
Abstract
A case study comprised of formal interviews, formal observations and informal discussions investigated the motivations and experiences accessing dementia care health and social care services for a Muslim, Pakistani male with dementia. Motivations derived from ‘desperation’ and an inability to access support from family or religious community. Experiences of accessing services were mostly negative. Dementia services were ill-informed about how to support persons with young onset dementia, with pre-existing mental health conditions, from an ethnic minority. Education and training to remove barriers to all dementia care services is required for persons with dementia, their families and within dementia services and religious communities.
Introduction
South Asian persons with dementia are underrepresented in UK health and social care services (Cooper, Tandy, Balamurali, & Livingston, 2010). Despite this, vascular dementia is more common in the UK among Asian and black Caribbean people than the majority white population (Adamson, 1999; Adelman, 2010; Richards et al., 2000; Seabrook & Milne, 2004). One explanation for this is due to the higher rates of cardio-risk factors for cardiovascular disease (Gorelick, 2004), diabetes (Ahtiluoto et al., 2010; Ott, Stolk, van Hanskamp, et al., 1999) and hypertension (Oveisgharan & Hachinski, 2010; Spence, 2004) in these cultural groups. Young onset dementia is especially prevalent in the UK Black and Minority Ethnic (BME) population (Seabrook & Milne, 2004) with 6.1% of all reported BME cases deriving from a young onset dementia variant, compared with 2.2% of cases from the majority ethnic population (Alzheimer’s Society, 2013). In BME communities, there is a higher prevalence of dementia in males than females, but research has shown this may just be a reflection of the higher rate of male immigration in to the UK, whom are now reaching old age (Moriarty, Sharif, & Robinson, 2011).
BME persons are often unaware of available services, unaware of the procedures to apply for these services, and are more likely to be turned down; if they are accepted in to services, they are more likely to be dissatisfied with the provision (Bowes & Wilkinson, 2003; Lindesay, Jagger, Hibbert, Peet, & Moledina, 1997). The Living Well with Dementia: National Dementia Strategy (NDS) (Department of Health, 2009) aimed to achieve better awareness of dementia, encourage early diagnosis of cognitive impairment and improve the quality of living with dementia in the UK. This involved a bid to address inequalities in dementia care, provide support and direction for health and social care commissioners and generate guidelines for planning, implantation and monitoring of services. The NDS aims to offer ‘world class commissioning guidance for dementia’ (Department of Health, 2009, p. 75) securing better quality of life for persons with dementia and their families.
Whilst describing itself as ‘a comprehensive strategy’ (Department of Health, 2009, p. 7) aiming to ‘transcend existing boundaries’ (Department of Health, 2009, p. 7) reduce the stigma associated with dementia, and address health inequalities – despite publishing images of persons from BME communities in the document – the NDS does not explicitly address issues of dementia in the context of BME communities, ethnicity, religion, or race. When stigma is discussed, it is referenced in a generic sense relating to the overall population. For example, ‘50% of the public believes that there is a stigma attached to dementia’ (Department of Health, 2009, p. 27). In antithesis, a later publication, The National Dementia Strategy: Equalities Action Plan (Department of Health, 2011) does account for the potential of religion as a link to services, whilst recognising the current paucity of data in this area. It is unclear if religion in this context relates to BME groups or to the ethnic majority, or to religious services for all persons with dementia. Further research is required in to religion and dementia care in BME persons, to inform policy documentation.
Ethnicity and religion have been identified as factors influencing perceptions of and attitudes towards dementia, and influencing dementia care decisions (Milne & Chryssanthopoulou, 2005; Regan, Bhattacharyya, Kevern, & Rana, 2013), yet many services are not perceived as being culturally appropriate or as delivering ‘culturally competent practice’ (La Fontaine, Ahuja, Bradbury, Phillips, & Oyebode, 2007). Regan, Bhattacharyya, Kevern, and Rana (2013) discuss cultural practices in the context of the National Health Service (NHS) in the UK: ‘The NHS operates within a cultural framework of Western society, where English is the primary language. The organisational culture of the NHS, whilst accommodating for other languages, primarily functions in an English language setting. Modes of being, i.e. communication between persons are governed as acceptable practices, due to the cultural expectations of the Western society. For example, a female touching a male in a simple exchange such as a handshake is considered culturally appropriate. Conversely, this means of communication may be deemed inappropriate in a South Asian cultural setting, for instance.’
The relationship between culture and religion is complex and personal and subject to many factors such as country of origin, country of residence and social setting. It is beyond the scope of this paper to explore this issue in depth, but an overview of the culture–religion distinction and the implications on UK dementia care, is as follows:
Culture
UK based research from the Buddhist, Hindu, Muslim and Sikh faiths (Bowes & Wilkinson, 2003; La Fontaine et al., 2007; Lawrence, Murray, Samsi, & Banjeree, 2008) identified BME people with dementia experience significant barriers when accessing dementia services. The lack of medical knowledge and sense of stigma about dementia and available services may impede access to care provision (Bowes & Wilkinson, 2003; Patel, Mirza, Lindblad, Amstrrup, & Samaoli, 1998). Despite these barriers to dementia services, there is consistent evidence that there is a higher prevalence of some mental health conditions in the south Asian culture than the white British culture (Parkes & Gilbert, 2010); a paradigm of this is the higher rates of suicide and self-harm demonstrated for South Asian women than white women (Husain, Waheed, & Husain, 2006). The reasoning for not accessing health and social care services is given a cultural explanation: ‘Family problems and emotional problems are kept hidden and not exposed to other people. That is our culture’ (Punjabi–Muslim participant, in research study conducted by Simich, Maiter, Moorlag, & Ochocka, 2009 in Parkes & Gilbert, 2010, p. 33). Thus, there is a need to recognise the specific mental health care needs for persons of South Asian culture in the UK (Rait & Burns, 1997).
The paucity of knowledge regarding the aetiology and prognosis of dementia in BME groups has been demonstrated strongly in existing research (Adamson, 1999; Azam, 2007; Beattie, Daker-White, Gillard, & Means, 2005; Brownfoot, 1998; La Fontaine et al., 2007; Lawrence, Samsi, Banerjee, Morgan, & Murray, 2010; Seabrook & Milne, 2003; Turner, Christie, & Haworth, 2005). Eastern Europeans face experiences of persecution as a result of stigma and need to ‘keep face’ (Moriarty et al., 2011). Marriage prospects have been damaged for the children of the family of the BME person with dementia (Mackenzie, 2006; Mackenzie, Coates, Ashraf, Gallagher, & Ismail, 2003; Seabrook & Milne, 2004). Carers feel tarnished by the stigma associated with the person with dementia (Forbat, 2003a). This can result in low service uptake. Both Indian and white British older adults in Manchester had poor knowledge of dementia, but awareness was worse among Indian older people (Purandare, Luthra, Swarbrick, & Burns, 2007). Research has shown lower awareness levels of dementia amongst Irish communities (Brownfoot, 1998) and Black Caribbean persons (Adamson, 1999, 2001; Ahtiluoto et al., 2010; Brownfoot, 1998) than white British counterparts. Carers of individuals with dementia in BME groups observed that awareness of dementia and understanding of the causes of dementia was poor (Adamson, 2001). In many south Asian communities, there is no literal translation for the word ‘dementia’ (Forbat, 2003b; Seabrook & Milne, 2003; Turner et al., 2005). This low awareness has implications for the care sought and received. If dementia is not perceived as an illness, then the appropriate health channels may not be consulted. Many South Asian communities perceive dementia as normal ageing (Azam, 2007; Mukadam, Cooper, & Livingston, 2011; Purandare et al., 2007; Seabrook & Milne, 2009; Turner et al., 2005) and therefore because it is not recognised as a medical condition, care services are not sought, or only accessed in very extreme cases where the family are unable to cope (Bowes & Wilkinson, 2003; Purandare et al., 2007). When a dementia diagnosis is received at a late stage in disease progression – as a result of late presentation to health services – conflict between service provider and dementia carer can arise regarding how best to care for the BME person with dementia (Forbat, 2003a, 2003b; Patel & Mirza, 2000).
Religion
More recent research identified that many of these ‘cultural’ issues identified in the empirical literature, as barriers to dementia care access for BME persons, are actually ‘religious’ specific. Further consideration and investigation of the impact of religious specific issues on dementia care experience for the individual with dementia is required (Regan et al., 2013). The Muslim faith asserts a strong duty of family care and respect for elders which offers one explanation for not presenting to services (Sheik & Gatrad, 2000). As Moriarty, Sharif, and Robinson (2011) exert, ‘religious beliefs may account for some stigma amongst Asian people’. An example of this is the notion that dementia is a result of reincarnation or punishment from a past life (Mackenzie et al., 2003). Negative religious perceptions of acquiring dementia as a result of karmic retribution or punishment, present a barrier to help-seeking (Bowes & Wilkinson, 2003; Jett, 2006; La Fontaine et al., 2007; Zhan, 2004); the notion of ‘religious duty’, leading to sole care within families, presents a barrier to accessing external care services (Braun, Takamura, & Mogeot, 1996; Jett, 2006; La Fontaine et al., 2007; Lawrence et al., 2008; Watari & Gatz, 2004); the stigma and shame of mental illness within faith communities generates a barrier to seeking support within the community (Bowes & Wilkinson, 2003; Braun et al., 1996; Jett, 2006; Jones, Chow, & Gatz, 2006; La Fontaine et al., 2007; Watari & Gatz, 2004; Zhan, 2004). Black Caribbean and Irish people have demonstrated to perceive dementia more as a mental illness with supernatural causes rather than as a biological brain dysfunction (Brownfoot, 1998). The behavioural symptoms of dementia may influence the ability to perform religious rituals, for example, incontinence impeded Muslim home prayer as the house was considered ‘dirty’ (Bowes & Wilkinson, 2003). Stigma associated with mental illness negatively affects religious practices such as arranged marriage; misconceptions regarding the aetiology of the dementia condition, as a result of religious views about God’s will or God’ plan, may prevent people accessing care provision.
South Asian dementia research
Recruitment of people from south Asian communities with dementia in research is notoriously challenging. Bowes and Wilkinson (2002) recognised many barriers to recruiting this particular cohort of people, and 10 years later, many of these barriers still stand: ‘researchers attempting to ascertain the views of south Asian people with dementia face many problems in identifying appropriate research methods’ (Bowes & Wilkinson, 2002, p. 236). The reasons for which are cited as follows: ‘dearth of previous research, few background statistics, issues of diagnosis, problem of identifying and contacting respondents, issues attached to the social identity of researchers and respondents and problems gaining informed consent’ (Bowes & Wilkinson, 2002, p. 236). Identification of persons with dementia is especially problematic due to underrepresentation in UK health and social care services. The carer is often taken as the closest possible advocate for the person and much of the existing research focuses on the views of the carer of the person with dementia (Lindesay et al., 1997). South Asian persons with dementia still warrant the title given to them 10 years ago as a ‘hidden population of extremely vulnerable people’ (Bowes & Wilkinson, 2002, p. 231), with very low numbers accessing health services, making identification for recruitment difficult.
Importance of case study
A person’s own experience of dementia is unique and is influenced by their worldview, outlook, religion and sense of identity; consequently, the care needs of each person with dementia may be equally idiosyncratic. Decisions about how and why to access care for dementia can be a reflection of, and impact upon, the individual’s dignity and ownership of the condition. It should not be presumed that each person follows the same pathways to care, or even perceives ‘care’ in the same way. In antithesis, persons should be fully informed about what care services are available when making decisions about which services to access.
The present study investigates the experiences of a Muslim, Pakistani service user accessing UK dementia health and social care services and aims to understand why and how; namely, why did he chose to access health and social care services solely, despite having a strong footing in a religious community and a supportive family? How did he experience these services once he made the decision to access them? The case study method has a ‘distinct advantage’ when asking a ‘how’ or ‘why’ question (Yin, 2012). The case study aimed to investigate:
Why would a service user from an underrepresented cultural and religious group be motivated to access UK dementia health and social care services? How are people from ethnic and religious minorities supported in UK dementia health and social care services?
Method
The data collection methods utilised to compile the case study
The data forming this case study derives from a larger PhD study investigating the impact of religion on dementia care access and experience for south Asians from the Sikh, Muslim and Hindu communities; focusing on attitudes and perceptions of dementia, decisions about dementia care, provision of dementia care, satisfaction with care services, adequate provision of religion in existing services and barriers to care, influenced by religion. The larger study is a Critical Realist (Strauss & Corbin, 1998; Strauss & Corbin, 1990) Grounded Theory (Charmaz, 2006; Glaser & Strauss, 1967) approach (N = 21) utilising semi-structured interviews and observations in a three phase iterative data collection and data analysis method implementing the Constant Comparison method (Charmaz, 2006), over a 12 month period. The warrants recognition as a ‘stand-alone’ study due to the depth and breadth of data obtained and provides a unique insight into the Muslim perspective of the dementia experience. In addition, this contributes a valuable addition to the overall formation of a theoretical model in the larger study.
Mr Q
Mr Q was initially recruited to participate in an interview for the overall PhD study. The researcher developed a natural rapport with Mr Q and he invited her to accompany him to appointments and to chat with his family and was receptive to attending a dementia peer support group. Mr Q was identified and introduced to the researcher through a dementia organisation already participating in the larger study. This dementia organisation supported and monitored Mr Q throughout the entire research process.
Case study method
The case study method enabled a depth of data to be obtained with a single participant. Recruitment of persons with dementia from the south Asian community is challenging (Bowes & Wilkinson, 2002). It was important to maximise the data collection possibilities once a south Asian person with dementia was identified. Yin (1989, p. 2) defines the case study method as follows: ‘an empirical enquiry that investigates a contemporary phenomenon within its real life context… in which multiple sources of evidence are used’. The case study of Mr Q investigated the experiences of a South Asian person with dementia in their own home and accessing dementia services. This case study employed the biography approach (van der Blonk, 2002) focusing ‘on the life and work of an individual or perhaps group of individuals’ (Remenyi, 2012, p. 134). The multi-faceted approach to data collection strengthened the quality of the resultant theory, ‘case study research is not limited to a single source of data…in fact, good case studies benefit from having multiple sources of evidence’ (Yin, 2012, p. 10). The range of data sources adds ‘methodological value’ to ‘policy analysis and public administration’ (Marinetto, 2012 in Exworthy, Peckham, Powell, & Hann, 2012, p. 332). Klein (1974) recognises the value of ‘methodological and intellectual pluralism’ (in Exworthy et al., 2012, p. 332).
Mr Q’s case study formed part of the third phase in a larger body of data sources and consolidates the defined theory in phases one and two of the overall study, ‘a case study that starts with some theoretical propositions or theory will be easier to implement that one having no propositions’ (Yin, 2012, p. 9). The case study is considered as one piece in the puzzle towards the overall theory development, ‘case studies are often used for theory development. In this case the answering of the research question is a step in the formulation of a theoretical conjecture’ (Remenyi, 2012). Hellström, Nolan, and Lundh (2005) postulates case studies do not permit generalization per se, but may provide insights that can be transferred or ‘recontextualised’ to other like situations.
The strength of the case study is the plurality of data sources enables it to be ‘positivist or interpretivist in orientation’ (Remenyi, 2012, p. 21). Yin (2009, p. 8–13) asserts ‘case studies have a distinct advantage when a ‘how’ or ‘why’ question is being asked about a contemporary set of events over which the investigator has little or no control’. In this sense, a case study can contribute to development of new theory, warranting it a suitable fit for a Critical Realist GT study. ‘In intellectual terms, this methodological flexibility allows researchers to generate theoretical insights’ (Marinetto, 2012, in Exworthy et al., 2012). This case study was constructed to meet the following criteria for exemplary case studies: ‘be significant, provide completeness, consider alternative perspectives, display sufficient evidence and be composed in an engaging manner’ (Yin, 2009, p. 8–13).
Ethical approval and considerations
A three phase process accessing the methodological and ethical rigour of the study was completed prior to data collection to ensure the participants were protected and supported throughout the research. Ethical approval for the overall study was received internally by Staffordshire University on 20th June 2011, externally by the West Midlands: Staffordshire Research and Ethics Committee (REC) on 25th October 2011 and within the Research and Development (R&D) departments of four respective NHS trusts between 28th February 2012 and 17th October 2012.
Informed consent in dementia
Persons with dementia are classed as vulnerable adults who require safeguarding. A topic raised at the West Midlands LREC panel to be addressed was: what measures are in place to account for a person with dementia, who may lack capacity to take part in the research study? The ethical criteria for persons with dementia stated persons with dementia would not be recruited from the offset of the study, if they were not deemed to have capacity. If a participant loses capacity after initial consent has been gained, an appropriate consultee will be approached to assist with the decision to continue (Section 32 (3) Mental Capacity Act, 2005). If consent is not given, the participant will be withdrawn from the study. Participants will be informed of this procedure in the information sheet, prior to initial consent. Mr Q was assessed by a trained consultee and deemed to possess capacity, based on the following criteria (Mental Capacity Act, 2005): understand the information, retain the information long enough to make the decision (to consent), consider the information available to make the decision (to consent) and be able to communicate the decision (to consent). Thus, a nominated consultee was not liaised with in this instance. There were two stages of informed consent for the case study. Mr Q was deemed to have capacity to consent at both stages. Initial consent was obtained prior to the formal interview; subsequent consent was attained prior to the additional data collection methods informing the case study.
Findings
Introduction
The purpose of this case study is to generate an understanding of the experiences and motivations of Mr Q, a Pakistani, Muslim service user accessing UK dementia health and social care services. Existing research postulates south Asian persons with dementia often do not present to dementia health and social care services and may access support from a religious community for a mental health condition, in the first instance (Argo, 2010). Thus, Mr Q’s care seeking behaviour could be viewed as atypical. The purpose of this case study is to understand the motives and circumstances surrounding this expression of atypical care seeking behaviour. It is anticipated that this understanding will have positive implications for dementia care recommendations.
Participant background information
Mr Q is a Pakistani, Muslim male aged 56. He has lived in England most of his life. Currently unemployed, Mr Q worked hard with two jobs, ‘he hired and fired’ in sales and enjoyed people based roles with social contact. At one stage he ran his own business. He speaks seven languages, including English, Gujarati, Urdu, Punjabi, French and local dialects and has worked as a translator. He completed a driving instructor’s course, although he no longer drives. He has excellent writing skills and edited a friend’s book for publication. He has assisted others in a variety of voluntary capacities. He is a very articulate, bright, intelligent and modest person with a dry sense of humour, good manners and social skills.
Family
Mr Q is a widower with three sons, one daughter and one grandchild. He lives with two of the youngest sons and his daughter lives close by. Following the death of his wife, he had a relationship with an English lady for four years but is currently single.
Physical health
Mr Q suffers from a heart condition and received major heart surgery at age 53. Despite appearing outwardly smart, Mr Q said he did not maintain his appearance or his personal hygiene and experienced difficulty bathing.
Mental health
Mr Q has experienced severe anxiety, social phobias and suicidal depression throughout his life and felt this has contributed to his dementia onset. He described himself as an ‘emotional, physical, psychological, every other –ogical there is – wreck – but I am still here’, and had suffered a lot ‘physically, mentally, emotionally and spiritually’ as a result of his mental ill health. Consequently, he rarely leaves the house despite previously being a very confident, sociable person. Mr Q said he has developed a ‘social phobia’ and feels ‘nervous at social gatherings’. He expressed that dementia contributed to him feeling he was ‘losing his identity’. This was very distressing for Mr Q: ‘I sometimes cry myself to sleep because of that’. He expressed his ‘suffering’ and articulated: ‘mental illness, it’s not just physical or psychological, it is also emotional I think’. Mr Q used the following words to describe his mental health difficulties: ‘useless’, ‘limited’, ‘hopeless’, ‘down’, ‘suicidal’, ‘suffered emotionally’, ‘scary’, ‘that wasn’t me’, ‘aching sort of nerve’, ‘salt in wounds’, ‘feel it so much’.
Mr Q described attitudes to mental illness within his Muslim community. He perceived mental illness as a ‘taboo subject’ with a lack of understanding and acceptance and those persons ‘probably think that it doesn’t exist’. Despite this, he articulated that ‘everyone suffers from one form or another’ (of mental illness) as a consequence of our humanity: ‘we are human at the end of the day’. Admitting this is a problem, not only within the Muslim community but across all ethnic groups, ‘it’s admitting that you have a problem, is a problem within all races and culture’. Sharing of problems allows them to be ‘halved’ and that people should be encouraged within their own community to be ‘honest’ and ‘passionate’ about their mental health.
Interestingly, Mr Q was comfortable sharing details of his mental illness with health professionals, but not within his family or friends, ‘I admitted it in front of my GP, but I couldn’t mention it to my family and friends; that was difficult you know’. He discussed ‘shame’ and ‘stigma’ in revealing mental health difficulties to his family and community. Mr Q stated mental illness is a ‘broad term’ that can be ‘misunderstood’ and has ‘assumptions of loopy…madness’. Furthermore, Mr Q’s perception was stigma was prevalent across all ethnicities: ‘I think with any community people would assume, top end of the scale, loopy’.
Diagnosis
Mr Q received a clinical diagnosis of fronto-temporal dementia at age 53. Acetylcholine medication is helping him manage the condition. The diagnosis was received during a check-up scan following heart surgery. Mr Q struggled to accept the clinical diagnosis of dementia he had received: ‘I used to say that I wanted a second opinion’. Mr Q stated the primary reason for this was that he was still at an age where he could work and be useful in society: ‘I couldn’t pinpoint it to dementia, I couldn’t relate to the fact that it is an illness’. Mr Q explained: ‘I thought that was just me, I am forgetful’. Mr Q believes dementia does not affect his daily life but his family notice a decline in memory and behavioural effect. Health services told him he was the ‘youngest person with dementia they know’. In antithesis, Mr Q explained that the diagnosis was useful as he felt comfort in receiving medications, but he had struggled with managing the dosage on his own and found the patches uncomfortable.
Accessing care services
Mr Q offered explanations for why he had sought UK dementia care services, instead of accessing support from family and friends and religious community. This decision derived from ‘desperation’ and ‘pain’ and the ability to ‘open up and admit I had a problem’. He described that he was ‘fortunate to have good knowledge of the (English) language’ which made it an easier decision to use UK services.
Mr Q articulated the difficulty in accessing UK dementia care services once a decision had been made to utilise these services, with ‘transport’ and ‘accompaniment to and at support groups is a problem’. Services are available, but they are not being accessed by members of the Muslim community: ‘there is a barrier of some sort whereby people who are there to help are not being accessed, not being used’. A further barrier to service access was identified through Mr Q’s social phobia: ‘But my problem is to first get in somewhere I have to know somebody, otherwise I will be in pieces’. Mr Q wanted to attend a local dementia café, but expressed a fear of going alone ‘I would go if somebody was there to take me’, ‘if I had somebody I would love to do that’.
Isolation
Mr Q had lost confidence since his dementia diagnosis and did not want people in his community to know about his mental condition, despite informing them of his physical illness. He had become withdrawn and isolated, he ‘hides things very well’, not wanting to ‘burden’ family: ‘I can’t talk to my kids, to my children, I don’t want to bother them’; it is ‘not a childrens’ place to worry about dementia’. Mr Q expressed ‘embarrassment’ at the prospect of sharing his mental illness with the community, of which he had previously been an integral member and a figurehead through ‘embarrassment’: ‘I haven’t told them this is the reason because I find it embarrassing because they know me as someone who has been there for them all the time’. He postulated ‘nobody has dementia’ in the Muslim community he was involved with: ‘I don’t know anybody who has suffered with dementia, so I can’t even relate to anybody’.
This led to feelings of isolation, ‘I have isolated myself from all that’ and ‘the only real problem that I have is that I feel alone’, Mr Q stated he needed ‘somebody that I can talk to’ and craved ‘social contact’ but felt ‘apprehensive’, a ‘bit scared’ and ‘unsure’ about how socialise.
Trust
Mr Q stated the importance of ‘building rapport’ and trust between service provider and service user and the effect on accessing services ‘I could only do that with somebody I could relate to’. He felt that home visits from services may be better than the person with dementia accessing external services as this allowed ‘trust to build up on a one to one level’. Building this trust between person with dementia and service providers would ‘take time’ to ‘talk in confidence’. The importance of communication in building trust was expressed: ‘trust factor is built up and maybe he or she would open up and talking cushions the blow’. Mr Q did not feel that language would be a problem in establishing trust for most Muslims desiring to access services, except ‘those over age 80 years who may experience a language barrier’.
Gender
Issues of gender were prevalent in the data. In terms of trust between care services and persons with dementia, Mr Q believed that this would take time, regardless of gender: ‘I personally believe that it is going to take quite some time for a Muslim person, male or female to earn that trust’.
In terms of care providers, Mr Q stated he felt more comfortable receiving care from females who he perceived as being ‘more sympathetic, more caring than men’ and this impacted on his level of trust and comfort within services he had accessed. He had received care from a female doctor during his heart surgery and perceived female care givers as being ‘more patient’ and a ‘different manner to male (doctors)’ and that female caring was a ‘skill’.
Religious adherence
Mr Q rates his religious beliefs as a strong, constant influence in his life and his faith influences his practice and behaviour more than once a day. He previously held a very influential role in the community as a religious leader, and his father was a respected elder in the Muslim community. He formerly had links with eight main mosques in his local area. His home is furnished with many volumes of religious texts and scriptures, of which he used to pride himself on knowing exactly where to find specific references. His dementia has now affected his ability to read these texts. However, he expressed strategies for keeping track of which volumes he had read. Mr Q’s faith appeared as a source of comfort in coping with the dementia diagnosis, ‘I believe that whatever, whoever is controlling all this has intended for you, you will have’. Despite this, Mr Q did not want to visit the mosques for fear of ‘doing wrong’ during worship.
Low knowledge
Mr Q’s knowledge of dementia was low at diagnosis and continued to be minimal. He was not aware of the prognosis, progression or how to manage dementia, nor was he aware of anyone in his community who had experienced dementia. Mr Q expressed an understanding that once he had received the diagnosis of dementia, he would die from the condition within a few months. Even with assistance from dementia services, Mr Q was unclear about how to manage the condition.
Motivations for accessing health and social care services
Mr Q presented to the dementia services and received his diagnosis, as a result of a physical co-morbidity. What may be considered atypical in this instance is his decision to access health and social care services primarily and solely, without enlisting the support of family, carers, friends or religious community. The reasons Mr Q gave for accessing services were: he had ‘lost the will to live’, he needed to ‘open up’ and admit that he ‘genuinely needed help’.
Perception of dementia services
Mr Q stated there is a ‘lack of communication’ about dementia organisations to the general public: ‘There isn’t a LINK between the organisations and the normal, average people out there’. Organisations do exist but knowledge of them is low: ‘these organisations are there, they exist because there is a demand for it, but even within the host community, there are not people who know about it’. There was recognition of the scale of the issue and that it could ‘take years’ to raise awareness of services and there is simply currently, ‘not enough publicity’.
Despite this, Mr Q felt the services he had accessed were ‘doing the best they can on the resources that they have’. Interestingly, Mr Q articulated that services ‘could be better, not should be better’. He had received ‘brilliant’ care as an inpatient, but that ‘aftercare’ services needed improving: ‘it is not as good as it could be’. Suggestions for improvements were through ‘basic education’, improving ‘rapport’ in care and ‘consistency’ in care providers.
Experiences of dementia care services
Mr Q experienced frustration and dissatisfaction with the eight dementia services he had accessed and felt that his needs had not been met. Three of these services, as observed by the researcher, are described below:
Dementia advocacy service
Mr Q was atypical to their usual service-user base; he was the only non-white service user out of 60 total persons. South Asian persons did not typically access their services, despite the prevalent south Asian demographic residing in the locality. This dementia service admitted being ill-informed about how to provide support for person with young onset dementia, who may be of working age, such as benefit entitlements and with multiple mental health conditions.
Dementia cafe
All attendees were White British in the age 65 years and above age range. The facilitator appeared surprised to see Mr Q and was honest about not being sure how best to offer him help. Mr Q expressed dissatisfaction that he had not ‘learned’ anything about the dementia condition, that no experts were there to speak about the condition, nor that the peer group had shared their own experiences. He felt it was just a place for people ‘to have a cup of tea’ and offered no practical support, information, education or even a space to share anything ‘worthwhile’. Mr Q was expecting an opportunity to ‘offload’ but ‘there was no-one to offload to’. The facilitator made reference to his ethnicity, which was upsetting as he wished to relate to the others on a ‘person-to-person’ level, regardless of culture. A representative of this service provider admitted being ill-informed about how to provide support for Muslim persons with a rare dementia type.
Memory clinic visit
During a clinical visit, Mr Q’s usual physician was not available which caused confusion and anxiety. Mr Q required clarification and reiteration of dementia type, prognosis and implications for care, and reassurance that his dementia was not a result of a ‘stressful life working two jobs’. Mr Q was satisfied that he was not given medication for his depression and anxiety. Mr Q left the service relieved but confused; with no consistent carer to reinforce this information to him if the need arouse at a later date.
Future outlook
Mr Q described his feelings of uncertainty towards his future: ‘what’s going to happen is uncertain still’. His low knowledge of dementia and low confidence in how to live with the condition was articulated through fear of hurting people accidently: ‘I’ve helped God knows how many people, and now that I am suffering from this particular illness, I don’t want to hurt anybody, because I might do that without me knowing’. This fear hindered all elements of Mr Q’s daily living, including his attendance at prayer services in the Mosque for fear of ‘doing the wrong thing’.
Positively, Mr Q perceived a role for himself in the future as assisting others in the Muslim community recognise and live with dementia and mental health issues. He expressed a need to develop a ‘platform for people to have their say’ and a strong desire to assist in working alongside existing health and social care providers to generate a Muslim specific service: ‘if I started something like that on my own and recruited people…go out there and promote the thing in some way’. Furthermore, Mr Q recognised the need to establish a network for all persons with dementia to act as a central hub about existing services and how to access them: ‘there are people that need help, they don’t know where to go, so I think we need something for dementia, but as a whole, we need some sort of advisory network, where they are at least made aware of what type of help is available’, and Mr Q was very enthusiastic about generating such a resource: ‘if I had assistance, someone who understands me 100% and he or she stood by me, I think I could do it’.
Service access disadvantage
UK dementia health and social care services did not adequately cater for Mr Q’s care needs. Mr Q presents a unique case for disadvantage across four levels:
Under age 65 years; Cultural and religious minority; Rare dementia type; Mixed mental health needs.
Recommendations
This case study presents a complex picture but a simple solution is offered. Education is required on three levels:
The person with dementia
On dementia diagnosis, a person should be educated in detail about the condition, the aetiology, available medication and implications, prognosis and care planning in terms of services available and how to access these and feel supported enough to not self-isolate from the religious and wider community.
Dementia services
Health services require education about local care available; incorporating alternative care pathways such as religious communities and promoting psycho-social care. Consistency in clinical consultation is important. Dementia services, advocacy services, dementia cafes and support groups require training on supporting persons with young onset dementia, supporting persons of minority ethnic groups, supporting persons who have rarer forms of dementia and supporting persons who have a multiple mental health issues. It is important to consider the emotional support needs of the individual – alongside the physical and physiological – when generating a care package.
Religious communities
Religious communities are an existing infrastructure which could be utilised as an invaluable resource of social, practical, economical and spiritual support for persons with dementia. Education in religious buildings to the congregation by health and social care professionals, facilitated by a respected leader is imperative for dispelling the stigma of mental illness and generating a strong psycho-social support network. This approach enables the religious practices of the person with dementia alongside practical support for daily living.
Discussion
Case study rigour
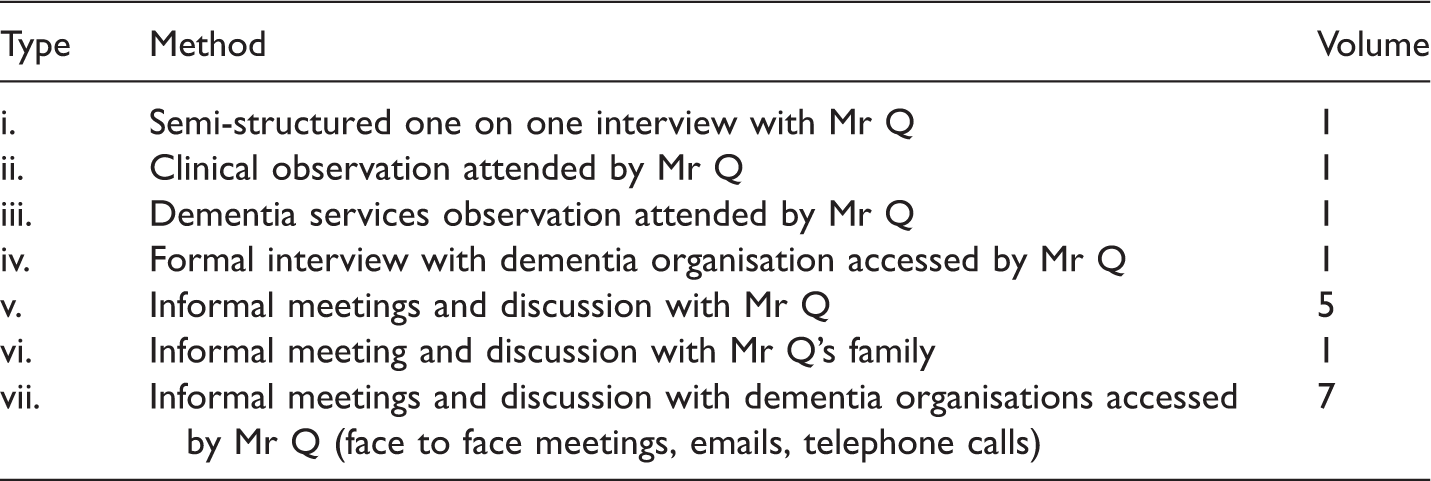
A Critical Realist Grounded Theory approach states the symbiotic influence of researcher and researchee on the data collection process, requires researcher reflexivity, to minimise subjective bias (Strauss & Corbin, 1990). Factors such as gender, socioeconomic status and age (Creswell, 2009, p. 233) may impact on the researcher’s interpretation of data and detract from its objective truth. The researcher – investigating a religion and culture outside of her own – took steps to avoid subjective bias, by utilising a multi-methods approach to data collection (see Table 1)
Generalisability
The objectives of the case study were to answer ‘why’ and ‘how’ questions: the ‘why’ question explored motivations for service access from an atypical service user. The findings demonstrated Mr Q accessed services through ‘desperation’; he did not have support from a spouse, chose not to ‘burden’ family with his care needs and did not access religious support through fear of embarrassment or ‘doing the wrong thing’. The ‘how’ question was twofold: firstly, how did Mr Q experience dementia care services, and secondly, the wider remit aimed to understand how people from ethnic and religious minorities are supported in UK health and social dementia care services. The latter may not be easily answered in a single case study. The researcher is not aware in the empirical literature of any other case studies of dementia focusing on access and experience, from a Muslim perspective; the researcher believes this is the first case study of its kind, which potentially warrants the findings as wholly substantive. Hellström et al.’s (2005) claim that case studies – whilst not able to provide a basis for generalisation – provide useful insights which may be recontextualised to other situations, is considered for the present research: This case study provides useful insights in to the experiences of a Muslim male with dementia, who self-isolated from his religious community and whose experiences with health and social dementia care services were predominantly negative. Based on this single case study, the ability to generalise Mr Q’s experiences is limited, but may potentially be reflective of experiences for South Asian persons with dementia from other faiths.
Furthermore, not only is there a lack of case study data for BME persons with dementia, there is a paucity in the wider research field of dementia and culture, exploring the specific issue of religion’s influence on service access for BME persons with dementia. A systematic review of the literature investigating the influence of religion on access to services for BME persons with dementia (Regan et al., 2013) identified from 1234 papers researching religion and dementia, only 2 papers directly investigated the influence of religion on BME persons with dementia access to services (Levkoff, Levy, & Weitzman, 1999; Sun, Roff, Klemmack, & Burgio, 2008) Both these papers were from research in the United States with Black, Christian communities.
Case study in wider research context
The findings from this case study replicate findings from the wider dementia and culture literature: Mr Q demonstrated low knowledge of available services and when services were accessed, he was predominantly dissatisfied with the provision; reflecting Lindesay, Jagger, Hibbert, Peet Moledina’s (1997) and Bowes & Wilkinson’s (2003) research. Mr Q expressed upset that his ethnicity was referred to whilst accessing a dementia cafe; this mirrors Milne & Chryssanthopoulou’s (2005) findings that dementia services may not be culturally appropriate. Mr Q described many personal and professional barriers to accessing existing services, replicating findings by Bowes & Wilkinson (2003); La Fontaine, Ahuja, Bradbury, Phillips & Oyebode (2007) Lawrence, Murray, Samsi & Banjeree (2008) and Patel, Mirza, Linbald, Amstrrup & Samaoli (1998). Bowes & Wilkinson’s (2002, p. 236) nomenclature of South Asian persons with dementia as a ‘hidden’ demographic highlights the subsequent difficulties identifying and recruiting South Asian persons with dementia in research. The researcher also experienced challenges identifying South Asian persons with dementia for potential recruitment and Mr Q described his ability to ‘hide things very well’, when describing his mental illness. Stigma is a prevalent theme in existing literature to explain the underrepresentation of BME persons in to dementia health and social care services (La Fontaine et al., 2007; Moriarty et al., 2011; Watari & Gatz, 2004; Zhan, 2004). Mr Q expressed a fear of stigma as one explanation for why he hid his dementia from his religious community; he was ‘scared’ of the response from the congregation and the impact of this on his family.
Implications
This highlights the need to focus on the influence of religion on access to care services for BME persons with dementia. Recent research is beginning to investigate perceptions of dementia in the Sikh community (Uppal & Bonas, 2014; Uppal, Bonas, & Philpott, 2014), demonstrating a shift in the research field from cultural influences in dementia care generally, to religious influences in dementia care specifically. The recognition of religion and culture, as two distinct yet intertwined entities is promising (Regan, 2014), but further research is required regarding the practical impact religious beliefs exerts on the motivations to access dementia care services and experiences of these services, once accessed.
Conclusion
This case study highlights the importance of recognising the motivations and experiences of a service user from an underrepresented cultural and religious demographic in to UK dementia health and social care services. Motivations to access health and social care services in the UK should not derive from ‘desperation’, but from an informed choice. Educating all services about dementia and dementia care – traditional and alternative – alongside the person with dementia and their carers is imperative. Whilst Mr Q’s experiences were often negative, investigation of his experiences provided an opportunity to promote the role religious communities, as one alternative care service. Utilisation of a person with dementia’s religious community as an existing untapped resource of support aims to reduce stigma, reduce self-isolation, remove strain from health and social care resources, and improve the dementia care experience, not only for underrepresented groups in dementia care services, but for all persons of faith experiencing dementia.
Footnotes
Author’s note
Written consent was obtained from Mr Q for participation in the study and publication.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.