
Abstract
Dementia is a global health issue and the effects on caregivers are substantial. The study aimed to examine the associations of burden, coping, self-efficacy with quality of life among family caregivers of persons with dementia in Singapore. Structured interviews were conducted in a convenience sample of 84 family caregivers caring and seeking clinical care for the persons with dementia in an outpatient clinic of a public hospital in Singapore. The outcome measures included the Family Burden Interview Schedule, Family Crisis Oriented Personal Evaluation Scale, General Perceived Self-Efficacy Scale, and World Health Organization Quality of Life Scale – Brief Version. In general, significant correlations were observed between the quality of life scores with coping strategy and family burden scores, but not between the coping strategy and family burden scores. Compared to demographic factors such as caregiver age and household income, psychosocial factors including family burden, coping strategies, and self-efficacy demonstrated greater association with quality of life in the participants. However, the dynamics of these associations will change with an increasing population of persons with dementia, decreasing nuclear family size, and predicted changes in family living arrangements for the persons with dementia in future. As such, it necessitates continuous study examining the needs and concerns of family caregivers and the relevance of ongoing interventions specific to caregivers of persons with dementia.
Introduction
The World Alzheimer Report estimates that there were 35.6 million people with dementia in 2010. This number is expected to almost double every 20 years, to 65.7 million in 2030 and 115.4 million in 2050 (Wimon & Prince, 2010). By 2040, it is estimated that 71% of people with dementia will be living in developing countries. In India, China, and their south Asian and western Pacific neighbours rates will rise by more than 300% during this period (Ferri et al., 2006).
Singapore is an island state in South-East Asia with a multi-ethnic population of 5.18 million. The majority of Singapore residents are Chinese (74.1%), followed by Malays (13.4%), and Indians (9.2%) (Singapore Department of Statistics, 2012). Approximately 5.2% of people over the age of 65 are suffering from various types and stages of dementia in Singapore; this percentage is predicted to more than double by 2020 with close to 53,000 persons suffering from the disease by then (Alzheimer's Disease Association [Singapore], 2010). Persons with dementia (PWD) can display a diverse range of symptoms and this places substantial demands on family caregivers. A number of Singaporean studies have looked at the impact of caring for a family member with dementia on caregivers, including psychological disturbances, physical health problems, and interpersonal problems (Lim, Griva, Goh, Chionh, & Yap, 2011; Netto, Jenny, & Philip, 2009). These problems can greatly reduce the caregiver's capacity to continue caring for the PWD at home and can result in deteriorating care and even neglect. The psychosocial strains experienced by family caregivers can also increase healthcare demands and socioeconomic costs when PWDs are prematurely institutionalized or unnecessarily admitted to hospital (Papastavrou, Kalokerinou, Papacostas, Tsangari, & Sourtzi, 2007).
While the amount of research about caregiving stress and coping has increased over the last decade (Etters, Goodall, & Harrison, 2008), there are still few studies that add to the understanding of caring for people with dementia in Asian families. Those that do exist rarely examine the dynamics between burden, coping strategies, self-efficacy, and quality of life within the same group of caregivers. This is particularly relevant to Asian societies, where the family is considered to be primarily responsible for caring for ageing relatives and caregivers can face insurmountable and complex demands (Chan, 2010). With rapid socioeconomic change and changes in caregiver demographics in Asian societies, it is important to understand how family members perceive their caregiving burden, and their coping abilities, so that appropriate interventions can be developed to help them. The primary aims of our study were to examine the associations of family caregiver burden, coping strategies, self-efficacy, and quality of life; the secondary aims were to investigate the relationships of these variables with caregivers' age, patients' age, and mean income of the family caregiver. In order to prevent any potential biases, specific inclusion and exclusion criteria outlined under the methods section were adhered to during the recruitment, and the PWD are comprehensively diagnosed for their dementia type and stage before their caregivers were approached to participate in the study.
Methods
Participants
A cross-sectional survey using convenience sampling was conducted on the family members caring for patients in mild to moderate stages of dementia living at home from June 2011 to June 2012. Dementia types included Alzheimer's disease (AD), vascular dementia (VaD), and mixed dementia. The diagnostic criteria dementia was based on DSM-IV TR while the diagnosis of AD and VaD was based on National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association (NINCDS–ADRDA) criteria (McKhann et al., 1984) and VaD based on National Institute of Neurological Disorders and Stroke and Association Internationale pour la Recherché et I'Enseignement en Neurosciences (NINDS–AIREN) criteria (Román et al., 1993). Mixed dementia consisted of AD with evidence cerebrovascular disease (based on clinical or brain imaging evidence) as per NINDS–AIREN criteria (Román et al., 1993). Mild dementia was defined by Global Deterioration Scale (GDS) (Reisberg, Ferris, de Leon, & Crook, 1982) of 4 and/or Clinical Dementia Rating Global Score (CDR Global Score) 0.5–1 while moderate dementia was defined by a GDS of 5–6 and/or CDR Global Score 2 (Berg, 1984; Hughes, Berg, Danziger, Coben, & Martin, 1982). Patients were assessed and evaluated by the geriatrician and caregivers were screened and recruited into the study in the Memory/Geriatric Medicine clinics. The research assistants screened the caregivers based on the inclusion and exclusion criteria stated below and arranged for an appointment to conduct the survey. Consent was obtained and survey conducted by the research assistants on the appointment. The physician and research assistants were fluent in English and Mandarin.
One caregiver was chosen from each family to take part in the study, with first priority given to the spouse, then any children and, finally, any siblings. The primary family caregivers:
had a minimum contact time of 4 h per day with the patient. This included time spent on caregiving activities alone or with the foreign domestic helper. were at least 21 years of age, able to understand English or Chinese (Mandarin) language and had no recorded history of mental disorder.
A total of 84 participants completed this study. This sample size was sufficient to give a power of 0.80 for a two-tailed test with an alpha of 0.05 and a moderate effect size (0.4) (Cohen, 1988).
Ethical approval
Ethical approval of the study was obtained from SingHealth Centralized Institutional Review Board, Singapore. Participants were informed that their participation was voluntary and were assured of confidentiality. Each participant was reimbursed with 10 dollars for their involvement in the study.
Instruments
Socio-demographic data, such as age, gender, income, relationship with the patient, and duration of the patients' illness, were obtained. The following four questionnaires were used to collect data. All the instruments were either in English or Mandarin and have been validated in both languages in Asian countries.
Family Burden Interview Schedule
The Family Burden Interview Schedule (FBIS) (Pai & Kapur, 1981) was used to assess the burden of care in our cohort of family caregivers. It comprises 24 items on a three-point Likert scale that assesses six domains of a caregiver's burden: financial; effect on family routine; effect on family leisure; effect on family interaction; effect on physical health of other family members and effect on mental health of other family members. Higher scores indicate a greater care burden. The FBIS has been validated in both English (Pai & Kapur, 1981) and Chinese (Chien & Norman, 2004) on psychiatric patients. The FBIS was subsequently used among a group of Chinese patients with Alzheimer's disease (Fu, Zhang, & Zhang, 2009). In this study, patients who stayed home experienced greater burden compared to those in nursing homes.
Family Crisis Oriented Personal Evaluation Scales
The Family Crisis Oriented Personal Evaluation Scales (F-COPES) (McCubbin, Thompson, & McCubbin, 2001) consists of 30 items that measure a family's coping strategies in different crises. It contains five subscales (Chui & Chan, 2007; McCubbin et al., 2001):
Acquiring social support strategies Reframing strategies Seeking spiritual support strategies Mobilizing family to acquire and accept help strategies Passive appraisal strategies.
The items were rated on a five-point Likert scale (1 = strongly disagree to 5 = strongly agree) with higher scores indicating that more coping strategies are being used. The F-COPES had previously been administered to a group of family caregivers of individuals with Alzheimer's disease (Pratt, Schmall, Wright, & Cleland, 1985) which found that confidence in problem solving, seeking spiritual support, and seeking family support was associated with less caregiving burden.
World Health Organization Quality of Life Scale – Brief Version
The World Health Organization Quality of Life Scale – Brief Version (WHOQoL-BREF) is an abbreviated version of the original WHOQoL-100 and was tested to have good validity and reliability (Harper & Power, 1998). The WHOQoL-BREF consists of 28 items rated on a five-point Likert scale. It measures QoL in four domains: physical health, psychological, social relationship, and environment. The domain scores obtained from the WHOQoL-BREF demonstrated high correlation (>0.88) with the original WHOQoL-100 survey. The WHOQoL-BREF was validated in a group of individuals with mild to moderate level of dementia, demonstrating an internal consistency ranging from 0.54 to 0.79 (Lucas-Carrasco, Skevington, Gómez-Benito, Rejas, & March, 2011).
General Perceived Self-Efficacy Scale
The General Perceived Self-Efficacy Scale (GPSE) scale was used to measure self-efficacy, which refers to the confidence that family members have in being a caregiver (Jerusalem & Schwarzer, 1992). It consists of 10 items rated on a four-point Likert scale. Higher scores indicate greater competence in coping across a wide range of demanding situations. The GPSE scale was validated (Luszczynska, Scholz, & Schwarzer, 2005) and subsequently administered to a group of early-stage dementia patients and their caregivers to examine the efficacy of an intervention program (Richeson, Boyne, & Brady, 2007).
Data collection
The survey was conducted over a period from July 2011 to May 2012. A research assistant collected data from 84 participants using structured face-to-face interviews. Caregivers who met the inclusion criteria were referred by the clinician to the study investigator at the study venue's outpatient clinic. The nature and purpose of the study were explained to the potential participants. Those who agreed to take part provided written informed consent. The questionnaires were completed using structured face-to-face interviews that took approximately 45 min in either English (75.0%) or Mandarin (25.0%). The interviews were conducted at the participants' residence or a quiet location near their residence. The surveys strictly followed the same order for each of the items stated in the instruments for all participants. Each participant was reimbursed with 10 dollars for their participation. All participants who gave consent completed the entire interview.
Data analysis
Data were analyzed using SPSS version 20. Pearson's r was used to examine relationships between variables. Independent t-test and one-way ANOVA followed by post hoc adjustments for multiple comparisons were conducted. Meaningful variables (all F-COPES subscales, GPSE, patient's age, caregiver's age, and income) were entered into a multiple regression analysis to explore their influence on the quality of life of the participants. Missing data were replaced with scores using the mean substitution method. As the missing data in the current sample were less than the recommended 10% of the full dataset and the items did not differ in difficulty, mean substitution was viable (Widaman, 2006).
Results
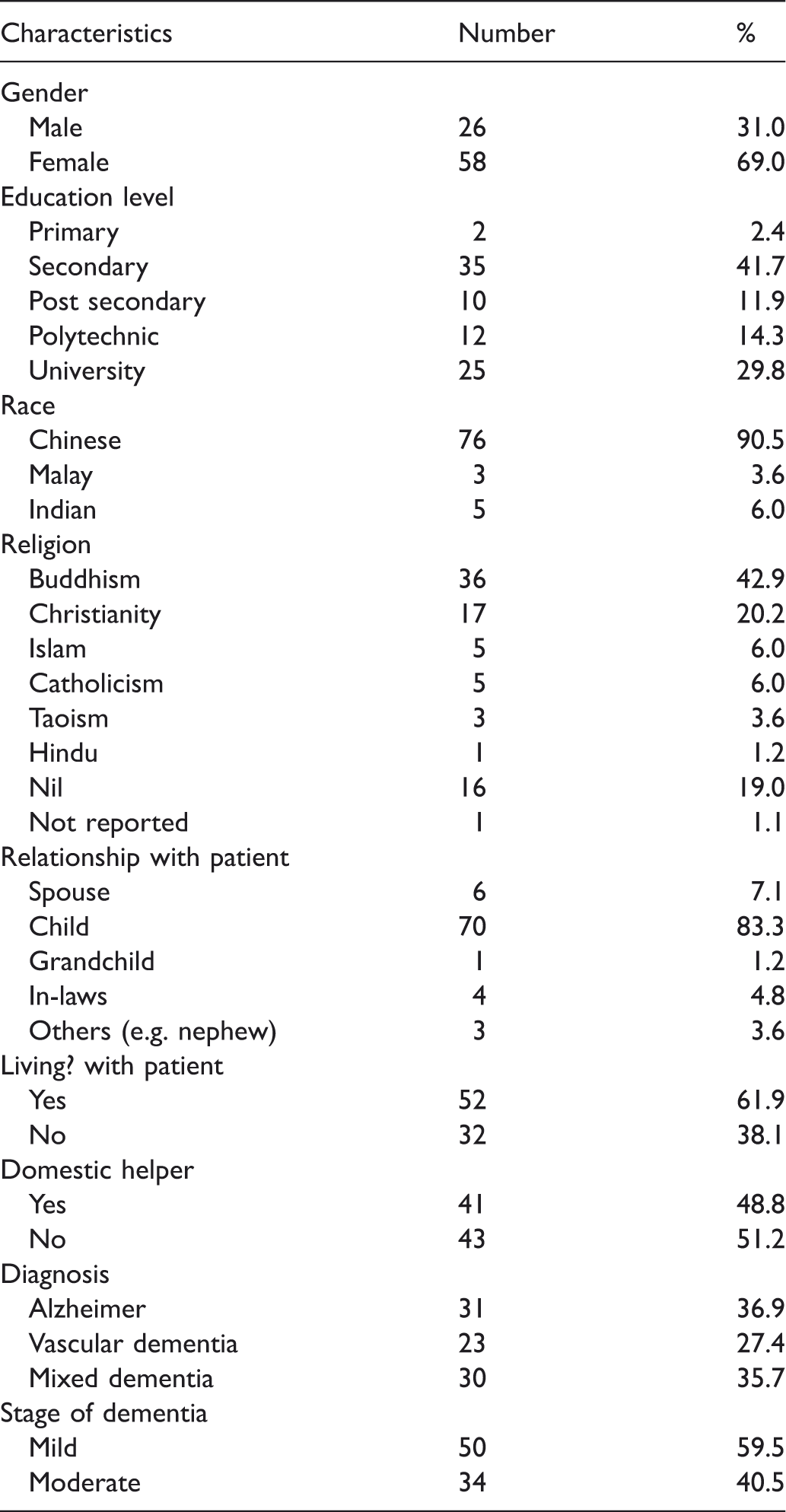
Sample characteristics (n = 84)
Summary scores of the rating scales (n = 84)
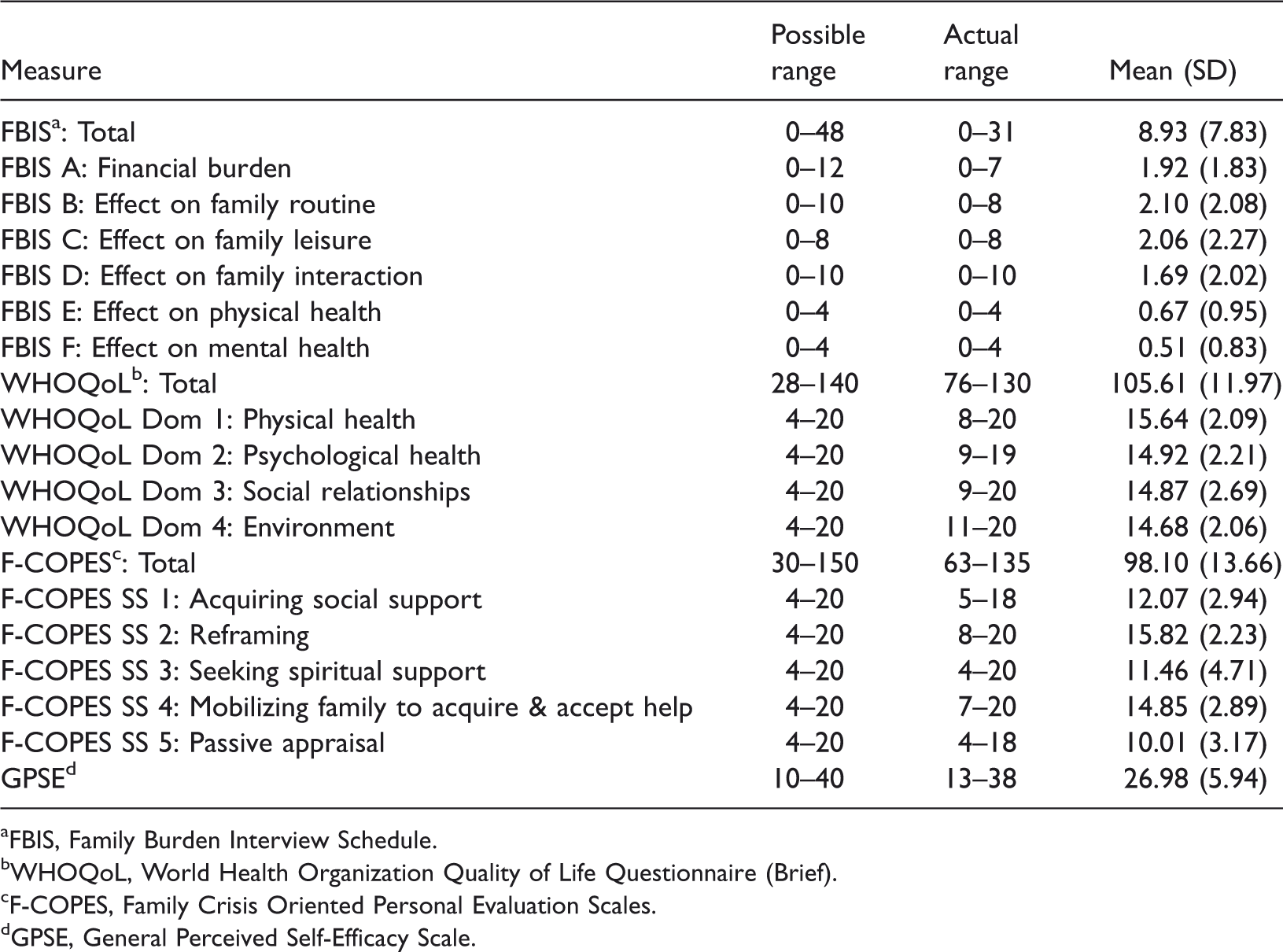
aFBIS, Family Burden Interview Schedule.
bWHOQoL, World Health Organization Quality of Life Questionnaire (Brief).
cF-COPES, Family Crisis Oriented Personal Evaluation Scales.
dGPSE, General Perceived Self-Efficacy Scale.
Correlations between caregiver burden, quality of life, coping strategies, and self-efficacy (n = 84)
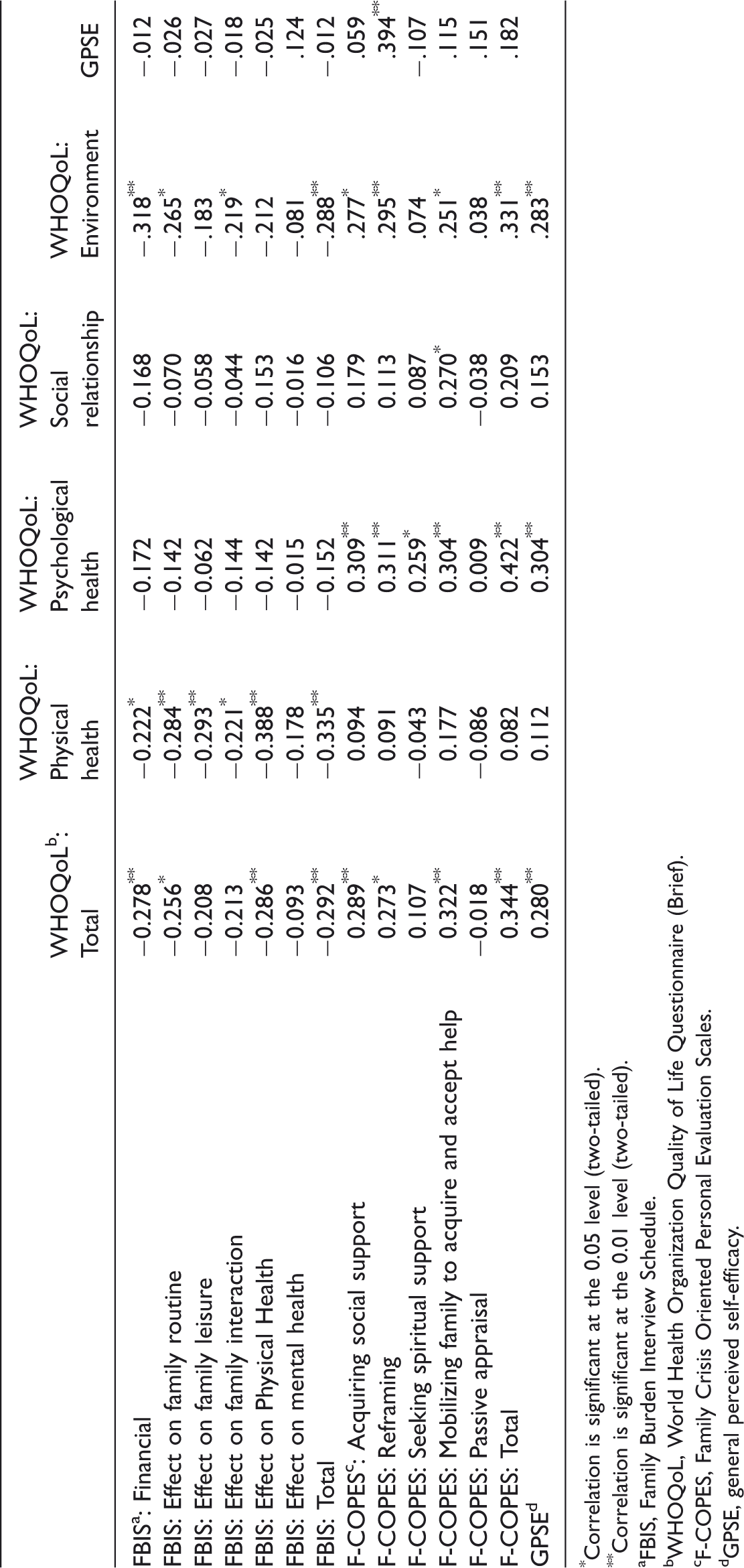
*Correlation is significant at the 0.05 level (two-tailed).
**Correlation is significant at the 0.01 level (two-tailed).
aFBIS, Family Burden Interview Schedule.
bWHOQoL, World Health Organization Quality of Life Questionnaire (Brief).
cF-COPES, Family Crisis Oriented Personal Evaluation Scales.
dGPSE, general perceived self-efficacy.
Correlations between the WHOQoL, F-COPES, FBIS and the demographic variables
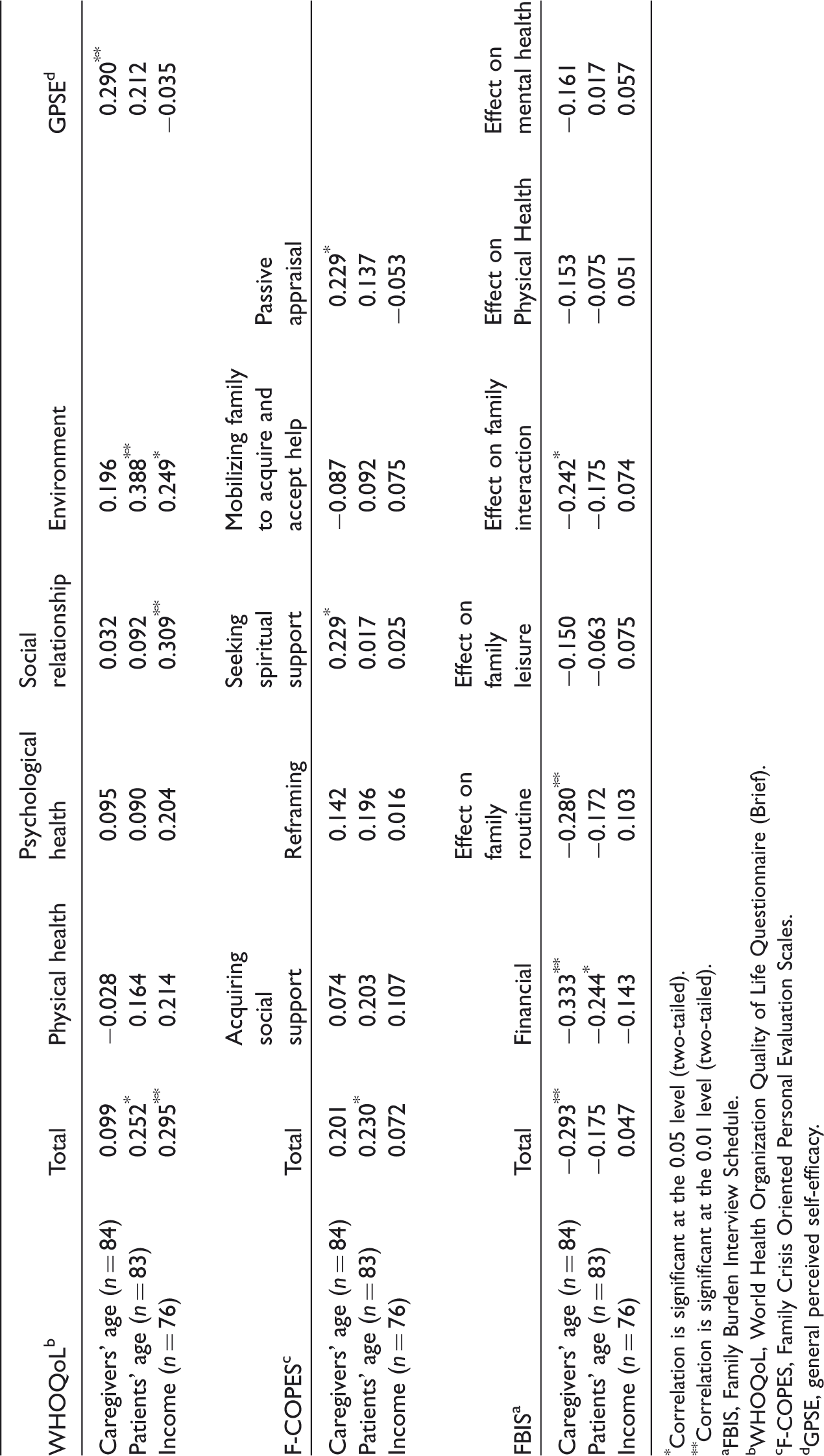
*Correlation is significant at the 0.05 level (two-tailed).
**Correlation is significant at the 0.01 level (two-tailed).
aFBIS, Family Burden Interview Schedule.
bWHOQoL, World Health Organization Quality of Life Questionnaire (Brief).
cF-COPES, Family Crisis Oriented Personal Evaluation Scales.
dGPSE, general perceived self-efficacy.
Dependent factors (FBIS, F-COPES, and GPSE) and demographic variables that attained significant correlations with the WHOQoL-BREF domains were entered into multiple regression analysis. The F-COPES total score (β = 0.29) and the FBIS total score (β = −0.28) were the two predictors that contributed significantly to the variance in the WHOQoL total score, accounting for 17% of the variance, F(2, 79) = 8.22, p = .001). The F-COPES total score (β = 0.39) and the caregivers' general perceived self-efficacy (β = 0.23) were the two predictors that contributed significantly to the variance in the WHOQoL psychological health domain, accounting for 23% of the variance, F(2, 80) = 12.19, p < .001). Both FBIS total score and household income predicted WHOQoL physical health domain and environment domain. Specifically, FBI total score (β = −0.33) and household income (β = 0.23) contributed significantly to the variance in the WHOQoL physical health domain, accounting for 16% of the variance, F(2, 72) = 6.706, p = .002), and FBI total score (β = −0.31) and household income (β = 0.27) contributed significantly to the variance in the WHOQoL environment domain, accounting for 16% of the variance, F(2, 72) = 7.031, p = .002). In all, while participant age and sex were not significant predictors for any of the WHOQoL domains, outcome variables including FBIS, F-COPES, and GPSE are generally associated with the WHOQoL scores particularly the physical health, psychological health, and environmental health domains.
Discussion
Family caregivers are instrumental in the care of PWDs and undertake caregiving tasks on a daily basis that take their toll on caregivers' mental, emotional, spiritual, and physical health (Lim et al., 2011; Papastavrou et al., 2007). While there have been previous research which independently explored caregiving burden, caregivers' perceived quality of life, coping strategies and factors contributing to gain in the caregiving experience in Singapore (Cheah, Han, Chong, Anthony, & Lim, 2012; Lim et al., 2011; Yap et al., 2008), this study examines the associations of caregiver burden, coping ability, self-efficacy with quality of life in family caregivers of PWD in Singapore which has hitherto not been explored in previous papers.
Associations of caregiver burden and QoL
While caregiver burden in this cohort was negatively correlated with quality of life of the caregivers, the quality of life domains affected were mainly the physical health and environment aspects. This is consistent with previous findings that suggested an association between poorer physical health and higher caregiver burden (Pinquart & Sörensen, 2007; Vitaliano, Zhang, & Scanlan, 2003). It is likely that daily physical proximity with a PWD can have an impact on burden and quality of life. A recent publication indicated that living with a patient with dementia was associated with a bigger burden compared to the non-live-in group of family caregivers (Raccichini, Castellani, Civerchia, Fioravanti, & Scarpino, 2009). We note, however, that further analysis of our data showed the live-in or live-out status of the family caregiver had no effect on quality of life or burden. Another consideration pertaining to the caregiver quality of life involves accessibility to health services and transport as the environmental domain questions in the WHOQoL-BREF included items such as “the ease caregiver could move from place to place” and “accessibility and quality of health and social care.” This could reflect caregivers' relative dissatisfaction with or lack of accessibility to dementia care centers.
Associations between coping and quality of life
The coping strategies employed in our study cohort centered mainly on acquiring social support, reframing and mobilizing family to acquire and accept help. These in turn had the greatest association with the psychological and environmental health of the family caregivers. The relationship with self-efficacy was highlighted by perceived self-efficacy having a positive impact on the same quality of life domains. Of note, reframing as a coping strategy had a significant and positive correlation with perceived self-efficacy. Reframing as a positive coping method refers to the family's ability to redefine stressful events in order to make them more manageable (Beck, 1993; Kliewer, Fearnow, & Miller, 1996) and turning stressful events into more positive ones (Pottie & Ingram, 2008). The use of reframing to cope with the burden of caregiving in dementia had been highlighted in a previous paper on Singaporean caregivers (Lim et al., 2011) whereby positive reframing was negatively correlated (but non-significant) with caregiver burden. In the current study, the ability to use this coping strategy is likely reflective of the caregiver profile of the cohort in which the child is the predominant family caregiver with majority (93%) having seconding school education and above; and 79% having a religious belief. These factors, together with filial piety, would likely enable the caregiver to employ reframing as a coping strategy. Filial piety is a pertinent concept in Asian culture where adult children are perceived to be responsible for the care of their aged parents (Chan, 2010; Chan et al., 2009; Mehta, 2005) and may contribute to the attenuation of caregiving burden (Lai, 2010). However, further research is necessary to clarify these conjectures.
Associations of variables with caregiver's age, patient's age, and mean household income
In examining the associations of the outcome variables with patient's age, caregiver's age, and mean income of caregiver, a few findings deserve discussion. While it is not unexpected that older patients with greater comorbidities and increasing frailty exert more burden on the family caregiver financially, and affect family routines and interaction (Cheah et al., 2012), surprisingly the older age of the patient was positively correlated with better quality of life (environment) and decreased financial burden on the family caregiver. A recent paper showed that increasing age of patient was associated with better quality of life and the authors conjectured that this may be attributed to older patients having more experience in dementia issues or being in a social circle with better acceptance of dementia (Banerjee et al., 2006). Regarding the correlation with decreased financial burden, this could be due to the presence of additional financial support from non-family members, family members who did not live with the PWD or financial aid/subsidies although our study was too small and not designed to analyze this.
The older caregiver had greater perceived self-efficacy, better coping ability with reduced caregiving burden but not necessarily better quality of life. Although information on the relationship between caregiver age and burden is limited, older caregivers may have more life experience, greater independence, resilience, and fortitude to cope with their burden (Markowitz, Gutterman, Sadik, & Papadopoulos, 2003). This, however, cannot be generalized. A previous paper on Singaporean caregivers of PWD demonstrated the effect of age on gains in caregiving was tempered by religious and spiritual beliefs as well as encouragement (Lim et al., 2011). The significance of religious beliefs was also demonstrated in the current study as there was a positive correlation with the older caregiver with seeking spiritual support as part of their coping strategy.
The use of passive appraisal as a coping strategy by the older caregiver deserves a mention. Research suggests that this particular coping strategy enables caregivers of patients with mental health issues to relax and recharge their batteries (Eaton, Davis, Hammond, Condon, & McGee, 2011). However, the prolonged use of passive strategies might prevent people from realistically appraising their situation and actively seeking help. This remains to be determined by future research using longitudinal methods.
Last but not least, the association between financial limitations and quality of life of the family caregiver is expected. Caregiving for a PWD is costly and diverts expenditure away from lifestyle choices of the family caregiver. Apart from long-term socioeconomic costs (Papastavrou et al., 2007), individual costs related to dementia care increases with the deterioration of cognitive ability (Hux et al., 1998; Langa et al., 2001; Leon, Cheng, & Neumann, 1998) and this in turn would adversely affect quality of life of the family caregiver.
Future trends and directions
While the current study provides an insight into the associations of burden, coping, perceived self-efficacy, and quality of life of the family caregiver of a PWD in Singapore, the dynamics of these associations would possibly change in future. A recent publication on the future living arrangements of Singaporeans with dementia based on systems dynamics modeling estimated that in 2050, there would be 80,000 individuals with dementia of which slightly over 75% would have limited or no family living arrangement (Thompson, Riley, Eberlein, & Matchar, 2012). Concomitantly, the number of children supporting a PWD, aged 65 years and above, would also be projected to decrease from 5.1 to 6.5 in 2010 to 1.3 to 1.7 in 2050 (Thompson et al., 2012).
In such a scenario of decreased support ratio and increased burden, coping strategies may also change in future. Current pertinent strategies such as mobilizing family members to acquire and accept help may not be relevant in future with decreasing number of children and reduced family network.
The caregiver of a PWD in Singapore in the decades to come would likely be a child (or two children) supporting one or two aging parents with dementia and his/her own family. The family caregiver and PWD would also likely to live apart. There will likely be increasing demand for foreign domestic workers (FDWs), nursing homes, dementia day care, respite care, and home accompaniment or home care services in the years ahead.
In parallel with the changes in caregiver demographics and living arrangement, healthcare financing for dementia care would also change and required to be responsive to the caregivers' needs. While there are current measures such as FDW grants and levy concessions (Ministry of Manpower, 2013), reimbursed transport costs to daycare for lower income earners and subsidized medication cost for low-income earners, future measures suggested include subsidies for home dementia care, respite care and after office-hours home care (Ministry of Finance, 2013). While such measures may ameliorate financial burden pertaining to dementia caregiving, further research on the effectiveness of such measures and the effects on caregiver quality of life should be considered.
Limitations
The current study has limitations. It used a cross-sectional sample of caregivers of PWD attending one outpatient clinic of a public hospital which may not be representative of the populations of caregivers of PWD in Singapore. We acknowledge that there are other caregiver factors not examined in our study which could potentially affect the variables studied such as the caregiver's personality, life/occupational experience, health, style and caregiver–PWD relationship. The cohort of caregivers was predominantly Chinese whose views may not be representative of other ethnic groups. The stage of dementia, behavioral and psychiatric features and their influence on caregiver response were also not considered. Other considerations include the use of community services or home care service which was not taken into account. However, we note that confounders such as whether the caregiver lived with the patient and the availability of a domestic helper did not influence the quality of life, burden or coping strategies used.
Conclusion
Compared to demographic factors such as age and household income, psychosocial factors including family burden, coping strategies and self-efficacy, demonstrated greater association with the quality of life in the present group of caregivers. With an aging population, decreasing nuclear family size and predicted changes in family living arrangements for the PWD in future, the challenges in caring for PWD will evolve in type and form. Burden, coping skills, and perception of self-efficacy will likewise evolve. Continued study of the needs and concerns of family caregivers and implementation of grounded interventions that meet different caregivers' needs will be the key challenge for healthcare providers and society.
Footnotes
Acknowledgements
The authors would like to thank all the participants in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Start-up grant from the Alice Lee Centre for Nursing Studies, Yong Loo Lin School of Medicine, National University of Singapore.