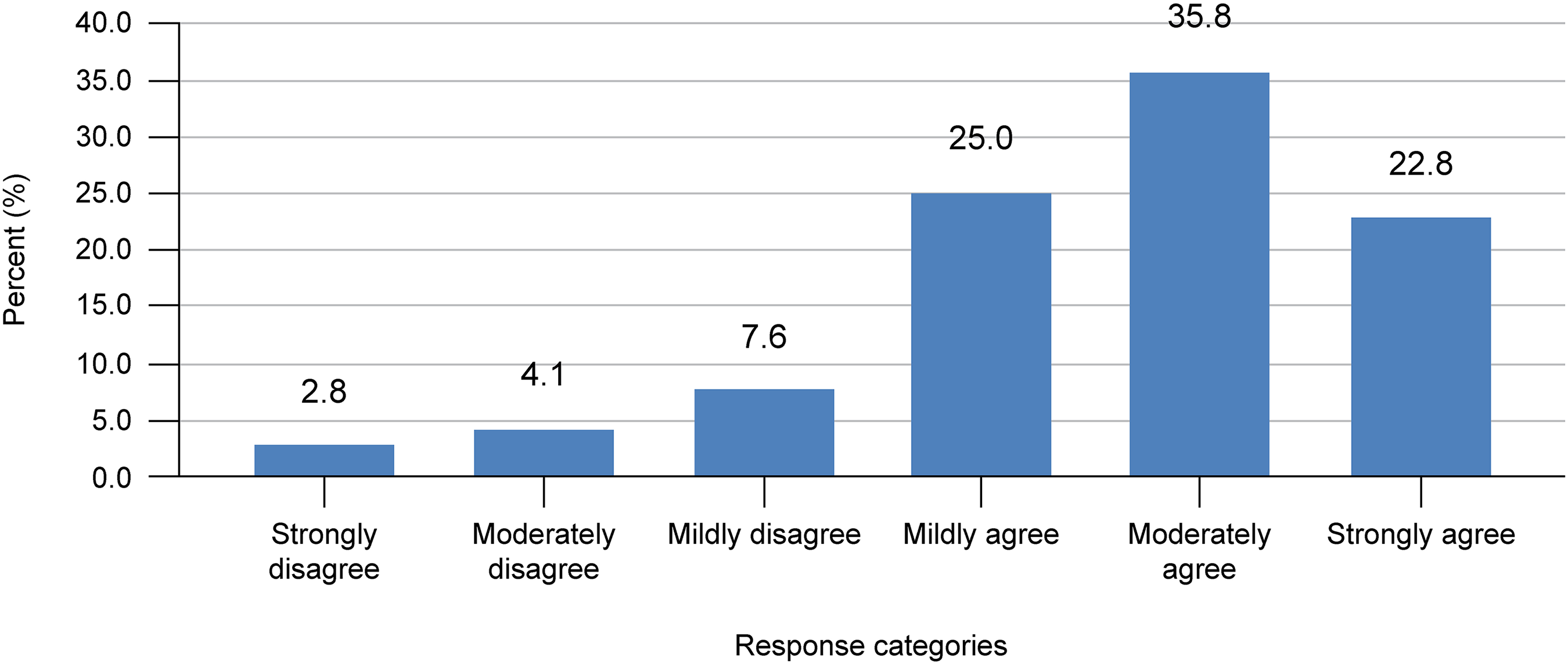
Social Workers’ Agreement or Disagreement about Importance of Initial Screening and Assessment for Eating Disorders.
Moreover, in an open-ended question, participants were asked what resources they needed to better assess clients for EDs. Two hundred and thirty-six participants responded to this query, and n = 80 did not answer this question. A majority of these social workers (47.3%, n = 112) indicated they needed additional education and training, followed by screening tools and questionnaires (23.2%, n = 55).
Impact of training hours on assessment
Correlation analyses were used to determine whether there was an association between training hours and assessment on intake forms and within the first two therapy sessions. The number of training hours specifically related to EDs received in the last five years and initial assessment of EDs/DE on intake forms were significantly positively correlated, r (219) = .15, p = .03. Furthermore, initial assessment on clinical intake forms and assessment within the first two therapy sessions were significantly positively correlated, r (221) = .60, p < .001. As shown in Table 4, the logistic regression revealed that only training hours reliably predicted the initial assessment of EDs/DE on their clinical intake forms, (Exp(B) = 1.06, p = .03). Furthermore, social workers with more training were more likely to include questions about EDs/DE on their intake forms.
Regression model predicting assessment of eating disorders and disordered eating on clinical intake forms (N = 316).
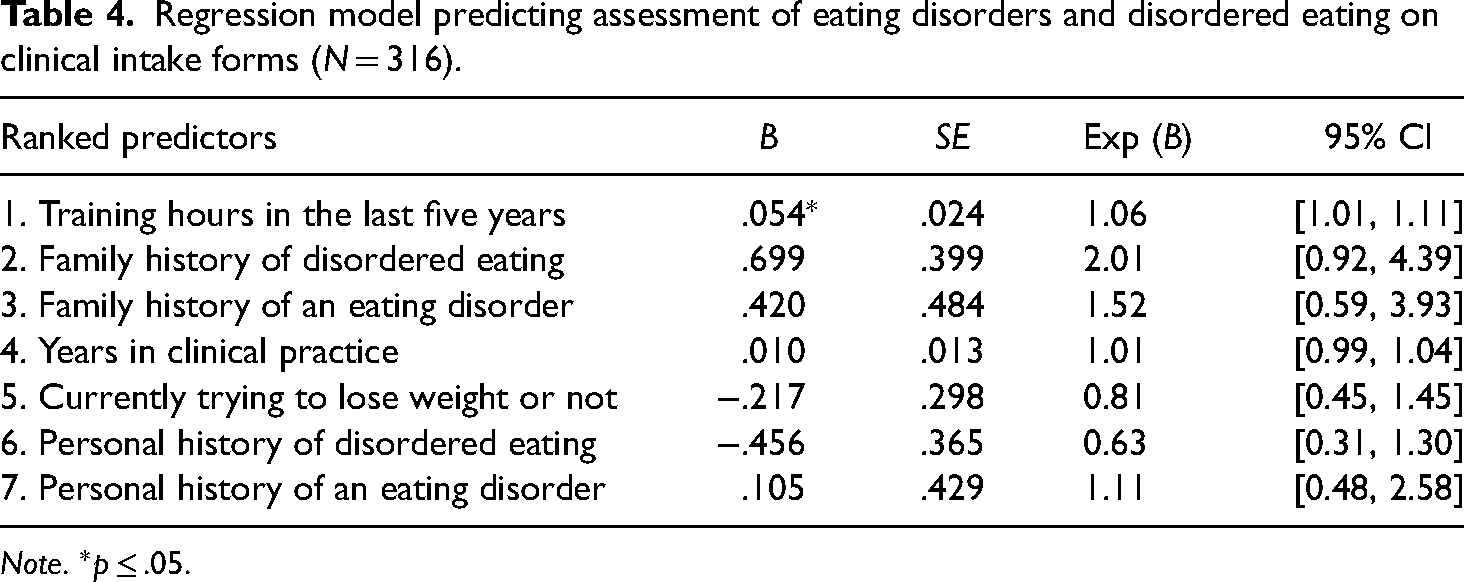
Note. *p ≤ .05.
Perceived comfort levels
Overall, participants’ perceived comfort levels in assessing for EDs were found in the low to moderate range. Participants’ average comfort level was 2.65 (SD = .89), as they were asked to rate their comfort level in assessing for EDs from 1 (very low) to 5 (very high). Perceived comfort levels in assessing for and treating EDs, and the number of training hours specifically related to EDs in the last five years, were statistically positively correlated, r (309) = .32, p < .001. However, there was no significant correlation between perceived comfort levels in assessing for and treating EDs, and the number of years in clinical practice, r (312) = .10, p = .09. The noted lack of training and education in EDs (26.7%, n = 75) was the most frequently endorsed response provided, in the open-ended question about what contributed to social workers’ perceived lack of comfort with conducting assessments.
Discussion
This study sought to fill a noted empirical gap in the ED-MHL literature related to outpatient social workers’ clinical practices. To the author's knowledge, the present study is the largest survey that has explored the assessment practices of EDs/DE on intake forms, and/or, within the first two therapy sessions among healthcare professionals, and the first in clinical social work. The robust sample of graduate degree–level practitioners was larger than anticipated and reinforced the perceived importance of the subject matter overall. Previous studies on ED-MHL for health care professionals had much smaller sample sizes (Hay et al., 2005, 2007; Jones et al., 2013; Worsfold & Sheffield, 2018, 2019).
A majority of these social workers reported seeing clients with EDs (71%, n = 221) and DE (82.9%, n = 261) in their day-to-day practices. Notably, 42.4% (n = 133) did not include any types of questions related to EDs/DE on their intake forms, and another 29.3% (n = 92) reported not using intake forms at all. However, the sample reported assessing other common problems via intake forms, including: medical problems, depression, substance use, suicidality, anxiety, and trauma. The fact that over 40% did not assess for EDs/DE on intake forms, yet they assessed for mental health disorders that commonly co-occur with EDs (APA, 2013; Hudson et al., 2007) is concerning. Without specifically assessing for EDs/DE, it may lead social work practitioners to focus on associated comorbidities, while leaving the EDs/DE undetected. Asking about and assessing multiple areas of physical and mental health is part of a comprehensive biopsychosocial assessment (Burns, et al., 2019), a form of assessment that social workers often tout as important and preferred because it is client-centered. Providers omitting questions about EDs/DE as part of a biopsychosocial assessment may be inadvertently create a large gap in social work practice.
Previous research has shown that highly educated health professionals may neglect to ask those with EDs about eating problems (Mond, Myers, et al., 2010). In this study, despite all having formal, masters’ degree–level social work education, 15% (n = 49) of the sample did not ask or screen individuals for EDs/DE, endorsing “it has not crossed my mind before.” Other participants noted that they did not because they “were not trained in eating disorder assessment in screening.” This was similar to Worsfold and Sheffield's (2018) research which found 87.7% of psychologists, naturopaths, and fitness instructors indicated being unable to properly treat clients, with the primary reason reported to be lack of skills (52.6%). This was also evident among a sample of medical practitioners (e.g., general practitioners, nurses, pediatricians, obstetricians) surveyed by Linville et al. (2010); a Canadian sample of primary care physicians and psychologists (Lafrance Robinson et al., 2013); and in a study of gynecologists and obstetricians in the UK that found only 20% were confident in their ability to identify EDs in practice, and 27% never inquired about or assessed for EDs in women who were pregnant (Morgan et al., 1999).
In regard to not assessing for EDs/DE within the initial therapy sessions, nearly three-fourths of the study sample herein noted it was often not the primary presenting problem, and that there were other comorbid diagnoses that required more immediate attention (see Table 2). Similarly, another study of nonsocial workers found that almost 75% of their sample of psychologists, naturopaths, and fitness instructors were reluctant to screen clients “as eating disorder symptoms were typically not the presenting issue” (Worsfold & Sheffield, 2019, p. 1268). Linville et al. (2012) national survey study also found that 68% of primary care providers (PCPs) did not think to screen or assess for EDs, as it was not the presenting concern. Given that this study sample often did not view EDs as the primary presenting problem, this may contribute to poorer detection, and thus more delayed interventions for this vulnerable population. An additional finding worth noting was the fact that 85.2% of participants mildly to strongly agreed that initial screening and assessment for EDs/DE is important, even when it is not the client's primary presenting problem. This finding was unique in that it demonstrated the majority of social workers herein endorsed the importance of initial screening and assessment for EDs/DE, yet they lacked the necessary education and training.
Given that MHL is knowledge linked to the possibility of action (Jorm, 2012), this study found that training received in the last five years specifically related to EDs was significantly associated with social workers’ assessment practices of EDs/DE, perceived comfort levels, knowledge, and consultation or supervision practices. Thus, training and education serve as a bridge between knowledge and action.
Implications for clinical practice
Study results revealed that this sample of social workers was similar to other health care professionals cited in the extant literature. Specifically, they had various deficits in their assessment practices and were not comfortable assessing EDs/DE. The noted difficulties with detection and screening practices appeared contingent on gaps in existing education and training related to EDs/DE. Future research may provide a potent means for increasing and assessing various aspects of ED-MHL. As such, the survey instrument itself functioned as a type of educational intervention, and additional research may have the ability to initiate needed change, as evidenced by the noteworthy finding that 86.1% (n = 229) of the sample reported that they would make proactive changes in their clinical practice, as a direct result of participating in this study. The most frequent changes cited were: to seek additional education and training (30.4%, n = 96); followed by asking directly/assessing for EDs/DE (17.7%; n = 56); and, revising/updating their clinical intake forms (7.9%, n = 25). Regardless of the number of years of one's clinical experience, these social workers noted a need for more continuing education and training about EDs/DE.
Given this identified need and the gatekeeper function of social workers, by seeking more education and training, they could improve universal screening for EDs/DE and other mental health problems. Results revealed practitioners need awareness of simple screening measures such as the SCOFF (Morgan et al., 1999). However, since EDs are a heterogenous group, future research investigating different tools for detection, assessment, and treatment of EDs is needed.
Furthermore, given the participants’ desire for more education and training specific to EDs/DE, it would be prudent for EDs to be included and discussed in undergraduate and graduate social work education. Over half of the study's sample reported either not taking an undergraduate or graduate course or seminar on EDs or not having one offered. In addition, over half of the sample reported never having an instructor lecture on EDs in undergraduate or graduate classes. In order to adequately prepare clinical social workers to provide biopsychosocial assessments, which include aspects of both physical and mental health, schools of social work need to include EDs/DE more fully in their curricula.
Lastly, by seeking more education and training specific to EDs/DEs, social workers may take on a proactive leadership role, particularly when working as a member of a multidisciplinary team. In Holosko's (2009) well-cited article on social work leadership, he noted that the social work profession has a long and storied history about not providing much professional leadership within health care settings and organizations. He contended that the social work profession lacked basic education and training about the actual concept of leadership and minimal knowledge about its core five skills. These were: vision; influencing others to act; teamwork/collaboration; problem-solving capacity; and creating positive change (p. 454).
Thus, as outpatient clinical social workers enquire specifically about and assess for EDs/DE, they may take on a leadership role on multidisciplinary teams. By building their ED-MHL, social workers can incorporate their practice knowledge with leadership skills and collaborate with cognate disciplines, family members of clients with EDs/DE, and most importantly, individuals suffering from EDs/DE.
Limitations of the study
First, the sample was disproportionately female and Caucasian. Although the sample size makes such findings more generalizable, the findings do not adequately capture the ED-MHL of social workers who are males and social workers who are from racial minorities. Second, given that a convenience sample was used, with recruitment occurring via social media, a precise overall response rate was unable to be statistically determined. Generalizability for future studies could be improved with random sampling and more incorporation of other health care disciplines in order to detect between-group differences. Finally, this study did not include a fictional case vignette to further assess ED-MHL, and this may be an important addition to future studies, given its current use.
Conclusion
The present study filled a distinct void in the literature, as no prior studies have assessed the ED-MHL of outpatient clinical social workers (in the United States). Furthermore, this study highlighted the need for improvements in the overall assessment practices and perceived comfort levels with EDs/DE among outpatient social workers. Related to the concept of MHL, different health care professionals, including social workers, need to be more aware of areas where they lack a basic literacy of EDs/DE. This sample identified many areas where such deficiencies existed. Overall, a baseline level of ED-MHL is not synonymous with social work practitioners needing to specialize in EDs/DE. Rather, such a baseline level is needed, in order for social work professionals to advocate for this vulnerable population, assess for the presence of EDs/DE in clinical practice, and to make more appropriate referrals for treatment. In sum, more empirical studies related to ED-MHL are needed for social workers and other cognate disciplines working in various mental health fields.
Footnotes
Ethics
Ethical approval for this project was given by Smith College School for Social Work Institutional Review Board [Ref number 2015-820].
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Acknowledgments
The author would like to thank Drs. Michael J. Holosko, Carolyn Mak, and Marsha Kline Pruett for their assistance with this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, [CRM], upon reasonable request.