
Abstract
The estimated glomerular filtration rate (eGFR) quantifies kidney graft function and is measured repeatedly after transplantation. Kidney graft rejection is diagnosed by performing biopsies on a regular basis (protocol biopsies at time of stable eGFR) or by performing biopsies due to clinical cause (indication biopsies at time of declining eGFR). The diagnostic value of the eGFR evolution as biomarker for rejection is not well established. To this end, we built a joint model which combines characteristics of transition models and shared parameter models to carry over information from one biopsy to the next, taking into account the longitudinal information of eGFR collected in between. From our model, applied to data of University Hospitals Leuven (870 transplantations, 2 635 biopsies), we conclude that a negative deviation from the mean eGFR slope increases the probability of rejection in indication biopsies, but that, on top of the biopsy history, there is little benefit in using the eGFR profile for diagnosing rejection. Methodologically, our model fills a gap in the biomarker literature by relating a frequently (repeatedly) measured continuous outcome with a less frequently (repeatedly) measured binary indicator. The developed joint transition model is flexible and applicable to multiple other research settings.
Introduction
Observational data, usually comprising of the longitudinal follow-up of a cohort, is one of the main data sources in kidney transplantation research. Apart from baseline information at the day of transplantation, parameters on renal function, like estimated glomerular filtration rate (eGFR) and proteinuria, are collected repeatedly at the occasion of clinical visits in order to detect and treat allograft injury. Via biopsies, performed in case of a clinical indication of renal graft injury (declining eGFR or increasing proteinuria), the so-called indication biopsies, data on kidney histology and rejection phenotypes are obtained as well. Next to indication biopsies, many centres also collect biopsies per protocol, leading to a less selected view on the progression of kidney histology post transplantation (Racusen, 2006; Wilkinson, 2006). Due to the invasiveness of biopsies, histological data are more scarce than data on renal functioning.
In recent years, there is an increased interest in the discovery of non-invasive biomarkers for acute and chronic rejection and chronic allograft injury after kidney transplantation (Salvadori and Tsalouchos, 2017; Van Loon et al., 2019). Advances in ‘omics’ research, for example, led to robust, predictive and useful biomarkers at the molecular level (Salvadori and Tsalouchos, 2017). A clinically useful non-invasive biomarker should allow for the early discovery of future kidney damage/failure and should be sufficiently sensitive. A well-performing biomarker for kidney histology could eliminate the need for conducting invasive biopsies (Lo et al., 2014; Peters et al., 2014; Lopez-Giacoman and Madero, 2015).
When conceiving renal functional parameters as a continuous biomarker for the presence or absence of kidney rejection at the time of biopsy, these data can be viewed as recurrent longitudinal sequences of marker measurements with binary indicators (rejection or not) in between. After all, rejection is not a final end-point. Jointly analyzing these outcomes requires the specification of their multivariate distribution. However, this specification is hampered because both responses are irregularly measured variables of a different type (continuous and binary). A popular approach for jointly modelling two longitudinal processes of a different type, and widely applied in biomarker discovery (Li et al., 2017), is the shared parameter model, which assumes conditional independence given a common set of random effects. These models are advantageous in the sense that the parameter estimates of the separate models can be interpreted as if they were modelled separately. A typical example is the joint longitudinal survival model, where a longitudinal continuous marker is correlated with a time-to-event outcome (Rizopoulos, 2011, 2012; Li et al., 2017). Extensions of the joint longitudinal survival model were made to include recurrent events (Liu and Huang, 2009; Kim et al., 2012), competing risks (Elasho et al., 2008; Rizopoulos, 2012) and multi-state models (Ferrer et al., 2016). In some cases, this time-to-event outcome can even be downgraded to a binary outcome. Examples can be found in Horrocks and van Den Heuvel, 2009 where a successful pregnancy was predicted from the adhesiveness of certain blood lymphocytes, or in Chen et al., 2015 where the development of self-esteem was related to anxiety disorder at a certain age. Yet, when the binary outcome is also measured longitudinally, a random-effects approach (Verbeke et al., 2014) is often preferred. By including separate, but correlated random effects, these models allow for more flexibility in the correlation structure between both longitudinal processes. An example can be found in Gueorguieva, 2001 where malformation (binary) and birth weight (continuous) of mice foetuses were associated with a certain toxic dose.
Instead of using a mixed model for the binary outcome, as in the random-effects approach, another valuable model for occasionally measured, longitudinal outcomes, is the transition model (Verbeke et al., 2014). Univariate transition models factorize the joint distribution of a longitudinal outcome into the marginal distribution for the first response and a set of conditional distributions for the later responses given the earlier ones (Diggle et al., 2002; Molenberghs and Verbeke, 2006; de Rooij, 2018). In case of categorical outcomes, transition models consider the data as a sequence of states (Liang and Zeger, 1989), which exactly corresponds to the research setting of recurrent biopsy data. In joint modelling, the use of transition models instead of mixed models is advantageous especially during the fitting process. Random-effects models require the specification of multiple, often complex, random effects structures, leading to intractable integrals in the likelihood. Transition models on the contrary allow for dependence in a sequence of states via a fixed parameter structure. In addition, transition models allow for a predictive interpretation, that is, using past measurements to determine future events, a property which is much more difficult to attain in a random-effects approach.
Combining characteristics of the transition model with these of the shared parameter model for evaluating a potential biomarker for a histological outcome is, to the best of our knowledge, never implemented before and will be addressed in this article. By doing so, we provide a new methodological framework for modelling the multivariate distribution of a frequently (repeatedly) measured continuous response and a less frequently (repeatedly) measured binary response, applied to a use case in kidney transplantation.
Motivating case study
At the University Hospitals Leuven, for kidney transplant recipients, an intensive protocol biopsy program has been established since 2004. On top of indication biopsies, performed in case of clinical suspicion, the staff decided on pre-planned biopsies at day 0, 3 months, 1 year and then every year up to 5 years post transplantation. By doing so, a full longitudinal picture of a patient's kidney histology is obtained, which is then used to diagnose transplant rejection. For this study, all single kidney transplantations performed between March 2004 and February 2013 were eligible. Recipients were included if they had at least two performed biopsies after baseline, at least one kidney function measurement in between every biopsy and complete data on the status of pre-transplant donor-specific antibodies (DSA). For each included biopsy, full data on the rejection type was required. In total, we disposed of 2 635 biopsies, 463 of which were indication biopsies, in 870 patients, and of 40.649 eGFR measurements. The inclusion flow chart is displayed in Figure 1.
Inclusion flow chart. Indication biopsies were performed in case of clinical suspicion while protocol biopsies were pre-planned
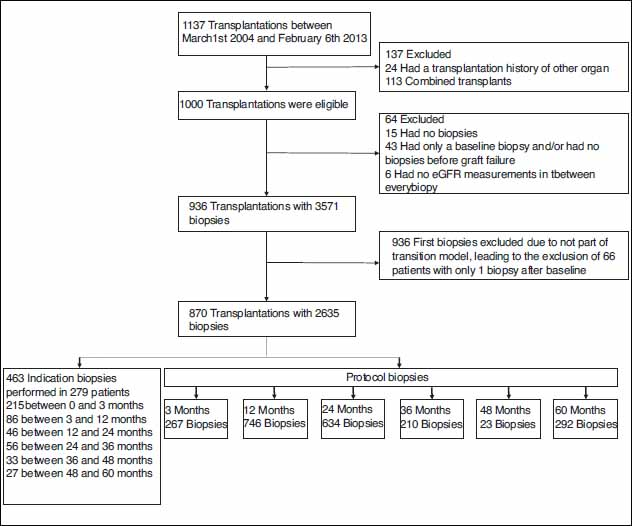
Inclusion flow chart. Indication biopsies were performed in case of clinical suspicion while protocol biopsies were pre-planned
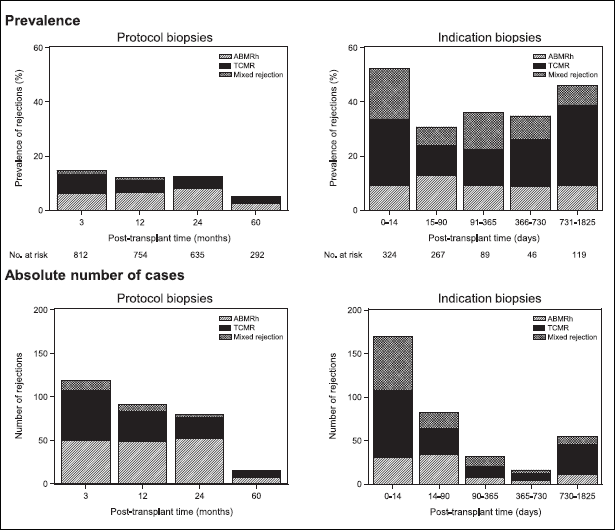
In renal transplantation, two main types of rejection are distinguished: antibody-mediated rejection (ABMR) and T-cell mediated rejection (TCMR) (Loupy et al., 2020). For the latter, effective treatment is available, while the first lacks efficacious therapy (Djamali et al., 2014; Van Loon et al., 2020). Both types of rejection can occur at any time after transplantation. Figure 2 shows the prevalence of ABMRh (=histological picture of ABMR as defined by the Banff 2019 classification without considering the DSA status), TCMR and mixed rejection in the Leuven cohort, indicating that any type of rejection occurs more frequently in indication than in protocol biopsies. In addition, it is clear that in the unselected (protocol) cohort the prevalence of rejection decreases by time. In indication biopsies, there is no time trend in the prevalence, showing their informative measurement. It has been shown that previous episodes of acute rejection are a risk factor for rejections in the future (Joosten et al., 2005).
Prevalence of rejection in protocol and indication biopsies in the Leuven cohort (3 571 biopsies in 936 patients). Indication biopsies were performed in case of clinical suspicion while protocol biopsies were pre-planned. ABMRh = Histological picture of ABMR as defined by the Banff 2019 criteria, TCMR = T-cell mediated rejection, Mixed rejection = ABMRh and TCMR
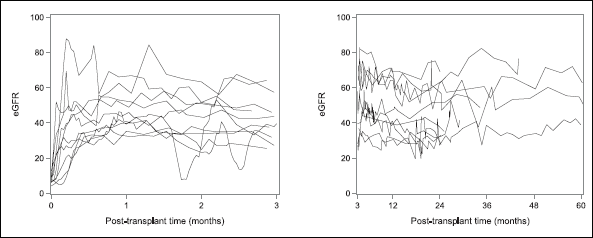
The clinical decision for proceeding to an indication biopsy is mostly based on poor or worsening kidney function, measured by eGFR. Figure 3 shows 10 randomly sampled eGFR profiles from the Leuven cohort, separately for the first three months after transplantation, and afterwards. There is an upward trend of kidney function shortly after transplantation, followed by a stabilizing period. After three months, eGFR exerts little variation in time. By definition, protocol biopsies are performed in patients with stable eGFR. As rejection occurs more often in indication biopsies than in protocol biopsies (Halloran et al., 2019), eGFR is expected to have at least some predictive value for the diagnosis of rejection, although eGFR was shown to be a rather insensitive biomarker of renal injury (Fassett et al., 2011; Loupy et al., 2015; Hollis et al., 2017). The lack of sensitivity of eGFR for kidney injury and rejection could be related to the fact that most studies in transplantation relate eGFR only at one fixed point in time to graft failure or histological outcomes (Viglietti et al., 2018; Loupy et al., 2019; Einecke et al., 2020), hence not considering its longitudinal profile. Other studies correlate renal function at 1-year post transplantation with late graft failure (Hariharan et al., 2002; Kasiske et al., 2002; Loupy et al., 2015). Even more, we found no statistical models that relate a longitudinal biomarker with a recurrent biopsy outcome.
10 randomly sampled recipients’ eGFR profiles from the Leuven cohort (n=936). eGFR, as a measure for renal function, is measured in ml/min/1.73mÃÂ2 according to the MDRD formula. The left panel shows the eGFR evolution in the first three months after transplantation. The right panel shows the eGFR evolution afterwards
The fact that no statistical algorithms for kidney allograft rejection were developed or implemented in clinical practice reflects the difficulty of its early diagnosis. The discovery of baseline risk factors, like the presence of DSA or the number of HLA mismatches, has not led to a sufficiently sensitive/specific marker for acute or chronic rejection. The inclusion of time-dependent information is therefore an essential next step. On top of the (time-dependent) biopsy history, longitudinal biomarkers have the potential of increasing the predictive power of a model by including information that is not always obvious during visual inspection. The increase or decrease of a longitudinal profile may be alarming for one person, but not necessarily for another. Hence, there is a need for a model that objectifies the risk estimate of rejection, based on longitudinal information contained in a potential biomarker, on top of the biopsy history. Once established, the model should be able to detect important biomarkers and should be extendable to multiple biomarkers. In our case, we aim at predicting kidney transplant rejection (ABMRh and/or TCMR) based on the prior rejection history and on the eGFR evolution. The rejection history is a well-known, time-dependent risk factor, while eGFR is a potential longitudinal biomarker. Statistically, the challenge comprises of combining the two longitudinal processes in one model, while adhering to a causal framework that only conditions on the past.
In the following sections, we present a modelling framework that combines transitional components with shared parameters in order to flexibly model the information carried from one biopsy to the next, taking into account the longitudinal information about renal functioning, collected in between the biopsies. Concerning inference, we expect our model to evaluate the importance of (longitudinal) eGFR in determining allograft rejection in a subsequent biopsy. Regarding prediction, we expect our proposed model to outperform a model in which the longitudinal information of eGFR is not included.
Likelihood factorization and random effects
We propose the use of a joint model in which we combine characteristics of transition models, together with characteristics of shared parameter models in order to specify the multivariate distribution of the rejection outcomes and eGFR profiles. First, we define the likelihood function, in which we incorporate all available information. We denote the vector of eGFR measurements in period

which can easily be factorized as
This type of factorization avoids the need for the direct specification of the joint likelihood (Diggle et al., 2002; Serroyen et al., 2009; Verbeke et al., 2014) by conditioning the outcome on other outcomes or on a subset of these (Fitzmaurice and Molenberghs, 2009). In case of longitudinal data, the factorization leads to the so-called transition model in which the current outcome is conditioned on the past responses. Indeed, rejection and the eGFR values in period j depend on the previous biopsies and eGFR measurements. This approach is natural to our research question in which we want to use historic information in order to predict future rejection. A common assumption in the transition model is the first-order autoregressive structure, AR(1), which indicates that the distribution of the measurements in period j only depends on the measurements taken in the preceding period and not on those taken in earlier periods. Clinically, this assumption is plausible since therapeutic decisions are usually made on the last biopsy outcome and the recent foregoing eGFR trajectory. Nevertheless, because the eGFR profile and biopsy outcome of period j-1 depend on the outcomes of period j-2, implicitly non-neighbouring periods are still associated. More specifically, we assume that

In addition to the previously proposed transition structure, we assume that the association between the longitudinal eGFR process (

Finalizing the likelihood expression in (3.4) requires the explicit modelling of every factor in the equation. The last factor pertains to the random effects resulting from a mixed model for eGFR, which are assumed not to be affected by the eGFR measurements or biopsy outcome in the previous period, that is,

where
When the decision for a biopsy is based on an eGFR deviation (indication biopsy), it is plausible to assume that only the measurements of the current period are predictive for rejection. Likewise, in case of a protocol biopsy with stable eGFR, also the current measurements will suffice for predicting the biopsy outcome. Hence, in modelling terms, we assume the rejection status in period j to depend on the previous biopsy and on the random effects of that same period:

Finally, we assume that a summary

Combining expressions (3.3) to (3.7) and substituting these in (3.2) results in a likelihood contribution of each individual patient of:


eGFR modelling choices
As eGFR is a continuous measure and rejection is binary (present/absent), we propose to jointly model a Gaussian linear mixed model with a logistic regression (transition) model. In the linear mixed model we include two time effects (in years): one models the timing of the biopsy at the end of the period under consideration and one models the timing of the eGFR measurement since the previous biopsy. Since the eGFR trajectory first increases in the initial post-transplant phase, and consequently decreases slowly, both ‘Time of biopsy’ and ‘Time since biopsy’ were log-transformed. In order to achieve extra flexibility in the time trend we also included the quadratic form of ‘ln(Time of biopsy+1)’ and the interaction with ‘ln(Time since biopsy+1)’. The vector
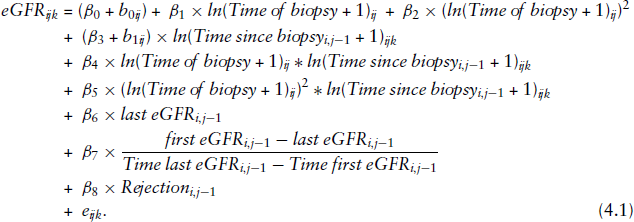
We further assume that the vector (
For rejection, a logistic regression model is used. As the prevalence of rejection is decreasing by time after transplantation, we assume a linear effect of the timing of biopsy on the logit for rejection. Also, the previous biopsy outcome and the presence of pre-transplant DSA are included in the model. The random intercepts (
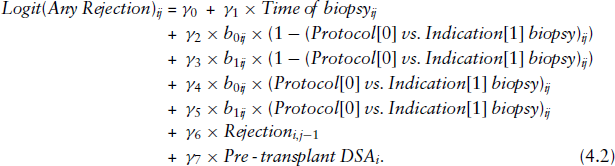
The procedure NLMIXED in SAS (v9.4; SAS Institute) is used to perform the analyses. In Supplemental Material (
Modelled (joint transition model) and observed eGFR profiles of three randomly selected recipients. eGFR, as a measure for renal function, is measured in ml/min/1.73mÃÂ2 according to the MDRD formula
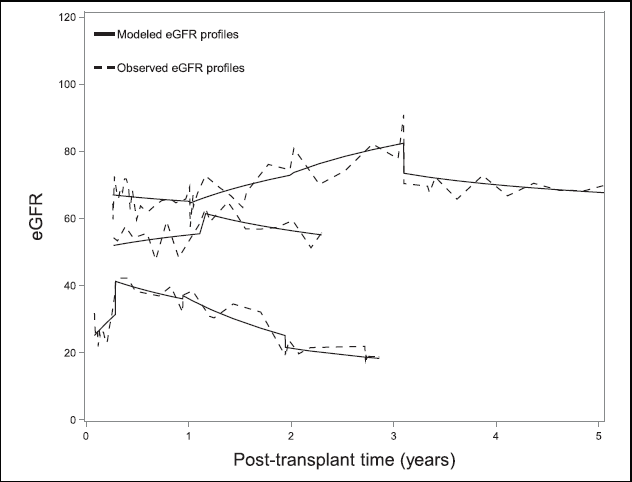
Modelled (joint transition model) and observed eGFR profiles of three randomly selected recipients. eGFR, as a measure for renal function, is measured in ml/min/1.73mÃÂ2 according to the MDRD formula
In the sub-model for rejection (the
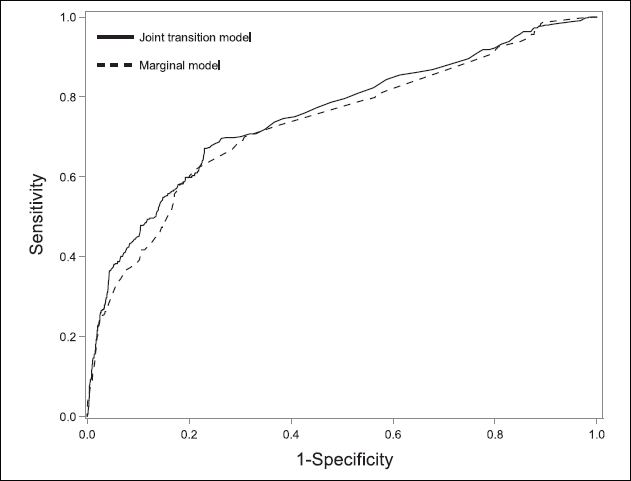
Next, it is of interest how well our model performs in terms of prediction. Rejection probabilities in the joint transition model are calculated based on the entire history, which is captured by the eGFR random effects and the previous biopsy outcome, that is,
General ROC curve comparison between the joint transition model and the marginal model (= univariate transition model) for predicting kidney allograft rejection (ABMRh and/or TCMR). The marginal model (AUC = 0.74) contains the timing of the biopsy, rejection in the previous biopsy (yes/no) and the presence or absence of pre-transplant DSA (based on 2 635 biopsies, in 870 patients). The joint transition model (AUC = 0.75) contains the same parameters + the eGFR trajectories (based on 2 635 biopsies and 40.649 eGFR values, in 870 patients)
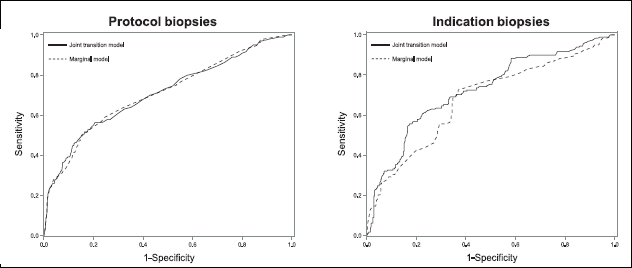
ROC curve comparison between the joint transition model and the marginal model (= univariate transition model), separately for protocol and indication biopsies for predicting kidney allograft rejection (ABMRh and/or TCMR) The marginal model (AUC = 0.72 for protocol biopsies and 0.68 for indication biopsies) contains the timing of the biopsy, rejection in the previous biopsy (yes/no) and the presence or absence of pre-transplant DSA (based on 2 635 biopsies, in 870 patients). The joint transition model (AUC = 0.71 for protocol biopsies and 0.72 for indication biopsies) contains the same parameters + the eGFR trajectories (based on 2 635 biopsies and 40.649 eGFR values, in 870 patients)
Based on the non-significance of the correlation between random intercepts and slopes, we also fitted a model assuming independence, leading to similar inferences and predictive power (AUC = 0.76 in general, AUC = 0.71 in protocol biopsies and AUC = 0.73 in indication biopsies).
Joint transition model for predicting rejection based on the history of rejection and eGFR. We show the maximum likelihood estimates together with the standard errors and P-values based on Wald tests. Joint p-values were calculated via approximate F tests. Inference on the covariance and correlation of the random effects was done via t-tests, in which the standard errors of the estimates were approximated using the delta method
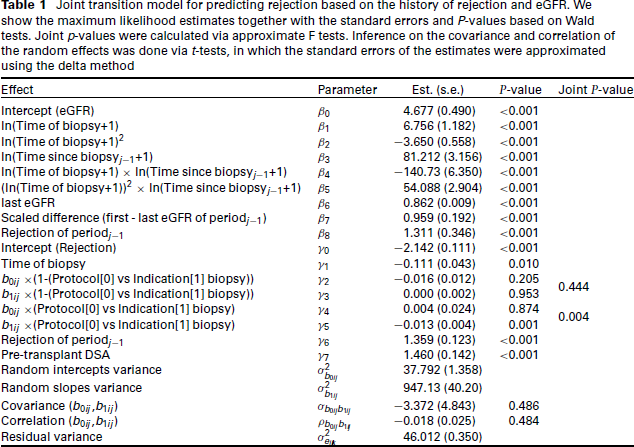
In this article, we developed a transition model with shared parameters in order to evaluate the predictive ability of biopsy history and eGFR for kidney transplant rejection. We confirmed the results reported before, showing that rejection in the previous biopsy and the presence of pre-transplant DSA increase the probability of rejection in the next biopsy. In addition, we confirmed the known fact that the chance of rejection decreases with time post transplantation. Concerning kidney function, evaluated using eGFR trajectories, we found that negatively deviating from the mean slope increases the probability of rejection in indication biopsies. Notwithstanding the significance of the latter effect, the added predictive ability of eGFR was minimal in comparison to a univariate transition model, excluding eGFR. Overall, the classification ability of the joint transition model is mediocre.
By fitting the joint transition model, we responded to the clinical question whether eGFR profiles are predictive for kidney allograft rejection. We showed that, next to the biopsy history, the additional information of longitudinally measured eGFR is rather insensitive for rejection. This opposes our hypothesis that the information contained in the eGFR trajectories would benefit the prediction of rejection, outperforming traditional statistical techniques, which not consider the time-evolution of eGFR. Nevertheless, traditional statistical techniques are not capable of making these complex inferences on the relation between the two longitudinal processes. More specifically, our model allowed to evaluate the strength of the relation between a recurrent biopsy outcome and a longitudinal biomarker and it was able to evaluate the predictive ability of this biomarker. In fact, we are the first to build a joint transition model for studying the association between a longitudinally measured (continuous) biomarker and a recurrent (binary) biopsy outcome. Concretely, we combined a transition model, accounting for historical information in the previous biopsies and eGFR trajectories, with a shared parameter model that correlated characteristics of the current eGFR profile with subsequent rejection.
In kidney transplantation, there is a need for accurate non-invasive biomarkers for rejection and graft failure. Research often focuses on blood or urine biomarkers for rejection at the time of biopsy, or on time-fixed predictors, usually measured at the day of transplantation. Few studies take advantage of the multiple biopsies per patient, or, when they do so, ignore the dependence between the measurements. On top, few studies make use of the multiple measurements of a biomarker. We suggest to focus on the longitudinal information contained in current and new biomarkers and on the combination of these into one model. Trajectory changes in biomarkers could then be related to changes in biopsy outcomes. By developing the joint transition model, we created a framework in which clinical researchers can check for the predictive value of their longitudinal biomarkers for any recurrent biopsy outcome. Because of the transitional component, we reduced the computational complexity of the joint model compared to, for example, full random-effects models. Hence, when several high-potential (longitudinal) biomarkers are detected, we propose to extend the joint transition model to multiple markers in order to implement the risk algorithm in clinical practice.
Although a diagnostic analysis to detect observations with extreme influence on the predictive power of the model would be useful, as shown by Lesaffre and Verbeke, (1998) and Rakhmawati et al. (2016a, 2016b, 2017), there is no unifying approach to measure influence. First, one needs to distinguish between influential observations, influential periods, influential sequences, and influential subjects. Second, many different influence measures can be defined, for example, global versus local influence. Third, influence can differ between various aspects of inference. For example, one needs to distinguish between influence for fixed effects and influence for variance components. Fourth, in contrast to traditional linear models, the influence measures proposed in the literature do not yield much additional insight in why some subjects, periods, sequences or observations have more influence than others. Finally, we are not aware of any influence measures that can be applied in the context of joint mixed models for multivariate longitudinal data with different types of outcomes such as binary and continuous. Therefore, based on these arguments, no influence analysis was performed.
Although the transition and shared parameter model can stand by themselves, the combination of both is unique and applicable to a multiplicity of settings where historic information, whether or not measured longitudinally, needs to be related to another repeatedly measured outcome. Our joint transition model is customized to the specific research setting but can be altered and extended in various ways. Here, we combined a linear mixed model together with a logistic regression model, while assuming conditional independence given the random effects. Yet, other data types require different modelling choices. For instance, Ivanova et al., 2016 used a linear mixed model and proportional odds mixed model to capture the joint distribution of a continuous and an ordinal outcome. We can also include more than one longitudinally measured biomarker, leading to potentially extra random effects, as in Jaffa et al., 2015. After all, the conditional independence assumption can only be justified by including sufficient random effects which capture the association between all processes. As in most transition models, we assumed a first-order autoregressive structure (Serroyen et al., 2009), but obviously, our modelling approach also allows for a more direct link to earlier periods. However, as shown by Diggle et al., 2002 imposing a further dependence in time means to discard at least one extra sequence from the transition model, while potentially affecting the inference for the explanatory variables. Instead of the dependence of the current eGFR profile on a specific summary of eGFR measurements in the previous period, one could also opt for a dependence on the random effects vector of that previous period, leading to a more complex association structure. And finally, from a clinical viewpoint, a possible extension could be to include an additional (marginal) model for the first biopsy post transplantation.
To conclude, we built a joint model that combines transitional components with shared parameters in order to correlate a frequently measured longitudinal biomarker with a less frequently measured binary biopsy outcome. Our model allows for the inclusion of historic data present in the previous biopsies and in the longitudinal trajectories of a biomarker in order to predict the outcome on the next biopsy. Applied to a case in kidney transplantation, we found that the longitudinal information contained in eGFR contributed little, on top of the biopsy history, for the prediction of kidney allograft rejection.
Footnotes
Acknowledgments
The authors received no financial support for the research, authorship and/or publication of this article.