
Abstract
In this study, the practical application of Integrative Validation Therapy (IVA) in a nursing home for people with dementia was investigated and evaluated from the perspectives of professionals and relatives by using Fourth Generation Evaluation. IVA, a complex intervention frequently applied in Germany’s long-term care settings, is a modification of Feil’s Validation Therapy and contains a specific attitude and several components of action. The findings demonstrate that professionals as well as relatives of nursing home residents gave the intervention a positive rating. From the perspective of the participating professionals, the application of IVA results in less agitated residents which also has an influence on the consumption of benzodiazepine and neuroleptics. The authors conclude that IVA is a beneficial nursing intervention helping to facilitate the illness-related transition process of people with dementia. IVA is able to support them to cope with emotional distress during transition (e.g. irritability, anxiety, depression, changes in self-esteem). Another conclusion is that IVA supports person-centred care because, with IVA, professionals react to typical needs people with dementia have: comfort, inclusion, attachment and identity (Kitwood, 2012).
Introduction
Validation Therapy, developed by Feil (1985, 1992, 1993, 1999), and Integrative Validation Therapy (IVA), a modification of the Feil method by Richard (1994), are two different approaches regarding the interaction with “very old maloriented or disoriented people (…) in the final stage of life” (Feil & Altman, 2004, p. 77) or, more simply, who have a form of dementia (Richard, 2010b). Both methods have differences and similarities regarding their assumptions, theory base, techniques and goals (Erdmann & Schnepp, 2012). The most important similarity is an attitude of respect and absolute appreciation of people with dementia, which is basic to both methods (Feil & Altman, 2004; Richard, 2010a). Feil assumes that very old disoriented people are no longer able to cope with the many physical and social losses they have incurred and this is why they turn back to the past (Feil, 1985; Feil & de Klerk-Rubin, 2010), whereas Richard follows the medical approach in which dementia is just an organic disease of the brain (Richard, 2010b). Based on these two fundamental assumptions, various validation techniques are used (Erdmann & Schnepp, 2012).
Richard’s (2010b) validation techniques are the following: (1) Perceive feelings (e.g. anxiety) and motivation (e.g. diligence) of the person. (2) Validate feelings and motivation with short sentences like “Everybody would be anxious about that.” (Richard, 2010b, p. 6; translation by the authors), “You know your duties.” (Richard, 2010b, p. 6; translation by the authors). (3) Generalize feelings and motivation with common phrases such as proverbs, wise saying, songs or biblical sayings: A day of sorrow is longer than a month of joy; Many hands make light work. (4) Validate the person with short sentences about biographical themes, for example, for a teacher: “As a teacher, you love children” (Richard, 2010b, p. 6; translation by the authors).
The Feil method came to be applied in dementia care in many countries of the world (Neal & Barton Wright, 2003). IVA is a comparably young intervention method, but currently training courses are being given in Germany, Switzerland, Austria, Italy, Croatia and in the Czech Republic (Richard, 2013). However, research about IVA does not yet exist (Erdmann & Schnepp, 2012). In this paper, we publish findings from our qualitative evaluation study in a long-term care facility (LTCF) for people with dementia in Germany, which forms part of the doctoral thesis by the first author.
The study
Objective
The evaluation study was based on two central research questions:
With which categories can we describe the practice of IVA? How is IVA evaluated by nurses and relatives?
From these questions, we derived the following study objectives. The first objective was
to develop a case study about how IVA is practiced in an LTCF, second, to generate hypotheses about the effects of IVA on people with dementia, their relatives and their nurses, third, to explore how IVA is accepted by nurses and relatives of people with dementia.
Research design
We chose Fourth Generation Evaluation (Guba & Lincoln, 1989) as a descriptive and exploratory design, which provides a structured framework for evaluation of new programs, processes, organizations (Lüders, 2006) or nursing interventions (Duhamel & Talbot, 2004). Fourth Generation Evaluation, also known as constructivist evaluation, is based on the assumptions of constructivism. The basic methodological assumption of constructivism is hermeneutic-dialecticism, that is, a process by which constructions entertained by the several involved individuals and groups (stakeholders) are first uncovered and plumbed for meaning and then confronted, compared, and contrasted in encounter situations. The first of these processes is the hermeneutic; the second the dialectic. (Guba & Lincoln, 2001, p. 1)
The authors emphasize that under this methodological assumption, nothing is said about methods, so both methods, qualitative and quantitative, can be used (Guba & Lincoln, 2001).
Data collection
Concerning our objectives stated above, we preferred qualitative methods for data collection. We performed “problem-centred interviews” (Lamnek, 1993, p. 74; translation by the authors) with an interview guide, observations with a low degree of participation and for the dialectic process, focus group discussions. Problem-centred interviews are conversational in style. The interviewer gives a narrative stimulus, but also an interview guide is used as a checklist to ensure that all relevant questions are asked before the interview ends. During the interview, the interviewer uses three strategies to follow the narration: (1) The interviewer establishes his/her understanding by mirroring the narration in own words, (2) he/she asks clarifying questions and (3) he/she confronts the participant with contradictions, unexplained topics or inconsistences. In the last phase of the interview, “ad hoc questions” (Lamnek, 1993, p. 76, translation by the authors) allow to raise not already discussed topics (Lamnek, 1993).
Setting
The study was carried out in a specialized nursing home for 61 elderly with dementia in a small village in Northern Germany. The residents in that nursing home spend their day in four different groups: One larger group for 30 people without challenging behavior, two smaller groups, each with 12 people suffering from behavioral disturbances and one small group of seven people in the last stage of dementia, who are immobile, cannot talk anymore and need a very quiet, caring environment.
Participants
Nursing home interview partners.
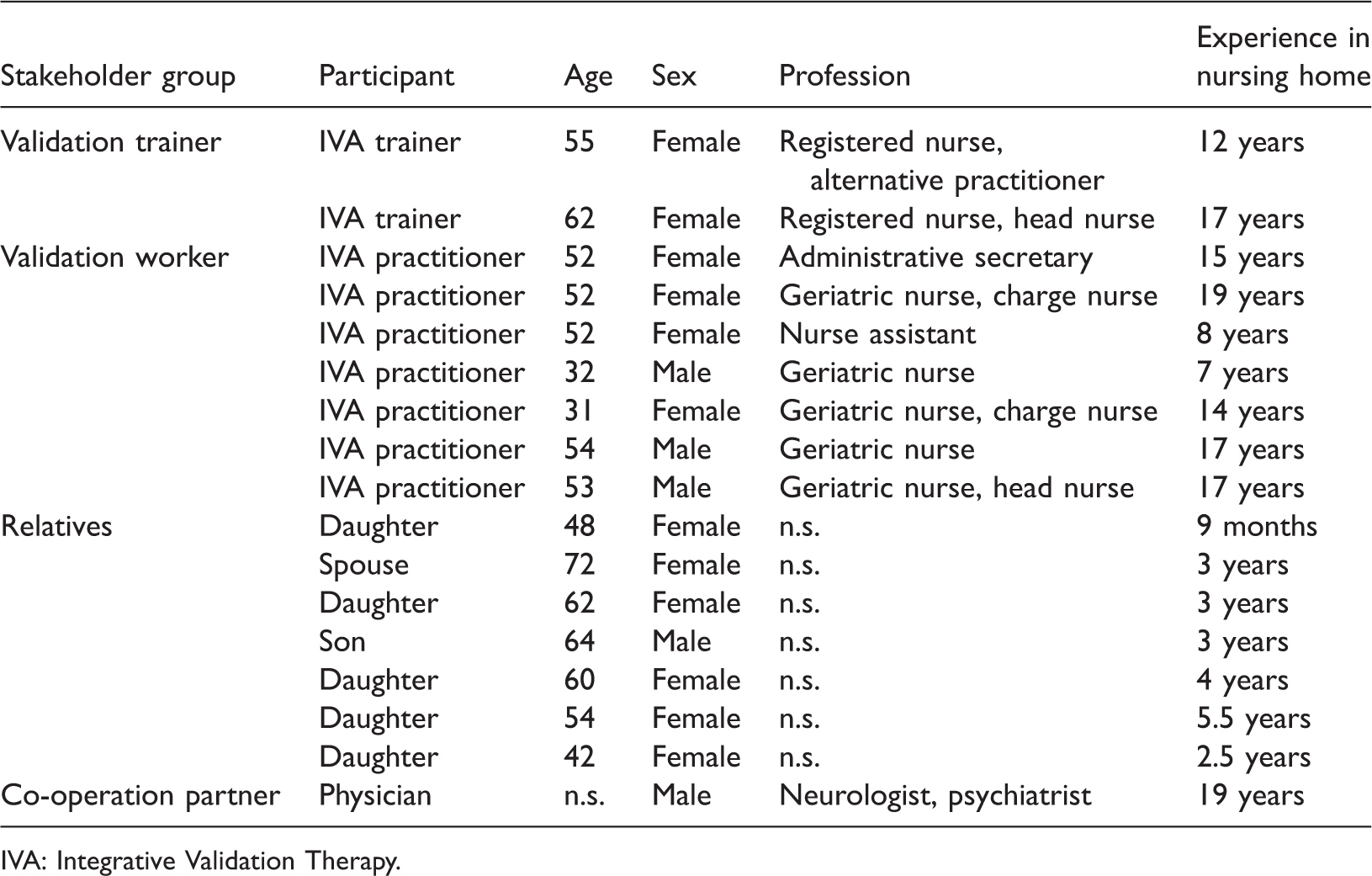
IVA: Integrative Validation Therapy.
Participating observations in nursing home.

After qualitative content analysis (Mayring, 2008) of the interviews, we presented and discussed our findings in two focus group sessions: (1) A focus group session with IVA practitioners and one IVA trainer from the participating nursing home and (2) a focus group session with two IVA trainers from the participating nursing home, 14 other IVA trainers from Germany and Switzerland and the originator of the method, Richard. During these focus group sessions, we compared and contrasted our findings and worked out a final “higher-level synthesis” (Guba & Lincoln, 1989, p. 149) of contradictory statements (dialectic process). The whole constructivist evaluation process is visualized in Figure 1.
Flow of Fourth Generation Evaluation modified for the evaluation of IVA (Erdmann & Schnepp, 2013; Guba & Lincoln, 1989).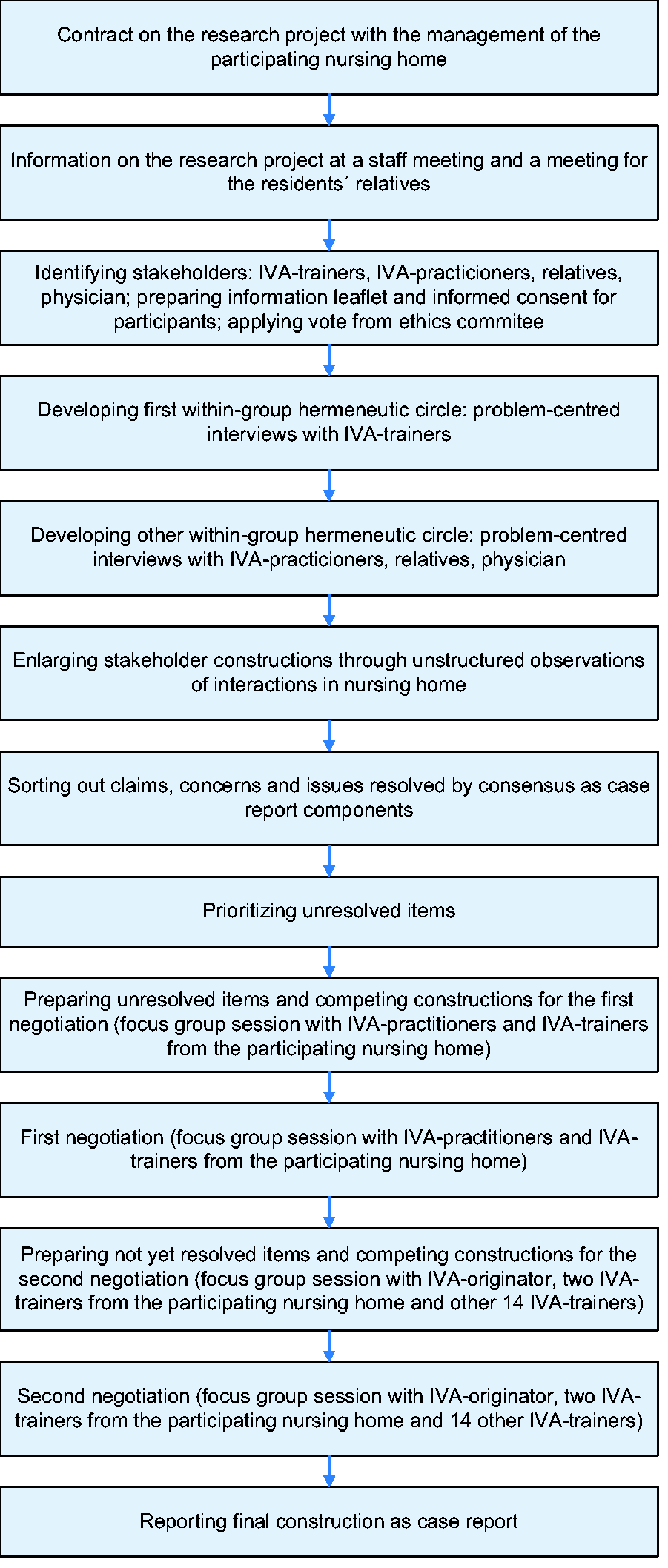
Ethical considerations
Ethical approval was obtained from the ethics committee of Witten/Herdecke University in Germany. All participants received an information leaflet in which the study was described. The first author offered participants the opportunity to ask questions personally. Written informed consent was obtained from all participants. The inclusion of people with dementia and resulting ethical issues is discussed elsewhere (Erdmann & Schnepp, 2013).
Data analysis
Individual interviews and the final group discussion were tape-recorded and transcribed verbatim. Observation data were recorded in writing during observations. Because of technical problems, the group discussion in the nursing home was not tape-recorded, but results were written up in a report (“condensed account”) (Spradley, 1979, p. 75), afterwards. Data were analyzed using qualitative content analysis developed by Mayring (2008) and MAXQDA software (VERBI GmbH, Berlin).
Theoretical framework
Data were interpreted referring to transition theory (Meleis, 2010) and the theory of person-centred care (Kitwood, 2012).
Rigour
Research was regularly discussed with research team peers (“peer-debriefing”) (Flick, 2006, p. 432). Results from qualitative expert interviews and observations were presented to and validated with participants (“member check” Flick, 2006, p. 432).
Findings
In our first research question, we asked with which categories the practice of IVA can be described. From qualitative content analysis, a number of main categories emerged, and the relations between these categories are highlighted in a model of IVA (Figure 2).
Model of Integrative Validation Therapy as a complex intervention (Erdmann, 2013).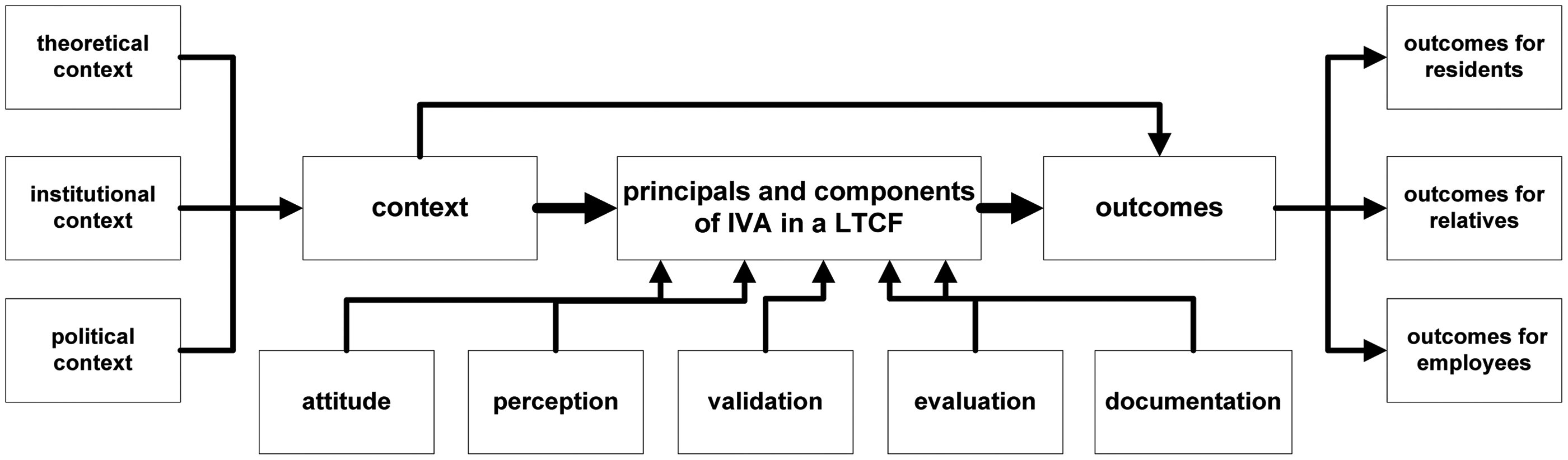
IVA contains a specific attitude toward people with dementia and a few other components of action: perception, validation, evaluation and documentation. As we will see later, the specific attitude and the other components influence each other. In this article, we describe the components, outcomes and the institutional context of IVA in a LTCF.
Attitude
The IVA practitioners’ attitude toward people with dementia encompasses the following cornerstones:
unconditional appreciation of and respect for persons with dementia, acceptance of their subjective reality, search attitude (Suchhaltung), empathy, congruence (genuineness), preparedness for unexpected reactions (flexibility), patience and equanimity.
In our study, unconditional appreciation of and respect for residents were identified in several observed situations. One of these situations was as follows: Mrs. O.:“I don’t really know, how did I come to be here?” Geriatric nurse P.:“I don’t know either, beats me. But I ‘m happy that you are here.” Mrs. O.: “And I’m happy that I’m here” (…) Mrs. O. again: “How is it that I am now here with you?” Geriatric nurse P.:“I don’t know either. Let’s just enjoy it.” Mrs. O.: “I think so, too.” (Observation notes, January 4, 2013, p. 29)
The statements of the geriatric nurse “I’m happy that you are here” and “Let’s just enjoy it” express appreciation for the old lady regardless of the fact that she has dementia. Obviously, this expression of appreciation and respect leads to the well-being of the old lady, because she responses in a positive way with the words: “And I’m happy that I’m here.”
Another interesting principle is the principle of congruence. To be congruent means that spoken words are in line with thoughts and feelings or, as this IVA practitioner says, to give up the temptation of the “therapeutic lie” (Feil & Altman, 2004) and therefore to be honest: Well, I’m absolutely against lying. I am really trying, I mean my feelings and my honest-, well, to react honestly. And if sometimes I’m stumped, I’lI actually say Mrs. So-and-so, it beats me, too, at the moment. I mean I wouldn’t lie. (IVA practitioner interview 7, p. 24)
Unconditional appreciation, respect and congruence are principles which Richard derived from humanistic psychology (Richard, 2010b). They are, beside the principle of empathy, elements in client-centred psychotherapy (Rogers, 2009). The analysis of interview text material indicates that most of the participating IVA-practitioners are aware of humanistic psychology as a theoretical foundation for IVA. Humanistic psychology is part of the institutional philosophy of the investigated nursing home, and this also gives some support to IVA practitioners. Although Richard does not name empathy as a principle of IVA in her publications, IVA practitioners have this principle in their tacit knowledge, as this extract from one interview indicates: I don’t understand validation as encompassing only those three principles but as a basic attitude. Really, this appreciative attitude and to try to understand the other person. And to be responsive to them. (IVA practitioner interview 5, p. 36)
In his early definition dating from 1975, Rogers (1980) describes empathy as follows: The state of empathy, or being empathic, is to perceive the internal frame of reference of another with accuracy and with the emotional components and meanings which pertain thereto as if one were the person, but without ever losing the ‘as if’ condition. Thus it means to sense the hurt or the pleasure of another as he senses it and to perceive the causes thereof as he perceives them (…). (Rogers, 1980, p. 140)
According to this definition, empathy rather results from perception than from an attitude. But Bischoff-Wanner (2002) describes different perspectives of empathy: the cognitive, affective and motivational perspective. In the statement above, the perception of feelings is subsumed under the verb “to try,” but the cognitive perspective of understanding and the motivational perspective of reacting to somebody’s plight are also expressed. Empathy is therefore not only a perception, and the cognitive perspective of understanding is part of the IVA attitude because IVA practitioners must have the intention to understand somebody.
The acceptance of the subjective reality of a person with dementia and the intention not to correct him is another principle which is shown in the following situation, narrated by a relative: Two gentlemen were sitting at my mother’s table. (…) Well, at any rate, he then confused the ladle with his spoon and then claimed the whole bowl for himself. The other gentleman didn’t like that at all and they started a brawl. Yeah, and the one with the giant spoon and, yeah, then people started complaining and there was some wrangling. (…) Well, pulled at the plate somehow and ‘How can one eat like that!’ But then someone arrived real quick and put down another bowl ‘That’s no problem at all, there’s enough food for everyone.’ (…) Problem solved. (Relative interview 1, pp. 106–110)
Instead of correcting the behavior of the resident who was eating from the bowl with the large spoon, the IVA practitioner let him keep doing that and found another solution, which satisfied everyone. By doing this, the IVA practitioner accepted the subjective reality of the resident.
But subjective reality is not always obvious as in the above example. More often IVA practitioners perceive residents’ behavior as unusual, but the reason behind it is unclear. So IVA practitioners need to look for residents’ subjective reality to understand and react using the IVA method. In line with the German psychiatrist Dörner (2013), Richard calls this principle “Suchhaltung” (Richard, 2010b, p. 5) which can be translated as “search attitude.” One IVA practitioner describes this as follows: To hold yourself back because we are at one, yes, we are oriented, always putting ourselves in the resident’s shoes, where is she at right now and fetching her there, that is very demanding. (…) That is challenging work. To realize what is happening right now, where can I get her. (IVA practitioner interview 2, pp. 8, 60)
Another principle of the IVA attitude is the preparedness for unexpected reactions of people with dementia. On the one hand, reactions can be very nice or funny; on the other, they can be insulting and the conversation ends unsatisfactorily for both. The participants argue that IVA practitioners must be prepared for any possible reaction and that requires flexibility.
The last principle of IVA attitude is patience and equanimity. IVA practitioners must not expect the use of IVA techniques in any particular situation to have lasting effects. More often desirable effects will only last a short time, and thus IVA practitioners must have the patience to begin over and over again.
Resembling patience, equanimity is a skill and part of the attitude required in IVA practice. Equanimity is needed when, for example, residents show challenging behavior. The principle of equanimity seems to be contradictory to the technique of verbal and nonverbal mirroring of the persons’ feelings; however, equanimity is needed to find the right words in difficult situations like this one: I experienced that too, someone had raised his hand, he paused, wanted to hit me, he paused at the last moment, is looking at me with big eyes. I said: 'You are very angry and would love to slap me right now’ - 'Yes, but I didn’t’, he said. (IVA practitioner interview 2, p. 72) The residents’ relatives also observe the principle of patience and equanimity with admiration: “Yeah, always calmly I think. Well, never somehow (…) I have never heard a raised voice from any caregiver, not even close. Yeah, always calmly and patiently”. (Relative interview 2, p. 79)
IVA attitude is one prerequisite for validation, perceptive skills are another.
Perception
In the investigated nursing home, perceptive skills encompassed the following:
the collection of biographical data, perception of feelings and motivation, observation of dementia-related symptoms (disorientation, impaired verbal communication, etc.) and behavioral disturbances, recognition of other diseases and symptoms, which can be contraindications for IVA such as schizophrenia and depression (Richard, 2011).
In the investigated nursing home, the collection of biographical data forms part of the nursing assessment before residents move in. The biographies are documented in writing and sometimes with the help of photos in order to obtain an extensive impression of the residents’ lives. This information is useful to understand the behavior of the residents and to validate their life themes.
The perception of current feelings or motivation people with dementia have is one of the most important tasks in IVA practice. Without it, validation of feelings or motivation is impossible. In the interviews with IVA practitioners and IVA trainers, the following motivation were mentioned: sense of order, sense of duty, sense of beauty, diligence, attention, timeliness, accuracy, willingness to help, precision, sociability, plenty of knowledge, sense of responsibility. Perceiving these and other individual motivation and knowing the patients’ biographies, IVA practitioners always have at their disposal a theme enabling them to establish contact with the residents. They can validate those motivation whenever they meet the person or the person manifests these motivation.
Like anyone else, people with dementia have feelings, and the experience of dementia including multiple psychological and physical losses often causes strong feelings. Rogers defines feelings as: “emotionally colored experience, including its personal significance. Feelings and the cognitive content of their significance are recognized in their area of experience” (Rogers, 2009, p. 28; translation by the authors). People with dementia do not have the ability to cope with their feelings in a cognitive way; they are, so to speak, at the mercy of their own feelings. With IVA, the feelings of people with dementia are expressed in spoken words, and this helps patients to cope with them. Stressful, but vocalized feelings become less troubling (Feil, 1999; Richard, 2010b). But before IVA practitioners can vocalize the feelings of a person, they must perceive them, often only inferring them from nonverbal behavior. In our interviews, the following feelings were expressed in connection with IVA, and so we can assume that these feelings are present in the investigated nursing home: sadness, dolefulness, desperation, excitement, anger, neediness, stress, anxiety, need to belong, loneliness, helplessness, uncertainty, exhaustion.
Validation
In practice, the component of validation encompasses principles and techniques of verbal and nonverbal interaction. These are
validating motivation, life themes and feelings with short sentences and nonverbal mirroring, the principle of action before reaction, the technique of a ritualized encounter, avoiding difficult questions, the use of yes and no questions, adjusting one’s voice in volume, tone and pitch to the individual situation, using keywords, generalizing feelings and motivation with proverbs, wise sayings, songs, biblical sayings and sentences with everybody, mirroring the body language of the person, touching the person at acceptable parts of the body (the hand, arm, shoulder), if he/she shows feelings of sadness, insecurity or anxiety, avoiding touching the person, if he/she is very excited or has strong feelings of anger, avoiding incongruent messages, adapting the validation techniques to the individual abilities of the person.
The core factors of IVA are the validation of motivation, life themes and feelings with the help of short sentences and nonverbal mirroring. Richard (2006a) asserts that the validation of motivation and life themes should be done as often as possible before a crisis involving overwhelming feelings occurs. In our interview, one IVA trainer called this the principle of “action before reaction” (IVA trainer interview 1, p. 198). This means the more often motivation and life themes are validated, the less frequently a crisis involving stressful feelings occurs (Richard, 2006b, 2010b).
Biography, motivation and life themes represent a person’s self and, like most other people, people with dementia have the need to express themselves as long as they can. In this context, we refer to Kitwood’s person-centred care. He argues that, besides other needs, people with dementia have the need of identity (Kitwood, 2012). During our observations, we noticed an interaction during morning care, in which a typical life theme of a person was validated: Geriatric nurse P.: “Well, and now you’ll put on the nice hand knitted sweater.” Mrs. O.:“Made from odds and ends”. Geriatric nurse P.:“I wouldn’t have noticed. Every piece is special. You won’t see that anywhere else.” Mrs. O.:“I’ve always loved knitting.” Geriatric nurse P.:“A good knitter. The sweater is really well made.” Mrs. O.: “I must always have something to do. Not just sitting there.” Geriatric nurse P.: “Always busy.” (Observation notes Jan 4, 2013, p. 29)
One technique to validate identity with the help of IVA is the so-called “ritualized encounter” (Richard, 2006b, p. 43). In a ritualized encounter, almost the same short sentences are always used to greet the person, to validate some of his or her life themes and to say goodbye to the person. The ritualized encounter is an opportunity to express appreciation for the individuality of the person. The person with dementia experiences his personality being appreciated.
During one observation, a geriatric nurse gave us an idea of how a ritualized encounter with a person is worked out by the nursing team to be used whenever a member of the team meets the person: 1. Ritualized conversational beginnings Hello Mrs. Winter! Edith Winter. Edith Winter from Cologne. 2. Validating sentences referring to the life theme You know the score. Yes! You see everything. You are very observant. We are clearing up. There is always something to do. 3. Ritualized conversational endings Needs must. Duty calls. Goodbye, Mrs. Winter (Shaking hands as kinesthetic confirmation) (Observation notes Jan 4, 2013)
In addition, IVA practitioners emphasize the importance of using keywords from the person’s biography. In one interview, an IVA practitioner gave an example of the use of typical characteristics of a resident’s hometown (harbor, bridge, name of hometown) as keywords: And I realize how important these words are to her. Now that everything around her is breaking down. Distraught, sometimes crying, weeping because she cannot bear it. And then I say ‘Last Saturday’ just as an example ‘I went shopping in W town at the harbor.’ And I realize W town, she, she becomes, pays attention. ‘I know that area’, she says. Doesn’t talk as much anymore. ‘I know that area.’ Then I say: ‘Yeah, there used to be a really beautiful bridge there, now there is a really modern one.’- ‘Oh?’, she replies.’ (IVA practitioner interview 2, p. 14)
The validation of identity is also possible using the evidence of the “embodied self” (Fuchs et al., 2010). This term is based on the phenomenology of the body described by Merleau-Ponty (1974) (Fuchs, 2010). Several authors (Fuchs, 2010; Kontos, 2003, 2004, 2005) describe the idea that fundamental aspects of self are expressed through the body and call these expressions “embodied selfhood” (Kontos, 2005, p. 556) or “embodied self” (Fuchs, 2010). The “subject body (Leib)” (Fuchs & Schlimme, 2009, pp. 570 f.) is a natural I, a personal character and is dealing with tasks in the world (Uzarewicz & Uzarewicz, 2005). “The intentionality of the subject body” (Merleau-Ponty, 1974, p. 165) can be perceived if people with dementia express parts of their embodied self (Kontos, 2005) by repetitive motions or typical professional behavior. An old floor tiler kneels on the floor and tries to do his former work by rubbing a newspaper against the floor (Vincentz-Verlag, 2007). Kontos and Martin (2013) cite “other examples of embodied selfhood” like “religious practices (…), food preferences (…), and “bodily dispositions that disclose expressions of class distinction” (Kontos & Martin, 2013, p. 291). Kontos argues that the expressivity of the body is preserved, contrary to the cognitive abilities of people with dementia (Kontos, 2003, 2004, 2005). The “habitus” (Bourdieu, 1991, pp. 277 ff.) of a person with dementia can be expressed through the body (Kontos, 2003, 2004, 2005, 2012) and can therefore be validated by IVA. In our interviews, we asked IVA practitioners and IVA trainers about the validation of the embodied self, and we learned that the theoretical underpinnings of the embodied self are unknown. However, our group discussions showed that validation of the embodied self is sometimes unconsciously performed in practice and discussed in IVA lessons as this IVA trainer stated: Or we had a soldier today. That was the same thing with him. There we spoke about this ritualized encounter, too, and we had been thinking how do we take our leave. And that was the case with him, he never shook hands with anybody since he had been a captain. He would never have done that. Instead we would, not in an exaggerated manner, but we would stand up straight, legs together, feet together, and take our leave. (IVA trainer interview 3, p. 49)
In our final group discussion, we discussed this example with Richard and IVA trainers, and they agreed that this technique can form part of IVA.
The interviewed IVA practitioners and trainers are convinced that the more often they validate the motivation of their residents, the less frequently the residents experience a crisis involving overwhelming stressful feelings. However, if residents show stressful feelings, IVA practitioners validate those feelings with short sentences, if necessary with two words only. How long the sentence should be depends on the individual resident’s ability to understand complex sentences: And in that case I find it rather helpful with integrative validation that I can directly relate to her feelings. And sometimes I deviate from these classical, these three factors for example or simply say only individual words. Because sometimes I also have the feeling that, when I say a complete sentence, she doesn’t understand it at all, that she cannot compute it. And when I look at her then and say “completely knackered” or “completely exhausted”, she can understand that and she will then say “Yes, I am.” (IVA practitioner interview 5, p. 2)
This example shows that IVA-practitioners have to adapt their validation to the individual abilities of the person. Our observations also showed that IVA practitioners adjust their voice in volume, tone and pitch to the individual situation.
In contrast to Feil, Richard (2006b, 2011), in her publications, always held the opinion that IVA practitioners must not ask people with dementia questions. Nevertheless, our observations showed that IVA practitioners ask residents short questions. In our ensuing interviews, the IVA-practitioners argued that whether they use questions or not is related to the individual abilities of the residents and that they usually pose simple yes-or-no questions. There seemingly existed a gap between IVA theory and its practical application, and so we confronted the IVA trainer with that contradiction in our final group discussion. Surprisingly, the participants gave up this original position that questions should be avoided at all cost, but they also highlighted that questions can evoke stress and anxiety and should therefore be carefully worded and that they should only be used in the early stage of dementia, when people still have the ability to answer.
Richard (2010b) describes the technique of generalizing feelings and motivation with the help of proverbs, wise sayings, songs and biblical sayings. One of the IVA practitioners explained that the intention behind this technique is to express our understanding of the person, to show that we think as he does. And that is why we use proverbs in validation because they are maxims. And every person has his or her own maxims, (…) but when I can express these maxims, then he feels accepted. He feels understood, he can open up. Because he knows, ah, there is someone who thinks like me. (IVA practitioner interview 6, pp. 156–158)
But there also is another technique which can be used to generalize the feelings and motivation of a person, for example, using sentences containing the word everybody. This technique is explained by one of the IVA trainers in the investigated nursing home and seems to be very useful. When I say for example: ‘That’ll make a person insecure’ then I am saying: ‘It’s not only you. Others in your situation would feel the same.’And that creates a feeling of attachment, the person doesn’t have the feeling why am I the only one feeling insecure, but others would feel the same way. And you get them on board this way (…). (IVA trainer interview 3, p. 8)
The investigation of techniques of nonverbal interaction was more difficult than expected. During our observations, we noticed that it is hard for one observer to simultaneously record verbal and nonverbal expressions. After having decided not to use videography in our observations, we had to accept that we could only get an impression of the situation as a whole. Consequently, we were not able to analyze the nonverbal behavior of the observed IVA practitioners in depth, but we could judge whether the nonverbal behavior was in line with their verbal behavior or not. In the cases we observed, we could not detect any incongruent behavior. And our interviews indicate that the technique of mirroring the body language of a person is well known in practice: Then I have to take a step back for a moment and say, oh, now, how does he feel.“– „So, you are assuming his posture?” – “Of the person concerned, yes. They do usually sit in a hunched position and, or something like that, and then you sit down near them and wait, try to get into their breathing rhythm.” (IVA practitioner interview 1, p. 96–98)
What we frequently saw during our observations was the technique of touching the person at an acceptable part of the body (hand, arm, shoulder). This technique is used not only to establish contact with the person but also when strong feelings of sadness, anxiety or insecurity occur. But the participants also knew that if somebody is very excited or has strong feelings of anger, it is not useful to touch this person because this gesture would rather upset the person.
Evaluation
To evaluate the individual application of IVA, IVA practitioners have the opportunity to present their difficult cases at a special IVA meeting, to which every IVA-practitioner of the nursing home is invited on a monthly basis. At this meeting, team members discuss difficult cases and try to find a solution together when IVA does not work. Sometimes the reasons are insufficient information about a person’s biography or a wrong assessment of the current subjective reality of the person. Other topics, which can be discussed in the meeting, are current feelings and motivation of the person or suitable keywords to use with the individual resident. The meeting is also an opportunity to practice validation techniques.
The application of IVA is also evaluated during interactions by observing the reactions of the resident. The participants report that there is always a risk of failing to perceive and validate a feeling, which the resident does not have, or to perceive and validate a wrong motivation. Even the validation of life themes can be wrong, for example, if a person has forgotten his/her profession because he thinks he/she is an adolescent now. Therefore, IVA practitioners must observe the person’s reaction during validation and correct their validation if necessary.
Documentation
The nursing record of each resident contains his or her biography. In some cases, typical motivation and suitable keywords are documented, frequently feelings or the individual ritualized encounter are included, but this depends on the individual commitment of the different nurses. In our first group discussion at the nursing home, the participants agreed that documenting information useful for IVA is beneficial. But on the other hand, they rejected the obligation to document this information and justified this with lack of time.
Outcomes
From the perspective of the participants, the results of IVA for persons with dementia can be summarized as follows:
an experience of trust, belonging, attachment, perception of own identity, the feeling of the person that somebody understands his or her situation and feelings, the opportunity to derive comfort from somebody, an experience of appreciation, respect, well-being and joy, less behavior disturbances like agitation or aggressive behavior reduced consumption of benzodiazepine and neuroleptics, for example risperidone.
“One of the main objectives of Integrative Validation Therapy is the promotion of self-identity and the feeling of belonging” (Richard, 2010b, p. 8, translation by the first author). From the perspective of the participants, these two goals can be achieved. Indeed the loss of identity caused by dementia is irreversible. And the participants disagree with the hypothesis that identity can be preserved with IVA or that loss of identity can be delayed. But the participants agree with Richard’s argument that IVA restores the residents’ identity “during the moment of the encounter” (Richard, 2010b, p. 8, translation by the first author), and that this moment is valuable because it strengthens their self-esteem.
The IVA practitioners also support the hypothesis that the person with dementia is given a feeling of belonging; moreover, they are convinced that with IVA they can build a trusting relationship with the person. One of the IVA trainers, who often visits different nursing homes, narrated her observation that in nursing homes where IVA is not yet implemented people with dementia do not seem to be well integrated. And in other facilities where they [the residents] are not being perceived, where staff is just quickly running past them calling from afar ‘Hang on a minute, I’ll be right there’ or ‘Why don’t you sit down here for the time being?’, that they really have a look there where they don’t feel anchored. (IVA trainer interview 3, p. 28)
The participants are also convinced that people with dementia feel that there is somebody who understands their situation. This feeling was evident in a situation observed when an old lady got up in the morning and felt bad and could derive comfort from the nurse: Geriatric nurse P. informs Mrs. O. that she is going to elevate the bed and pulls her to the edge of the bed. Mrs. O.’s eyes are still closed. She says: ‘I’m not feeling well today.’ Geriatric nurse P. puts her arm around Mrs. O.’s shoulder. Mrs. O. leans on the nurse’s breast. Geriatric nurse P. stays in this position for a while and says: Every beginning is hard. (Observation notes Jan 4, 2013, p. 27)
In the situation above, the geriatric nurse used the proverb “Every beginning is hard” to show her empathy.
When we asked our participants about the benefits of IVA, they frequently answered that people with dementia experience appreciation, respect, well-being and joy. The IVA effect of well-being and joy was described as lasting only a short moment, but sometimes the IVA practitioners see effects lasting for the duration of a care-giving situation. For all relatives, the effect of well-being is evident: But I’m thinking, it’s simply, you do see that the people are doing well there. And I’ve seen my father at home. He became more and more grouchy. (Relative interview 4, p. 121)
The most impressive outcomes reported by the participants are reduced agitation and consumption of benzodiazepine and neuroleptics, for example risperidone. These outcomes are expressed, for example, in the following statement: Well, I think that this way of dealing with patients relaxes them a lot. We often have the case that we’re supposed to receive new residents who are said to be very difficult, really fixated, sedated, says so in their admission papers. And then they arrive and we are really able to decrease their medication. (…) So I think that this is an indication that validation really, that this method, well, reassures and relaxes patients. (IVA practitioner interview 4, pp. 86–88)
The involved physician acknowledges that also, when IVA is used, people with dementia suffer less from agitation. In addition, he is convinced that in the investigated nursing home where IVA is applied the consumption of benzodiazepine and neuroleptics has decreased. “Well, a lack of validation rather causes a behavior of refusal, makes people more tense, you know. If validation, and that is the goal, right, doesn’t cause people to become agitated so quickly” (…) “And if you have the impression that in that case you need less medication, now regardless of the severity of the illness, what medication is it that you prescribe less?” – “Oh, those are mainly benzodiazepines and neuroleptics.” (Interview with co-operating physician, pp. 57–59)
Although these outcomes are expressed several times by different participants, these assumptions should be investigated in further studies.
But it is not only people with dementia who benefit from IVA, the employees and relatives of the investigated nursing home also experience some advantages. The positive effect for the relatives can be described in a few words: freedom from the responsibility to care for the resident. All interviewed relatives stated that they felt their mother, father or spouse was well cared for in that nursing home: And I really always feel that there she is always, that she is truly in good hands. Really a comforting feeling. Even if I am on holiday like last week, (…). Yeah then, hey, I don’t have to worry. She is fine all the same, even if I am not there on an occasional weekend. (Relative interview 2, p. 121)
From the perspective of the participants, the outcomes for the employees are the following:
less psychological stress, decreased resistance to care and danger of violence in nursing care, improved communication with colleagues and management, employee satisfaction in general.
The interviewed employees of the investigated nursing home perceive IVA as very useful, and they are certain that IVA makes their everyday life much easier. They suppose that, without IVA, dealing with the residents would either be much more difficult or that the residents would receive more sedative medication. And this would lead to the staff having to promote the residents’ mobility to a much larger extent. In addition, the IVA practitioners presume that, without this intervention method, violence between residents and nurses would arise much more easily. One IVA practitioner made another case for IVA: Without IVA, the employees’ psychological stress would be more extensive: And of course that’s somehow psychological strain for me as well, you know. When three or four residents are becoming very agitated. Then I don’t know either to whom should I go first. But if I can reduce this strain a little by using these ritualized encounters, then everyone concerned is feeling better again. (IVA practitioner interview 5, p. 94)
From the perspective of the employees, IVA also has a positive effect on the work environment. Communication with colleagues and management improves.
In summary, the employees at the investigated nursing home are very happy to work there, which is also evident from low employee turnover. Employee satisfaction in general is expressed in this statement: That is why I love working here. That people are not numbers here, but made to feel safe. They have feelings just like you and me and that is very important. (IVA practitioner interview 7, p. 36)
Institutional context
In this case study, the investigated nursing home has some specific characteristics which can exert an important influence on the application of IVA or which in themselves effect the reported outcomes. These characteristics are:
the knowledge and skills of the employees, an organizational culture of appreciation and trust between management and employees, segregative care of people with dementia, the inclusion of other interventions like music and dance therapy, milieu therapy, information and support of the relatives.
All employees, not only the nurses, have the opportunity to participate in a basic IVA training course so that everybody in the nursing home has some basic knowledge. A few practitioners attended an advanced IVA training course. In addition, low employee turnover enables employees with many years of experience to serve as an example to newcomers. Furthermore, the IVA encounter, which is held monthly, provides an opportunity to discuss difficulties relating to the application of IVA. Thus, employees receive some support during their learning process. Moreover, our interviews indicate that management and the head nurse predominantly act showing appreciation for their employees and that they have a trusting work relationship. This creates a pleasant work environment, which also benefits the application of IVA. It also has to be mentioned that the investigated nursing home is specialized in people suffering from dementia and that means that people not suffering from the condition will not be admitted there. This is an advantage because the acceptance of the subjective reality of a person with dementia demands that his deviant behavior not be corrected and this requires a degree of tolerance which cannot be expected from residents without dementia. Moreover, other interventions such as music therapy can also have an effect on the reported outcomes, especially if music therapy and IVA are combined as described by Brinker-Meyendriesch and Erdmann (2011). Finally, the employees care for the relatives of their residents by giving them necessary information about IVA. The relatives have to accept that the subjective reality of the person is not corrected by the employees. This requires tolerance which is sometimes difficult for the relatives. In summary, this special institutional context seems to facilitate the application of IVA.
Discussion
Considering the significance of the different findings, we acknowledge that people with dementia have to cope with multiple changes and losses and that these losses cause strong feelings. People with dementia experience a “transition process” (Chick & Meleis, 1986/2010, p. 33) caused by their illness and their response to that process shows typical patterns, which can be observed in many other transition processes: “disorientation, distress, irritability, anxiety, depression, changes in self-concept, changes in role-performance, changes in self-esteem” (Chick & Meleis, 1986/2010, p. 27). These typical responses require an intervention helping people with dementia to cope with that experience during the transition from leading a largely independent life to life in a nursing home where they are, however, contented and happy with their social relations. Our results provide a strong argument for the assumption that IVA is a beneficial nursing intervention helping to facilitate the transition of people with dementia. IVA practitioners facilitate this process not only because of the acceptance of the subjective reality of the person and their expression of appreciation, congruence and empathy, which helps people with dementia to express their strong feelings, but also because of the validation of motivation and life themes, which encourage a feeling of pride in the accomplishments of a life-time, support self-esteem and restore personal identity. If well-being in general and well-being in interpersonal relationships are indicators of a successful transition process (Schumacher & Meleis, 1994/2010, p. 45), then we can conclude that, from the perspective of all stakeholders in this study, IVA can make a large contribution to that process. The experience of trust and belonging, the feeling that somebody understands the emotions of the person, the possibility to derive comfort from somebody and the experience of appreciation and respect are reported outcomes of IVA, which indicate well-being in interpersonal relationships. Our findings underline the hypothesis that less agitation and, as a consequence, a reduced intake of benzodiazepine and neuroleptics are related to the fact that with IVA the psychological needs of people with dementia can be met, and therefore one of the multiple causes of behavior disturbance (Halek & Bartholomeyczik, 2006, p. 49f; Kolanowski, 1999, p. 8) is eliminated. Since IVA contributes to the fulfillment of typical needs people with dementia have: comfort, attachment, inclusion, identity (Kitwood, 2012), IVA emphasizes person-centred care, which has, as Chenoweth et al. (2009) have demonstrated, a positive influence on agitation. We also support Kitwood’s thesis that a knowledge of details of a person’s life history can help to have their identity restored by others (Kitwood, 2012, p. 84), and we recommend that IVA practitioners be more conscious of the embodied self of a person, which also provides information about their identity (Kontos, 2004, 2005, 2012).
Limitations
An inherent limitation of a Fourth Generation Evaluation study is that findings from a case study cannot be generalized. As we have seen, many institutional and also political variables can affect our findings, so that in other long-term care facilities or other countries with a different health-care system results could deviate from ours. Therefore, a measurement of the institutional context variables should be included in further research on IVA to explain different results from different nursing homes and to evaluate the outcomes. In addition, our observations gave only a rough impression of nonverbal validation techniques, and therefore further research with videography is necessary to describe nonverbal interaction with IVA in depth.
Footnotes
Acknowledgements
We wish to acknowledge all professionals, residents and relatives from the nursing home Haus Schwansen in Rieseby (Germany) who participated in this study and made this research possible. We would also like to thank all IVA trainers, who participated in interviews or group discussions. The authors wish to extend special thanks to Anja and Henry Wright for proofreading and the translation of the respondents’ statements and Johannes Möller from HFH – Hamburger Fern-Hochschule – University of Applied Sciences for his general support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.