
Abstract
Summary
Accumulating evidence indicates the multifaceted nature of social support. Although support seekers may receive help, they may also encounter upsetting responses. It remains unclear how seeking and receiving social support, when differentiated, are associated with individuals’ strengths and well-being. This study collected survey data from 357 adults recruited from the southeastern United States. We classified participants using the factors of support seeking and support received into four groups: Interconnected (high on support seeking and receiving), Tended (low on support seeking, high on support receiving), Rebuffed (high on support seeking, low on support receiving), and Isolated (low on support seeking and receiving). We then examined the differences among groups.
Findings
The study found significant differences among the four groups in measures of regulatory strengths, meaning-making strengths, interpersonal strengths, and perceived well-being. In general, the Interconnected group scored highest among the four groups, followed by the Tended group, the Rebuffed group, and lastly, the Isolated group.
Applications
The finding that the Rebuffed group did not score significantly lower than the Isolated group underscores the importance of support seeking. Individuals may benefit from the support seeking process even though they do not obtain the support needed. Social work practitioners should facilitate and optimize their clients’ support seeking, including removing clients’ barriers to support seeking and addressing clients’ negative experiences in the support seeking process. Social work researchers should measure multiple aspects of social support, including support received and support seeking.
Prior research on social support tends to focus either on support received or support seeking. Accumulating evidence, however, has indicated the multifaceted nature of social support. Although support seekers may receive help, they may also encounter unsupportive or upsetting responses (Ingram et al., 1999; Sangalang & Gee, 2012). Although numerous studies (Cook-Craig & Koehly, 2011; Lee & Hwang, 2014; Schwartz & Frohner, 2005; Shen et al., 2004) have demonstrated the importance of social support for sustaining well-being and other outcomes, it remains unclear how seeking and receiving social support, when differentiated, are associated with individuals’ strengths and well-being. To examine how the dual factors—social support received and seeking—are associated with individuals’ strengths and well-being, we classified the study participants using seeking and receiving social support and investigated associations with individuals’ strengths and well-being. Social support was conceptualized to include both informal and formal support and includes different forms of support, such as emotional and instrumental support. This study extends the inquiry in examining seeking and receiving social support in youth (Hamby et al., 2020) by analyzing social support and its associations with the strengths and well-being of an adult sample. We first classified the study participants into four groups: Interconnected (high on support seeking and receiving), Tended (low on support seeking, high on support receiving), Rebuffed (high on support seeking, low on support receiving), and Isolated (low on support seeking and receiving). We then examined differences between the four groups in measures of regulatory strengths, meaning-making strengths, interpersonal strengths, and perceived well-being. This study provides empirical evidence on the importance of examining seeking and receiving support simultaneously.
Social support as a protective factor
The importance of social support (providing tangible or intangible resources to help someone) in social work practice is evident. Existing literature has found significant associations between social support and desired outcomes, including physical functioning (Shen et al., 2004), psychological well-being (Lee & Hwang, 2014), quality of life (Schwartz & Frohner, 2005), and housing stability (Cook-Craig & Koehly, 2011). The lack of social support is linked to numerous undesired outcomes, such as depressive symptoms (Bedaso et al., 2021; Kim et al., 2017), anxiety symptoms (Bedaso et al., 2021), and late rent payment (Martin-West, 2019).
Prior studies have found that social support can mitigate the effects of stress on individuals. A survey with a sample of undergraduate social work students found a positive moderating effect of friend support on the association between academic stress and resilience, suggesting that friend support is an effective coping resource for social work students (Wilks & Spivey, 2010). Similarly, using the Behavioral Risk Factor Surveillance System (BRFSS) data, a study found that social support can mitigate the association between mental health needs and engaging in HIV risk behavior for men (Fang et al., 2019). Social support was also found to play an important role in low-income mothers’ mental health. Analyzing data from a sample of mothers with children in mental health care, a study found that economic stress was associated with depressive symptoms and appeared to exert part of its effect by reducing social support (Gjesfjeld et al., 2010). These studies, taken together, imply that social work interventions can aim to strengthen the social work population's support network, as evidence indicates that social support serves as a protective factor mitigating the effects of stressful, adverse events on individuals.
Interventions to strengthen social support
The concept of social support is not unfamiliar in social work assessment and interventions. In social work practice, it is critical to assess the structure (e.g., existence and quantity of social relationships) and function (e.g., whether the social relationships serve the needed functions) of a client's social network as they inform case planning and service delivery (Tracy & Whittaker, 1990). Enhancing social support can also be a specific targeted goal in an intervention (Hogan et al., 2002). For instance, social support interventions may directly provide emotional, informational, and instrumental support (e.g., professional-led or peer-led social support group), or social skills training (e.g., expressing feelings, conflict resolution) to help participants increase social networks and improve perceived support (Hogan et al., 2002). Social support interventions can be categorized as dyadic interventions (e.g., interpersonal exchanges of resources), social network interventions (e.g., mobilizing existing informal sources of resources), mutual aid groups (e.g., creating new links between community members), and community interventions (e.g., participating in actions to address collective needs; Hernández-Plaza et al., 2006).
Available research suggests the efficacy of social support interventions. Jason et al. (2010) evaluated a support buddy intervention with individuals with chronic fatigue syndrome. The study found that individuals receiving the support intervention had a greater reduction in fatigue severity and an increase in vitality, compared to the control group with no support intervention. Czaja et al. (2013) assessed the efficacy of a technology-based social support intervention in supporting caregivers of patients with dementia. The study found that caregivers receiving the intervention reported an increase in positive perceptions of the caregiving experience. A review of 92 studies evaluating the efficacy of social support interventions indicated that over 80% of the reviewed studies reported benefits of support interventions (Hogan et al., 2002).
Multifaceted nature of social support
Social support research tends to conceptualize and measure social support as individual perceptions of support received or availability of support (Dam et al., 2016; Hogan et al., 2002; Taylor, 2011). Commonly used social support measures in social work literature include the Multidimensional Scale of Perceived Social Support (Zimet et al., 1988), the Medical Outcomes Study Social Support Survey (Sherbourne & Stewart, 1991), the Social Support Questionnaire (Sarason et al., 1983), the Social Support Survey (Richman et al., 1993), and the Interpersonal Support Evaluation List (Cohen et al., 1985).
Both the Interpersonal Support Evaluation List (Cohen et al., 1985) and the Medical Outcomes Study Social Support Survey (Sherbourne & Stewart, 1991) assess the perceived availability of social support resources. The functional components include appraisals, belonging, tangible (e.g., material aid), and self-esteem in the Interpersonal Support Evaluation List (Cohen et al., 1985), and tangible support, affectionate support, positive social interaction, and emotional/informational support in the Medical Outcomes Study Social Support Survey (Sherbourne & Stewart, 1991). Recognizing the varied sources of social support, the Multidimensional Scale of Perceived Social Support (Zimet et al., 1988) assesses the perceptions of social support from family, friends, and significant others. The Social Support Questionnaire (Sarason et al., 1983) quantifies the availability and satisfaction with social support by asking respondents to list the individuals they can rely on and how satisfied they are with the support provided. Conceptualizing social support as a process, the Social Support Survey (Richman et al., 1993) assesses individual satisfaction with the support received, perceived difficulty in obtaining the support, and perceived importance of the support.
While these validated measures have advanced research on social support, it is worth noting that social support can be negative. Well-intentioned social support efforts can be perceived as controlling or directive by the recipient and may create interpersonal conflict and psychological distress (Taylor, 2011). In addition to providing support, the same support network can create strains given that social relationships are often rooted in expectations, obligations, and norms of reciprocity (Sangalang & Gee, 2012). Social support interventions like peer support groups may generate negative interactions if the support provided is perceived as hostile (Hogan et al., 2002). Support seekers may also be declined for support.
Social work-involved populations, in particular, may encounter unsupportive or upsetting responses in the support seeking process (Ingram et al., 1999). Members in marginalized communities are notably vulnerable to being disregarded, rejected, and mistreated when they seek support. Shankar et al. (2013) use the concept of double victimization to describe the experiences of South Asian victims of domestic violence in support seeking. They first experience violence perpetrated against them by their intimate partner and second from Canada's mainstream service providers who fail women by being culturally insensitive. Aujla (2021) used a similar concept of revictimization to indicate secondary victimization experienced by South Asian immigrant women who suffer domestic violence in support seeking. The study describes forms of oppression from professionals, including the lack of professional boundaries, the use of victim-blaming language, and being judgmental. In a systematic review of 21 studies, Waller et al. (2022) examines African American women's support seeking experiences in addressing intimate partner violence. The review reveals women's experiences of being objectified, overlooked, and overtly mistreated in various systems.
Barriers to support seeking derived from negative, insensitive social responses are evident (Aujla, 2021; Ingram et al., 1999; Sangalang & Gee, 2012; Waller et al., 2022). It remains unclear how support seeking itself—even without receiving support at the end—may be associated with individual strengths. Hamby et al. (2020) examined a sample of 440 youths aged 10–21 on their support seeking and received. Through classifying youths into four groups using the dual factors of social support, the study found that youths who actively sought social support reported higher levels of strengths and well-being than youths who did not actively seek support—no matter if they received the support eventually or not. The results suggested that the support seeking process itself can cultivate strengths and benefits in individuals.
Current study
The current study examines how seeking and receiving social support, when differentiated, are associated with individuals’ strengths and well-being. To assess the impact of seeking and receiving social support simultaneously, we used a dual-factor approach to measure social support. Based on their responses to measures of social support seeking and receiving, we classified participants into four groups: Interconnected (high on support seeking and receiving), Tended (high on receiving, low on seeking), Rebuffed (high on seeking, low on receiving), and Isolated (low on seeking and receiving) to determine whether these groups differed on individual strengths and well-being. Informed by the Resilience Portfolio Model (Grych et al., 2015), individual strengths examined in the current study were regulatory strengths (managing emotions and impulses), meaning-making strengths (connecting to something larger than oneself), and interpersonal strengths (healthy relationships across the social ecology). We predicted that the Interconnected group would report higher scores on the measures of strengths and well-being and that the Isolated group would report lower scores. Using the similar dual-factor approach and analytic strategies, our prior study (Hamby et al., 2020) with an adolescent sample found that the Rebuffed group reported higher scores on several indicators of strengths and well-being than the Tended group. However, given that no studies have been conducted with an adult sample, we did not form hypotheses regarding the Rebuffed and Tended groups.
Methods
Participants
Table 1 presents the sample characteristics. The participants were 357 individuals in the Appalachian region of a U.S. southern state. The sample was 65% female and included adults aged 18–76, with a mean age of 37.60 (SD = 15.59). The participants predominantly identified as White or European American (75%), followed by Black or African American (13%), Latino or Hispanic (5%), and other race/ethnicity. Over half of the sample reported residing in a smaller city or town, and over a third of the participants reported living in a small town or rural area. More than two in five participants (42%) indicated a household income of less than $30,000 per year, 24% reported a household income between $30,000 and $50,000, 11% earned between $50,000 and $75,000, and 21% reported a household income of more than $75,000 per year. About one in seven (15%) participants reported ever living with foster parents or being placed with relatives. Close to half of the sample (47%) reported receiving free or reduced lunches at school at some point in their lives. These characteristics suggested adverse childhood experiences for a significant proportion of the sample.
Sample characteristics.
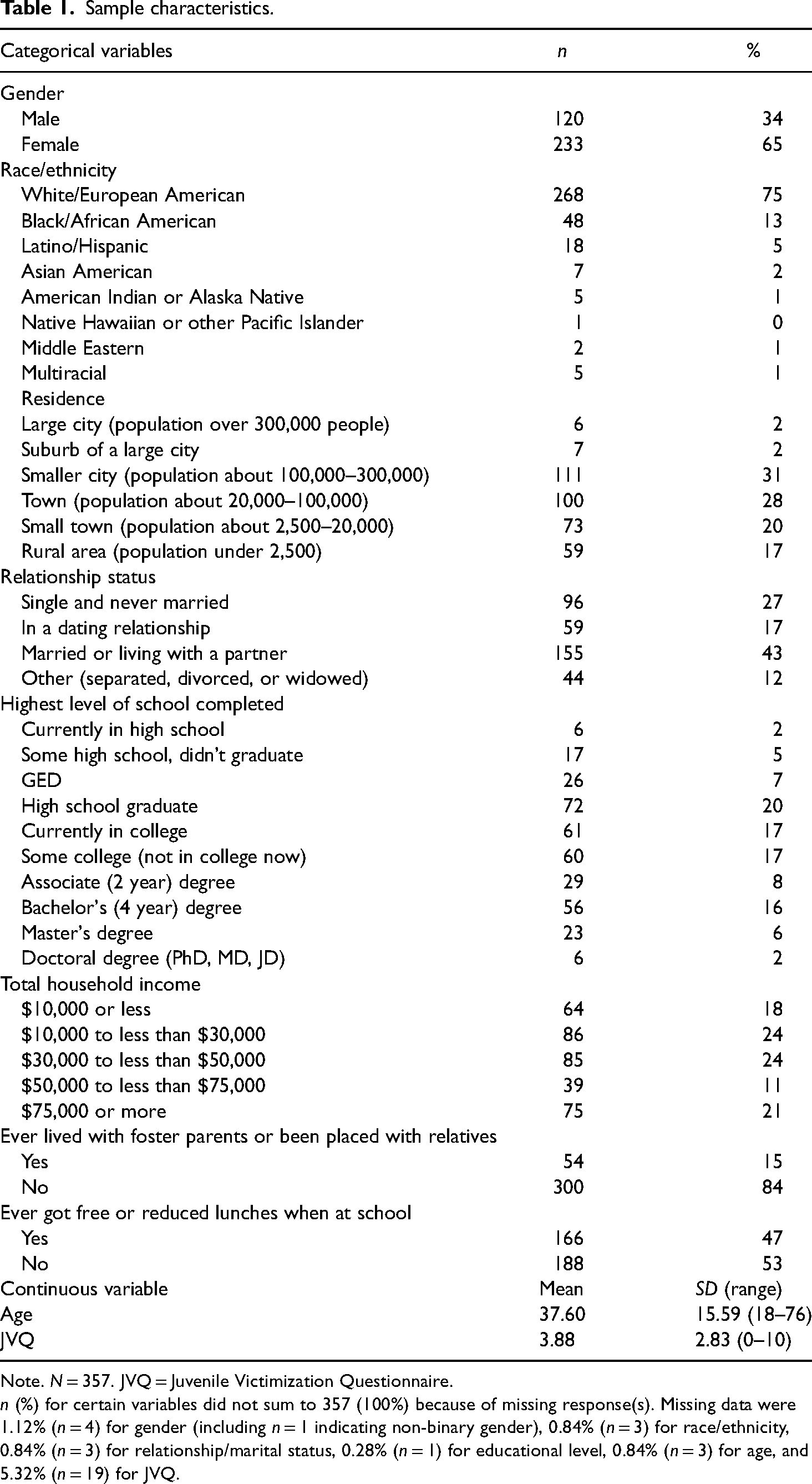
Note. N = 357. JVQ = Juvenile Victimization Questionnaire.
n (%) for certain variables did not sum to 357 (100%) because of missing response(s). Missing data were 1.12% (n = 4) for gender (including n = 1 indicating non-binary gender), 0.84% (n = 3) for race/ethnicity, 0.84% (n = 3) for relationship/marital status, 0.28% (n = 1) for educational level, 0.84% (n = 3) for age, and 5.32% (n = 19) for JVQ.
Procedures
A range of techniques was used to advertise the survey, including local community events and festivals and word-of-mouth recruitment. All surveys were self-administered in 2017 using tablets, and the survey software Snap11 was chosen because it does not require Internet connectivity, as many areas in Appalachia are without reliable cellular and Internet service. An option was given for the participants to have the survey read to them by a research assistant for those with limited reading skills. In addition, the participants were asked at the end of the survey how well they understood the survey questions using a 4-point scale (ranging from “I understood all of the questions in this survey” to “I didn’t understand most of the questions.”). Out of the original sample of 377, no participants requested for having the survey read to them, six participants indicated that they did not understand most of the survey questions and were removed, and 14 more participants were removed due to incomplete surveys, resulting in a final sample of 357. Overall, the completion rate was 96%. Each participant received a $20 Walmart gift card and information regarding local resources. All procedures were conducted per American Psychological Association ethical principles and approved by the institutional review board of the University of South.
Measures
All measures in the current study were developed or adapted from Hamby et al. (2018a) using a three-step approach, beginning by conducting four focus groups with youths and caregivers recruited through local community organizations serving children and families. From focus group responses, an initial survey was drafted, and cognitive interviews were conducted. Based on feedback from the cognitive interviews, a final version of the survey was developed (Hamby et al., 2018b). Given the relatively low educational attainment of the Appalachian region, high priority was given to brevity and to writing all survey items at a fifth-grade reading level. The response categories for measures were on a 4-point Likert-type scale ranging from 1 (“not true about me”) to 4 (“mostly true about me”) unless otherwise indicated. Higher scores represented higher levels of each construct.
Social support
Social support was measured by the 11-item Social Support Scale (Hamby et al., 2018b). We conducted explorative and confirmatory factor analyses to explore the factor structure of the scale. A two-factor structure was determined using the eigenvalue-1 criterion with the principal component analysis with a Varimax rotation (Brown, 2009; Hatcher, 2013). Factor 1 represents Social Support Received (five items, α = 0.87, e.g., “Someone was there for me when I was having a hard time”) and accounts for 46% of the variance. Factor 2 represents Social Support Seeking (six items, α = 0.90, e.g., “Talking it out with someone helps me when I’m upset”) and accounts for 54% of the variance. Both the Support Received items (α = 0.87) and the Support Seeking items (α = 0.90) had satisfying internal consistency reliability. Table 2 presents the results of the confirmatory factor analysis for the two-factor social support measurement model. All estimates were significant at p < .001 and most factor loadings were 0.65 or above, suggesting that they can be considered significant in defining the latent variables (Ford et al., 1986). In the current study, we classified the participants into four groups based on their responses to the measures of social support seeking and receiving: Interconnected, Tended, Rebuffed, and Isolated.
Results of confirmatory factor analysis.

Note. N = 357. CFI = 0.93, TFI = 0.91, RMSEA = 0.11, SRMR = 0.05. SE = standard error.
***p < .001.
Regulatory strengths
Regulatory strengths refer to individuals’ capacity for self-control when encountering adversity and difficulty. We assessed regulatory strengths with four subscales: the Positive Emotion Regulation Scale, the Endurance Scale, the Impulse Control Scale, and the Self-Reliance Scale (Hamby et al., 2018b). The Positive Emotion Regulation Scale assesses individuals’ ability to cheer themselves up in distress (five items, α = 0.83, e.g., “I don’t let small problems ruin my day”). The Psychological Endurance Scale assesses one's ability to persevere despite challenges (six items, α = 0.74, e.g., “I am quick to pick myself back up again when I get “knocked down”). The Impulse Control Scale assesses behavioral self-regulation (five items, α = 0.77, e.g., “I stop to think before I act”). The Self-Reliance Scale assesses one's preference to cope on their own (five items, α = 0.78, e.g., “I like to solve problems on my own”).
Meaning-making strengths
Meaning-making strengths refer to the extent to which individuals perceive their connections to something beyond the self. We assessed meaning-making strengths using the Mattering Scale, the Purpose Scale, the Religious Meaning-Making Scale, and the Future Orientation Scale (Hamby et al., 2018b). The Mattering Scale measures the extent to which the participants felt appreciated and valued by others (five items, α = 0.88, e.g., “I feel appreciated by my family and friends”). The Purpose Scale measures individuals’ feelings of having a sense of meaning in life (five items, α = 0.89, e.g., “My life has a clear sense of purpose”). The Religious Meaning-Making Scale measures individuals’ engagement in faith and religious/spiritual practices (five items, α = 0.93, e.g., “I often think about my faith or spiritual beliefs”). The Future Orientation Scale measures the desire for self-fulfillment (five items, α = 0.76, e.g., “I try to live up to my potential”).
Interpersonal strengths
Interpersonal strengths involve participants’ relational skills and perceptions of their social environment. We assessed interpersonal strengths using the Compassion Scale (Hamby et al., 2018b), the Community Support Scale (Roberts et al., 2015), the Group Connectedness Scale (Hamby et al., 2018b), and the Relational Motivation Scale (Hamby et al., 2018b). The Compassion Scale measures the extent to which participants engage with others in a caring and helpful way (five items, α = 0.76, e.g., “If I know someone is upset, I check up on them”). The Community Support Scale assesses the degree to which one's neighbors get along and help one another (five items, α = 0.76, e.g., “People in my neighborhood talk to each other”). The Group Connectedness Scale assesses the feelings of closeness and support from peer groups (five items, α = 0.94, e.g., “I have belonged to a group or team with people who stand up for me”). The Relational Motivation Scale assesses participants’ efforts in fulfilling important others’ expectations (five items, α = 0.78, e.g., “I try to live up to my family's hopes for me”).
Well-being indicators
Measures were adopted to assess psychological, physical, and spiritual well-being and functioning (Hamby et al., 2018b). The Subjective Well-being Scale measures general life satisfaction (five items, α = 0.93, e.g., “I feel really good about my life”). The Family Well-being Scale assesses the subjective well-being of one's immediate family and other relatives who live with the child (seven items, α = .91, e.g., “My family is happy”). The Spiritual Well-being Scale includes both a Theistic subscale (five items, α = 0.96) and a Non-theistic subscale (five items, α = 0.84). The Theistic subscale assesses well-being from a sense of god or similar higher power (e.g., “I feel better when I talk to god or a higher power”). The Non-theistic subscale captures a similar sense of awe or well-being from less religious sources, such as connectedness to nature (e.g., “I feel all living things are connected”). The Physical Well-being Scale (Banyard et al., 2017) assesses participants’ perceptions of their own physical health (five items, α = 0.78, e.g., “During the last month, for about how many days did your health stop you from doing your usual activities, like going to school or spending time with friends”) with a response option ranging from “0 days” to “every day or almost every day.” The Trauma Symptoms Scale (eight items, α = 0.93, e.g., “Feeling worried or anxious in the last month”) assesses a range of feelings of dysphoria, anxiety, or guilt.
Poly-victimization
Poly-victimization was assessed with the Juvenile Victimization Questionnaire (JVQ)—Key Domains Short Form (Hamby et al., 2004). The JVQ includes 10 questions asking the participants the lifetime history of a range of interpersonal victimizations. A sample item is “During your childhood, did one of your parents threaten to hurt another parent and it seemed they might really get hurt?” Dichotomous items (“yes” or “no”) were summed to create a total poly-victimization score (α = 0.81). The median number of victimizations reported by youth was 4, with a mean of 3.88 (SD = 2.83).
Data analysis
To understand the participant differences in their reports of strengths and well-being, we classified the participants into four groups: Interconnected, Tended, Rebuffed, and Isolated based on their responses to the measures of social support seeking and receiving. Median splits (up to and including 50th percentile = 0, over 50th percentile = 1) for the Social Support Received score and Social Support Seeking score were used to create the social support groups. The social support group membership thus incorporates individuals’ help-seeking skills and attitudes as well as the outside support and resources offered to those individuals.
Analyses of covariance (ANCOVAs) were conducted to examine differences in the psychosocial strengths and well-being indicators among the four social support groups, controlling for age, gender, and poly-victimization. Age, gender, and poly-victimization were conceptualized as covariates given their potential impact on receiving and seeking social support. Eta-squared,
Results
As presented in Table 3, the most and least endorsed Social Support Received items were, respectively, “Someone was there for me when I was having a hard time” (M = 3.37, SD = 0.89) and “Someone went with me to get some help” (M = 2.60, SD = 1.26). For Social Support Seeking, the most and least endorsed items were “It helps me to discuss ideas with someone when I have a problem” (M = 3.42, SD = 0.83) and “I ask people to help me make tough decisions” (M = 3.09, SD = 1.00), respectively. The Interconnected group (n = 127, 35%) scored high on both seeking and receiving social support. The Isolated group (n = 132, 37%) had low scores on both support seeking and receiving. Both the Tended group (n = 49, 14%) and Rebuffed group (n = 49, 14%) had a mixed profile with the Tended scoring high on social support receiving and low on social support seeking, and the Rebuffed scoring low on social support receiving and high on social support seeking.
Means and standard deviations of social support items.

Note. N = 357. All items ranged from 1 (“not true about me”) to 4 (“mostly true about me”).
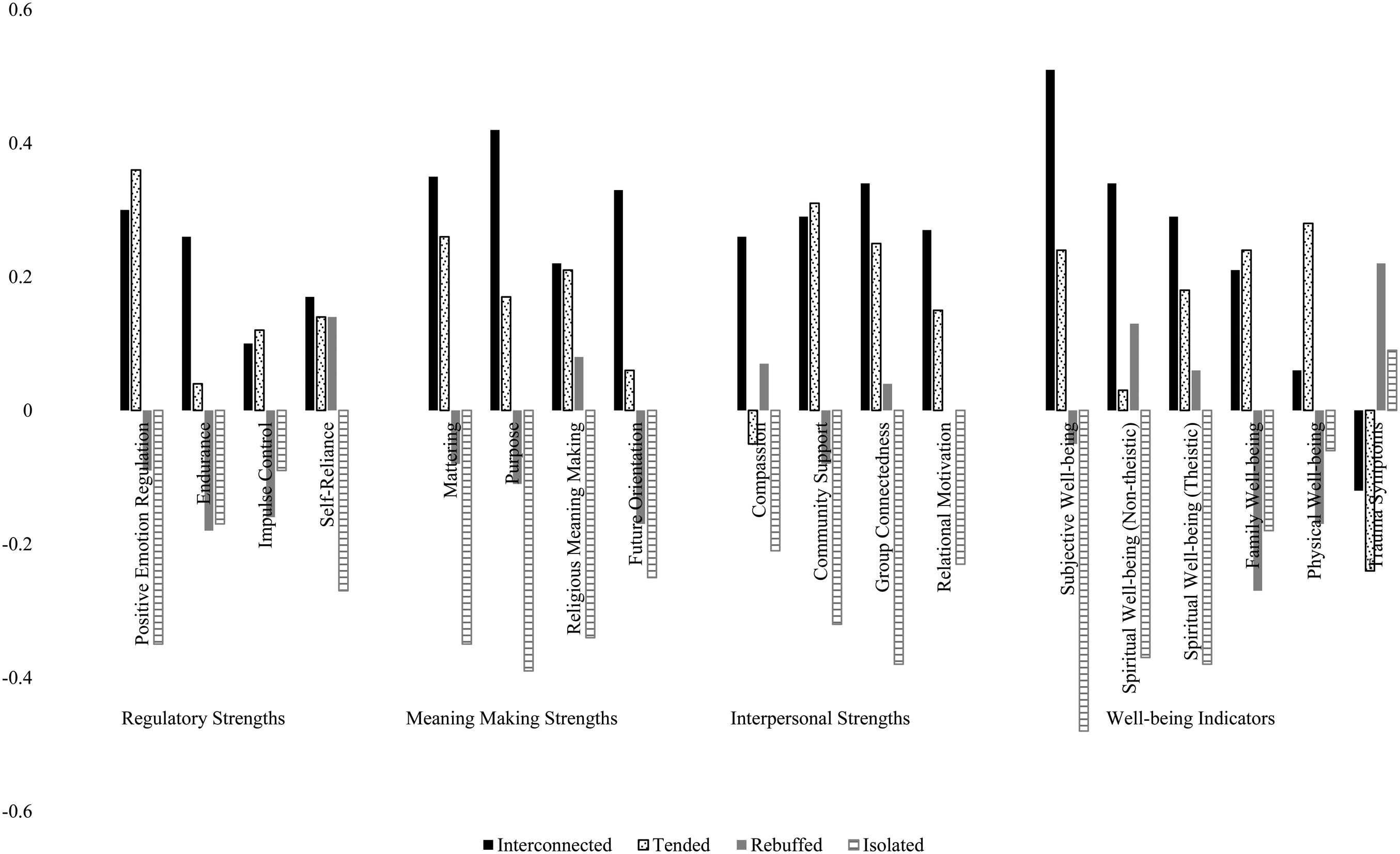
Table 4 presents the results of ANCOVAs. The results suggest significant differences in psychosocial strengths among the four social support groups, after controlling for age, gender, and poly-victimization. To facilitate interpretation regarding the differences among the four social groups, we created Figure 1 using the findings presented in Table 4.
Comparison among social support groups in strengths.
Comparison among social support groups.
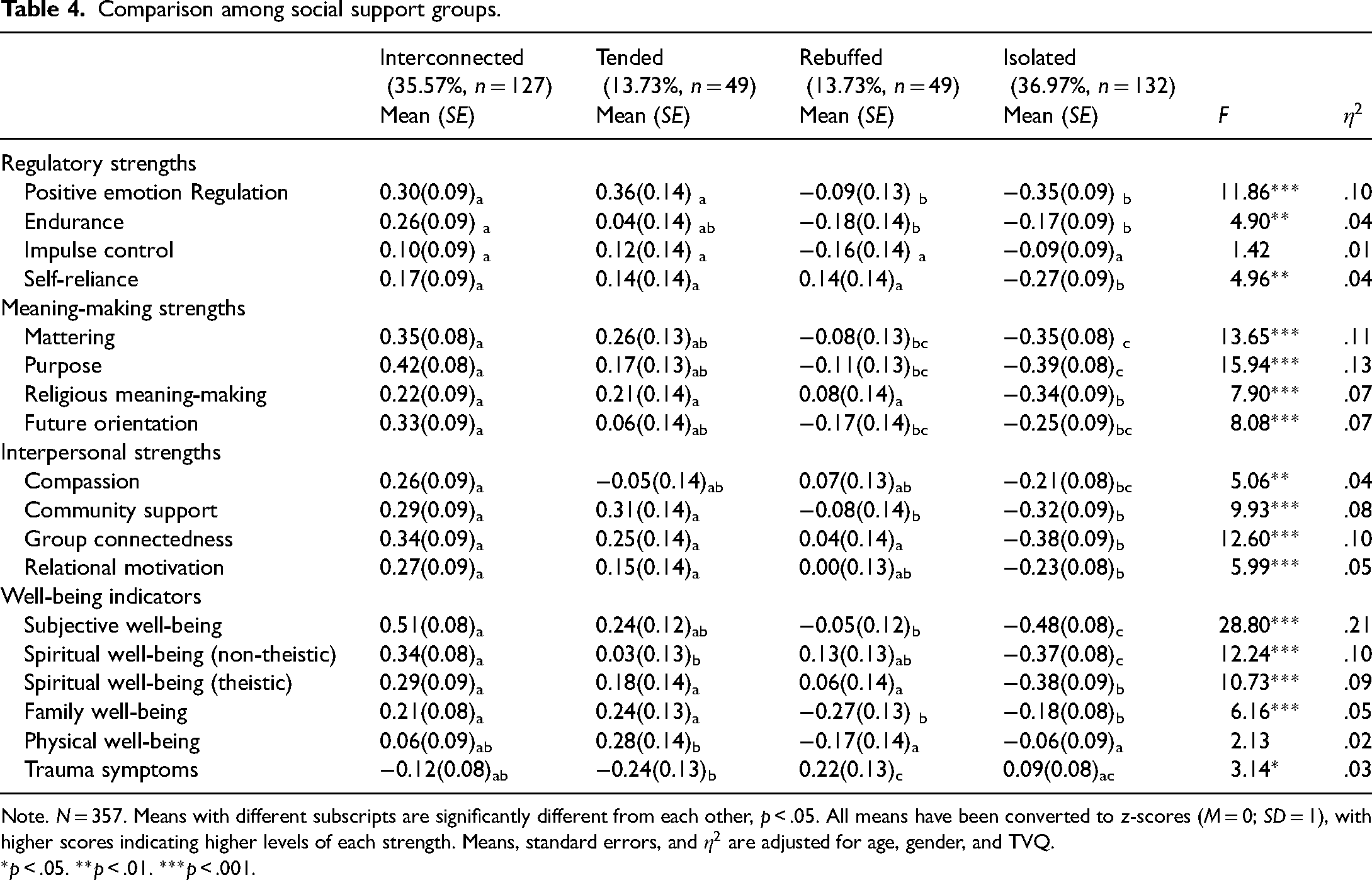
Note. N = 357. Means with different subscripts are significantly different from each other, p < .05. All means have been converted to z-scores (M = 0; SD = 1), with higher scores indicating higher levels of each strength. Means, standard errors, and
*p < .05. **p < .01. ***p < .001.
Regulatory strengths
We found significant differences among the four social support groups in Positive Emotion Regulation (
Meaning-making strengths
The results showed significant differences between groups in all the meaning-making strengths measures: Mattering (
Interpersonal strengths
The social support groups scored significantly differently in all four measures of Interpersonal strengths: Compassion (
Well-being indicators
The social support groups scored significantly differently for Subjective Well-being (
Discussion
Using a dual-factor approach that created four groups that varied in reports of social support seeking and receiving, this study found significant differences among the four groups in almost all measures, with the Interconnected group (high on social support seeking and receiving) scoring significantly higher than the Isolated group (low on seeking and receiving) on most measures, largely in line with predictions. The findings are consistent with prior literature underscoring the importance of social support in sustaining individual well-being and other outcomes (Cook-Craig & Koehly, 2011; Lee & Hwang, 2014; Schwartz & Frohner, 2005; Shen et al., 2004).
The findings around the Tended and the Rebuffed groups are intriguing. The current study found that the Tended group (high on receiving, low on seeking) scored significantly higher than the Rebuffed group (high on seeking, low on receiving) on several measures of strengths and well-being (Positive Emotion Regulation, Community Support, Family Well-being, and Physical Well-being) and reported fewer Trauma Symptoms. These findings are contradictory to our prior study that examined social support with a sample of 440 youths aged 10–21. Using the same Social Support Scale with a dual-factor approach, Hamby et al. (2020) found that the youth in the Tended group scored significantly lower than the Rebuffed group on multiple measures of strengths and well-being. The Rebuffed group may benefit from the process of toughening themselves up for difficult challenges, which may be particularly important for teens and young adults as they are at the stage of seeking independence (Nadeem & Romo, 2008; Schrag & Schmidt-Tieszen, 2014). For instance, through interviewing young, unmarried mothers with a mean age of 20 years in a homeless shelter, Schrag and Schmidt-Tieszen (2014) identified the tension between wanting to be supported by family or friends and the desire for independence. It is possible that receiving support when not asking for support signals dependence to teens and thus led to lower levels of well-being and strengths for the Tended group than the Rebuffed group with an adolescent sample (Hamby et al., 2020).
In contrast, the current study, conducted with an adult sample, found that the Tended group scored significantly higher on some measures of strengths and well-being than the Rebuffed group (and the reverse never occurred). It is possible that for this sample of adults, receiving social support and messages of interdependence may weigh more than the desire to seek independence. The care-getting model at different stages of the life course sheds a light on this finding (Kahana et al., 2009). Kahana et al. (2009) proposed a conceptual framework to understand the proactive options for care-getting for patients living with a chronic or life-threatening illness. They illustrated that the barriers and facilitators to care-getting vary across the stages of one's life course. For adolescents, fears of stigma from peers and the feeling of being embarrassed were identified as challenges to care-getting. For young adults, challenges were job and family responsibilities, being fearful of appearing weak and needy, and fears that help-seeking would threaten independence. For midlife adults, the challenges included job and family responsibilities and worries about the loss of self-esteem. The various barriers identified echo the differences in findings around the Tended and Rebuffed group in Hamby et al. (2020) and the current study. While the fear of losing independence is perceived as a barrier to support seeking for adolescents, the barriers to support seeking for adults are more likely to be practical, logistic challenges.
An important finding of the current study is that the Rebuffed group did not score significantly lower than the Isolated group on any variable and reported significantly higher levels than the Isolated group on Self-Reliance (regulatory strength), Religious Meaning-Making (meaning-making strength), Group Connectedness (interpersonal strength), Subjective Well-being (well-being indicator), Non-Theistic Spiritual Well-being (well-being indicator), and Theistic Well-being (well-being indicator) (see Figure 1). The Rebuffed group did report lower levels than the Isolated group on a few measures, including Endurance (regulatory strength), Impulse Control (regulatory strength), Family Well-being (well-being indicator), Physical Well-being (well-being indicator), and higher levels of Trauma Symptoms (well-being indicator), but the differences were never significant in pair comparison.
It is possible that negative interactions in the support seeking process could be buffered and that the support seeking process itself may cultivate strengths and benefits in individuals—no matter if they received the support eventually or not (Hamby et al., 2020).It is consistent with the resilience portfolio model that it is preferable to have a strength in one's portfolio than not have it, even in an adverse environment (Hamby et al., 2018a). Another possible explanation is that support seeking individuals were more resilient in the first place. Future research should consider using qualitative interviews to offer more in-depth insights into support seeking experiences. It is important to note that this finding does not discredit or contradict the literature discussing the negative aspects of social support (e.g., Aujla, 2021; Ingram et al., 1999; Sangalang & Gee, 2012; Taylor, 2011; Waller et al., 2022). The relatively lower levels of strengths and well-being found in the Rebuffed group than in the Interconnected and Tended group serve as a piece of evidence that being rejected from one's support network can be harmful to individuals. These findings should not be used to justify unprofessional, insensitive responses from service organizations that induce double victimization or revictimization to support seekers (Aujla, 2021; Shankar et al., 2013). The finding, instead, highlights the resilient nature of individuals in the support seeking process and underscores the importance of support seeking. Individuals grow when they overcome their fears, take the risk of being vulnerable, and seek support from others. Individuals who step out and seek support can gain strengths in this process despite whether they may or may not obtain the support at the end.
Limitations of the study
The study findings should be interpreted with caution in light of its limitations. First, data were collected via self-report surveys and could be influenced by certain sources of measurement errors, such as social desirability. Second, the dual-factor Social Support Scale was developed to assess social support received and social support seeking in the general sense without differentiating formal and informal support. Individuals may have different perceptions and behaviors when facing various life challenges. For instance, individuals may be willing to seek help and support from their social networks when encountering general relationship challenges while not willing to do so if the relationship problems involve abuse and violence. As the current data allowed us to differentiate support seeking and support received, we were not able to further contextualize the findings by connecting the life challenges that triggered support seeking or analyzing the types of support being sought and provided. Third, the data were collected with a sample in the Appalachian region of a southern state with a disproportionately higher percentage of White women participants. The findings from the current study may not generalize to other settings.
Implications for social work research and practice
The results suggest that social work interventions should go beyond assessing service recipients’ social support networks or providing social support group interventions that assume service recipients would automatically benefit from these contacts (Lanctôt, 2020). Members in marginalized communities are more likely to experience unsupportive responses or rejection. The current study found that the Rebuffed group scored lower in strengths and well-being indicators when compared to the Interconnected group and the Tended group. This finding indicates the need to further work with individuals who seek help but do not receive the support they need. These negative experiences may, in turn, shape individuals’ future support seeking (Waller et al., 2022). Social work practitioners should assess their client's experiences with support seeking and address negative experiences to facilitate individual strengths and positive social support experiences. As social support interventions are commonly used in practice, practitioners should recognize that such interventions may generate negative interactions if the support provided is perceived as hostile (Hogan et al., 2002). Ongoing assessment of the social support process is needed when performing social support interventions.
The finding that the Rebuffed group did not score significantly lower than the Isolated group in general and scored significantly higher on some measures for regulatory strengths, meaning-making strengths, interpersonal strengths, and well-being highlights the importance of support seeking. This finding suggests that the support seeking process itself can cultivate strengths and benefits in individuals even though they may not receive support eventually (Hamby et al., 2020). Practitioners should facilitate and optimize their clients’ support seeking skills and address related barriers. For instance, research has indicated that adults with adverse childhood experiences may use disconnection and rejection schemas as a protective mechanism to help themselves cope with difficult experiences such as child maltreatment (Lanctôt, 2020). These mechanisms, usually involving distancing and disconnection in interpersonal relationships, likely lead to compromising their ability to seek social support. Social work practitioners should assess clients’ relationship patterns and cognitive schemas that contribute to disconnection, mistrust, and reluctance toward support seeking.
Accumulating evidence has indicated the multifaceted nature of social support. While support seekers may receive help, they may encounter unsupportive or upsetting responses (Ingram et al., 1999; Sangalang & Gee, 2012). The current study found significant differences in measures of strengths and well-being among the four social support groups. Future social work research should take efforts to measure multiple aspects of social support. In addition to assessing social support perceived and received by individuals, it is equally important to assess their perceptions and behaviors related to support seeking. Being supported to seek help can play a critical role in one's support seeking process. Future research should consider the influence of perceptions of support seeking in support seekers’ families and communities.
Lastly, research indicates that there are numerous reasons why someone may not seek social support, many of which were exacerbated during the COVID-19 pandemic (Yonemoto & Kawashima, 2022). For instance, a 2020 population-based survey in the U.K. found that many individuals who experienced a potential cancer symptom during the pandemic decided not to contact their healthcare provider because of various reasons, including being worried about wasting the doctor's time, not wanting to put a strain on healthcare services on top of the pandemic, or not wanting to make a fuss (Quinn-Scoggins et al., 2021). A similar pattern was also observed in individuals experiencing mental health symptoms and intimate partner violence (Ruiz et al., 2022; Yonemoto & Kawashima, 2022). Future social work research should take into account the impact of the COVID-19 pandemic on individual support seeking.
Conclusions
The current study investigates how seeking and receiving social support are associated with individuals’ strengths and well-being using a dual-factor approach. The study found that overall, the Interconnected group scored highest in regulatory strengths, meaning-making strengths, interpersonal strengths, and well-being indicators, followed by the Tended group, the Rebuffed group, and lastly, the Isolated group. The finding that the Rebuffed group did not score significantly lower than the Isolated group suggests that individuals can gain strengths in support seeking even though they may not always obtain support. Individuals grow when they overcome their fears, take the risk of being vulnerable, and seek support from others. Social work practitioners should facilitate and optimize their clients’ support seeking, including addressing their clients’ negative experiences in the support seeking process and removing clients’ barriers to support seeking.
Footnotes
Ethical Approval
All procedures were conducted per American Psychological Association ethical principles and approved by the institutional review board of the University of the South.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declarations of conflict of interests
The authors confirm that they have no conflict of interest in respect of the material submitted in this article.
Acknowledgement
This project was made possible through the support of the Appalachian Center for Resilience Research.