
Abstract
A quasi-experimental study using a pre–posttest design was conducted in four aged care facilities to assess the effects of a person-centred care (PCC) multisensory stimulation (MSS) and motor stimulation (MS) program, implemented by direct care workers, on the behaviors of residents with dementia. Data were collected at baseline and after the intervention through video recordings of morning care routines. Forty-five residents with moderate and severe dementia participated in the study. A total of 266 morning care routines were recorded. The frequency and duration of a list of behaviors were analyzed. The frequency of engagement in task decreased significantly (p = .002) however, its duration increased (p = .039). The duration of gaze directed at direct care workers improved significantly (p = .014) and the frequency of closed eyes decreased (p = .046). There was a significant decrease in the frequency of the expression of sadness. These results support the implementation of PCC–MSS and MS programs as they may stimulate residents’ behaviors.
Keywords
Introduction
Currently, dementia is the leading cause for placement of older people in long-term care facilities. Approximately half of these individuals are cared in aged care traditional facilities (i.e., large, private, nonprofit organizations of collective accommodation) (Prince, Prina, & Guerchet, 2013), as specialized units for people with dementia are still scarce.
It has long been recognized that aged care facilities are limited in resources and skilled direct care workers (DCWs) to meet the needs of people with dementia (Stone, 2012). Previous studies have reported high levels of passivity and low levels of interaction among residents with dementia, being most of their time asleep, socially withdrawn, or not engaged in any meaningful activity (Cohen-Mansfield, Marks, Dakheel-Ali, Regier, & Thein, 2010). This lack of stimulation is detrimental as it has been linked to decline in residents’ physical, behavioral, and cognitive functioning, as well as in their quality of life (Cohen-Mansfield et al., 2010).
Providing DCWs with education and training have typically been used as the means to improve quality of care for people with dementia and ensure a motivated and stable workforce (Nolan et al., 2008). Person-centred care (PCC) has become the cornerstone of such educational interventions and is perceived as the ideal opportunity to deliver high quality of care to people with dementia (Edvardsson, Winblad, & Sandman, 2008). It is a philosophy of care that focuses on the need to treat them as individuals, to view the world from their perspective, to maximize their retained abilities, and to create a positive psychosocial environment for them (Brooker, 2007; Kuske et al., 2009).
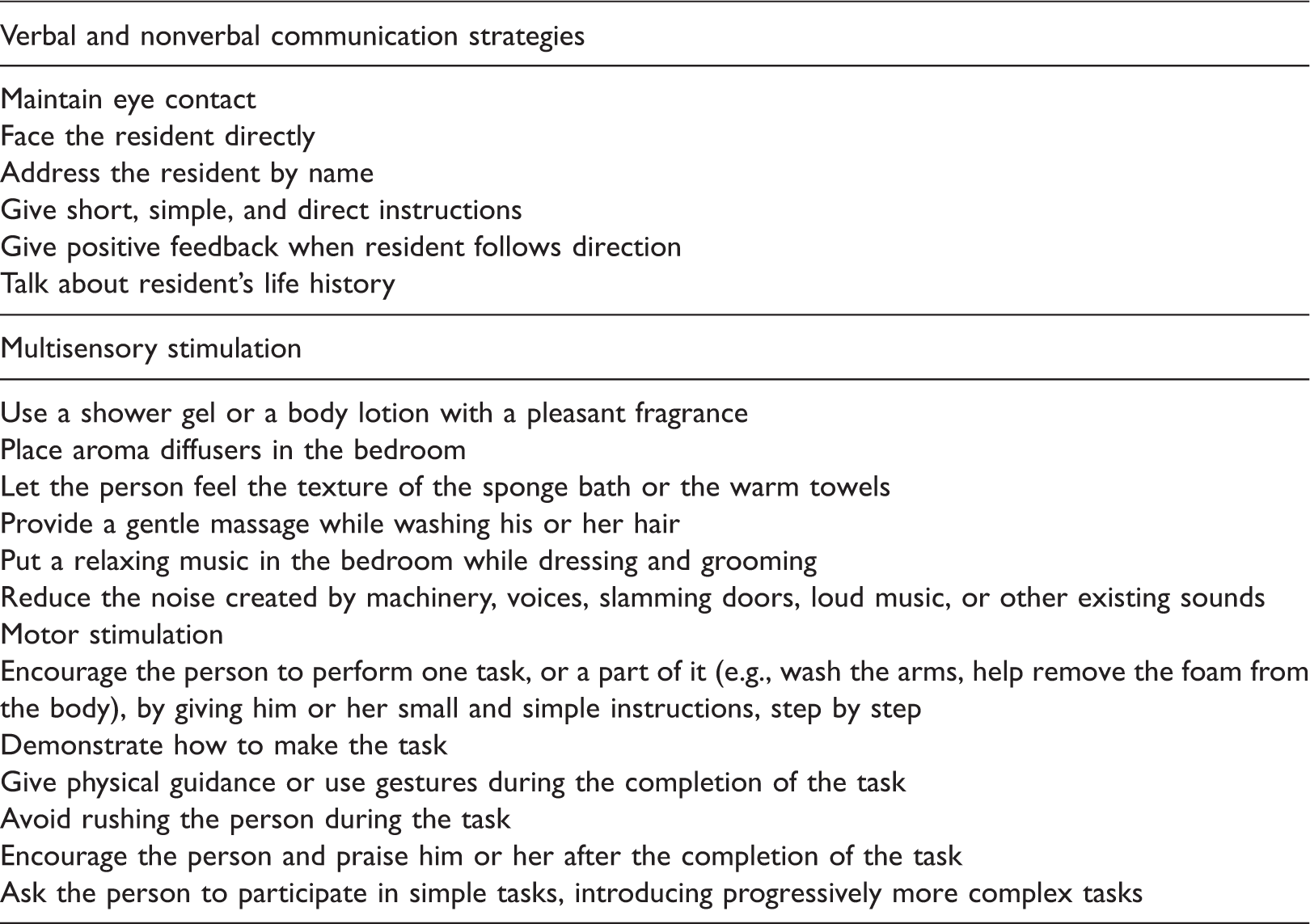
Among the wide range of valuable approaches to deliver PCC, multisensory stimulation (MSS) and motor stimulation (MS) are of special interest as they do not require the use of higher cognitive processes (Baker et al., 2003; van Weert, van Dulmen, & Bensing, 2008), being suitable to residents at all stages of dementia. MSS and MS are used to provide adequate stimulation and assistance in activities of daily living (ADL), while respecting people’s abilities and preferences (Bowlby, 1998). Overall, MSS, previously known as snoezelen, is an approach aiming to stimulate the senses through the provision of visual, auditory, olfactory, and tactile stimuli, therefore providing an alternative to cognitive-based activities (van Weert, van Dulmen, & Bensing, 2008). The development of MSS may be viewed as a valuable response of institutional settings to face the well-described sensory deprivation and consequent deleterious of the dementing process (Baker et al., 2001; van Weert, van Dulmen, Spreeuwenberg, Ribbe, & Bensing, 2005). It may be implemented without specialized equipment, space, or environment and it has been found to reduce disturbed behaviors and apathy, enhance residents’ attentiveness, and increase resident–staff interactions process (Baker et al., 2001; van Weert et al., 2005). MS aims to delay residents’ functional decline through, simple, familiar, and individually tailored exercises known to promote active movement (Rolland et al., 2007; Tappen, Roach, Applegate, & Stowell, 2000). This is important because of the decreased physical activity and mobility with dementia.
Training programs for DCWs to implement PCC–MSS and MS strategies in daily care provision of residents with advanced dementia hold promise as a means of improving residents’ interaction. Preliminary investigations have suggested that the implementation of these strategies in dementia care routines would result in an increase in residents’ nonverbal communication (e.g., eye gaze, smiling) (Cruz, Marques, Barbosa, Figueiredo, & Sousa, 2011; van Weert et al., 2005), verbal communication (van Weert et al., 2005), and engagement (Cruz et al., 2011) in morning care routines. On the basis of these findings might be the fact that MS and MSS are considered undemanding approaches, which can result in a more relaxed working style while allowing DCWs to get their work finished (van Weert et al., 2005). Despite this, there are still few research studies that have specifically trained these workers with basic skills to implement motor and MSS in daily care provision to residents with dementia (Cruz et al., 2011; Marques, Cruz, Barbosa, Figueiredo, & Sousa, 2012; Sidani, Streiner, & Leclerc, 2012).
The potential impact of DCWs implementing MSS and MS on residents with dementia requires further research. Therefore, this study assessed the effects of a PCC–MSS and MS program on residents’ behavior during morning care. Residents’ engagement in the morning tasks was defined as the primary outcome. Eye contact, mood, and verbal and nonverbal communication were established as secondary outcomes.
Methods
Design and setting
A quasi-experimental study using a single group with a pretest and posttest design was conducted. Ethical approval was previously obtained by the Ethics Committee (Ref. 5–11/2010).
The study was conducted in four aged care facilities with a staff–resident ratio between 1:2 and 1:3. After a meeting to explain the study, all managers agreed to participate and ensured no simultaneous participation in similar studies or significant organization changes would occur during the intervention period. The intervention period occurred between November 2011 and March 2013.
Participants
The physician of each care facility was asked to identify residents who met the following inclusion criteria: (1) presented a clinical diagnosis of moderate to severe dementia, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV criteria) (American Psychiatric Association, 2000); (2) had no other psychiatric diagnosis; (3) required staff assistance during ADLs (i.e., bathing and grooming); and (4) were living in the facility for at least two months, to ensure that residents’ adaptation to staff and care home environment had already occurred.
A total of 51 residents were identified. The legal guardian of each resident was contacted and informed about the study. Residents’ anonymity and confidentiality were assured and informed consent was obtained from proxy consent prior to any data collection. One legal guardian refused residents’ participation, one resident refused to be assessed by video, and one resident died before data collection. During the intervention, three residents died and their information was removed. Thus, a total of 45 residents with moderate-to-severe dementia participated in the study.
DCWs were identified by the manager of each facility. These workers had to be employed in the facility for at least two months (to ensure that the adaptation to residents and facility has already occurred) and provide personal care to residents with dementia. Temporary workers, trainees, and other health and social care practitioners (physicians, nurses, and social workers) were excluded, as they did not provide personal care on a regular basis. All DCWs agreed to participate and signed the written informed consent. Fifty-eight staff members were identified, however, two dropped out due to sick leave. Thus, 56 DCWs participated in the study.
Intervention
The design of the intervention was based on: (1) a comprehensive literature review about dementia, intervention for DCWs, PCC-based interventions, MSS and MS strategies and (2) findings from a pilot study conducted in one aged care facility with six residents previously (Cruz et al., 2011; Marques et al., 2012).
The PCC–MSS and MS program for DCWs was conducted by a gerontologist and a physiotherapist with training and experience in PCC approaches. Eight weekly group sessions of approximately 90 minutes were conducted.
Strategies to interact with the person and provide stimulation.
Content of the PCC–MSS and MS program.
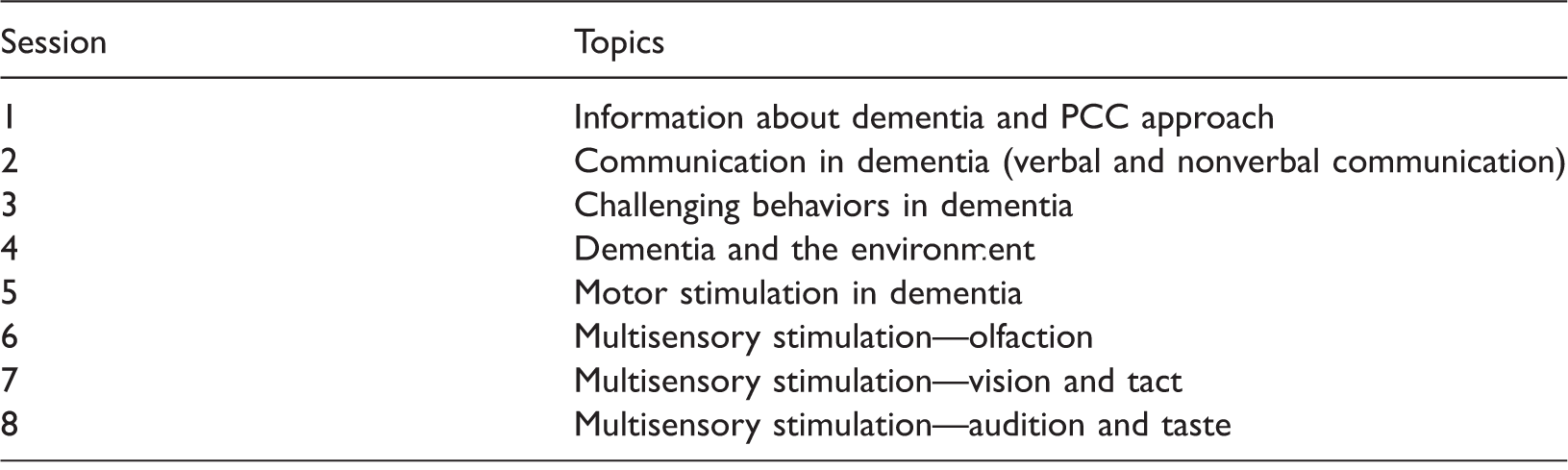
Note: PCC, person-centred care; MSS, multisensory stimulation; MS, motor stimulation.
In the following three days after each session, the gerontologist and the physiotherapist assisted DCWs during the provision of morning care, clarifying doubts and making suggestions to help them to implement the PCC–MSS and MS strategies. Morning care (i.e., activities concerning dressing and toileting) was selected as this is the period of the day where more interaction between DCWs and residents occurs, and also when residents’ problematic behavior (e.g., agitation) is more frequent (Sloane et al., 2004, 2007; Sidani et al., 2012; van Weert et al., 2006).
Data collection
Residents’ sociodemographic data
Residents’ sociodemographic data (gender, age, and type of dementia) and functional ability were first collected at baseline from the resident’s profile. Information concerning residents’ interests, preferences, favorite colors, or smells was provided by legal guardians and DCWs. Mini Mental State Examination (MMSE) (Guerreiro et al., 1994) was used to confirm residents’ cognitive impairment. This instrument includes 30 questions, which assess cognitive functions, such as episodic and working memory, language, praxis, and spatial and temporal orientation. Higher scores correspond to better cognitive function. Cutoff scores used for the MMSE were: 22 for 0–2 years of education, 24 for 3–6 years of education, and 27 for ≤7 years of education (Morgado, Rocha, Maruta, Guerreiro, & Martinas, 2009). The Global Deterioration Scale (GDS) (Leitão, Nina, & Monteiro, 2007) was used to measure the progression of dementia according to seven levels, ranging from “no cognitive decline” (score 1) to “very severe cognitive decline” (score 7). The use of this scale ensured that only residents with moderate to severe dementia were included (score of 4 or above).
Residents’ behaviors
The impact of the PCC–MSS and MS program on the behavior of residents with dementia was studied through the observation of video recordings of morning care. The observation has been described as the best way to assess residents’ behavior and recognize when a meaningful interaction is occurring (Elder, 1999). This method has been used in similar studies, showing to reduce observation bias (Cruz et al., 2011; Marques et al., 2012). The video camera was fastened to a tripod in the room where personal care was being provided to the resident and turned on when DCWs entered the room. Researchers were not present in the room to avoid affecting residents’ behavior by the presence of strangers. All DCWs were instructed to inform the resident about the camera, ask their permission to record, and stop or remove the video camera if they noticed any residents’ negative reaction caused by the presence of the device. Nudity was not recorded to protect residents’ privacy. To guarantee this, DCWs were instructed to stop the video before the person with dementia would be naked (e.g., before bathing). Moreover, to minimize the effects of the camera on the behavior of DCWs and/or residents and reduce reactivity effects, several video recordings were performed prior to data collection, so participants could become accustomed to the video cameras (Elder, 1999). Data were collected at baseline and two weeks after the PCC–MSS and MS program. Assessments lasted about two to three weeks. Each resident was recorded three times before and three times after the intervention to guarantee that the behavior was not due to chance. In total, 266 episodes of morning care routines were video recorded, 132 at baseline and 134 after intervention.
DCWs’ sociodemographic data
DCWs’ sociodemographic data were collected at baseline with a structured questionnaire including variables such as gender, age, education, marital status, and length of time working in the facility.
Data analysis
A sample size calculation using one behavior category—duration of engagement in task—was performed based on a previous pilot study previously (Cruz et al., 2011; Marques et al., 2012). It was found that 34 residents with dementia would be required to provide 95% power (α = 0.05) to detect significant differences between assessments. However, the pilot study had a dropout rate of 25% and to cover for this a sample size of 45 residents was considered necessary.
Sociodemographic data were analyzed through descriptive analysis, performed with the software Statistical Package for the Social Sciences version 20 (IBM Corporation, NY, Armonk, USA).
Categories of the ethogram.
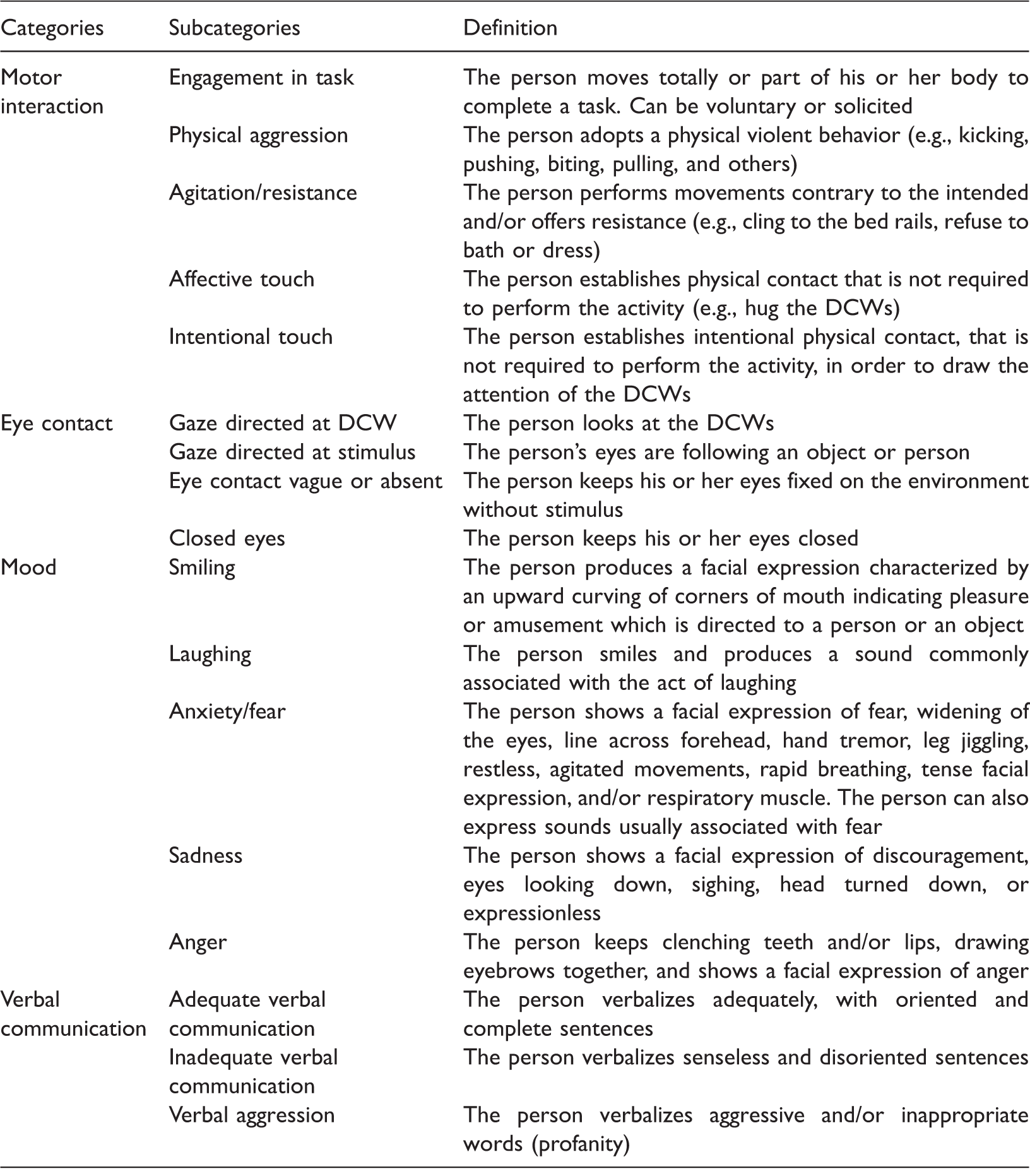
Note: DCW, direct care worker.
To be able to compare the variables between the different participants and across different moments (pre- and postintervention), the video recordings were edited so that they would have the length of the average duration—8 minutes and 29 seconds (509 seconds). For videos under this average duration, proportional scores were used. Then, for each participant, the average results of the three videos collected at each moment were calculated and paired t-tests were used to compare residents’ behaviors before and after the intervention. The level of significance was set at p < 0.05.
Statistical analysis was completed with the estimation of effect sizes (ESs), which evaluate the magnitude of the treatment effect (Kraemer & Kupfer, 2006). The Cohen’s d was used (mean change score divided by the standard deviation of change), as this is the ES index recommended for matched pairs (Faul, Erdfelder, Lang, & Buchner, 2007). Cohen’s d was calculated for each outcome measure using the Comprehensive Meta-Analysis (CMA) software, version 2 (Biostat, Englewood, New Jersey) and was interpreted as a small (≥0.2), medium (≥0.5), or large (≥0.8) effect.
An additional observer blinded to the study phase analyzed residents’ behaviors in order to calculate interobserver reliability. For this purpose, intraclass correlation coefficients (ICC) (equation 2,1) were used for the frequency and duration of each behavior category. In addition, the Bland and Altman method was used to assess interobserver agreement. The values of ICC ranged between 0.62 and 0.95 for behavior frequency and 0.60–0.94 for duration, indicating moderate to excellent reliability (Fleiss, 1986). The results obtained through the Bland and Altman method showed a good agreement with no evidence of systematic bias (Bland & Altman, 1986).
Results
Characteristics of the residents with dementia.
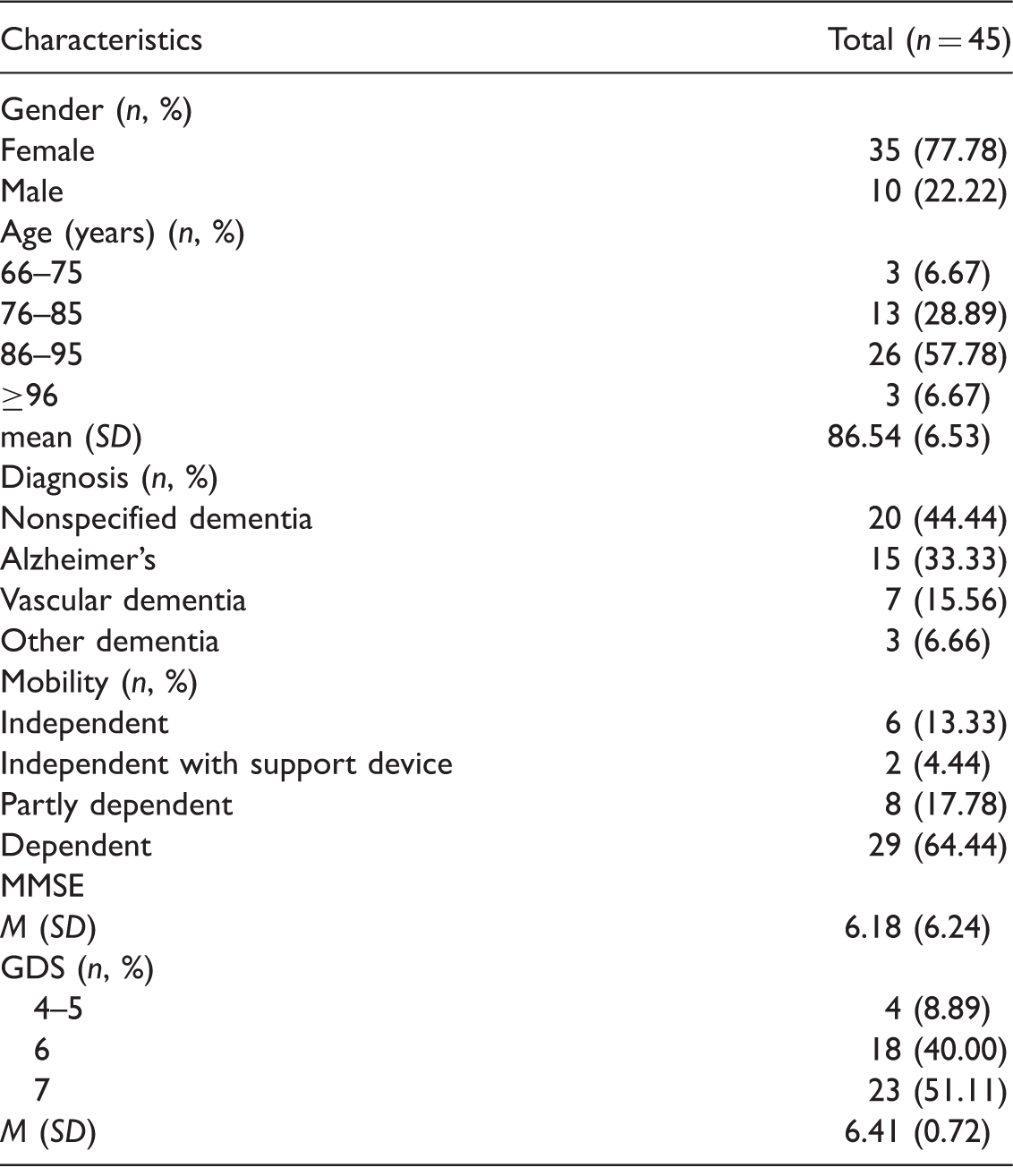
Note: SD, standard deviation; GDS, Global Deterioration Scale; MMSE, Mini Mental State Examination.
Values shown as n (%) or as M (SD) as indicated.
Characteristics of the direct care workers.
Note: SD, standard deviation.
Values shown as n (%) or as M (SD) as indicated.
Changes in residents’ behavior at baseline and after intervention.
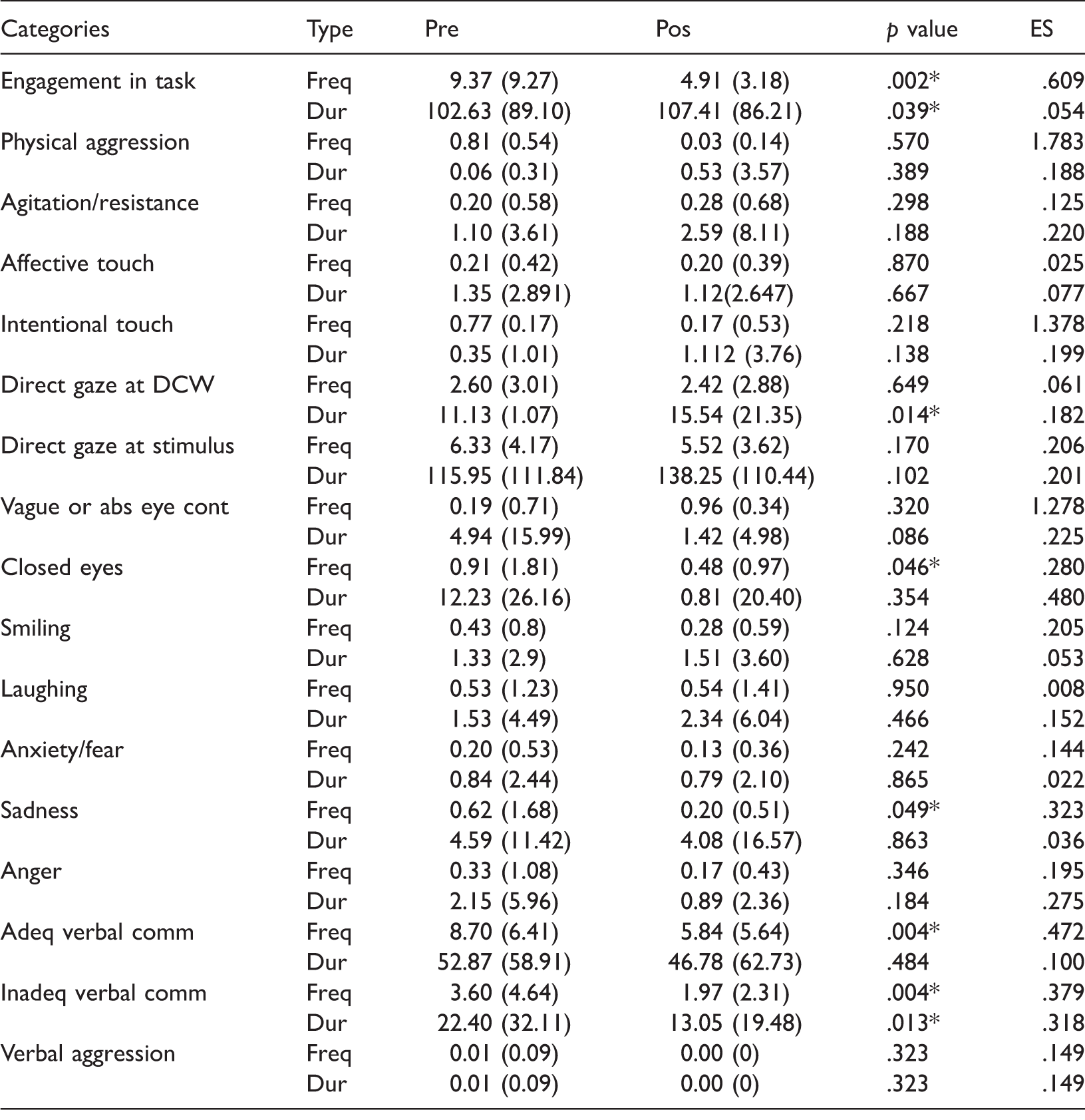
Note: Pre, baseline intervention; pos, after intervention; ES, effect sizes; Gaze direct stimulus, Gaze directed at stimulus; Vague or abs eye-cont, vague or absent eye contact; Adeq verbal comm, adequate verbal communication; Inadeq verbal comm., inadequate verbal communication; Freq, frequency; Dur, duration.
Values shown as n (%) or as M (SD) as indicated. *p < 0.05.
Discussion
The present study assessed the effects of a PCC–MSS and MS program implemented by DCWs on residents’ behavior during morning care.
Considering residents’ engagement in task, the findings showed that the duration of this variable increased significantly after the intervention, whereas its frequency declined. According to these results, after the intervention, residents seemed to spend more time involved in their morning care tasks with fewer interruptions. Similar findings have been found previously (Cruz et al., 2011; Marques et al., 2012), sustaining the relevance of a PCC–MSS and MS program to maximize residents’ retained abilities during morning care. Hence, motor learning is known to remain relatively intact in people with dementia, suggesting preservation of neural structures that integrate sensory and kinaesthetic information (Yan & Dick, 2006). MSS and MS were adapted to match sensory preferences and individual needs; the increased resident’ engagement in task is consistent with findings that demonstrated an increase in performance through stimulus presentation that match the cognitive ability of the individual. Also, results suggest that through training in PCC-based approaches, DCWs can become more aware of residents’ needs for independence and engagement, which can lead to improved quality of care (Sidani et al., 2012; Sloane et al., 2004, 2007; van Weert et al., 2005, 2006).
The results of this study indicated that there were also significant improvements in the duration of the gaze directed at DCWs and in the frequency of closed eyes. These findings may represent a progress in residents’ consciousness and awareness (Cruz et al., 2011). Similar studies (Cruz et al., 2011; Marques et al., 2012; Sánches, Miillan-Calenti, Lorenzo-Lópes, & Maseda, 2013) also showed an increase of eye contact between the residents and the DCWs after the training intervention. This is considered to be central in establishing a good relationship between the dyad, being associated with increased closeness, kindness, and attention (van Weert et al., 2005).
The frequency of the expression of sadness decreased significantly after the intervention. Although not statistically significant, there was also a positive trend in the duration of smiling, in the duration and frequency of laughing, anxiety/fear, and anger after the implementation of PCC–MSS and MS program. This corroborates the findings obtained from a recent literature review on the effects of MSS interventions, which demonstrated positive short-term effects on residents’ mood (Sánches et al., 2013). These are important results that reinforce the current literature stating that, even at advanced stages of dementia, individuals are still able to interact with their carers (Magai, Cohen, & Gomberg, 2002). In addition and similar to previous studies (Marques et al., 2012; Sánches et al., 2013), the findings showed a decrease in residents’ verbal communication, which can be explained by the increase of nonverbal communication as well as with by the losses of verbal communication skills, especially in people with moderate-to-severe dementia (Hubbard, Cook, Tester, & Downs, 2002). Assessing nonverbal communication, expressed by facial expressions and gestures (van Weert et al., 2005), is therefore essential to understand the relationship between the resident and the DCW. Nonverbal communication is an eminent mode of expression of empathy and an important tool to make contact with the DCW (Baker et al., 2001). Although the focus of this study was the residents themselves, the induced changes are dependent on the implementation of the intervention by DCWs. In fact, data on DCWs have been collected and published elsewhere (Barbosa, Nolan, Sousa, & Figueiredo, 2015; Barbosa, Sousa, Nolan, Marques, & Figueiredo, 2016). Positive benefits on DCWs were found on communicative behaviors with the residents (Barbosa et al., 2016), reduced levels of burnout, improved knowledge about dementia, enhanced feelings of being worthwhile, improved group cohesion, emotional management, and self-awareness (Barbosa et al., 2015). Therefore, it is believed that adequate and consistent implementation of the intervention has been ensured.
Overall, the results of the PCC–MSS and MS program support positive results at residents’ involvement and nonverbal communication levels. Nevertheless, several limitations need to be acknowledged. Changes in residents’ behavior were analyzed two weeks after the PCC program delivered to the DCWs. Thus, a short period of time was given to these professionals to adapt their practices and implement all the proposed strategies to stimulate residents during morning care. Future studies should provide a longer time of implementation and explored the long-term impacts of a PCC–MSS and MS program (Sidani et al., 2012). Although the use of power calculation may be considered a strength of the study, it was only performed for the variable engagement in task. It is possible that a larger sample would be required to obtain statistical significance in the other variables. The purpose of the study was to explore the impacts of MSS and MS on residents’ behaviors. Nevertheless, future research could also explore correlations between different measures of the ethogram. The fact that residents were not always recorded with the same DCW may have influenced their behaviors. Although this reflects the common practice, future studies should consider this aspect whenever possible. Moreover, the position of the camera could have occasionally hindered the observation of residents’ nonverbal communicative behaviors. Nevertheless, it is important to emphasize that compared to other usual methods (checklists fulfilled by DCWs), the assessment method used in this study, i.e., video-recordings through a behaviors analysis software (Haidet, Tate, Divirgilio-Thomas, Kolanowski, & Happ, 2009), shows significantly higher levels of objectivity and reliability. This methodology also reduces the bias caused by the social desire to report improvements after the intervention (Kuske et al., 2007).
Also, the study design lacked a control group. It is recognized that single-group pretest and posttest designs lack control for a number of confounding variables and this may have operated between the pretest and the posttest and affected scores. Among these variables may be, for example, DCWs’ maturation (i.e., DCWs that received the intervention tend to improve their competence over time simply due to increasing maturity), different intervention components, or organizational characteristics (e.g., leaderships’ support). Control (or comparison) groups are important for avoiding unwarranted interpretations of data and are therefore recommended.
Conclusion
Despite these limitations, several strengths are worth of consideration. The intervention was focused on a PCC–MSS and MS program approach for residents with dementia, which are commonly neglected in care homes. After the intervention, DCWs were individually followed to clarify possible questions; this is considered an important didactic strategy to sustain implementation of new knowledge. The ethogram showed moderate to excellent observer reliability, which is suggestive of its applicability. Future evaluations of the tool in order to further develop its acceptability, utility, and validity are recommended. Finally, video-recordings are a pioneer methodology in the field of dementia care and the use of modern and complete software to analyze the behaviors minimizes possible biases in the study.
This study offers objective data to support a PCC–MSS and MS intervention to improve residents’ engagement in task and nonverbal communication, being particularly associated with an increase in gaze directed at DCW, and a reduction in the frequency of closed eyes and sadness. This intervention might therefore increase residents’ interaction (Marques et al., 2012), well-being, and quality of life (Lawton, 1994) even at more advanced stages of the disease. As this is a topic of increase interest in dementia care, further research is warranted in order to investigate the long-term sustainability, cost-effectiveness, and extent of the benefits of this intervention on DCWs and organization.
Footnotes
Acknowledgements
The authors would like to acknowledge all facilities for their participation in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a scholarship from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Ref. BEX 7358/13-0.