
Abstract
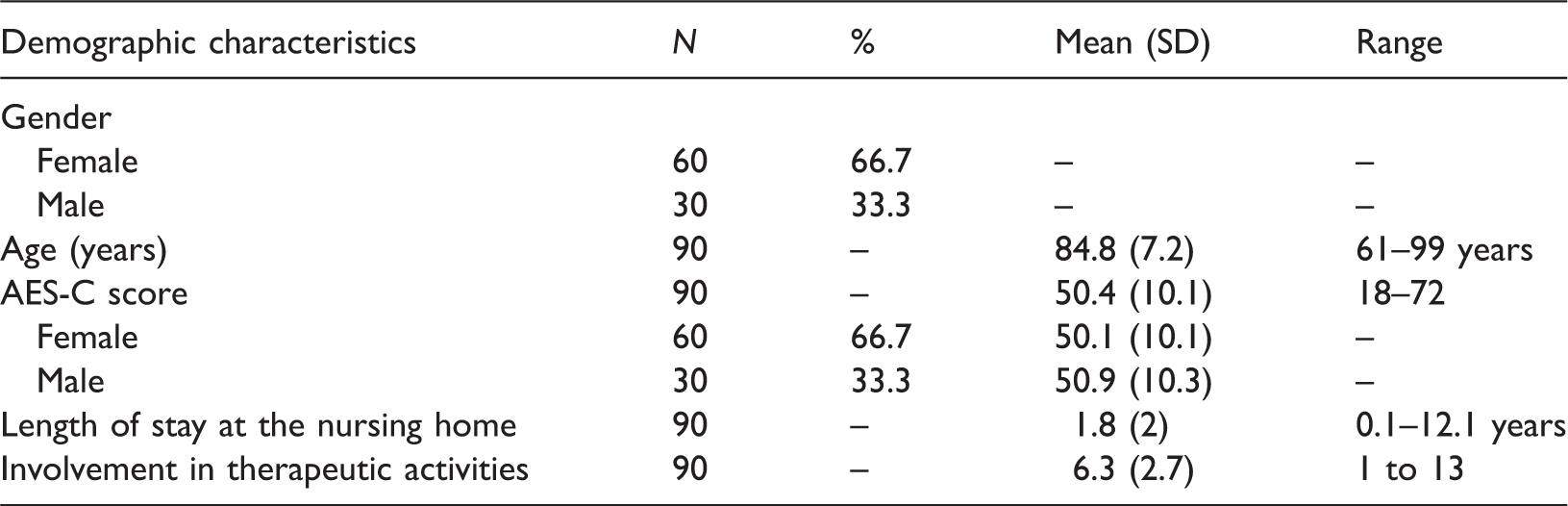
Apathy is one of the most frequent and early symptoms of dementia. Because apathy is characterised by lack of initiative and motivation, it leads to considerable burden being placed on carers to ensure that the person living with dementia has a reasonable quality of life. The aim of this study was to investigate the relationship between apathy and participation in therapeutic activities for older people with dementia living in nursing homes. Ninety residents were recruited into the study, and apathy was measured by nursing home staff using the Apathy Evaluation Scale Clinician version. Staff also compiled data on each resident’s involvement in therapeutic activities. Among this sample, the mean age was 84.8 years, and mean length of stay in the nursing home was 1.8 years. The mean apathy score was 50.4, indicating that on average the residents had a moderate level of apathy. Overall, residents participated in six activities per week and those residents who were involved in the most activities had the lowest levels of apathy. This paper provides evidence that residents involved in therapeutic activities have lower levels of apathy. Further research should be conducted on the direction of causality, whether apathy levels can be changed through participation in therapeutic activities, the relationship between dementia severity and modifiability of apathy, and the intensity of therapeutic activities required to maintain functioning.
Introduction
Apathy or passivity is one of the commonest symptoms of dementia. Lerner, Strauss and Sami (2007) estimated that 92% of people with Alzheimer’s Disease experience apathy, and it appears to become more common as people progress to later stages of dementia (Chow et al., 2009). It has been defined as an absence of responsiveness to stimuli, with lack of responsiveness demonstrated by a lack of self-initiated action (Stuss, van Reekum, & Murphy, 2000). Apathy can be differentiated from depression both clinically and psychometrically even though the two disorders share some common characteristics (Stuss et al., 2000). While apathy may appear to deserve less active treatment than the more overt behavioural and psychological symptoms of dementia, there is some evidence that family carers find it distressing and consequently find it has a greater effect on the quality of relationship between the caregiver and patient than excessive behaviours such as aggression (Doyle & White, 2009; Kuuppelomäki, Sasaki, Yamada, Asakawa, & Shimanouchi, 2004). Apathy may also be misinterpreted by professional carers as resistance to care (Lawlor, 2002). Therefore, it merits treatment not only due to caregiver distress, but also because it is associated with adverse outcomes for the person experiencing apathy, including reduced functional level, decreased response to treatment and poor illness outcome (Van Reekum, Stuss, & Ostrander, 2005).
Psychotropic medication use in residents of nursing homes is controversial because of reports of over-prescription and lack of good evidence for its effectiveness (Huybrechts et al., 2012; National Institute for Health and Clinical Excellence, 2012). A recent systematic review concluded that there is as yet no drug treatment that works well in treating patients for apathy (Brodaty & Burns, 2012). The NICE guidelines for dementia (National Institute for Health and Clinical Excellence, 2012) recommend non-pharmacological interventions as the first line of treatment of behavioural and psychological symptoms of dementia, but in the area of treatment targeted specifically at apathy, few methodologically sound studies have been undertaken, and those studies reviewed generally did not use apathy as the main outcome measure (Brodaty & Burns, 2012).
The highest prevalence of apathy has been found in surveys of nursing home residents, and it has been suggested that some characteristics of the residential care setting (e.g. possible lack of stimulation) may exacerbate the symptoms (Wood et al., 2000).The aim of this study was to examine the association between stimulating therapeutic activities provided in nursing home settings and apathy in the residents living with dementia. We hypothesised that there would be an association between stimulating therapeutic activities and apathy in residents with dementia and that those residents with low apathy would be engaged in stimulating activities. Therefore, we aimed to investigate the relationship between therapeutic lifestyle activities and apathy in nursing home residents with dementia, and propose directions for further research in the area.
A number of therapeutic recreational activities have been evaluated in nursing home settings, without focussing specifically on apathy as an outcome measure. Activities showing positive effects on residents include toy stimulation (Murray, Dickerson, Lichtenberger, & Cox, 2003), horticultural therapy (Gigliotti, Jarrott, & Yorgason, 2004), group music with movement (Sung, Chang, Lee, & Lee, 2006), aerobic exercise (Yu, Savik, Wyman, & Bronas, 2011) and dance (Hamill, Smith, & Rohricht, 2012). Other studies have found improvements in neuropsychiatric behaviours, social behaviour and function as a result of therapeutic activity, such as dog therapy (Perkins, Bartlett, Travers, & Rand, 2008), Tai Chi (Tadros et al., 2013) and multisensory stimulation, which has also been shown to have immediate positive effects on behaviour and mood of people with dementia (Sanchez, Millan-Calenti, Lorenzo-Lopez, & Maseda, 2013). However, Turner (2005) concluded that interventions using aromatherapy, bright lights, walking groups and music showed few promising results, especially in the long term for severe behavioural and psychological symptoms of dementia. Another activity that has been studied is cognitive stimulation therapy (CST). It has been identified that the use of CST for residents with dementia in care homes has resulted in (a) improved cognition and quality of life (Aguirre et al., 2013), (b) improvement on the Dementia Rating Scale (Eckroth-Bucher & Siberski, 2009), (c) improvement in cognitive function with a maintenance program of CST (Orrell, Spector, Thorgrimsen, & Woods, 2005) and (d) promotion of language function (Spector, Orrell, & Woods, 2010). In a qualitative study, participants reported their involvement in CST was emotionally positive and they experienced some cognitive benefits (Spector, Gardner, & Orrell, 2011).
Two papers described the development and evaluation of an intervention called the ‘enriched opportunities program’ (Brooker & Woolley, 2007; Brooker, Woolley, & Lee, 2007). They found a statistically significant increase in the levels of observed well-being and diversity of activity in the 127 older people who were participants in this study. There was also a statistically significant increase in the number of positive staff interactions with the residents following the implementation of this program. Depression in the participants also decreased.
A study by Schreiner, Yamamoto and Shiotani (2005) investigated affect and behaviour in 35 older people with dementia during ordinary time and recreational time. They found that happiness was expressed seven times more often during the recreation time than during the ordinary time. They also identified that almost half (48.9%) of all participants’ ordinary time was spent in doing nothing, and 60% of their ordinary time was spent alone.
In the comprehensive process model of engagement (Cohen-Mansfield et al., 2011) apathy is described as the opposite of engagement, where engagement is defined as ‘the act of being occupied or involved with an external stimulus’ (Cohen-Mansfield, Dakheel-Ali, & Marx, 2009, p. 300). One hundred ninety-three residents with dementia were presented with different stimuli and results indicated that personal attributes (particularly higher cognitive status), environmental factors (especially 2–24 people in the room) and stimulus characteristics (from social stimuli, especially one-to-one interaction) contributed to engagement duration, attention and attitude.
Therefore, in summary, the literature to date provides broad support for the positive benefits of a number of therapeutic recreational activities. However, most studies of therapeutic activities have used broad outcome measures without targeting specific symptoms of dementia, and there needs to be more evidence about the impact of therapeutic activities on specific symptoms, especially apathy. The aim of this study was to increase understanding of the relationship between therapeutic recreational activities and apathy in dementia, and to propose suggestions for further research to improve the quality and methodology used to address the topic.
Method
Our study was conducted in seven nursing homes in Melbourne, Australia. In total, the nursing homes had 710 residents, of whom 310 had a diagnosis of dementia (any type). Residents were assessed on admission using a standardised clinical assessment procedure that is used to apply for federal subsidy of care. The assessment procedure includes the PAS (Jorm et al., 1995) as a standardised indicator of cognitive impairment. Inclusion criteria for the study were:
Residents with mild to moderate dementia diagnosed by their medical practitioner prior to entry or by clinical assessment in the nursing home on admission (or later if available); Residents who were mobile (as above); Residents who have been living in the nursing home for more than a month. Residents diagnosed with severe dementia that precluded involvement in any therapeutic activities; Residents confined to bed; Residents who lived in the residential aged care homes/nursing home for less than one month.
Exclusion criteria:
The above criteria led to 113 residents being approached to participate in the study. Of those approached to participate, 90 agreed and 23 refused, leading to a response rate of 79.6%.
Ethics approval for this study was obtained from the Human Research Ethics Committee of La Trobe University (approval number UHEC 10-064) following organisational approvals from the participating nursing homes.
Measures
The Apathy Evaluation Scale (AES) (Marin, Biedrzycki, & Firinciogullari, 1991) was used to measure apathy in dementia residents. The scale has established reliability and validity, and is suitable for assessment of apathy in people living with dementia (Clarke et al., 2007). It treats apathy as a continuous dimension that may be evaluated in patients whose apathy characterises their overall clinical state, and those in whom it is a symptom of some other syndrome, such as delirium, dementia or depression. The aims of the AES are to: (1) provide a cut-off point for clinically significant apathy; (2) discriminate depression from apathy; and (3) distinguish between different diagnostic groups using only items related to apathy. The scale assesses items such as lack of interests, productivity, initiative, perseverance and affect. These characteristics are consistent with the definition of apathy as lack of motivation. For this study, we used the clinician version (AES-C) (Marin et al., 1991). Items are scored so that high scores indicate more apathy and scores range from 18 to 72. In the original validation study, the mean (standard deviation) score for 30 healthy elderly controls using the AES-C was 26 (SD = 6). The cut-off point recommended for clinically significant apathy is 37.5 (Clarke et al., 2007).
Residents to be approached to participate in the study were identified by nursing staff. The researcher (SS or JE) visited the residents, explained the project, provided the Research Information Guidelines and collected the signed consent form. A standardised training program was delivered to train nursing staff in how to use the AES-C. Lifestyle staff did not assess apathy using the AES-C. The nursing staff were then asked to complete at least one AES while the researchers were at the residential aged care home/nursing home, and the activities staff were also asked to complete an activities questionnaire for these residents (activities staff in nursing homes generally have a one year or less qualification in recreation studies or, less frequently, a degree in occupational therapy). The researchers (JE and SS) collected information from the residents’ medical records. The rest of the assessments were conducted over the following week. Ten residents were assessed by two registered nurses, to check inter-rater reliability. Inter-rater reliability for the AES-C was tested using Cohen’s Kappa which yielded a high reliability score of 0.89. The AES-C was completed by trained nursing staff based on his/her knowledge of the resident over the last month. Items were rated based on the resident’s current functioning (i.e. current interests and daily activities) as evident from the resident's ‘thoughts, feelings, and actions’ during the past four weeks.
Demographic data were collected from the resident’s medical records and consisted of age, gender, medical conditions, medications for dementia and depression (yes/no), length of stay in the facility and marital status. Age was recoded into categories of five years.
The types of activities that the resident was involved in during the previous week, were recorded by the activities staff from the detailed records of each resident. They also documented whether the activity was a group activity or individual activity. These activities were then recoded into five different types of activities: community interaction, cognitive activities, physical activities, spiritual activities and relaxation activities.
Residents’ involvement questionnaire for activities staff

Analysis of data was undertaken using SPSS PASW version 18.0. Statistical analysis was conducted using frequencies, descriptive statistics, mean and standard deviations and parametric and non-parametric tests were used to identify relationships and to test for significance between selected variables and the other variables as identified.
Results
Demographics
Participant demographics
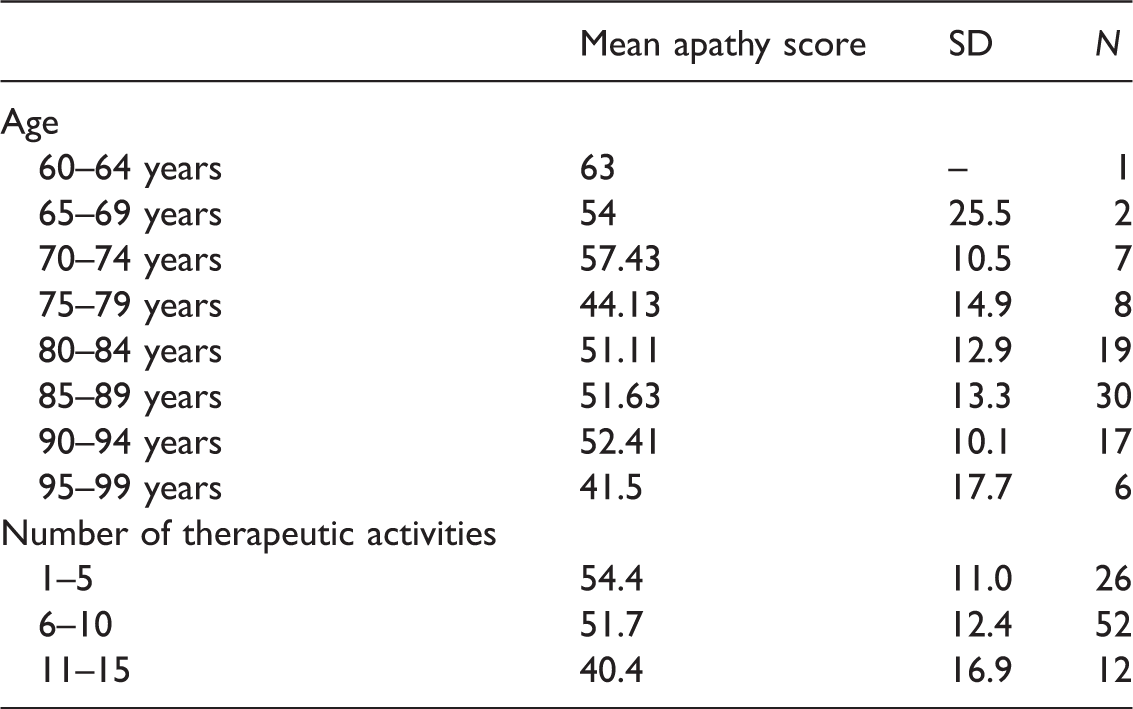
Apathy scores (AES-C) for significant predictor variables
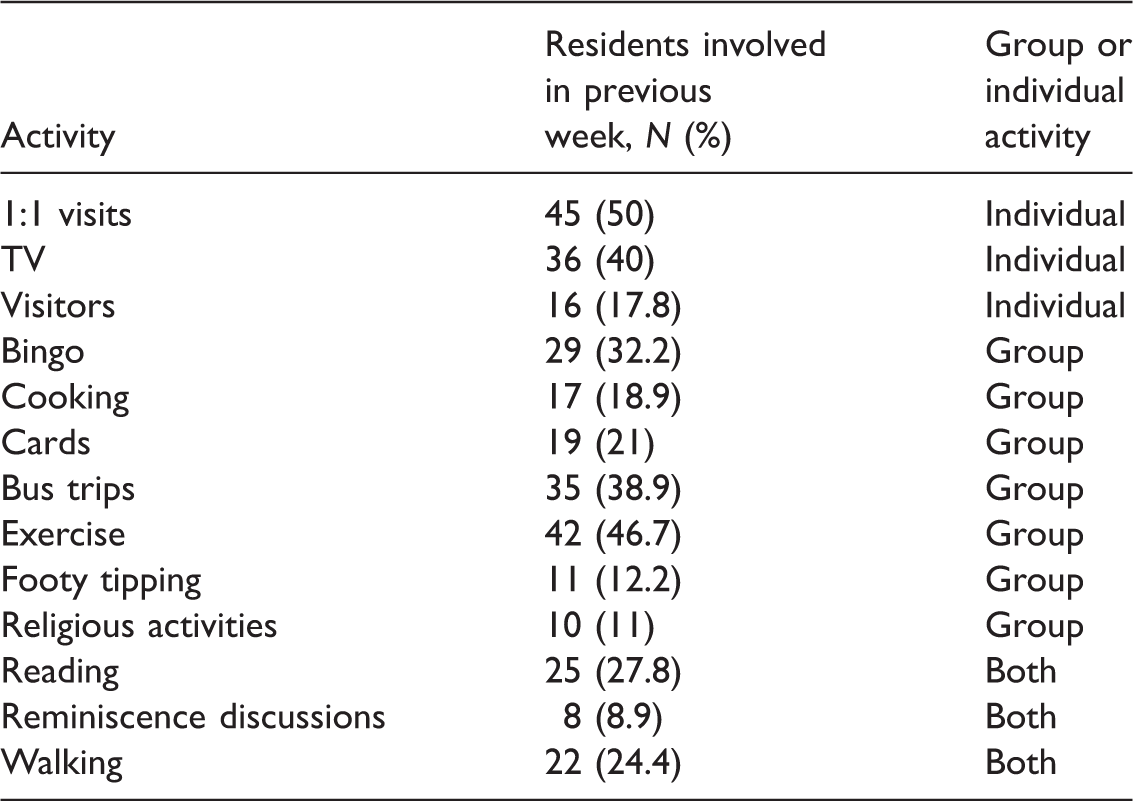
Examples of lifestyle activities and number of residents involved in the previous week
Number of times (%) the 90 residents participated in the five types of activities in the previous week

Community interaction activities consisted of six group events, including bus trips, garden visits, pet therapy, carer visits and visits from relatives and friends and special events, held for publically recognised events, such as football finals (M = .79, SD = 0.73). Thirty-four residents (37.8%) were not involved in a community activity, and 56 residents (62.2%) were involved in between one and three community activities in the previous week. Of interest to the researchers was the number of residents identified by the activities staff who had received visitors in the previous week. The total number of residents who received visitors was only 16 (17.8%). However, there were 60 visits in total, meaning that on average these 16 residents received 3.75 visits per week. A review was undertaken of visitors to the research participants in one residential aged care facility during one week of the study. The information was counted in the visitors’ log, in which all visitors are to sign in on each visit. Of the 35 residents at one of the residential aged care facilities in the study, only 15 received visitors, and the majority received one visitor in the week. However, one resident received 10 visitors in the week and another resident received eight visitors. The total number of visitors to the 15 residents was 40 visits, so these 15 residents received on average 2.7 visits per week. This is less than that identified by the activities staff across all the seven facilities involved in the study.
Spiritual activities consisted of two events, religious services and spiritual activities. On average, residents were less involved in spiritual activities than in any of the other themes (M = 0.31, SD = 0.6). Approximately, 75.6% (n = 68) of residents were not involved in any spiritual activities.
There were 14 activities that were grouped into the Cognitive stimulation theme. Examples were word games, bingo, cards, reminiscence, postcards, reading, talking book, armchair travel, sing-along’s, men’s/ladies group, fun games, news/book club, footy tipping and 1:1 chats with lifestyle staff. On average, residents were involved in more than two cognitive stimulation activities (M = 2.36 with SD = 1.4), range, 1–6 activities. Sixty-two residents (68.9%) were involved in one, two or three cognitive stimulation activities and 22 residents (24.4%) were involved in four, five or six activities.
Physical stimulation activities consisted of eight activities: cooking, active games, bowls, exercise, walking, floor games, creative art and craft. On average, residents were involved in almost two physical stimulation activities (M = 1.61, SD = 1.3). Seventeen residents (18.9%) were not involved in any physical activities; 54 residents (60%) were involved in one or two physical activities, and 19 residents (21.1%) were involved in three, four or five physical activities.
Relaxation activities (nine in total) consisted of watching TV or movies, listening to music, attending concerts, hand massage, aromatherapy, beauty therapy, Sundowner group, happy hour and attending Bar-B-Ques. On average, residents were involved in at least one relaxation activity (M = 1.27, SD = 1.4) and range, 0–5. Fifty-two residents (57.7%) were involved in relaxation activities.
Apathy and therapeutic activities
Overall, there was a significant negative correlation between the apathy score and the sum of therapeutic activities, indicating that the more activities the resident was involved in, the lower their apathy score ( −.239, p = .02). Residents with high apathy scores were involved in fewer activities. There was also a statistically significant negative correlation between apathy score and the relaxation activities, indicating that residents who were involved in the most relaxation activities had the lowest apathy scores (−.388, p = .000).
Number of residents (%) involved activities: Apathy × Lifestyle scores (recoded)

Discussion
Nursing home staff often attempt to include all residents in as many therapeutic activities as possible, motivated perhaps both by instinct that staying active is helpful and the fact that government standards encourage full therapeutic activity programs. Our analysis has shown that although participation in activities is highly variable, the average number of activities for these participants was higher (6.3) than the average number of activities (approximately five) identified in a study by Chiu et al. (2013). We also found that apathy scores correlate with participation, as residents who are participating in many therapeutic activities are those with the low apathy scores. There has also been some recent evidence showing a causal relationship between engagement in therapeutic activities and improvements in apathy (Ferrero-Aras et al., 2011), suggesting that it is worthwhile to try to encourage residents with high apathy to engage in more activities in order to reduce apathy.
Activities could have been categorised in more than one way and activities rated were not mutually exclusive. Only a small percentage of residents were involved in spiritual activities even though spiritual activities were considered an important part of daily life for older people and preferences included in care plans. Staff routinely inquired about spiritual preferences of residents.
One of the major challenges for staff conducting therapeutic activities in nursing homes is to balance the rights of residents to decline being involved in activities that are on offer with the potential therapeutic benefit of getting engaged. Staff also need guidance on what activities are most therapeutic for their residents, and how much activity is necessary. In the same way that a drug is only effective at the right dose, so we need guidance on the right therapeutic dose for activities that are provided in nursing homes. Our results indicate that the participants in relaxation activities had statistically significant lower apathy scores. We propose two reasons for why this result was identified: firstly, it is possible that these activities are familiar and meaningful (Leone, Deudon, Piano, Robert, & Dechamps, 2012) to the residents, and are generally activities that they have participated in for much of their lives – watching TV, listening to music, attending Bar-B-Ques and evening drinks. Meaningful activities were an important determinant of engagement for participants with apathy in the study by Leone et al. (2012). The second reason is that these activities may be more suited to some of the participants’ personalities, and the linking of activities to personality type has been found to decrease passivity and agitation and improve engagement (Kolanowski & Buettner, 2008; Kolanowski, Litaker, Buettner, Moeller, & Costa, 2011).
The role of the activities provided for residents living in residential aged care homes is providing social and psychological interactions with others, which is an important aspect of person-centred care. One of the most important aspects of caring for a person with dementia is to maintain their personhood (Kitwood, 1997). Maintaining personhood and therefore psychological well-being is dependent on the positive relationships people with dementia have with others in their lives. The positive interaction with others sustains the dementia sufferers’ personhood. The person with apathy in dementia often cannot initiate interactions with others and is therefore dependent of others initiating the positive interactions with them. The dementia sufferers with apathy appear to be totally disinterested in those around them, and as indicated by Marin et al. (1991) they do have a lack of motivation, but as a person, still need positive interactions for their psychological well-being. In this study, residents did have the lowest apathy scores when they were involved in a large number of activities, increasing their opportunities to be involved with many other people.
It is important that all staff working in residential aged care homes increase their interactions with all residents, especially those with dementia and not leave this aspect of care to the activities staff. Activities staff identified more residents with apathy than did nursing staff, perhaps because they interacted with residents more than nursing staff who were mainly involved in assessment and medical care and considered activities outside their job roles. People with apathy need everyone to communicate with them to maintain their engagement, not just the activities staff.
Directions for further research
Nursing home environments are not only one of the most challenging environments to conduct research but also one of the most important as the potential for poor outcomes is so great with this vulnerable population. One of the limitations of this study was that we were reliant on the nursing home staff choosing the participants whom they decided would be appropriate to invite into the study, thus meaning that it was a convenience sample used. However, there was no indication of bias in nursing staff’s choice of residents as nursing staff were largely unaware of apathy levels until being trained for this study. Advance care plans that identify whether residents are willing or interested in participating in research would avoid the gatekeeper role of nursing home staff who make decisions on behalf of their residents about whether to invite participation in research. We were reliant on nursing staff conducting the apathy assessments on all of the participants. This was necessary as it is a requirement of the AES-C that the person conducting the assessment must have known the participant for at least one month. We did conduct training and reliability assessments for staff who completed the AES-C scales. During the conduct of our study it became apparent that staff were often unaware of the nature of apathy, and were surprised about the ability to differentially diagnose apathy and depression. Further research is required on the knowledge and attitudes of nursing home staff about apathy, as well as knowledge and attitudes towards the place of activities in the care of residents. This would be particularly pertinent in Australia, where diagnosis of depression is part of a funding model for residential aged care, and staff may confuse apathy with depression.
Nursing staff were involved in resident selection while lifestyle staff were involved in recording level of activities for residents. There was no indication that nursing staff only chose residents for the study who had a high level of activities in order to show their home in a good light. Activities records were used to verify that the activities identified by the lifestyle staff were also shown in the records. As records were retrospective there was no suggestion that activity levels or types of activities were changed to bias the results.
A limitation of this study was that we did not measure dementia severity independently from existing medical records. Ideally, the dementia severity would have been assessed as part of the data collection for the study. However, we did not examine dementia severity as an independent variable. The influence of dementia severity on apathy and activity participation would be an interesting further research question. In this exploratory study, dementia was an inclusion criterion only. The intent of this inclusion criterion was to ensure that we only included residents with dementia in the study, and to exclude residents who had advanced dementia which did not allow them to participate in any of the scheduled activities at all.
We cannot interpret the relationships we found between apathy score and activities undertaken as a causal relationship, although we can speculate that high apathy probably leads to low involvement in activities. Nevertheless, the direction of causality is an empirical question in need of further exploration, as well as further research to understand the causal relationship if it does exist. However, further trials in this area require careful differentiation of the stage of dementia of participants, as apathy may be more easily treated at earlier than later stages of dementia before further cognitive deterioration has occurred. Proper diagnosis of apathy and depression using diagnostic criteria as well as continuous scales, and proper diagnosis of the type of dementia would lead to better identification of the sample in the research, which is very challenging in a nursing home environment.
Further research is also needed into the types of activities that are most likely to impact on apathy, and the role of the social and physical environment that is the context of the intervention, as well as the dose of activities required to impact on apathy. It would also be worthwhile to explore the relationship between severity of dementia and severity of apathy, possible links with environmental factors such as level of stimulation, and the role of personality factors. A time and motion study of the time residents spend in activities and their meaningfulness would be beneficial areas for further study. Finally, when analysing the activities, we only identified the total number of activities as documented by the activities staff. We did not identify the time the residents were involved in the activity or the meaningfulness of the activity, for example, for residents watching TV we did not know if they were interested in watching the program. A source of bias may have been that the televisions might be on and residents assumed to be engaged when in fact they were not. Further research may also be required on the impact of time of day on apathy, since we know that people with dementia are often sensitive to diurnal rhythm. Finally, apathy may fluctuate according to sleep quality and comorbidities such as pain.
Conclusion
In this study, it has been shown that there is a relationship between being involved in therapeutic activities and apathy levels of people living with dementia. A number of suggestions have been made for further research, including the nature of any causal relationship, the impact of severity of dementia on modifiability of apathy, nosology of apathy symptoms, the impact of the social and physical environmental context, attitudes and knowledge of nursing home staff about apathy, and the impact of comorbidities and diurnal rhythm on its manifestation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a small university research grant, which allowed the employment of the research assistant.