
Abstract
Does current music therapy practice address the goals encapsulated in the UK Department of Health document, Living well with dementia: a national dementia strategy (the Dementia Strategy) published in 2009? A survey elicited the views of clients, family members, music therapists, care home staff and care home managers, about this question by focusing on the relationship between music therapy and the 17 objectives outlined in the Dementia Strategy. The results showed that the objectives that are related to direct activity of the music therapists (such as care and understanding of the condition) were seen as most fulfilled by music therapy, while those regarding practicalities (such as living within the community) were seen as least fulfilled. Although the responses from the four groups of participants were similar, differences for some questions suggest that people's direct experience of music therapy influences their views. This study suggests that many aspects of the Dementia Strategy are already seen as being achieved. The findings suggest that developments of both music therapy practices and government strategies on dementia care may benefit from being mutually informed.
Introduction
Living well with dementia: a national dementia strategy (the Dementia Strategy) was initially launched in 2007 1 by the Department of Health, UK in order to improve ‘the quality of services provided to people with dementia … [and to] promote a greater understanding of the causes and consequences of dementia’ (Department of Health, 2009, p. 9). The Dementia Strategy was a response to the increased number of people affected by dementia in the UK and to the limited care provision for dementia sufferers and their families. The Dementia Strategy set out to transform dementia services by maximising public awareness of dementia, achieving earlier diagnosis and ensuring high-quality treatment throughout the various stages of the condition.
Music therapy has a long history of contributing to the standard and quality of care provision in the dementia care sector (Aldridge, 2000). Music therapists have worked in dementia care settings with people at different stages of the condition, and there is some evidence of the range of the impact of music therapy on dementia sufferers and on wider dementia care settings (Vink, Birk, Bruinsma, & Scholten, 2004). Indeed, the Dementia Strategy acknowledges that music therapy, as well as other arts therapies, ‘may have a useful role in enabling a good-quality social environment and the possibility for self-expression where the individuality of the residents is respected’ (Department of Health, 2009, p. 58).
This study focuses on the extent to which music therapy practice is seen to contribute towards the aims encapsulated within the Dementia Strategy. As practitioners, we directly experience the focused and committed engagement of residents and staff in music therapy sessions, and our recent study suggests that music therapy's ripple effect reaches beyond the time and physical confines of the music therapy session, through a ‘musicalising’ of the entire social ecology of the residential care setting (Pavlicevic et al., 2015). As practitioner-researchers, we have long grappled with the methodological complexities of carrying out research that is both representative of a music-based practice and that speaks to the demands for evidence from funding bodies and commissioners. It seems that, like many arts-based practices, music therapy risks remaining at the mercy of studies that look at impact and effect while ignoring the practice itself. At the other extreme, studies that focus on the practice remain puzzling and less relevant to the demands for evidence. For this study we forayed into different territory: that of ‘testing’ music therapy against government policy – and found that there has not been any investigation of the perceived extent to which music therapy adheres to the goals encapsulated in the Dementia Strategy. Moreover, since dementia is highly topical in contemporary UK society, we were curious to gauge the extent to which music therapists themselves were familiar with the Dementia Strategy.
Aim
To assess the extent to which the music therapy profession is seen to contribute towards the aims of the Dementia Strategy by conducting a survey with a targeted group of people who were selected due to their personal or professional connection to people living with dementia.
Preparatory analysis of Dementia Strategy objectives
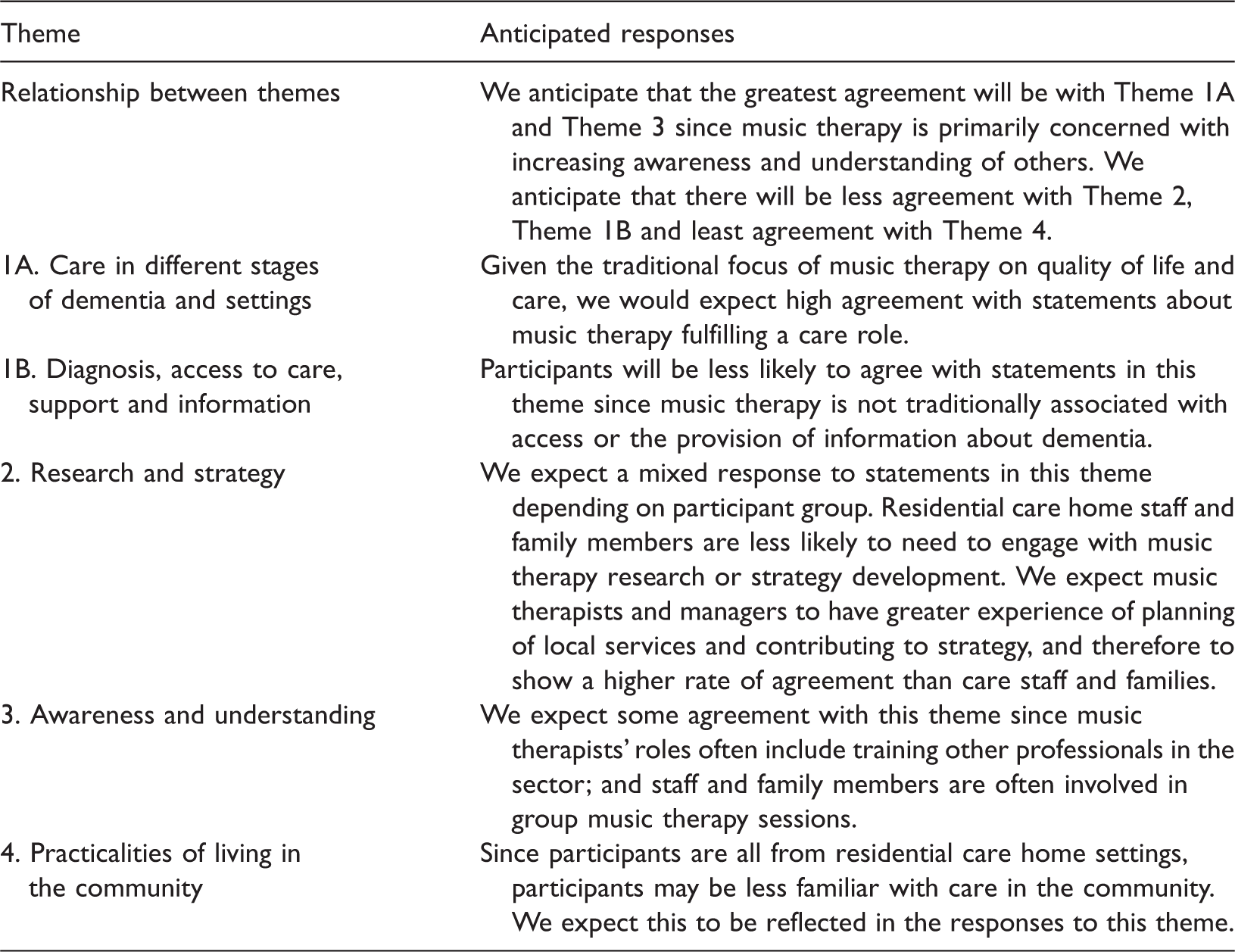
We were concerned that the dense wording and presentation of the original Dementia Strategy document would render the document inaccessible to those less familiar with policy or strategy documents, so we conducted a preliminary analysis and a consequent reconfiguration of the Dementia Strategy's 17 objectives. This resulted in a clustering of the objectives into four broad themes (see Appendix 1). 2 We hoped that this would enable participants to directly engage with our specific task and purpose. Below we present our four themes, and add a brief commentary from the perspective of music therapy.
Theme 1: Care and pathways to care
The Care and pathways to care objectives were clustered into two subthemes: (1A) care in different stages of dementia and settings such as care homes or hospitals (Objectives 8, 9, 11 and 12; Appendix 2); and (1B) diagnosis, access to care, support, and information (Objectives 2, 3 and 4; Appendix 2). The anticipated responses to these two areas are discussed separately in the following analysis.
Theme 1A: Care in different stages of dementia and settings
The Dementia Strategy describes care for individuals throughout three stages of the condition: at and immediately following diagnosis, end-of-life care, and the ‘intermediate’ stages. Studies have explored the effects of music therapy for a number of outcomes that fall within the care theme; including cognition, emotional well-being, memories (Greenyer, 2003), and social behaviours (Vink, Birks, Bruinsma, & Scholten, 2003), as well as ‘problematic behaviours’ (for example, wandering or agitation; Ledger & Baker, 2007), and abilities to participate in music making (Bannan & Montgomery-Smith, 2008). These studies have included participants from different stages of the condition and in different settings, but not one has explored the role of music therapy across all stages. In addition, Powell has found that through participation in music therapy family members and care staff become aware of the ways music therapists perceive and interact with persons with dementia. This may in turn affect they ways they interact with the residents around them. Taken together, these studies suggest that music therapy contributes to the Dementia Strategy's objectives related to care a) through directly improving quality of care, and b) through staff changing the way that they perceive and care for residents in care home settings.
Theme 1B: Diagnosis, access to care, support and information
One objective in the Dementia Strategy highlights the needs of carers, which relates closely to the Department of Health's A national strategy for carers (1999) (objective 7; Appendix 2). There are fewer reports on the role of music therapy in enabling access to care, although there is an indication that music therapy sometimes has this function. A study by Clair, Tebb and Bernstein found that carers saw music therapy as giving them an opportunity ‘to learn about new resources that could be used to enhance their relationship with their spouse’ (Clair, Tebb, & Bernstein, 1993 as described in Aldridge (2000, p. 52)). Music therapists are not generally involved in diagnosis, in enabling access to support or care, or providing information about dementia about the condition or available services. There are reports concerning the psychological support music therapy can provide family carers, who often suffer high levels of depression and physical illness, and can have a diminished quality of life (Clair et al., 1993 as described in Aldridge (2000, p. 52)).
Theme 2: Research and strategy
The Dementia Strategy highlights a need for clear understanding of dementia and the ways in which its sufferers can be cared for. Our second theme includes the objective related to research (objective 16; Appendix 2) and objectives related to strategic national and regional planning (objectives 14, 15 and 17; Appendix 2).
Theme 3: Awareness and understanding
Two objectives are related to increasing awareness and understanding of the condition by staff, people with dementia and the public (objectives 1 and 13; Appendix 2). The Dementia Strategy identifies problems with support and treatment for persons living with dementia. This is largely attributed to a lack of understanding and a social stigma associated with the condition, which “creates an environment in which both the public and non-specialist professionals find it hard to talk about … the possibility of an individual being affected.. [and results] in low priority being accorded to the development of the skills needed to identify and care for people with dementia” (Department of Health, 2009, p. 25). In addition, the “widespread mis-attribution of symptoms to ‘old age’, results in an unwillingness to seek or offer help” and there is “a false view that there is little or nothing that can be done to assist people with dementia and their carers” (Department of Health, 2009, p. 25).
Aspects of awareness and understanding of the condition can come from general interaction with individuals with dementia. Since music therapy provides a way of communicating with sufferers when other avenues are no longer possible (Brotons, 2000), it is now thought to have influence beyond the individual client (Pavlicevic et al., 2015); as mentioned above, through direct engagement with music therapy, the family members (FMs) and care staff become aware of the ways music therapists perceive and interact with persons with dementia (Powell, 2006).
Theme 4: Practicalities of living in the community
Objectives related to independent living and inclusion of people with dementia and their carers in the planning of local services and support services at home were clustered under the theme Practicalities of living in the community (objectives 5, 6 and 10; Appendix 2).
Two-thirds of people with dementia live in their own homes in the community, usually in early or very late stages of the illness (Department of Health, 2009). Apart from family members or friends, who provide the majority of care and support, home care is probably the most important service for supporting people with dementia in their own homes. Good-quality, flexible home care services contribute significantly to maintaining people's independence, reducing social isolation, preventing admissions to care homes and hospitals, and supporting carers (CSCI, 2006). Emerging research indicates that there are considerable benefits to both people with dementia and their carers from specialist dementia home care when compared with standard home care services. Improved outcomes include reduced stress and risk of crises for carers, and extended capacity for independent living for people with dementia (Department of Health, 2009; Rothera et al., 2007).
Since music therapy provision seems to be primarily in care homes, there are few reports about music therapy that might resonate directly with the objectives in this theme. However, one study (Claire et al., 1993) reports on the availability of music therapy to dementia sufferers and their carers living at home.
****
Anticipated responses to survey.
Methods
Range and profile of participants
Given that people's different roles and tasks within residential care homes might lead to different perspectives on and experiences of music therapy, we included participants from as many subgroups as possible who live, work or are associated with the care homes: (1) family members (FMs) of clients, (2) music therapists (MTs), (3) care home staff (staff) and (4) care home managers (managers). We anticipated that staff and FMs would engage with the survey from their experiences of accompanying clients to music therapy throughout the onset and progression of the illness.
Survey participants
The survey was distributed to 108 participants from four different participant groups (clients' FMs, MTs, staff and managers). All participants work at Barchester care homes or visit FMs or friends living there. 3 All of the MTs in this study are Nordoff Robbins MTs. 4
All participants took part voluntarily and consented to the use of the data they provided. Managers and MTs were emailed directly and asked to complete an electronic questionnaire, whereas FMs and staff were asked to participate by the MT in each care home by completing hard copies of the questionnaire. 5
Seventy-one completed questionnaires were returned (68%). Fourteen FMs of people living with dementia, nine MTs, 33 staff and 15 managers completed questionnaires. 6 The Nordoff Robbins and Barchester Healthcare Research Ethics Committees granted ethical approval for the study.
Preparing for data collection
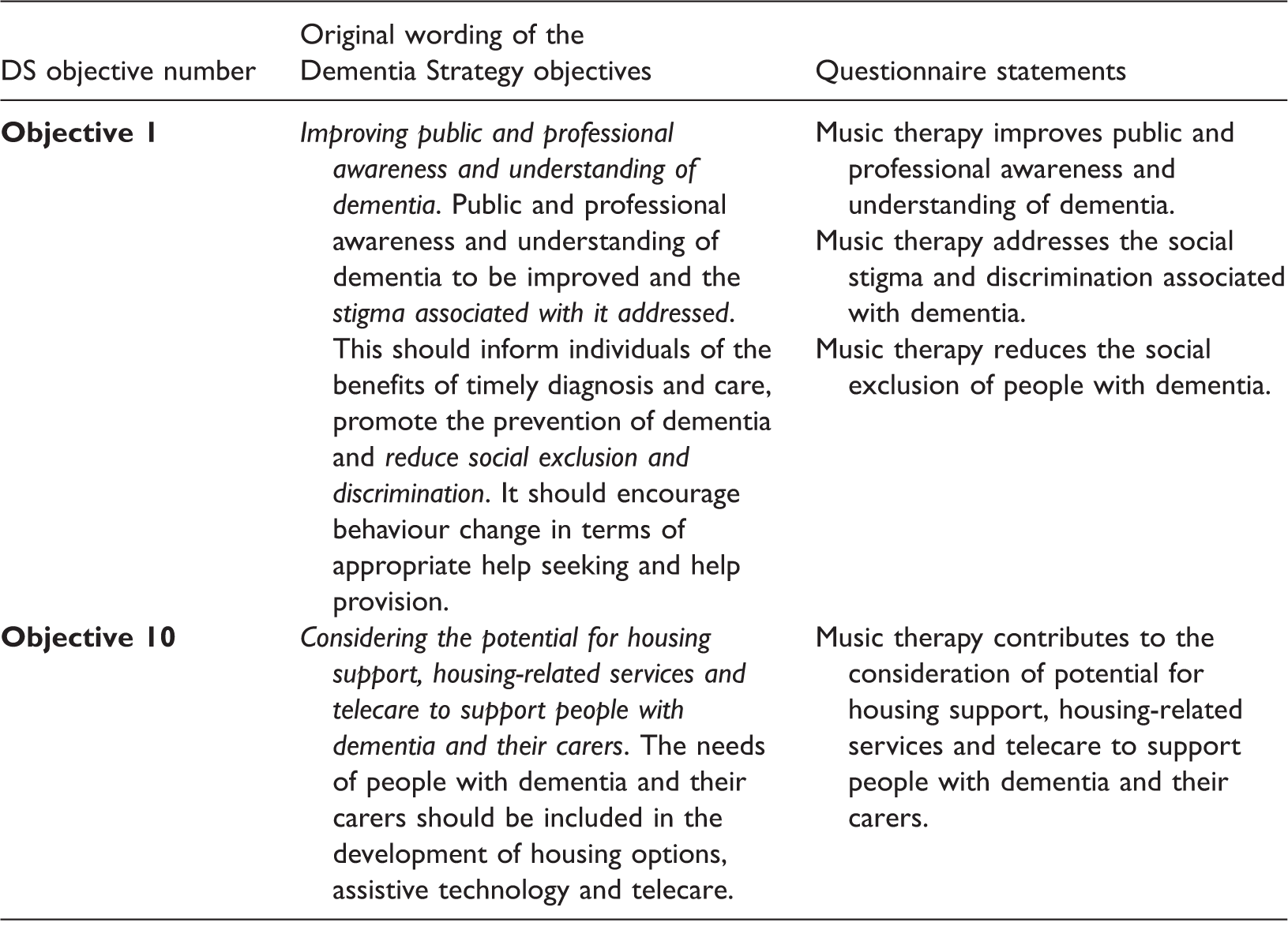
Conversion of Dementia Strategy objectives 1 and 10 to questionnaire statements.
For each of the 30 statements, participants were asked to indicate whether they strongly agree, agree, disagree, strongly disagree or don't know.
The first survey focussed on the Dementia Strategy, and the second collected information about the participants, including their familiarity with the Dementia Strategy, their familiarity with music therapy, and, where appropriate, the settings in which they have worked. This questionnaire design was piloted by two experienced MTs who then provided feedback that contributed to revisions in the layout and structure of the questionnaire. 7
Results
Distribution of familiarity with the Dementia Strategy
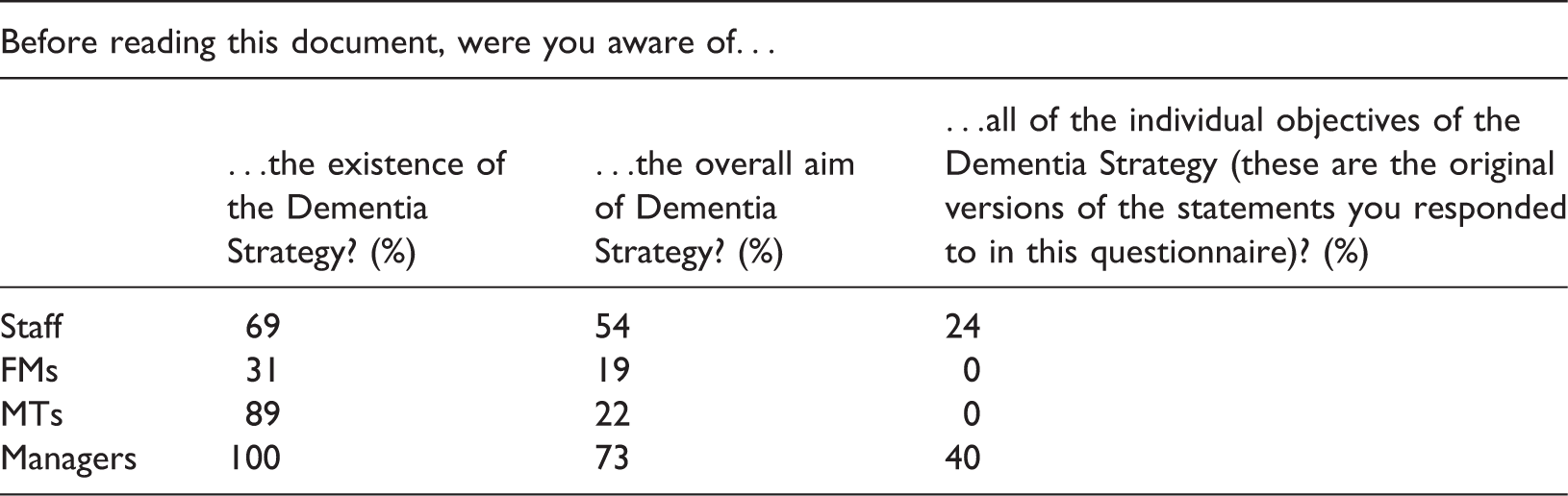
Familiarity with the Dementia Strategy.

With regard to familiarity with music therapy, 56% of non-MT participants report having been involved with music therapy sessions (43% of FMs, 73% of staff and 71% of the managers). Since there is no statistical difference in responses to the questionnaire between those who have and have not participated in music therapy, 8 the subsequent analysis of the results is discussed with relation to participant groups rather than with level of familiarity with the Dementia Strategy.
Responses and speculative commentary
Overall trends
Overall responses to all the statements ranged from 64% (agree or strongly agree) to 6% (no response) with 27% (don't know) and 12% (disagree or strongly disagree).
9
This suggests a general trend towards agreement with the statements. There is greater agreement with statements about care (Theme 1) and least agreement with statements about practicalities (Theme 4) (Figure 1).
Ranking of agreement per theme. Ranking of agreement per participant group.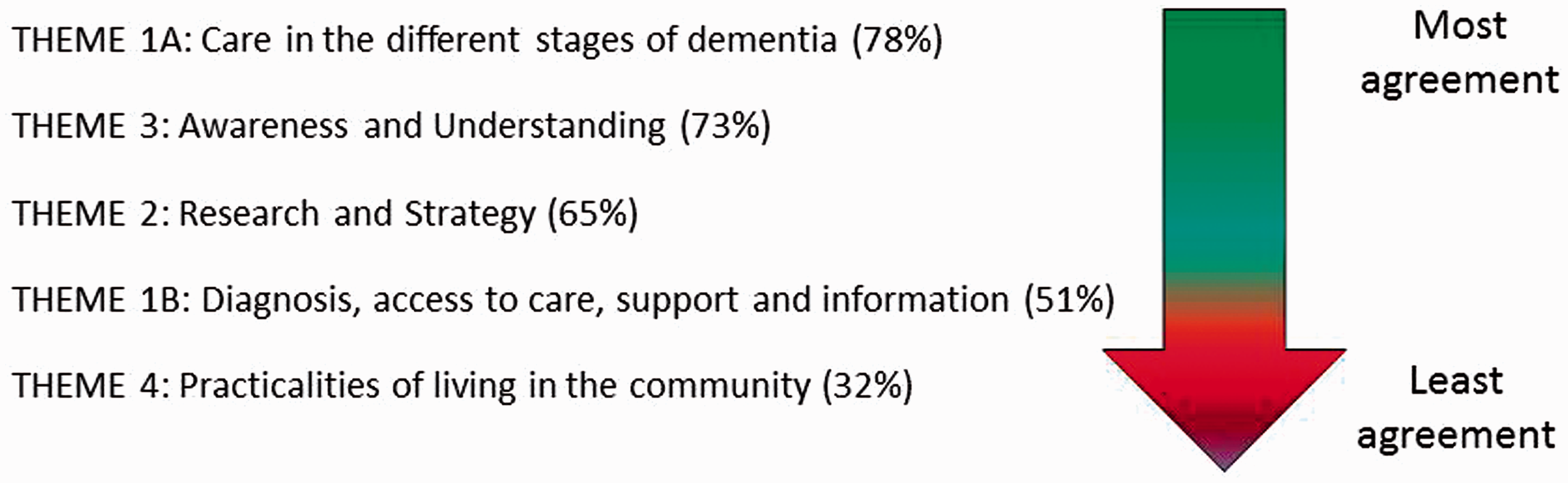
The difference between themes is significant when all the response options (strongly agree, agree, disagree, etc.) for each of the themes are compared (Friedman χ 2 (n = 71) = 91.06, p < 0.001). 10 The rate of agreement with statements in Theme 1A is significantly higher when compared to all the other themes (e.g. compared with Theme 3 z(n=71) = –2.7, two-tailed p < 0.01, using the Wilcoxon test). 11 As expected (Table 1), agreement with statements on Theme 4 is significantly lower than with statements in all the other themes (e.g. compared with the Theme 3 (z(n=71) = –5.7, two-tailed p < 0.001, Wilcoxon). 12
Overview of responses by population group
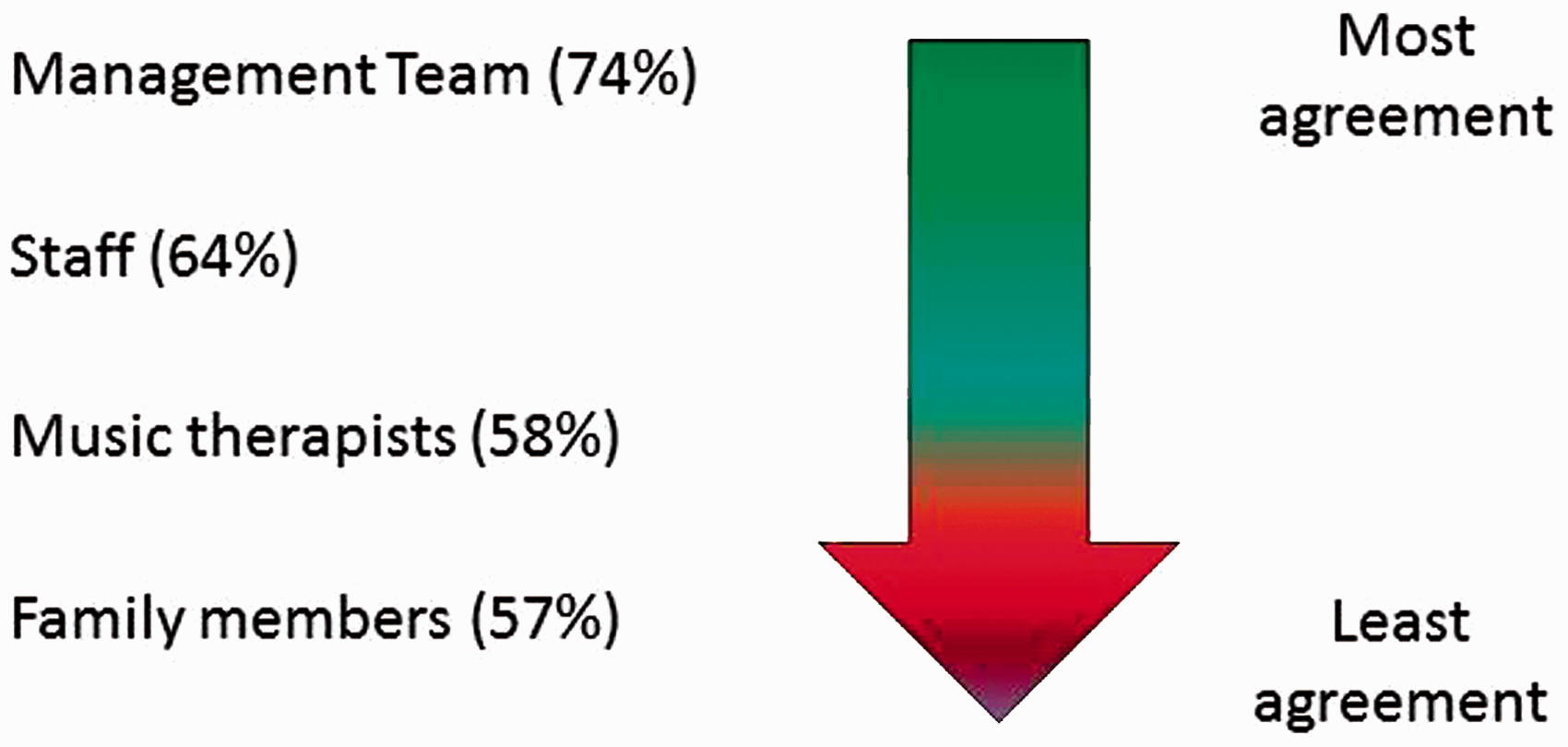
The managers have the highest overall rate of agreement with the statements throughout the questionnaire, while MTs have the lowest, closely followed by FMs (Figure 2).
Results by theme
The following section presents the responses to the individual statements in more detail and is structured according to the four themes:
Theme 1A: Music therapy and care in different stages of dementia and settings Theme 1B: Music therapy and diagnosis, access to care, support, and information Theme 2: Music therapy and research and strategy Theme 3: Music therapy and awareness and understanding Theme 4: Music therapy and practicalities of living in the community
Theme 1A: Music therapy and care in different stages of dementia and settings
In this theme, 78% of responses are strongly agree or agree. Responses to statements concerning care (Figure 3(a)) received on average 82% agreement, responses to statements to do with care at the various stages of the condition (Figure 3(b)) received on average 89% agreement, while responses to statements to do with location of care (Figure 3(c)) on average 62% agreement.
Music therapy and care in different stages of dementia and settings (Themes 1A). (The key shown here applies for this and all subsequent graphs that show the six response options.)
The first statement, Music therapy is part of care and support of individuals with dementia is the statement with which all respondents unanimously agree. Pairwise comparisons suggest that the differences between responses to this statement and all the other statements in the theme are significant. 13 The second general statement, about the efficacy of music therapy for the support of carers' needs has less agreement (63%), with highest agreement coming from the MTs.
The pattern of responses to these two statements is to be expected. Music therapy traditionally focuses on psychological support of the person living with dementia and is most often discussed and assessed within this context. As discussed earlier, recent studies have suggested that music therapy is also of benefit to the people surrounding the patient – the carers, family and staff members (Pavlicevic et al., 2015). It seems that the MTs questioned share this view more than the other groups.
The next four statements concern the role of music therapy in care at different stages of the condition – as subdivided in our preparation of the questionnaire (Figure 3(b)). This group of statements has the highest rate of agreement in the study; agreement is particularly high for early, mid and late stages of dementia. Amongst these, the lowest agreement rate is found in late stage dementia; and here, interestingly, the MTs' responses lower the agreement level. Overall, the highest rate of agreement is the mid-stage category; the lowest rate is within the late-stage category though the differences here are not statistically significant. Indeed, all of the groups' responses to statements about all three stages are above 80% agreement, except the MTs who are the only group of respondents who show very different responses for the various stages of dementia. Only 67% (n = 8) of the MTs agree with the statement that music therapy improves care for people in the late stages of dementia. Interestingly, they do not disagree either – three choose don't know and one leaves the response blank. This suggests either that this subgroup of MTs is more critical, and perhaps has a clearer notion, of the impact of music therapy at the different stages; or, more likely, it is indicative of some respondents' limited experience of working with dementia sufferers in the later stages of the condition.
The next three statements concern care in different settings and planning for care in hospitals (Figure 3(c)). The statement regarding the improvement of the quality of care in care homes has a high level of agreement (90%). The statements regarding planning of end-of-life care and end-of-life care in hospitals receive least agreement (47 and 48% agreement, respectively) with pairwise comparisons showing that the differences between these two statements and the majority of the other statements in the theme are significant (for the most part z is between –6.37 and –3.056, p < 0.001 (Wilcoxon test)).
The three statements in Theme 1A regarding music therapy and end-of-life care (see Figure 3(b) and (c)) receive strikingly different responses from all groups of participants: there is high agreement with the statement regarding music therapy in general end-of-life care (86%); much less agreement with the statement regarding the efficacy of music therapy for end-of-life care in hospitals (47%) and also for the planning of end-of-life care (48%).
The response choice for the questions regarding hospitals (see Figure 3(c)) perhaps reflects the experience of the respondents. For example, only three of the MTs have current or past experience of working with people with dementia in a hospital setting and these two questions have among the highest number of don't know and no responses of all statements. We can therefore attribute the low rate of agreement to respondents' feeling that they do not have sufficient information to make an informed judgement. The high disagreement and don't know response concerning the role of music therapy in planning end-of-life care is unsurprising as music therapy has little to do with the planning mechanisms surrounding a client.
Theme 1B: Music therapy and diagnosis, access to care, support, and information
Disagreement and don't know responses feature strongly in the subtheme Care and pathways to care (50%). This resonates with the anticipated responses (Table 1).
In general, the managers are most in agreement with statements in this theme, with their rate of agreement being consistently above 50%. In contrast, the MTs' response is consistently below 50%. FMs generally disagree with the statements concerning provision of information about dementia, whereas they consistently agree that music therapy helps with access to care and support. The differences in response to the following examples illustrate the different patterns of relationship between groups.
Between-group differences are significant for the statement Music therapy is part of good-quality early diagnosis (Kruskal–Wallis: χ2(3) = 15.4, two-tailed p < 0.01). In this case, FMs and managers agree with the statement more than the MTs (Mann–Whitney U test: U(n1 = 14, n2 = 9) = 21.500, two-tailed p < 0.01, U(n1 = 9, n2 = 15) = 13.5, two-tailed p < 0.001, respectively).
The generally lower rate of agreement with the statements in this subtheme may be because the topics covered are not traditionally associated with music therapy. MTs answering this questionnaire are not part of the diagnostic process since residents often enter the care home with a diagnosis in place. Similarly, MTs are not involved with providing access to other services and information about dementia or associated services. FMs may agree with the statements about access and support because they feel supported by their involvement in music therapy at the care homes. However, there is less agreement with the idea that information is provided via the MT, which is to be expected. Managers' greater level of agreement may be partly due to a form of professional responsibility – they are in a position to observe indirect connections that others on the ground do not perceive.
Theme 2. Music therapy and research and strategy
Sixty-five per cent of responses agree with statements in this theme. In the following analysis, research and strategy are discussed separately.
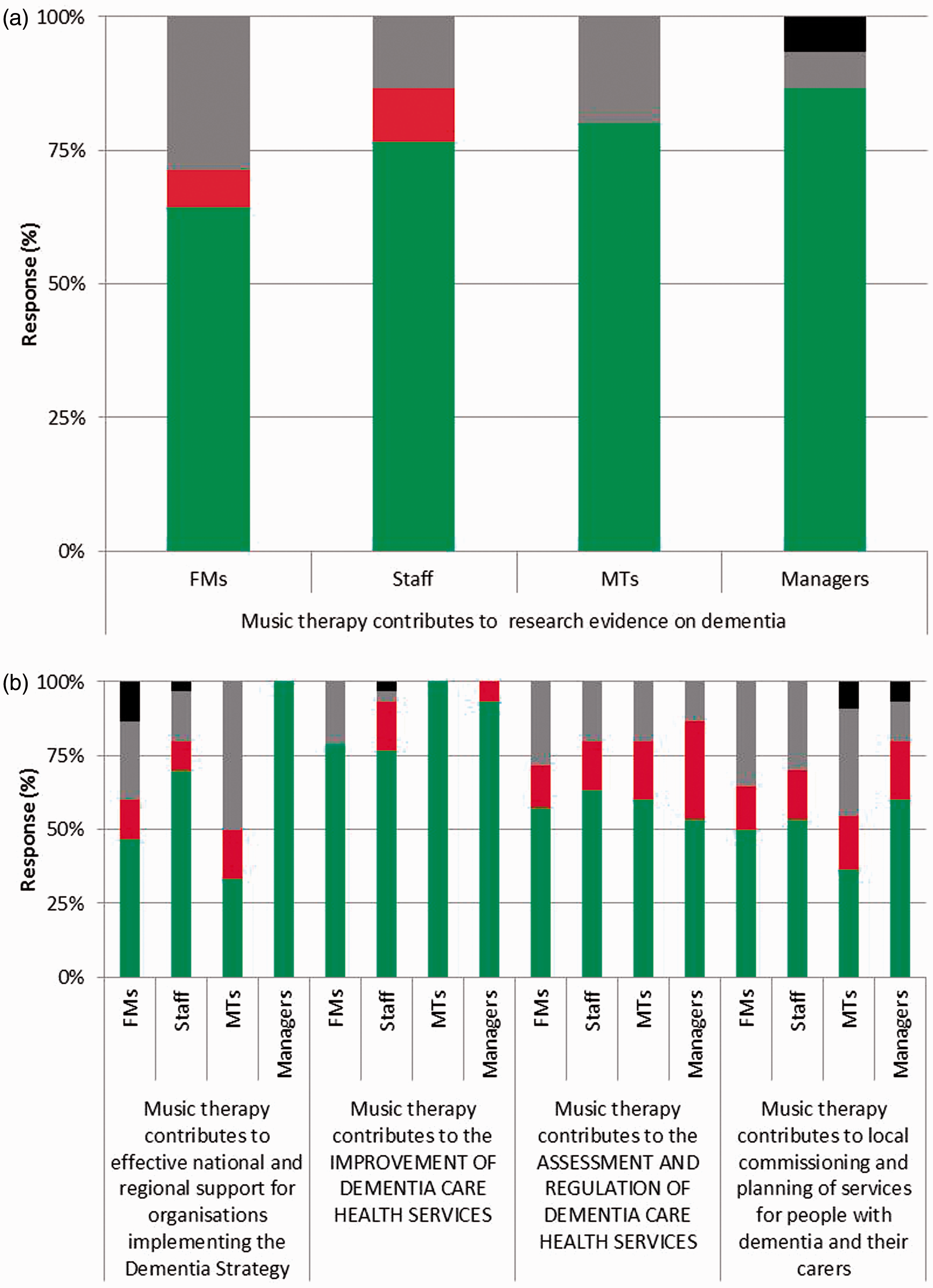
The frequent use of don't know suggests that respondents do not consider themselves to be informed about music therapy research. The FMs use this option most. The decreasing rate of agreement from managers to FMs mirrors an expected variation of interest in, and professional use of, research.
There is most agreement with the second statement in Figure 5(b) regarding music therapy contributing to the improvement of dementia healthcare services; 100% agreement by MTs and 93% by managers. Agreement with this statement is significantly higher than that with other statements in this theme. For example, the difference between responses to the first and second statement is significant (z(n=71) = −3.53, two-tailed p < 0.001, Wilcoxon test). 14
The first statement, regarding contribution to national and regional organisational support, received a varied response from each group of respondents; managers responded with 100% agreement, while MTs agreed far less (33%). There was also a high use of don't know (24%) and a rare use of strongly disagree by FMs (13%). For the statements regarding assessment, regulation, commissioning and planning of services, there is a rather low rate of agreement (53%) and a high use of both don't know and disagree. The differences between the groups were not found to be significant for any of the questions. 15
The wide range of responses within this theme reflects the range of awareness of strategy amongst the four groups of participants. For example, managers interact with regional strategy as part of their daily work, whereas this is a topic far removed from the everyday life of FMs.
Theme 3. Music therapy and awareness and understanding
This theme has the second highest rate of agreement of all the themes in the Dementia Strategy (73%, see Figure 1 above).
There is high rate of agreement with the four statements (Figure 6(a)) which together concern understanding and awareness of dementia as well as associated stigma and discrimination. However, there is a difference between the responses from MTs and managers on one hand, and from staff and FMs on the other: MTs and management are in almost 100% agreement with the statements, whereas FMs and staff make frequent use of the disagree, strongly disagree and don't know options as well as leaving some blank. The differences between MTs and managers on one hand and staff and FMs on the other may reflect their various interpretations of the role and function of music therapy for people living with dementia. Within music therapy discourse, ideas regarding the role of music therapy in changing peoples' view of individuals living with the condition have become standard (Powell, 2006). Similarly, at Barchester Healthcare a number of initiatives have contributed to sharing information about this possible function of music therapy (Wood, 2007). However, the fact that managers and MTs agree that music therapy influences public opinion, yet staff and FMs do not agree, suggests that this function of music therapy is not explicitly communicated within every care home.
Music therapy and diagnosis, access to care, support, and information (Theme 1B). Music therapy and research and strategy (Theme 2). Music therapy and awareness and understanding (Theme 3).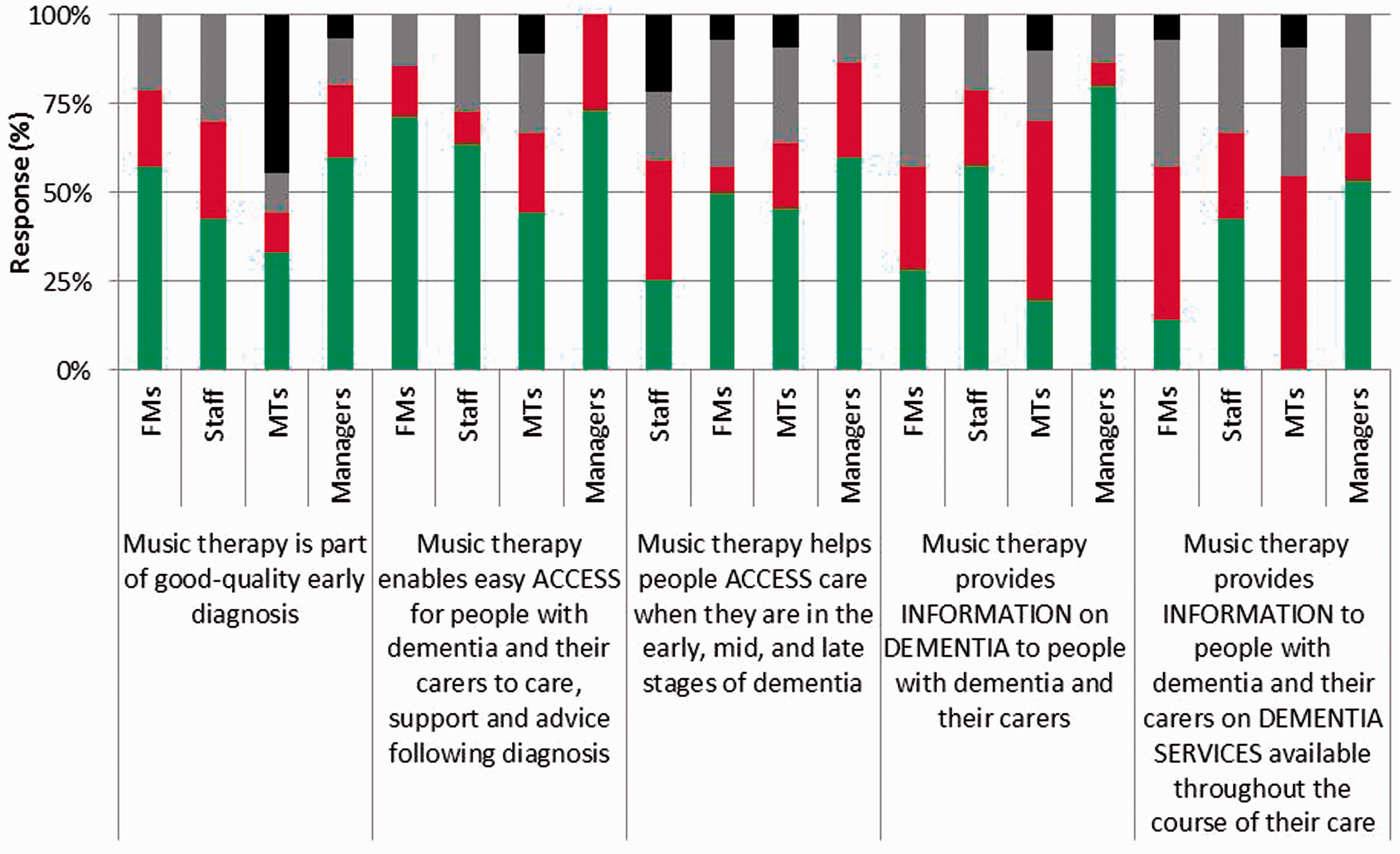

The lowest agreement within this theme is with the first statement in Figure 6(b) about seeking appropriate help for people with dementia. Pairwise comparisons show that the difference between responses to this question and most of the other statements in this theme is significant. 16
The rate of agreement with the rest of the statements in Figure 6(b) is again mixed. The lowest rate of agreement is with the statement regarding the impact of music therapy on the seeking of help (43%), while the statements regarding the provision of help received a higher level of agreement from some groups, including 100% from managers. There is a high use of don't know in statements about peer support and seeking help (30%).
The high use of don't know suggests that respondents are less familiar with the topics in these statements. The lowest agreement rate (for the statement regarding seeking help) suggests that, as expected, music therapy does not help with the seeking of appropriate help. Since this statement concerns the actions of FMs and carers, managers and MTs may have felt less equipped to give an opinion.
Theme 4. Music therapy and practicalities of living in the community
There is least agreement with statements from this smallest theme as anticipated (see Figure 1 and Table 1 above); with the highest use of don't know (42%) and the joint highest level (with Theme 1B) of disagreement (21%).
The third statement, regarding telecare, is the only one that has received no agreement from the MTs. It also has the highest use of the strongly disagree option (37.5%; Figure 7). Despite the low level of agreement overall in the theme, there is a high level of agreement by staff that ‘music therapy enables people with dementia and their carers to take an active role in developing local services’. This may be due to an interpretation of the statement, where ‘local services’ are understood to indicate activities delivered within the care home.
Music therapy and practicalities of living in the community (Theme 4).
Since the theme concentrates on topics that are far removed from the remit of music therapy work and from the respondents in this study whose focus is work in the care home, it is unsurprising that the majority of respondents do not agree with the statements. Also, statements in this theme concern issues that are no longer so relevant for those living in the care home (such as the second and fourth statements in Figure 7).
Discussion
In summary, the findings present some trends: there are broad differences between the groups, with some themes (e.g. Theme 1B, Diagnosis, access to care, support and information) eliciting larger differences between group responses than others (e.g. Theme 1A, Care in different stages of dementia and settings); and there are different patterns of response to individual questions. Overall, in approximately two-thirds (64%) of the responses participants selected agree or strongly agree to statements, which suggests that current music therapy practice fulfils many of the objectives of the Dementia Strategy.
Some themes have a higher proportion of agreement than others. There is greatest agreement with statements concerning care (Theme 1A) and awareness and understanding (Theme 3), and least with practicalities of living in the community (Theme 4). The two subthemes of Theme 1 elicit rather different responses: Care at the different stages of dementia and care settings (Theme 1A) has greatest agreement, and Diagnosis, access to care, support, and information (Theme 1B) has less agreement. These responses resonate with music therapists being predominantly involved in the care and well-being of individuals with dementia and less involved in the processes of enabling access to care. For Theme 2, a high proportion of respondents agree that research on music therapy and dementia contributes to ‘a clear picture of the research evidence’ on dementia. In terms of strategy, the responses suggest that music therapy can contribute to effective services more on an organisational level than on national ones. Responses in Theme 3 suggest that although music therapy is traditionally practised with the person with dementia, the sphere of influence includes people around the clients. Indeed, more than half of those who took part in the survey had previously been directly involved in music therapy sessions. The suggestion that music therapy has direct and indirect spheres of influence is closely tied to the idea of the ‘ripple effect’ – discussed in our related paper (Pavlicevic et al., 2015). Finally, with regard to Theme 4, there is most disagreement with, or least knowledge about, the idea that music therapy plays a role in helping people with dementia and their families to develop local services and support services for living at home.
The range of agreements and disagreements is in alignment with the expectations suggested at the start of the paper and fits with what has come to be considered the purpose of music therapy for people with dementia. While music therapy is known to support the well-being of clients, and seen to increase the awareness and understanding of dementia (aided by research and strategy), it is less associated with access to care and practicalities of living in the community. Music therapy is, therefore, seen to fulfil a large proportion and distinct aspects of the objectives of the Dementia Strategy.
The survey highlighted disparities in perception between respondent groups, and it may be worth redressing the missing connection between what music therapists do and how they communicate it to others. In particular, to what extent are music therapists efficiently communicating their work to care home colleagues and family members? For example, music therapists agreed more than any other group that their work contributes to carers' needs. This prevalent opinion of music therapists may be derived from recent studies suggesting that music therapy reaches people surrounding the resident – the carers, family and staff members (Pavlicevic et al., 2015). It is unclear whether this disconnect between the perception of music therapists and that of the other groups is connected to awareness (i.e. music therapy does contribute to carers needs, however it is not directly obvious) or is an issue connected to the perception of potential influence rather than reality (i.e. music therapy could support carers' needs but does not do so explicitly at the moment). We therefore suggest that clarifying and addressing the cause of this difference in opinion is a professional imperative.
This study has explored how music therapy might be seen to contribute to the implementation of the Dementia Strategy, through exploring the ‘fit’ with the strategy's objectives. The growing ageing demographic trend in the UK and in Europe, together with the degenerative, highly personal and isolating nature of dementia bring particular challenges for all of those close to the sufferer.
The Dementia Strategy focuses both on the individuals and on the community around them, aiming to maximise public awareness of dementia, and ensure high-quality treatment throughout the various stages of the condition. Music therapists have for many years contributed to the quality of life of people living with dementia, focusing on people's individual and collective well-being and emotional needs. Music therapists facilitate intimate emotional–musical communications with those whom words and language have long ceased to function and work to build flourishing musical communities in residential care homes (Stige, Ansdell, Elefant, & Pavlicevic, 2010).
We suggest that for the arts-based professions, this exploration is timely – even it if does not sit altogether comfortably within the ambit of arts-therapies research, often concerned with efficacy, impact and advocacy. However, it would seem that in light of current reconfigurations of healthcare provision, the moves towards personal budgets and the evolving nature of clinical commissioning for services that include all the arts therapies, more engagement with such strategy and policy documents may well need to become part of the everyday work of music (and arts) therapy practitioners and researchers.
Finally, we suggest that this study can be a foundation for future collaboration between national policy strategists and music therapists, in planning the delivery of care for people with dementia. We suggest that music therapists could contribute to future government strategies by drawing on the long-lasting practical consequences of their work – which includes the valuing of family and carers' needs and opinions as highly as those of dementia sufferers. The alignment of objectives and outcomes of music therapy with the objectives and outcomes of the Dementia Strategy indicates that there is a strong basis for the inclusion of music therapy within the statutory provision of dementia care.
Footnotes
Acknowledgements
Many thanks to our colleagues at Nordoff Robbins, to Barchester Healthcare, and to family members who took part in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Neta Spiro is a researcher at the Research Department, Nordoff Robbins, London Centre and is a member of the Faculty of Music, University of Cambridge.
Camilla L Farrant is a research assistant at the Research Department, Nordoff Robbins, London Centre and head music therapist at Music Therapy Tree which specialises in providing music therapy to vulnerable children in mainstream education.
Prof Mercédès Pavlicevic is director of research and of the PhD programme at Nordoff Robbins Music Therapy, and research associate at School of Oriental, African Studies (SOAS), University of London.