
Abstract
Background and aim
Learning about changes in communication of Deaf with dementia (DWD) is important in order to improve services and support DWD and their families. We explored family members’ views on the changes in communication DWD have and the ways communication was adapted due to progression of dementia.
Methods
A qualitative content analysis of thematic interviews that were conducted with eight close family members of DWD.
Results
With decreasing vocabulary and increasing sign-finding difficulties, conversations became poorer, and DWD tended to diverge from the topic. Nonverbal communication became more important as the verbal communication abilities of DWD deteriorated, and the adult children took a more active role by taking initiative and guiding conversations.
Conclusion
DWD seem to go through similar changes in communication as hearing people with dementia. Adult children of DWD need to get used to interpreting and assisting their parent’s communication through different phases of dementia.
Introduction
Dementia, a syndrome consisting of a memory disorder and at least two other cognitive dysfunctions (McKhann et al., 2011), is increasing significantly globally. In 2010, the number of people with dementia (PWD) was 36 million: by the year 2030, the number is expected to double (World Health Organisation & Alzheimer’s Disease International, 2012). Dementia causes remarkable changes in cognitive functions along with communication (McKhann et al., 2011). Linguistic skills deteriorate already in the early phases of dementia, and they tend to do so as dementia aggravates (e.g. Bayles, 1982; Murdoch, Cheney, Wilks, & Boyle, 1987; Pekkala et al., 2013). According to Savundranayagam, Hummert, and Montgomery (2005), dementia is very much a communication disorder. Deficits in communication influence an individual’s ability to create, maintain and enhance close relationships. Deficits in communication along with changes in personhood of PWD have an impact on emotional interactions between the affected people and their close family members (Parker, Young, & Rogers, 2010).
Although Alzheimer’s disease (AD) was first described over a hundred years ago (Alzheimer, 1907) and there is a great body of research on AD, there are only a few studies on Deaf 1 with dementia (DWD) (e.g. Allan, Stapleton, & McLean, 2005; Atkinson et al., 2011; Falchook et al., 2012). For example, no statistics on the numbers of DWD are available globally. However, knowledge about well-being and health of minorities, such as DWD, is essential in order to set up and develop social and other services for them. Additionally, Allan et al. (2005) postulate that DWD perceive that the hearing world does not recognize the experiences and needs of the Deaf due to the lack of a common language. In general, the hearing health care professionals know very little about the Deaf community, sign language and the Deaf culture. Furthermore, lack of knowledge about dementia may cause negligence and can put a stigma on dementia in the Deaf community. Thus, DWD may suffer from social isolation and loneliness in the community.
The aim of this study is to explore how communication of Deaf persons changes during the progression of dementia and how family members adapt their communication with a Deaf individual with dementia. This study concentrates particularly on introducing various observations made by family members on the changes that occur in the communication of DWD and the responsive ways in which their family members adapt their communication and support the communication of the affected individual.
Method
The present study applied a qualitative approach. The data were collected by thematic interviews, and the focus of interest was on the experiences and perceptions family members of DWD have on communication (see also Polit & Beck, 2012). This paper follows the guidelines of the consolidated criteria for reporting qualitative research (COREQ) (Tong, Sainsbury, & Craig, 2007).
Participants
Interviewees were recruited in co-operation with the personnel in the Nursing Homes of the Service Foundation for the Deaf in Finland and with the Services Department of the Finnish Association of the Deaf. The criteria for participation were as follows: (1) family member of DWD, (2) using Finnish/Swedish or Finnish Sign Language (FiSL) and (3) in regular contact with the parent with dementia. Before the interviews, the interviewees were informed about the research and a hand-out was given for further information. The interviewees were also encouraged to ask questions about the research. Eight persons were interviewed, one Deaf and seven hearing daughters of Deaf people. DWD were their mothers (n = 6) and fathers (n = 2), who were over 75 years and had AD (n = 5) or clinical symptoms of dementia (with no diagnosis) (n = 3). The age of the interviewees varied from 29 to 64 years. The interviews were made by the first author who speaks fluent Finnish and FiSL. Thus, no interpreter was needed.
Data collection and analysis
Themes of the interview.
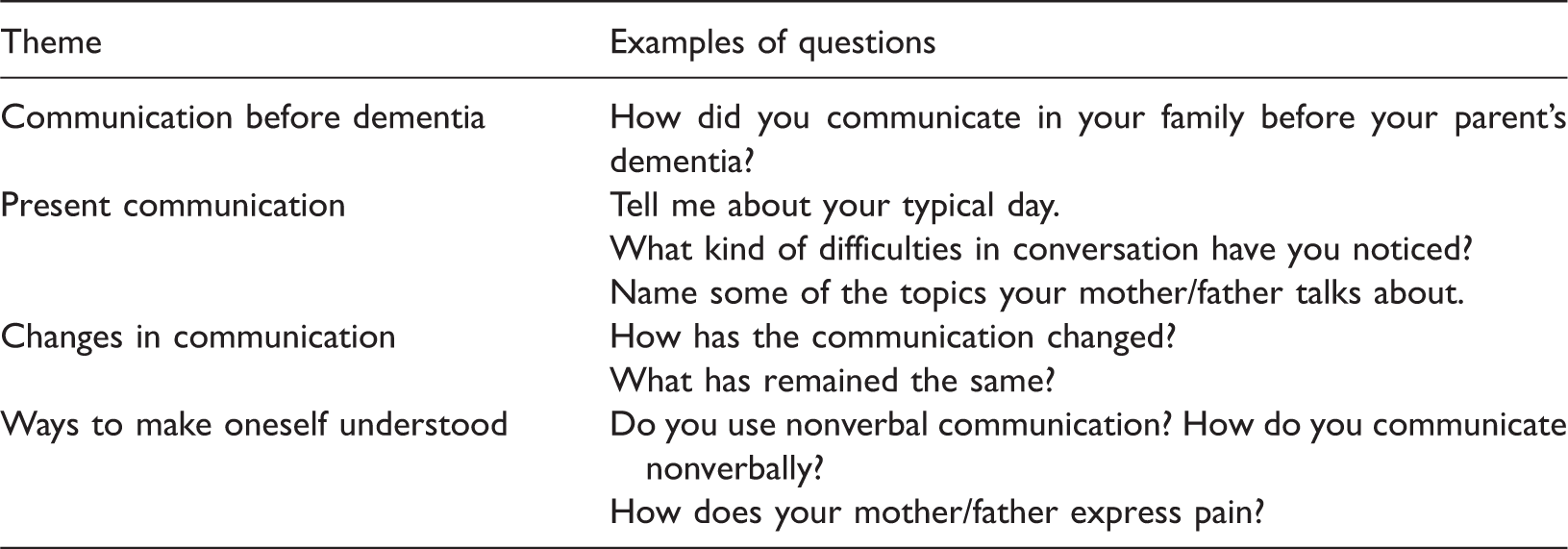
The data were collected between September 2012 and January 2013, and the interviews lasted from 48 minutes to 2 hours 22 minutes, the average duration being 1 hour 13 minutes. The whole data constituted 9 hours and 48 minutes in total. Six out of eight interviews were conducted at the homes of the interviewees; one interview took place at the work place of an interviewee, and one was made in the first author’s house. The interviews took place in a peaceful and comfortable space free from outsiders and interruptions. The interviews made in Finnish (n = 7) were audio-recorded and transcribed verbatim. One interview was made in FiSL, video-recorded, translated and transcribed as text by the first author.
The data analysis followed the process of the inductive content analysis described in Elo and Kyngäs (2008). First, the written material was read through four times, after which the units of analysis (i.e. themes) were selected, e.g. ‘He simply does not understand what I mean’. Second, these themes were simplified, e.g. ‘He does not understand me’, and abstracted into subcategories, e.g. ‘Problems in understanding verbal concepts’. All abstracted themes were collapsed into categories that were similar or dissimilar, e.g. ‘Problems in understanding concepts’, ‘Problems in understanding instructions’ and ‘Problems in being able to participate in animated conversations’. Third, subcategories were grouped under higher order headings, e.g. ‘DWD has problems in understanding’, ‘Family has problems in understanding DWD’ and ‘Other people have problems in understanding DWD’. Finally, four main categories were created: (1) means of communication, (2) interaction, (3) language comprehension and (4) social relationships and communication.
Ethical consideration
This study is a part of a larger project investigating daily interaction of people with AD (called the MIVA-project) commenced in 2011 at the University of Helsinki (Pekkala, Poutiainen, & Virtanen, 2013). The research project has an ethical approval of the Faculty of Behavioural Sciences of the University of Helsinki. The ethical principles of Belmont Report (1979) were followed in this study. The interviewees participated voluntarily, and they were able to stop the interview at any point without explanations. Additionally, each participant signed informed consent before the interview. Both the Deaf and the hearing family members of DWD had equal possibility to attend this study, and the interviews were conducted in the language of their choice. If an interviewee showed emotional reactions during the interview, as recounting experiences can be stressful for participants (Pesonen, Remes, & Isola, 2011), empathy was shown and a short break was taken when necessary.
Results
All DWD, five with AD and three with clinical symptoms of dementia (with no diagnosis), had had dementia for two to 10 years, and they all lived in a nursing home. All but one lived in the Nursing Homes of the Foundation Service for the Deaf in Finland. These nursing homes had signing personnel. One DWD lived independently with her Deaf husband in a communal Nursing Home with non-signing personnel.
Communication before dementia
In order to understand the changes in communication and the means family members and DWD have for making themselves understood, we examined what the communication was like before dementia. All interviewees but one indicated that their Deaf parent with dementia was born Deaf and that he or she went to a school for the deaf. In Finland, as in many other countries, schools for the deaf followed the oralistic tradition from the late 19th century to as late as the 1970s (Salmi & Laakso, 2005). The oralistic tradition meant that teaching in schools for the deaf was performed by speech and lip-reading was emphasized. Additionally, no use of sign language was allowed, and the deaf children were physically punished when they were caught using it. As a result of this, even today many elderly Deaf strongly feel that it is not acceptable to sign with hearing people. However, it is very typical in Finland that Deaf over 75 years of age use multiple means of communicating depending on the person they socialize with. When they socialize with hearing people outside the Deaf community, speech and lip-reading along with writing and mime are used, and when they are in contact with other Deaf, FiSL is used.
Consequently, four of the interviewees reported their parent had not signed to them when they were children. The parent had mainly used speech, and the children had spoken to their parent using clear mouth movements. DWD used speech, lip-reading or writing when communicating within the hearing community and their hearing relatives. Speaking to unfamiliar hearing people was not found comfortable. The interviewees reported that in a case where both of their parents were Deaf, FiSL was used with the Deaf spouse and in the Deaf community. This way also those children, whose parents avoided signing to them, were able to learn FiSL.
Because of different means of communication, the interviewees had already experienced communication problems with their parent in their childhood, as well as later in their lives. Communication was not profound, and there were often problems with understanding each other. The messages their parent conveyed were simple and concrete, and the topics of conversation consisted mainly of practical everyday issues. The problems in language comprehension were likely to cause frequent misunderstandings and unawareness of whether the message had been understood. The interviewees said they had had a habit of repeating things several times to ensure their parent understood them properly.
Changes in communication
The interviewees expressed themselves as devoted daughters and explained that they had experienced sadness and apprehension when facing the fact that their parent had fallen ill with dementia, an incurable and progressive illness. Not being able to communicate the same way they used to before dementia made the interviewees feel sad and helpless. They also felt irritated and annoyed having to repeat answers to the questions DWD made over and over again. The interviewees also shared delightful moments of joy when communicating with their parent. I felt really sad when I could not ask him whether he had been on a trip or had he enjoyed himself during the week. (Participant 2) I became worried when she bought the same things over and over again, because when in a shop, she did not remember if she already had that thing at home or not. For example, she had several packs of washing powder in her cupboard. And when she did not know how to use the washing machine, I got scared. (Participant 5) He still has his sense of humour. Every time I go there, he makes a funny comment on someone's appearance or clothes or on our children. (Participant 6) The main categories and features of changes in communication in DWD. DWD: Deaf with dementia; FiSL: Finnish Sign Language.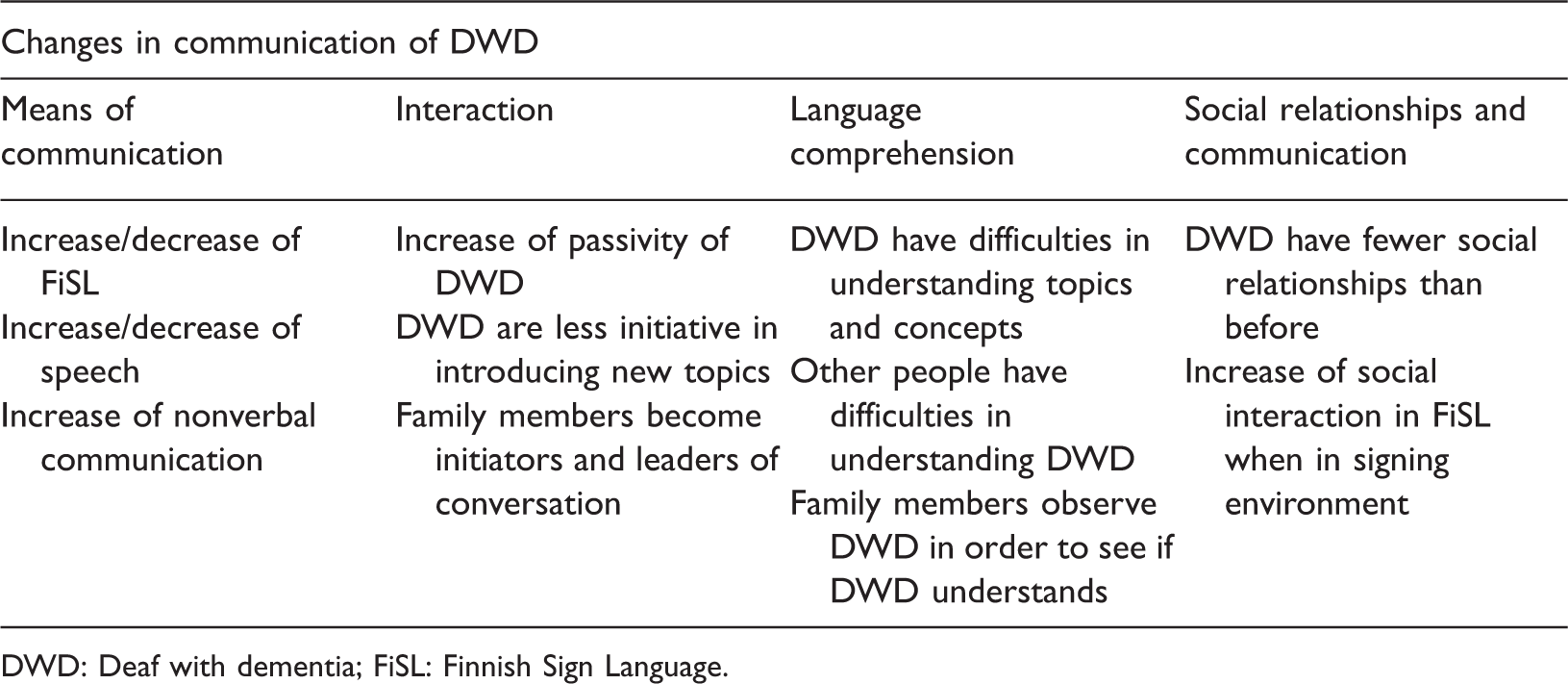
First, DWD continued to use speech and lip-reading with hearing people and FiSL with Deaf friends and other members of the Deaf community as the means of communication after falling ill with dementia. However, there was a change in the amount of speech they produced: when conversing with their close family members, some DWD produced more speech, while others tended to use less speech than before. Samples of the interviews are provided to show the changes in communication of DWD. Somehow I feel or at least I do not remember that my mother had spoken to me so much, I mean used speech. (Participant 1) When he was younger, he used speech very much, and signs too, of course, but now he does not really speak, I mean, he mainly signs. (Participant 2) My mother has always liked to have company and even now she always mingles with the others [in the Nursing Home for the Deaf]. (Participant 7) Now that she lives in the Nursing Home for the Deaf, I think it is good, because she is safe and will not get lost [outdoors]. (Participant 8) And that’s why I nowadays visit her at dinner time, as I feed her, and she’s like mine then, and at least we [communicate] in some way. (Participant 3)
Changes in communication were observed as a decrease of interaction and an increase of passivity. The initiatives of DWD decreased. They did not respond to questions nor did they spontaneously share things they had done during the day unless they were asked to do so by the family members. When meeting someone, DWD did not make the first move to greet them. There was a lot of variation in the communication abilities of DWD, as sometimes they were able to ask for something or they answered the questions, but their story telling or event description was poor. The data showed that both speech and signing of DWD decreased compared to the time before dementia. The changes in FiSL were in the form of changed and forgotten signs: Every day he would come and ask the same thing, and then some signs in FiSL changed, if he needed something like a ‘key’, he would sign ‘shoes’, and all the signs were mixed up. (Participant 2) These events from her childhood interfered with all the stories, and then she would all of a sudden (claps her hands together) return to the original topic and continue with it. (Participant 4) These younger nurses in the Nursing Home are not experts in FiSL and they do not have the knowledge of the Deaf culture, so they do not have the knowhow to deal with DWD and how to lead conversations in a way that they would not end up in conflicts. (Participant 6) My mother’s [hearing] sister was visiting her and they had a sign language interpreter there, but the interpreter did not understand my mother because she uses older signs. (Participant 7) Once, when my mother was still taking care of my father, they went to see a doctor with a sign language interpreter. But my father did not understand what the interpreter was signing and so my mother had to interpret it to him. (Participant 6)
According to the interviewees’ observations, DWD had fewer social relationships than before. It was common that DWD had felt lonely and socially withdrawn even before dementia. Moving to a Nursing Home for Deaf, on the contrary, increased their social interaction in FiSL. The need to use a sign language interpreter decreased, as did contacts with hearing relatives when living in a Nursing Home. Diminishing social relationships were also partly due to the deaths of aging friends and relatives of DWD. Visits made by a volunteer worker (e.g. organized by the Service Foundation for the Deaf in Finland), even when using FiSL, were not helpful in easing feelings of loneliness, because DWD felt the volunteer worker was a stranger.
Generally, DWD continued to use the same means of communication in their relationships as before. They used FiSL outside the family with Deaf friends and with the personnel and other Deaf residents in the Nursing Home for the Deaf. Communication in speech continued with the hearing family members, hearing relatives and other hearing people. Other means of communication were also used, such as pointing with a finger, demonstrating, drawing pictures and using self-made signs. It was often the adult children or the personnel in the Nursing Home who helped interpreting the communication of DWD with their hearing relatives.
Ways of making one understood
The interviewees reported that they used several ways to help their parent understand them. First, they helped DWD by repeating, explaining and modifying their own utterances to make their parent understand their messages. Second, the interviewees took responsibility for the interaction with DWD by being an active partner in conversation: they gave clues to their parent, guided the interaction and told about the events their parent had attended when they were not recalled by the parent.
Nonverbal communication became more important during the progression of dementia. Both positive and negative feelings were expressed nonverbally by crying or laughing, and pain and discomfort were shown by facial expressions and gestures. Equally, the interviewees reported that they carefully observed the environment and the nonverbal communication of DWD in order to prevent problems and conflicts from arising. One interviewee used touching as a means to communicate, because her mother was no longer able to communicate. As an example of her nonverbal means of communication, she always hugged her mother when entering and leaving the room, stroked her cheeks and hands and touched her arm as a sign of goodbye.
Summary of findings
The means of communication of DWD consisted of FiSL, speech and nonverbal communication. Both FiSL and speech decreased gradually and even ceased in advanced dementia. However, it was possible that in a stimulating environment, the amount of FiSL increased. Communication of DWD changed both in content and linguistic form. The topics of conversations involved everyday life topics and stories about the past events and childhood memories. Moreover, the verbal expressions of DWD were characterized by the loss of the gist of a story and the inconsistency of stories. A prominent change in communication was difficulties in language comprehension. This concerned all partners in conversation. Interaction changed in a way that contact making and moving on in conversation became more difficult than before. DWD showed less initiative in introducing new topics; they would suddenly change the topic and were not always responsive to what had been said to them. The poorer expressive communication and the problems in language comprehension had an impact on the process and quality of interaction. The role of the family members in conversation changed so that they became initiators and leaders of conversation. They reported that they modified their own communication making it simpler and clearer by signing slowly and using more repetitions than before. They also tended to pay a lot of attention to the situation and anticipate how the conversation would proceed. Additionally, they used nonverbal communication such as touching, exaggerated facial expressions and gestures more often than before.
Discussion and conclusion
Changes in communication of PWD increase their behaviour problems and the burden of the close family members (Parker et al., 2010; Savundranayagam et al., 2005). The participants in our study had experienced sadness and anxiety when their parent had fallen ill with dementia and when they were not able to communicate the same way they had before dementia. As the data in our study indicate, it is important for the close family members to recognize their feelings and the impact dementia has on their interaction with their loved one with dementia. The burden family members feel due to the breakdown of communication, as well as their needs of social support, should be examined in future research.
All participants in this study reported that communication of DWD changed in several ways. Our data showed that DWD repeated questions the same way hearing people do (Purves & Phinney, 2012/2013) and DWD had sign-finding failures (Hake & Farlow, 2006) similar to the word-finding failures found among hearing PWD (e.g. Bayles, 1982; Murdoch et al., 1987; Pekkala et al., 2013). All these impairments can hamper the flow of conversation (Hays, Niven, Godfrey, & Linscott, 2004). Furthermore, initiative to introduce new topics in conversation decreased and passivity in conversation increased overall as found in studies of Hays et al. (2004) and Parker et al. (2010). The result is in line with the earlier research on DWD (Falchook et al., 2012; Hake & Farlow, 2006).
Our study revealed that communication of DWD became poorer along with the diminishing vocabulary, a finding corroborating that of Hays et al. (2004; see also Purves & Phinney, 2012/2013). Furthermore, our study lends support to other studies showing that difficulties in language comprehension increased (Hake & Farlow, 2006; Pekkala, Kangas-Lumme, & Rainò, 2013; Wong, Anand, Chapman, Rackley, & Zientz, 2009). DWD in our study had difficulties in understanding concepts, instructions, explanations and the effects of their own behaviour. Parker et al. (2010) and Purves and Phinney (2012/2013) have noted that it is hard for the PWD to follow lively conversations. Similarly in our study, taking part in lively conversations became difficult for DWD.
Our study supports the finding of Falchook et al. (2012) that it was difficult for other people to understand DWD because DWD answered questions in an inappropriate way, as also shown in Hake and Farlow (2006) and Parker et al. (2010). The communication abilities seemed to weaken along with the progression of dementia, and, in some cases, resulting in a total lack of communication. It is possible that any linguistic execution of DWD decreases due to advancing dementia and stiffness in hands, which makes the formation of signs difficult. Sometimes, however, it is possible that DWD use speech even when they have not used any language for a long time.
The communication problems concerning the sign language interpreters and younger nurses in our study are similar to those reported by Allan et al. (2005). Limited knowledge of Deafness and proficiency in FiSL can lead to misunderstandings and conflicts. It is crucial, particularly with DWD, that the sign language interpreters and nurses are native signers who have knowledge of dementia and who know how to communicate effectively with DWD.
This study showed that when interacting with DWD, the role of family members as the promoter and guide of communication becomes very important, in a way similar to communicating with hearing PWD (Jootun & McGhee, 2011; Wilson, Rochon, Mihailidis, & Leonard, 2012). First, the interviewees took initiative in interaction and shaped the content and the form of messages to make them more easily understood for DWD, a finding corroborating that of Purves and Phinney (2012/2013). Second, they reported that they had adopted their own communication and made it simpler and clearer for the affected individual to understand by signing slowly and repeating their messages when necessary. Finally, they also paid careful attention to the situation and anticipated the course of the conversation to maintain their parent’s ability to participate in conversation.
Furthermore, our study showed that it is essential to use multiple means of communication in order to support communication of DWD. The result is in line with the finding of promoting communication of hearing PWD in Wong et al. (2009). Our study indicated that the signing environment helped DWD to revive and improve their FiSL. The finding corroborates the study of Parker et al. (2010) who revealed that linguistic stimulation supports the communication of DWD.
The interviewees indicated that they often interpreted communication of DWD based on the behaviour of their parent, which is in line with the earlier research on hearing PWD (Keady & Jones, 2010). It was also shown that family members understand PWD because they know their biography and things they like and dislike (see also Polk, 2005). When communicating with PWD, family members use this biographical knowledge and change the subject or use other distractions to avoid conflicts in communication.
When verbal communication is very limited, particular attention should be paid to nonverbal clues and specific behaviour of DWD in expressing, for example, pain, the expression of which is often underestimated (Cunningham, McClean, & Kelly, 2010). The interviewees reported that they used more nonverbal communication, such as touching, when adjusting their own communication with DWD. Additionally, they carefully observed the behaviour of DWD and interpreted their facial expressions to be able to respond to their communication initiatives. Nonverbal communication is an important way of expressing oneself in advanced dementia. Touching seems to be the last way to communicate with DWD when dementia progresses to the phase in which verbal communication is no longer possible. Our study showed that family members of DWD used comforting speech with an expressive touch, which has been demonstrated to have a soothing effect on individuals with dementia (Kim & Buschmann, 1999). Finally, it seems that in a stimulating environment, DWD use more signs and gestures than before dementia. As dementia aggravates, DWD tend to express themselves nonverbally. Therefore, the use of multiple means of communication and the role of environments with communication expertise, such as Nursing Homes for the Deaf, are worth investing in the future.
Strengths and limitations
The present study makes an internationally unique contribution by producing scientific knowledge on communication of DWD. Additionally, this study may be one of the first studies dealing with Children of Deaf Adults (CODA). Very little research has been conducted on this minority within a minority, even though the needs and unique experiences of CODA are largely unknown. Coming from the CODA minority herself, the first author of the paper shares common grounds with the interviewees, which is likely to have helped the authors to understand and interpret the interviewees’ descriptions of Deaf culture and the experiences of CODA.
The reliability of this study was evaluated in the light of credibility, dependability, confirmability and transferability (Lincoln & Guba, 1985). The credibility of this study was secured by making two pilot interviews. Dependability was reached by collecting the data within a reasonable time, five months. In order to control for the confirmability of this study, the recruitment of the interviewees, the themes of the interview, as well as the process of analysis were reported in detail. Finally, the transferability of this study is attempted by a thorough report of the research process and by the presentation of findings with quotations.
This study has some limitations that need to be taken into account when drawing conclusions. Although the sample of participants was quite small (N = 8), the interviewees described their experiences and observations confidentially and in detail (the average duration of an interview was 1 hour 13 minutes), which increases the reliability of this study. However, all the participants were female, so the findings may be biased and remain overemphasized without male participants, the role of whom as communication partners needs to be taken into account in future research. As far as Finland is concerned, adult daughters are probably more involved in their parent’s live than adult sons, as all the interviewees reported they had been interpreters for their parent and helped them in various ways even before dementia.
Implications for future research and for the care of DWD
As reported by the interviewees, the social network of DWD had declined but was maintained in the Nursing Homes for Deaf. For this reason, more research is needed on the social network of DWD and on social support of DWD and their family members. In the future, it would also be useful to investigate communication rehabilitation on DWD, because it is very seldom that Deaf people with a neurological disease have an opportunity to attend speech and language therapy (Marshall, Atkinson, Thacker, & Woll, 2003). Evidence of the effects of speech and language therapy were presented by Feyereisen, Berrewaerts, and Hupet (2007) who found that practical exercises done with another person increased the word production of PWD and that repetition of communicative exercises were beneficial for them.
This study showed that knowing the life story of DWD is crucial to understanding a Deaf individual with dementia. Therefore, co-operation with the family members of DWD is essential. This study also showed that the care of DWD in an environment in which sign language is used promotes communication skills of DWD. Our finding implies that the care personnel should be educated in dementia in DWD and the Deaf culture in general. The ideal would be that there were more native signers among health care professionals to create a fluent signing environment for DWD. Equally, knowledge about language and culture is the key element for understanding minorities with dementia (Hanssen, 2013) and DWD in particular (Parker et al., 2010). Finally, as indicated in this study, it needs to be emphasized that a common language in a family is important.
Conclusion
This study aimed to illuminate the reflections of family members on the changes in communication of DWD. To conclude, DWD undergo similar linguistic and communicative degradation as hearing PWD. DWD tend to forget signs and have difficulties in understanding language and in following conversations. They lose the gist of stories, become passive in interaction and express their feelings and needs nonverbally. The family members explain, repeat and sign calmly, as well as interpret the behaviour of DWD. The importance of nonverbal communication grows as dementia progresses.
Footnotes
Acknowledgements
We would like to thank the family members of Deaf with Dementia who participated in this study. We would also like to thank the personnel at the Nursing Homes of the Service Foundation for the Deaf in Finland and the Services Department of the Finnish Association of the Deaf for their help with recruitment of the interviewees. We would like to express our gratitude to the Service Foundation for the Deaf in Finland for supplying the funding required to complete the interviews. Finally, we would like to thank Professor Emerita Arja Isola and M. A. Ira Virtanen for their valuable comments on the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Service Foundation for the Deaf in Finland in the form of travel expenses during the data collection. The views expressed in this publication are those of the authors and not necessarily those of the Service Foundation for the Deaf in Finland.