
Abstract
Providing support in the form of information, advice and access to services or social events is promoted as beneficial for people newly diagnosed with dementia and their families. This paper reports on key findings from an evaluation of a post-diagnostic support pilot project in Scotland addressing local service gaps, namely information provision, emotional and practical support and maintaining community links. Twenty-seven participants (14 people newly diagnosed with dementia and 13 family carers) were interviewed at two time points: T1 shortly after joining the pilot project and T2 approximately six months later, to ascertain their views on existing services and the support offered by the pilot project. A comparative thematic analysis revealed that the project facilitated increased independence (associated with increased motivation and self-confidence) of people with dementia. The project illustrates what can be achieved if resources are targeted at providing individualised post-diagnostic support, particularly where there are service delivery gaps.
Introduction
In response to the rising incidence of dementia in the United Kingdom (Knapp & Prince, 2007), dementia has become a national priority with national dementia strategies being developed to address service delivery challenges (Department of Health, 2009; Department of Health Social Services and Public Safety, 2010; Scottish Government, 2010). A key area for these strategies is the provision of excellent support and information to people with dementia and their families following a diagnosis of dementia, in recognition of the gaps they experience following a diagnosis and the potential for crises to occur as a result (Scottish Government, 2010). With a similar focus on the importance of early diagnosis and treatment, the Scottish Government included dementia as one of its core set of health improvement objectives, targets and measures for the National Health Service (NHS), known as HEAT (Health, Efficiency, Access and Treatment) targets (Scottish Government, 2007). This target aims for the early identification and treatment of dementia.
For people recently diagnosed with dementia and their family/friends, there is often a need for emotional and practical support that can help them work through the psychological process of coming to terms with and adapting to their diagnosis. The importance of early intervention has been advocated by Moniz-Cook, Vernooij-Dassen, Woods, Orrell and Interdem Network (2011) and providing support soon after a diagnosis is a key way to promote this agenda. Post-diagnostic support for people with dementia and their families and friends should include activities that enhance or provide social contact and peer support to reduce isolation, provide information and opportunities to overcome limitations imposed on them by the condition and preserve or bolster self-worth by finding ways for them to make a contribution and to feel useful (Clare, 2002). Key to such provision is sufficient knowledge and appropriate engagement of key professionals. Bowes, Mackintosh and Andrews (2009) in a survey of professionals’ information provision to people with dementia and their family carers across Scotland found that:
Oral information giving predominates (98%) with leaflets and books also widely used (87%). As dementia progresses, there is more engagement with carers and less with people with dementia themselves. Twenty per cent of respondents had used information in minority languages and 25% had used formats for people with disabilities. Professionals believe that people with dementia and their carers get their information both from professionals and from family and friends. Eighty per cent consider that people should seek out information for themselves. Fewer than half respondents felt they had sufficient published information available to give out. (Bowes et al., 2009, p. 2)
Bowes et al. (2009) found that some professionals were less knowledgeable about dementia and were less able to provide sufficient information. Their survey indicated a shortage of up-to-date written information, with some information being incomplete or inaccurate. There was also a shortage of locally relevant information of available services and support. Although this study is limited in that it does not seek the potentially quite different views of people with dementia or family members themselves about their experiences of information provision, it usefully draws attention to the patchiness of information provision across Scotland. Even if information given is informative, it may not always be satisfactory, as Mountain and Craig (2012) identified in their exploration of post-diagnostic experiences of people with dementia and their family members in the United Kingdom. They found that people with dementia considered that information was aimed at their family members rather than at them, resulting in increased feelings of powerlessness and helplessness.
Recognition of the need to support people with dementia and their family members has resulted in the development of dementia cafés. The first dementia café was opened in 1997 in the Netherlands, with the original concept described by (Miesen and Blom2001, p. 2) and described as a ‘meeting place for persons with dementia, family, carers and other interested parties’. Since 2000, over 20 dementia or memory cafés have opened in the United Kingdom that follow Miesen’s model. This approach is being further developed with user-led groups for people with dementia (Pratt, Clare, & Aggarwal, 2005). Mason, Clare and Pistrang (2005) in their evaluation of mutual support processes that occur in support groups for people with dementia concluded that a support group for people soon after a diagnosis of dementia can be important for establishing social contacts and building an identity based on social ties with others in the group rather than on the difficulties encountered as a result of the dementia. One way of achieving this, they suggest, would be the opportunity to talk about everyday things and events that are unrelated to the experiences of living with dementia. They suggest that the remit of support groups should go beyond the usual emotional or practical support, to facilitate the development of social contacts and ties. This might be particularly useful for women; for as Dijkhuizen, Clare and Pearce (2006) identify, women stress the importance, for their sense of self or identity, of remaining connected with family and friends.
Pratt et al. (2005) discuss the importance of peer support and sharing of experiences and the value of such groups for increasing self-confidence. They emphasis the importance of bringing people together who can empathise and understand what it is like to live with dementia. Of immense importance, particularly considering the degree of stigma (Goffman, 1968) experienced by people with dementia and their families (Kitwood, 1997), is the role of support groups in allowing people with dementia and those involved in dementia care to meet as equals (Capus, 2005).
This brief review illustrates the variety of initiatives that have been developed to support people with dementia and family members; each with slightly different aims (for example, information provision, peer support or socialisation) and philosophies (for example, person-centred or citizenship approaches). While many service providers take the view that such services can enhance living with dementia, there is little evidence available to draw clear conclusions from. Thus, this evaluation of a post-diagnostic support pilot project provided a particular opportunity to explore the difference (or lack of difference) that post-diagnostic support may make to people’s quality of life in the medium term. This paper reports the views of the project held by people newly diagnosed with dementia and their family members; as such it builds on the body of literature focusing on the views of people with dementia and their carers (Clare, Roth, & Pratt, 2005; Innes, Kelly, & Dincarslan, 2011; McKillop & Wilkinson, 2004; Mountain & Craig, 2012; Mason et al., 2005; Sixsmith & Gibson, 2007).
The post-diagnostic support pilot project
The post-diagnostic support pilot project was funded by the Scottish Government from February 2009 to June 2011. Working in partnership with the Local Council and Community Health Partnerships, the project set out to provide person-centred, personalised support to people who had recently received a diagnosis of early stage dementia and their families. Support was offered for the duration of the project by two project workers employed by a national Alzheimer’s association and with training in mental health and expertise in dementia, with the type and intensity of support varying in intensity according to assessed need. The project workers’ roles were complimentary to the work carried out by existing services delivered, for example, by Community Psychiatric Nurses, Physiotherapists or home care workers. Their work ranged from one-off enquiries (5), to participation in the workshops (39), and/or ongoing support mostly in the form of drop-in cafés (41), one-to-one face-to-face and telephone support (52), through to much more intensive casework, which included planning for the future and/or exploring self-directed support (8). Self-directed support (Scottish Government, 2013) allows people to choose the types of social care support they receive and the level of control they have over their support arrangements; the project workers supported five people with dementia to put in place personalised support packages.
The number of hours of support ranged from a minimum of 1 h for a one-off contact to a maximum of 182 h for someone who was supported by the project for its duration. The mean number of hours of support received was 27 h (see Gilmour, 2011 for a fuller description of the project).
The project was evaluated from January 2010 to April 2011 by a research team based at the University of Stirling.
Evaluation questions
The key evaluation questions guiding interviews with participants with dementia and their family carers were as follows:
What difference, if any, does the post-diagnostic support service make to service access and service use for people with dementia and their carers? What difference, if any, does the post-diagnostic support service make to promoting independence and choice for people with dementia and their carers?
This paper provides a brief overview of the difference the project made to access and service use before focusing on the key concern of this paper, the extent to which post-diagnostic support facilitated independence and the impact this had on participants with dementia, their family carers and wider networks.
Design and methods
Ethical approval was obtained from a Local NHS Research Ethics Committee (LREC). All participants had capacity to give informed consent.
This was a mixed methods study (Silverman, 2005) comparing the experiences of people with dementia and their families who participated in the post-diagnostic support project at two time points (T1 and T2). Methods included semi-structured interviews with people with dementia and their family caregivers (Appendix 1) and administration of quality of life questionnaires, QoL-AD (Logsdon, Gibbons, McCurry, & Teri, 2002), to people with dementia and coping with stress questionnaires, called COPE (Carver, 1997), to family caregivers. The aim of the comparative design (T1 and T2) was to ascertain whether there was any difference in experience of using a post-diagnostic support service over time. This paper reports on the semi-structured interview data as these elucidate very clearly the impact of the project on participants’ experiences and abilities. See Innes, Kelly, Bowes, Macintosh and Robertson (2011) for details of the evaluation.
Sample and recruitment
Posters advertising the evaluation were distributed in participating memory clinics inviting people newly diagnosed with dementia and/or their family members to contact the researchers if they were interested in taking part in the study. To maximise responses, participants were also approached by the post-diagnostic support project team to inform them of the evaluation and their details passed to the researcher with their consent if they wished to discuss the evaluation in more depth with them before deciding whether or not to participate. Fourteen people with dementia and 13 family carers agreed to participate in the evaluation.
Data collection
Semi-structured interviews using a topic guide took place from April 2010 to February 2011. Participants were interviewed at two time points: the first (T1) shortly after joining the project and the second (T2) (using a modified topic guide to reflect findings from initial interviews) approximately six months later to explore their views about the diagnosis, their experiences of current service use and their expectations and plans for the future. The researchers had planned to interview people with dementia and carers separately, to allow for the free and confidential expression of views. However, all but one dyad were interviewed together at their request. One ‘golden rule’ was agreed by participants: that the researcher would direct all questions initially to the person with dementia and then invite the perspective of the family member. This was to ensure the views and perspectives of the person with dementia, which might be in contrast to family members’ views, were given priority and space.
Written consent was obtained by the researcher carrying out interviews from all participants at both interviews. This was particularly important for people with dementia who might have forgotten that they had given consent for the first interview. All participants with dementia were able to give informed consent and, at T2, many remembered the researcher from the first interview. Interviews were carried out in participants’ own homes and audio-recorded with their consent.
Analysis
All audio recordings were transcribed verbatim. Transcripts were read by two researchers to identify thematically similar text within and between interviews (Fielding & Thomas, 2002). Analysis was refined as new themes emerged and these were systematically compared and contrasted across interviews to test emerging propositions (Silverman, 2005). One researcher made initial comparisons over the two time periods and these were verified by a second researcher. All interview data were managed using qualitative data management software Nvivo8. Rigour in data analysis was ensured through regular cross-checking of data, independent verification by another researcher and discussion on areas of disagreement.
Findings
Participant characteristics
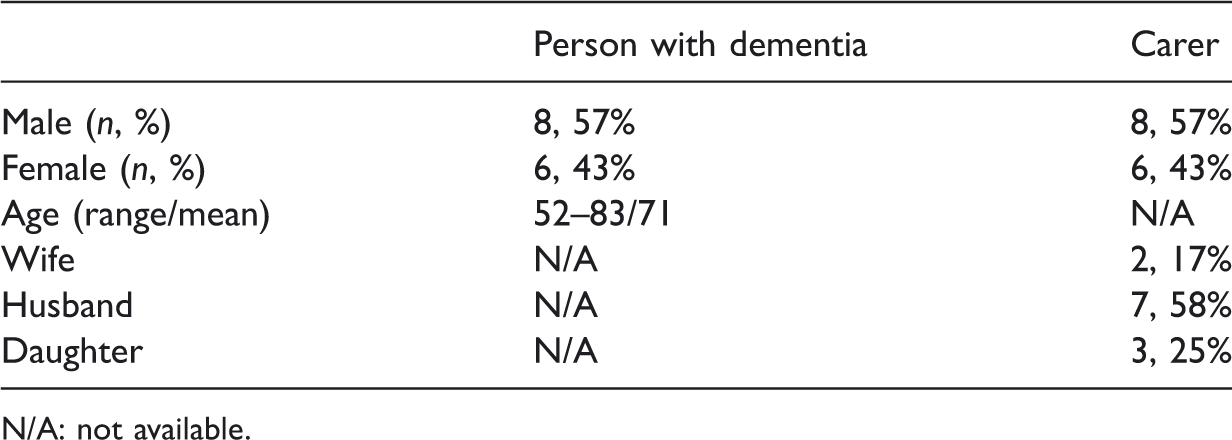
N/A: not available.
A key finding was the extent to which the project facilitated independence of those who used it, and the impact this had on both the participant with dementia and family carers. Associated with increased independence were increased self-confidence and increased motivation; these will be discussed in relation to their role in facilitating independence. First, we will compare participants’ experiences of (1) ‘usual’ services – that is the post-diagnostic support they received from health and social care professionals and (2) support received from the project workers. We will then look more explicitly at the ways the project facilitated choice, and increased motivation and self-confidence of participants with dementia, thereby increasing independence.
‘Being sent away’ versus ‘Opening the door’
Many participants expressed feelings of abandonment or ‘being sent away’ by professionals on receipt of diagnosis. This was particularly the case for those diagnosed with vascular or mixed dementia, who had little or no regular contact with the memory clinic or other services. For example, this carer recalled how, on the day her mother was diagnosed with vascular dementia, there was no discussion or arrangement for follow-up appointments: We were just really told that Mum had mixed dementia. And the doctor explained to me what that meant, and then they were, sort of, cheerio. And basically, to be quite honest, that really was … that really was it. (Carer 6, 1st interview). She (consultant psychiatrist) explained what vascular dementia was. That's all I remember about her visiting there … I'm thinking a year, maybe longer; it could be two years (since her mother had had a medical review). (Carer 6, 2nd interview) If you need them (Memory clinic staff), phone them. That’s all. That’s it. Nobody pops in, you know, you’re kind of just left on your own. To get on with it! (Carer 9, 2nd interview) But they came in and just kind of threw open the door that there's another world out there; yes, you've got it, we can't get away from it, but you've got a life, you've got things to do, and it was just their whole approach … their whole approach, the things they were telling you, the information they gave you, and the way it was done, was the boost or the kick that he needed to get him kind of going again. (Carer 4, 2nd interview) So the girls (Project workers) came out and they actually helped with filling in forms and things like that. (Carer 9, 1st interview)
Several carers also spoke of receiving support with arranging Power of Attorney and valued the input from project workers in negotiating the process. For example: Tomorrow we’ve got a lawyer coming in to give me the power of attorney sort of thing so they gave us all that information. (Carer 5, 1st interview)
Information provision: ‘One size fits all’ versus ‘targeted to individual’
Findings also indicated variation in the quantity and type of information received by people newly diagnosed with dementia and their family carers from medical professionals; it was often in written format (leaflets and books) or verbal format (information and advice on services and support). Five family members and one person newly diagnosed with dementia found the information they received (books and leaflets) along with general advice useful, for example: Oh no, she was very nice, she really was and right away with … we were just coming back, within about two weeks, we got a social worker to give us advice on what to do to get any benefits, or whatever. (Carer 10, 1st interview) It was very good, aye. I think getting started initially down at the clinic down there, conversing with somebody rather than having to read through it all you seem to pick up an awful lot more, so we had a better understanding when we left that day and how things might work out. But the nurses … they were quite good. They were very good as well. (Carer 14, 1st interview) I never really … I never looked for information. I just thought ‘well, we’ll carry on as we are’. (Carer 2, 1st interview) The first one (carers’ group) I went to I wasn’t going back because some of the things, and I’m glad that X (husband) wasn’t there and I don’t really want to repeat some of what I heard there, quite frankly, terrified me and made it ten times worse and I wasn’t going to go back. (Carer 7, 1st interview) But I don’t really want to read about it. (Person with dementia 4, 1st interview) I read them (leaflets) over. (Person with dementia 5, 1st interview) I’ve always tended to take to do with that. (her Carer) But, as I say, there’s been one or two things that have came up that’s kind of helped and things that probably we would never have thought about, we never thought about the rates, getting a cut in rates. It’s only because it was mentioned. (Carer 14, 1st interview) … is probably one of the biggest things that people who are new into this require, somebody that you can talk to without having to think am I annoying them, am I being a nuisance, you know. Never get any impression like that from them. They’re always open to talk to you. (Carer 14, 1st interview) I feel she talks straight to me, so I can handle that, you know what I mean (Person with dementia 15, 1st interview).
In a move away from a ‘one size fits all’ approach, the project workers aimed to deliver individualised information according to a need and desire to know basis. Their approachableness meant that participants felt able to contact them at any time, knowing that they would receive the information they required.
The following sections will explore the extent to which the project facilitated social contact and choice of participants with dementia.
Facilitating social contact
A key issue for some participants was their increasing difficulties with travelling. This had the potential to isolate them as their means of travelling diminished, either through difficulty accessing public transport due to increasing frailty, or through having to give up driving due to increasing cognitive impairment or for financial reasons. One of the ways the project workers supported participants with travelling was to arrange and pay for a taxi or by using their own cars to transport participants to the dementia café or other social events. Providing transport not only alleviated concerns about how to get to the events organised but also maintained social contact. For example, this participant, who had to give up driving, described the positive impact of a bus trip organised by the project workers: So, yes, we had a lovely day up at [place], so little things like that just brighten up your life, don't they? (Person with dementia 8, 2nd interview) But X (project worker) is one of the best taxi drivers going, that’s for sure. She’s jolly, you can talk to her and have a wee laugh about whatever, so she’s really worthwhile talking to. (Person with dementia 9, 2nd interview) The odd chat to one another is half the battle isn’t it? Mingle with one another. That’s a big help itself. When you think of those women that are lonely, left without a man or whatever. Same as men, on their own, things like that. Well that’s … they’ve been in amongst company where they can all chat and that’s it. It’s a big help. (Person with dementia 9, 2nd interview) You get talking to other people and the carers are there as well so you can hear things that they’ve done … . somebody comes up with a wee answer for it. (Carer 14, 1st interview)
Choice and planning ahead
Choice relates to the range of services and support available to both carers and people with dementia that meet their individual needs and preferences rather than the availability of certain service solutions. Planning relates specifically to the aim of the pilot project to support people with thinking about future wishes and needs (advance care planning).
People with dementia and their carers appeared ambivalent about choice of services and choices available to maintain their preferred lifestyle; whether this was because they were still quite early on in the project or whether having a choice in the type of services received was not a familiar concept is unclear. They also had mixed opinions on the frequency of services offered to them by the project: some were happy with it but some wanted more frequent opportunities to meet with others in coffee mornings or more frequent group trips out. This is an example of participants expressing their wishes and possibly wanting to exercise choice and have some control over the types of activities and services offered by the project.
One carer was supported by the project team to use self-directed support to help her to care for her mother in a way that suited them both. Self-directed support allows people to arrange some or all of their support instead of receiving directly provided services from their local authority social work or housing department. This had only just got under way when her mother died, but was positively reported on by the carer: But I’d never heard of self-directed support again until X came on board. I’d never heard of anything like that. I really just kind of thought that we had to put up with what we had. So they were instrumental in putting that across that no, there are other options out there … you can employ someone of your own to come in and do what you want to do. (Carer 2, 1st interview) And I’m saying she enjoyed the company, I mean I was told that she just got so immersed in her art that just really everything was … you know, you didn’t speak to her or anything, she just was immersed in that and that was really good. (Carer 2, 2nd interview)
However, some participants talked of having to give up certain activities, for example Bridge, because of the cognitive difficulties their spouse was experiencing: We miss our Bridge; we used to play Bridge a lot. We don’t now, so we both miss that. Well he was having problems and we just … and it’s a very competitive game, it’s not like a wee friendly game of cards … you get the feeling you’re spoiling other people’s game, if you’re not quite a hundred percent, so we’ve just … just didn’t go back. (Carer 11, 1st interview)
These accounts indicate the importance of people’s families and networks as valuable sources of support; however, for various reasons these may decline or disappear altogether, leaving the person with dementia and their carer at risk of isolation. The post-diagnostic support project enabled people with dementia and their carers to continue activities, to meet new friends and to fill a gap in service delivery following the diagnosis until the dementia progresses and intensive service provision is required.
Participants had some suggestions to improve services offered to them through post-diagnostic support projects, including holding the dementia café on different days to accommodate carers who cannot attend on the regular day: I just wish the workshops were on a Thursday, that's all [laugh], just so that I could have went, because I'm sorry that I miss them. (Carer 6, 1st interview) Line dancing would be good. (Person with dementia 6, 1st interview) They did talk about maybe trying to do wee movie shows, and I thought that would be quite a good idea. (Carer 9, 2nd interview) I think I’d like bus runs, because we used to go a lot of bus runs, didn’t we? (Carer 9 1st interview) And his son played football, so they were thinking, oh well we’ll get a night just for the males, no carers, just for the males and they can all sit and talk about their football, which I thought was a great idea. (Carer 9, 1st interview)
The project was also very useful in alerting participants to and supporting them with applying for entitlements and benefits – many participants would not have accessed these had they not been alerted to their entitlement by the project workers. Support with accessing other services such as Power of Attorney or home care requires a degree of planning and thinking ahead that many participants were not able or willing to engage with. However, the main area in which the project did not achieve its intended outcome was in supporting people to think about what services and supports they might want in the future (advance care planning). This was not necessarily because the project workers did not broach the topic – they did with many participants. Interviews over the two time periods revealed no shifting in thinking from those who just did not want to think ahead. For example: Well, see I don’t like to plan ahead, because I can’t say how I’m going to feel, (Person with dementia 15, 2nd interview) We know that things are not going to improve, we know that, it’s not like a physical illness that can get better. We know that but maybe I’m just like an ostrich and sticking my head in the sand, I don't know. (Carer 10, 2nd interview)
The final finding derived from the interviews is the extent to which the project workers not only promoted independence through their different activities and interventions, but how this started to be enacted by some participants with dementia. This transition appears to have been facilitated, over time, through the personalised one-to-one support offered by the project workers.
Facilitating independence
The post-diagnostic support project aimed to promote independence for participants. Our findings reveal that, through individualised, one-to-one support, some participants with dementia began to re-engage socially or with old hobbies. One carer who wished her mother could become more independent, even though her mother had regular trips to the shops or her church with a volunteer organised by the project workers, was pleased that, over time, her mother had become more outgoing and participated in conversations with other people in the project more often than before: I think they're (project workers) great. My mum, whenever I used to take her anywhere, she didn’t speak. Now, she … you know, she … you don't just speak whenever you're asked a question, you … she actually joins in the conversation, … I think if you hadn't have been going to those things, I don't think she would have. (Carer 6, 2nd interview) But what he has done is because of the nice way they’ve gone about it he has gone out for lunch with them and he’s popped in for a cup of coffee because it’s on his shopping route, you know. He shops at X’s so when he goes in has, you know … he would do that. That’s the one thing I’m quite surprised about, that he’s done that. (Carer 3, 1st interview)
The process of facilitating independence was not an overnight process; for this younger participant, the key issue was first accepting his diagnosis and realising it was not a death sentence. This was achieved with the support of the project workers. His wife says: When you were first diagnosed, one of the questions he kept asking is, how long have I got, how long have I got. He literally viewed it as a death sentence. And the project workers and the group have been good at both saying to him it's not a death sentence, you know, think positive and get on; and then seeing people and meeting people who, you know … you realise that it's not the end of the world for you … . So that's been good. Because … I think it just sort of drags you down. (Carer 4, 2nd interview) It's a skill that I've lost, but I'm trying hard to get back to it and draw something that I can be happy with (Person with dementia 4, 2nd interview)
Discussion
This paper reports on an evaluation of an 18-month post-diagnostic support pilot project established in one region in Scotland in response to government policy to improve the provision of support and information to people and their families following a diagnosis of dementia.
Due to the small number of participants, it is not possible to make generalisations; thus, our discussion is contextualised within this limitation. Several participants felt that the level of ‘usual’ support dropped off once the person with dementia was stable (medication or functioning) and this seemed to be an area of concern, particularly for carers who wanted a regular point of contact. We identified that the post-diagnostic support project had the potential to fill possible gaps (declining networks, reducing clinical input) by offering ongoing, long-term support, whether through social events, advice, information or help with planning as needed and wished.
Our findings align with (Gilmour2011, p. 52), who proposed five key pillars of post-diagnostic support to be worked towards in any post-diagnostic service. These are
Understanding the condition and managing symptoms Supporting community connections Peer support Planning for future care Planning for future decision making.
We identified, and will discuss, the first three in operation: participants valued the different formats and quantities of information provided to them by the project workers and targeted to meet their need for information; participants who had lost natural community supports and were in danger of becoming isolated found new supports through the efforts and organisation of the project workers and participants found comfort and solidarity through meeting others ‘in the same boat’. The last two pillars were less widely achieved, although, as we will discuss, this was not surprising within the timescale of the project.
From the perspective of family members, benefits of a diagnosis include obtaining information, having an explanation for the changes noted and prompting future planning (Connell, Roberts, McLaughlin, & Carpenter, 2009). From our analysis, it would seem that memory clinics and other health services were constrained in the amount and regularity of ongoing information and support they could offer. Our findings also resonate with Mountain and Craig’s (2012) and Bowes et al.’s (2009) findings that information provision is not always satisfactory, particularly targeting information specifically for people newly diagnosed with dementia. As our evaluation has identified, accurate, timely information is crucial both for accessing services, such as carers’ benefits and for fostering in the person with dementia a sense of control over their situation.
The project aligned with the call for early intervention following a diagnosis of dementia (Moniz-Cook et al., 2011) and took a personalisation approach to care provision and support (Mental Health Foundation, 2011). A key finding from this evaluation is that some participants with dementia developed renewed confidence and motivation to take up old hobbies or to re-engage socially. The support given to the woman with dementia to attend an art class to re-kindle her love of painting and the support given to the younger man with dementia to first accept his diagnosis and second take up technical drawing again stand out as examples of the difference a personalised approach and team working can make in the lives of people with dementia and their carers. This was not an overnight process, but resulted from skilful individualised one-to-one support from the project workers, focusing on what was important to the person with dementia and through the stepping stones of increasing socialisation with peers and wider society, imparting relevant information and facilitating choice. This finding, while based on a small sample size and derived from evaluation of one post-diagnostic support pilot project, illustrates that a diagnosis of dementia need not be a ‘death sentence’. It also illustrates one mechanism by which people with dementia may be supported to live well in their own communities (Department of Health, 2009; Scottish Government, 2010).
Findings from interviews suggest that, for carers and people with dementia, the project benefitted them socially through dementia cafés and information sessions, through meeting other people with dementia and their carers, through trips out and through the more intensive one-to-one visits from project workers. This was particularly important for people with dementia living on their own. Participants with dementia spoke of the friendships developing during the dementia cafés, sometimes with other people with dementia and sometimes with other carers. Carers also spoke of the supportive nature of the project. These findings reflect other evidence of the importance for sociability of such groups (Mason et al., 2005), the importance of such groups for increasing self-confidence of those who attend (Pratt et al., 2005) and, as identified above, for allowing people to meet and engage as equals (Capus, 2005). This last point is of significance and was reported by participants, often with surprise, and indicates both the degree of stigma felt by participants in general (Kitwood, 1997) and the shedding of such stigma during the meetings, outings and events facilitated by the project workers.
The project had limited success in facilitating and promoting advanced care planning. This was due to participants’ reported reluctance in thinking too far ahead, while still adapting to the diagnosis. It might also have been due to the relatively short period of involvement with the project and participants’ immediate demand for information and activities rather than forward planning. This reflects Sampson et al. (2010) who identified that carers’ difficulties with making advance care plans for family members with severe dementia included conflicting family dynamics, a general unwillingness to address end of life issues, difficulty with making decisions about hypothetical scenarios and difficulty accepting future deterioration. Hertogh (2011) identified difficulties with advance care plans made by people with dementia themselves as including concerns over the stability of decisions over time, the desire of people not to make decisions about their future or to share decision making with others, and a conflict between professional duty of care and the person’s decision. These, and our findings, highlight the importance of recognising that decisions on difficult topics, particularly advance care planning, will take time and of allowing people to arrive at their own position in their own time, with the support of a familiar and trusted support worker.
Conclusion
Findings from an evaluation of a post-diagnostic support pilot project in a region of Scotland show that it was valued by people with dementia and family members who received support from the project workers. Using the five pillars framework (Gilmour, 2011), post-diagnostic projects such as the one reported on have the potential to fill possible service gaps (insufficient information, absent or reducing clinical input) and compensate for declining social networks. They can offer ongoing, long-term support, whether through social events, advice, information or help with planning as needed and wished. Crucially, this evaluation identified the potential to increase independence, self-motivation and confidence, through provision of one-to-one individualised support, socialisation with peers and wider society and accurate, timely information in a format and pace that suits both the person with dementia and his/her family carer. The strength of the project was its focus on the person with dementia as well as on the family member, with solutions and strategies aimed to meet both their needs. We contend that this type of one-to-one individualised support along with opportunities for socialisation and accurate, timely information are the key elements of post-diagnostic support that have the potential to make a real difference to the lives of people affected by a diagnosis of dementia.
Government targets aimed at increasing the numbers of people diagnosed with dementia and supporting people with dementia to live well in their own communities are laudable; however, there is now a need to develop sufficient, targeted post-diagnostic support services to ensure people newly diagnosed with dementia and their families are not let down by the inability of existing services to meet their needs or achieve these goals. This is particularly important in the current era of financial austerity.
Footnotes
Acknowledgements
We extend our sincere thanks to those with dementia and their family members who took the time to speak to us about their experiences of dementia. We would also like to thank all staff members, including the post-diagnostic support project workers, who gave generously of their time to participate in this study. We would also like to thank Jane Robertson for her help with analysis of data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This evaluation was funded by the Dementia Services Development Trust.