
Abstract
The physical and mental health of older adults with dementia is affected by levels of social integration. The development of dementia special care units (D-SCU) arose, in part, to facilitate more meaningful social interactions among residents implying greater social integration of D-SCU residents as compared to residents in a traditional nursing home (TNH). But, it is unknown whether D-SCU residents are receiving equal or greater benefits from living on a segregated unit intended to enhance their social environment and integration through both design and staff involvement. The purpose of this study was to pilot test a comprehensive objective assessment to measure social integration among nursing home residents with dementia and to compare levels of integration of residents living on a D-SCU to those living in a TNH. A total of 29 residents participated (15 D-SCU and 14 TNH) and data were gathered from medical charts, visitor logs, and through direct observations. Over 1700 interactions were recorded during 143 h of observation. Specifically, the location, context, type, quantity, and quality of residents’ interactions were recorded. Overall, the majority of resident interactions were verbal and initiated by staff. Interactions were social in context, and occurred in public areas, such as the common room with a large screen TV. Average interactions lasted less than 1 min and did not change the resident’s affect. Residents spent between 10% and 17% of their time interacting with other people on average. D-SCU staff were significantly more likely to initiate interactions with residents than TNH staff. D-SCU residents also experienced more interactions in the afternoons and expressed more pleasure and anxiety than residents in the TNH. This study helps to lay the groundwork necessary to comprehensively and objectively measure social integration among people with dementia in order to evaluate care environments.
Background
Levels of social integration have a significant and direct impact on our physical and mental health (Berkman, Glass, Brissette, & Seeman, 2000; Umberson & Montez, 2010). Higher levels of social integration are associated with longer survival rates, higher perceived quality of life, successful aging, psychological well-being, and are a mediator to both physical decline and depressive symptoms among nursing home (NH) residents (Guse & Masesarm, 1999; Kiely & Flacker, 2003; Powers, 1991; Retsinas & Garrity, 1985; Yeung, Kwok, & Chung, 2012). Social integration can be weakened by the onset of dementia and a subsequent move to a NH can further disrupt social connections affecting social integration. Little is known about the social integration of NH residents with dementia (Grenade & Boldy, 2008). One reason for this oversight stems from the multiple and varied ways social integration is measured. In order to develop interventions that can improve social integration for this highly vulnerable and fast-growing population, we need to be able to comprehensively measure social integration. The assessment of social integration of NH residents with dementia can lead to future studies of the influence of integration on their health and quality of life.
Approximately 35.6 million people worldwide have dementia and this number is expected to double by 2030 (World Health Organization, 2012). Dementia is a major cause of institutionalization due to informal caregiver burden related to behavioral symptoms and the need for more skilled care and physical assistance (Buhr, Kuchibhatla, & Clipp, 2006; Smith, Kokmen, & O’Brien, 2000; Yaffe et al., 2002). Since the 1980s, with the number of older adults with dementia increasing, the presence of dementia special care units (D-SCU) within NHs has been steadily rising (Lai, Yeung, Mok, & Chi, 2012). Almost 22% of all NHs were found to have D-SCU in 2006, considerably out numbering any other types of special care units including subacute, head trauma, and hospice units (Castle, 2008).
The development of D-SCUs arose in order to facilitate more meaningful social interactions among residents. D-SCUs typically cater to a small number of residents and include distinctive environmental and social features as well as specially trained staff which differ from what is found in traditional nursing homes (TNH). The environmental design of D-SCUs typically includes casual living and activities areas in close proximity to bedrooms, open kitchens, alternatives to traditional nursing stations, and wandering paths (Kovach, Weisman, Chaudhury, & Calkins, 1997; Moore & Verhoef, 1999). D-SCUs can also include environmental features such as homelike decorations, low visual and auditory stimulus, enclosed courtyards, and specially designed social spaces (Campo & Chaudhury, 2011; Grant, Kane, & Stark, 1995; Park-Lee, Sengupta, & Harris-Kojetin, 2013). ‘Specially’ trained staff is a feature of D-SCU that are a part of residential care communities (Park-Lee et al., 2013). Dementia-specific activities and programming usually includes small group activities and sundowning programs (Grant et al., 1995; Park-Lee et al., 2013).
The implication of these special features are that they lead to greater social integration of D-SCU residents as compared to TNH residents. But, it is unknown whether D-SCU residents are receiving equal or greater benefits from living on a segregated unit intended to enhance their social environment and integration through both design and staff involvement because the evidence has shown mixed results. While some studies have found that D-SCU residents spend less time in their rooms and more time in the hall and dining room, and have more social interactions (Kovach et al., 1997), other studies have found no differences. For example, Wood, Harris, Snider, and Patchel (2005) observed residents living on a D-SCU and found that the residents were asocial the majority of the day, had limited conversational exchanges, rarely had a pleasurable affect, and rarely interacted with one another throughout the day including mealtime. In addition, a systematic review evaluating the effects of D-SCUs on residents with dementia and behavioral problems found no evidence of more social interactions (Lai et al., 2009). Moore and Verhoef’s (1999) found that the majority of the time the D-SCU residents were being observed, including during mealtime, they were not interacting with anyone. Additionally, the spaces intended for social interaction (the activity room and the outdoor area) were utilized the least by the residents. However, they did find that if the residents were seated in a structured activity, they were likely to be engaged and socializing with someone. All of these studies have looked at D-SCUs in isolation and there is a dearth of empirical evidence comparing D-SCUs to TNHs when specifically evaluating interactions.
Purpose of study
The purpose of this study is to compare levels of integration between residents living in a D-SCU to a matched group of residents in a TNH using a comprehensive and objective assessment of social integration. The specific objectives of this study are to describe residents’ interactions by observing the: 1) location of interactions, 2) context of interactions (e.g. social, care related, or re-direction), 3) type of interactions (verbal or non-verbal and with whom), 4) quantity of interactions (frequency and duration), and 5) quality of interactions (resident affect). In addition, this study seeks to develop measures useful for comparing social interactions of residents in traditional units with special care to lay the groundwork necessary to measure integration and compare similar residents receiving different types of long-term services and supports.
Methods
Recruitment and sample
We partnered with a single NH provider with a 16-bed D-SCU attached to a 63-bed TNH. All 16 residents living in the D-SCU were eligible to participate in the study. In addition, we sought a comparison group of residents in the TNH. Because the D-SCU had a set of admission criteria, we recognized that there would be differences in some characteristics of the two groups. For example, for individuals to be admitted and remain in the D-SCU, they needed to be continent of both bowel and bladder. With consultation from the staff at the facility, we used the following criteria to find a comparison group of residents in the TNH: 1) medical record diagnosis of dementia, 2) no history of a severe psychiatric disorder, 3) able to follow one step directions, and 4) able to perform at least one of the following behaviors: able to function in a small/group setting; able to focus on an activity or task for at least 10 min with one person assisting; able to be redirected through verbal and/or physical cues. Using these criteria, the Dementia Care Coordinator (DCC) and TNH Social Worker identified 20 residents from the TNH for our comparison group and sought written informed consent from families of both groups. For the combined 36 participants, all but one family provided consent for their relative to participate citing the short time since moving into the facility. The study was reviewed and approved by a federally assured Institutional Internal Review Board.
Residents are placed in either the TNH or the D-SCU when a room becomes available. Internal residents from the assisted living section or the TNH receive priority placement in the D-SCU. A waiting list of external candidates is maintained for the D-SCU for individuals who can afford a private room and have been assessed as meeting the criteria for the program. Additional criteria for entry to the D-SCU include being independently mobile with, or without, an assistive device; and being able to complete all of the following activities of daily living (ADLs) with partial assistance (i.e. verbal, physical, gestural prompts): grooming, dressing, and eating.
The staff/resident ratio was similar across the two environments for some staffing positions, but not all. For example, the ratio for certified nursing assistants (CNAs) to residents is 1:8 in the D-SCU and 1:8.5 in the TNH. One housekeeper was assigned to the 16 D-SCU residents while one housekeeper was assigned to 20–21 residents in the TNH. There was one part time social worker (16 h/week) assigned to the D-SCU and one full time social worker assigned to the TNH for 63 residents. Major differences appear with regard to recreation/activity staffing with the D-SCU having a lower staff/resident ratio. The D-SCU has one recreation staff member work 8–4 pm and a second work 9–5:30 pm with a third person from 3 to 9 pm. The TNH had between 2–3 recreation members during the 9–5 shift and one person from 5 to 9 for 63 residents. However, the recreational positions are not equivalent and have different job descriptions. For example, the recreation staff in the D-SCU serve meals, while the recreation staff in the TNH do not. One nurse manager and one housekeeping manager covered both the TNH and the D-SCU. Finally there was one Director of Nursing who provided support to both environments and a DCC who provided full time support to the D-SCU only.
With regard to staff training, we were told that there were no differences in the required training for staff in both environments. All staff members complete the Center’s for Medicare and Medicaid Services (CMS) modules related to dementia called Hand in Hand: A Training Series for Nursing Homes. However, the DCC joins the D-SCU staff members across all three shifts to lead a discussion after the completion of each module and applies the material to specific residents living in the D-SCU. A similar discussion does not take place in the TNH. The DCC also integrates informal training during meetings on behavior management. For example, what are the best ways to approach resident X and how to observe residents to look for reasons that may be behind a new behavior. Finally, the universal worker philosophy in the D-SCU works to support teamwork across staff. According to the DCC, “we’re all equivalent in the D-SCU. If there is a spill anyone can clean it up, if on the [TNH] you would have to wait for a housekeeper to come clean up a spill.”
Procedures
We utilized three primary data gathering sources, 1) medical charts, 2) visitor logs, and 3) direct observations. Clinical and demographic information was abstracted from participant medical charts and from the Minimum Data Set 3.0 (MDS 3.0) and included the following variables: number of diagnoses, medications, behavioral or mood disturbances in past three months, health service utilization (hospitalizations, emergency department and doctors’ visits), falls in past three months. In addition, visitor logs were reviewed to record the following information for each participant in the study: number of times signed out (leave of absence) in past three months, number of outside visitors in past three months, and the number of unique (different) visitors in past three months. Finally, direct observations of social interactions were used in attempts to objectively measure, describe, and compare social integration between the two groups.
In this section, we detail the procedures for direct observations along with reliability checks for research observers. Five hours of observations per participant were performed between March and May 2013. For each participant, the 5 h of data collection were completed within a three-week period. Observations were 2-h blocks of time across three different time periods and days between the hours of 8 am–8 pm Sunday through Saturday. We believed that weekend observations were important as they are typically excluded from data collection and are often times with less structured activities offered. Three different observation periods were conducted: one morning observation was performed (8–11:59 am), one afternoon observation was performed (after lunch between 1:00 and 8 pm) and one meal observation was performed (lunch or dinner as many residents ate breakfast in their rooms) all on different days.
During each observation period, data collectors followed procedures per instructions for using the Affect Rating Scale (Lawton, Van Haitsma, & Klapper, 1996). For example, observers “positioned themselves to be as unobtrusive as possible while still maintaining a full view of the resident’s face” (p. 7). Observers were also instructed to follow residents wherever they went in the facility, except for following resident’s into their rooms or bathrooms. Observers were given stop watches and instructed to collect the following information: where interaction took place (location), context of interaction (social, care, or re-direction in nature), type of interaction (verbal or non-verbal), who initiated the interaction (resident or other), with whom the interaction occurred (resident, staff, or visitor), number and length of interactions in seconds, and resident affect (anger, pleasure, anxiety, sadness, no affect) using the Apparent Affect Rating Scale (AARS, Lawton et al., 1996). An interaction was defined as any communication between two people that transmitted a message. We included non-verbal interactions, such as a resident motioning to another resident to pass them a tissue as well as verbal interactions where residents spoke. The actual length of the interaction was coded except in instances where the interaction was under 5 s in length. For those interactions, we coded that the interaction was 5 s in length.
The physical layout of the two settings varied in that the D-SCU had an open floorplan so that when residents left their room they could see the dining area, kitchen, and activities area. In contrast, the TNH was a traditional floorplan with longer hallways and a separate dining area divided by a glass wall that is locked when not in use. We coded four main areas for locations of interactions that both settings used (i.e. dining room, common area with a large screen TV, hallways, and resident room). Another difference we noted between the two settings in our field notes was that the D-SCU utilized a universal worker philosophy while the TNH did not.
Multiple observer training sessions occurred prior to data collection. In these trainings, the first author discussed in detail the procedures of observations. Three people were involved in collecting observational data (first and second author plus an undergraduate student). Each observer had a timer, clipboard, and standardized data collection forms. Procedures included being close enough to the participant to view their facial expressions without being obtrusive. For example, observers did not enter participant rooms during times of personal care. But, the interaction was recorded from the time the staff member went into the participant’s room and exited. Observers watched the “gold standard” training video associated with the AARS (Lawton et al., 1996) which includes a practice session of rating older adult’s affect and matching responses to a provided answer key. Three observer reliability sessions were held to assess the comparability of observer reports. During these sessions, all three data collectors observed and recorded interactions on the same individual in either the D-SCU or TNH. Codes were compared and discussed. Coding reliability sessions occurred prior to data collection, and again at one and three weeks into data collection with all sessions continuing until 90% or greater agreement was achieved across the three observers.
Statistical analysis
Cross-tabs with Chi-square were used with categorical variables (e.g. location, context, and type of interaction) to test for differences between the two groups. Independent sample t tests were used with continuous variables (e.g. hospitalizations, quantity and quality of interactions) to test for mean differences between the two groups. Analyses of the observation data were grouped by morning (AM), afternoon (PM), and meal observation times. We did not combine data across the three observation time frames because it would have violated the assumption that the samples are independent (no overlap between group members). We also hypothesized that there would be differences in interactions by time of day and would have lost this nuance if we merged the data.
Results
Comparability of D-SCU and TNH groups
Demographic and clinical characteristics
Comparison of demographic and clinical characteristics of traditional nursing home and dementia special care unit residents (N = 29).
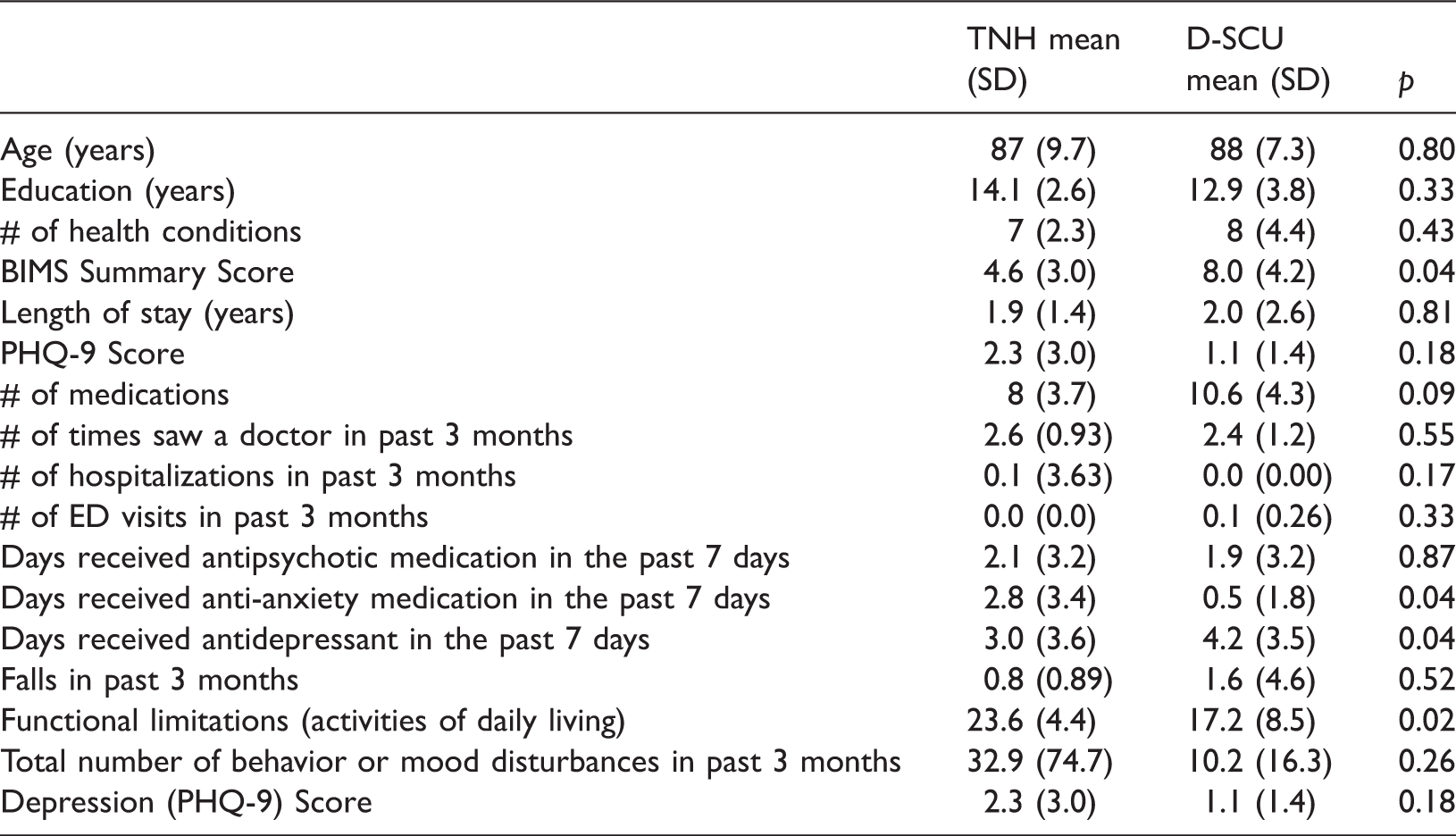
However, there were statistically significant differences between the groups on the Brief Interview for Mental Status (BIMS) summary score (Saliba et al., 2012) and number of days receiving anti-anxiety medications. TNH residents were more cognitively impaired and received more anti-anxiety medications than the D-SCU residents. The groups were also not similar on their ADL scores (the TNH group was more functionally impaired). Specifically, there were statistically significant differences between the two groups on bed mobility, transferring, dressing, toilet use, and personal hygiene. In addition, residents on the TNH were more likely to be incontinent of both bowel and bladder.
Visitor logs
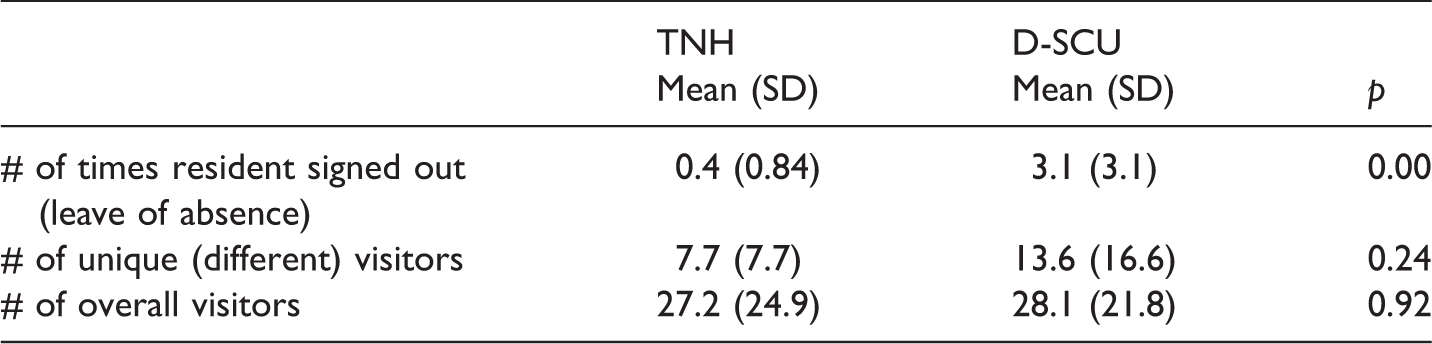
Comparison of visitor log data between traditional nursing home and dementia special care unit residents (N = 29).
Direct observation findings
Over the course of 143 h, we observed 1704 interactions (626 during morning hours; 588 during meals, and 490 during afternoon/evening hours). There was an average of 296 min (4.9 h) of observation per person across three different days (SD 18.78; range 246–320 min). Results are presented below based upon the five descriptive categories of location, context, type, quantity, and quality. First data are presented as combined for all participants and then compared by group (TNH vs. D-SCU).
Location of interactions
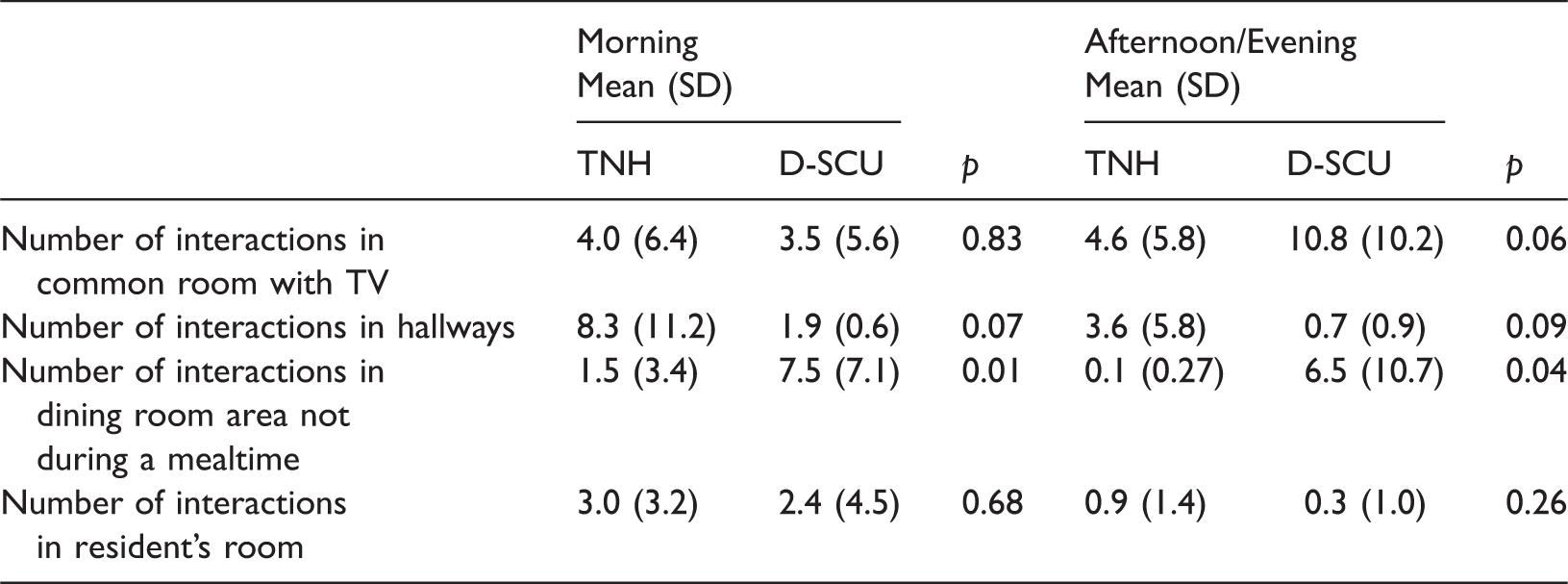
Comparison of observations of location of interactions during morning and afternoon/evening observations by traditional nursing home (TNH) and dementia special care unit (D-SCU) residents (N = 29).
Context of the interaction
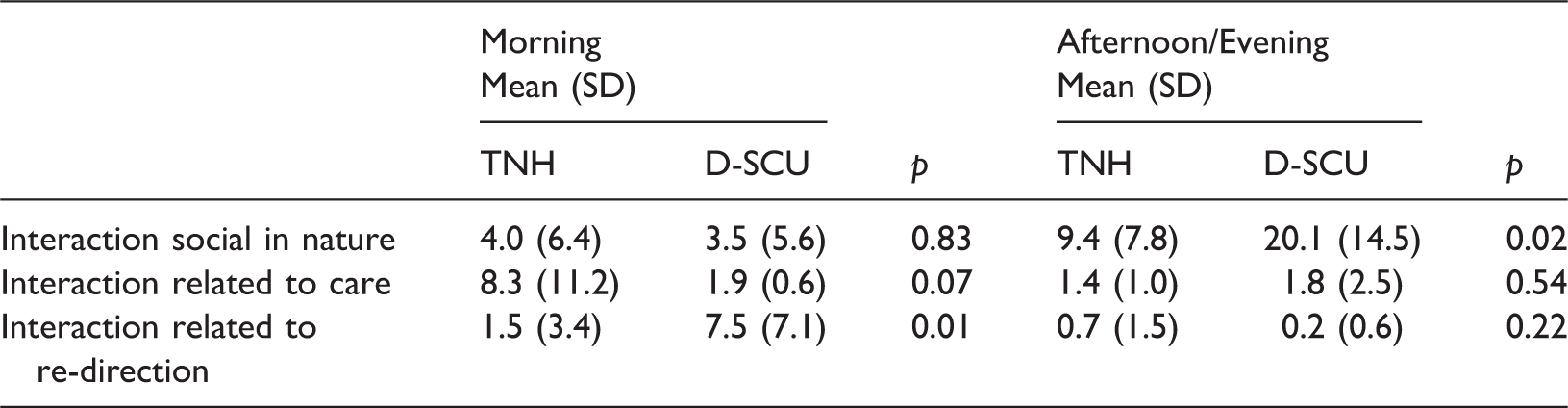
Comparison of observations of context of interaction by traditional nursing home (TNH) and dementia special care unit (D-SCU) residents (N = 29).
Type of interaction
Overall, interactions during the morning and afternoon/evening observations were verbal in nature (93% during both am and pm interactions). When comparing the two groups there were no statistically significant differences. During the morning, TNH residents averaged 95% of interactions being verbal and 89% during the PM observations. D-SCU residents had similar findings with an average of 93% in the am and 97% during pm interactions. The proportion of interactions that were verbal in nature during meals averaged 85% overall with a range of 25–98%. When comparing groups, no statistically significant differences were found with 81% of TNH residents and 88% of D-SCU residents interactions being verbal (p = 0.24).
Comparison of observations of type of interaction (with whom) by traditional nursing home (TNH) and dementia special care unit (D-SCU) residents (N = 29).

Quantity of interaction
Comparison of quantity of interactions by traditional nursing home (TNH) and dementia special care unit (D-SCU) residents during morning and afternoon observations (N = 29).
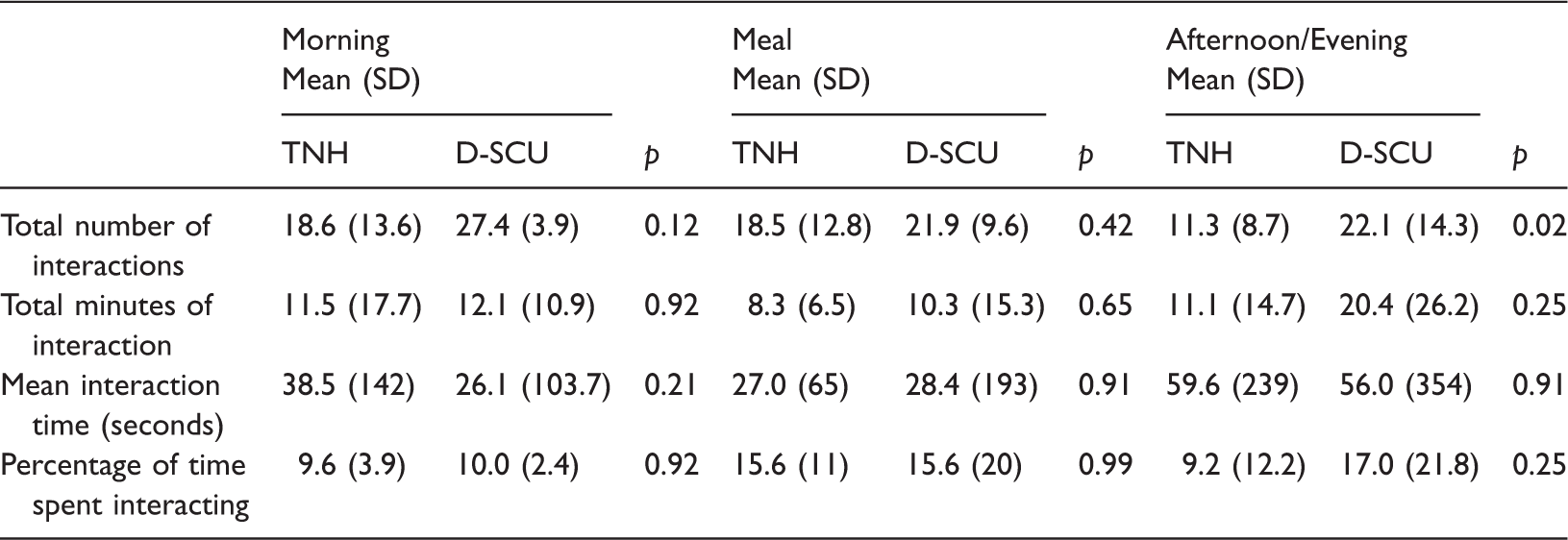
For interactions during meals, we observed 22 residents during lunch and seven during dinner. Ninety percent of residents ate without assistance. Residents were seated at the dining table for an average of 58 min (SD 16 min; range 16–120 min) with at least one other person. Overall, residents had an average of 20 interactions (SD 11.2; range 4–53) during meals lasting 28 s long (SD 150 s; range < 5 s to 58 min). The average total amount of interaction over the course of the meal was 9 min (SD 12 min; median 6 min). Proportionally, this accounted for 16% of their time during meals spent interacting. We found no differences between the groups in the number of interactions or time spent interacting during meals (see Table 6).
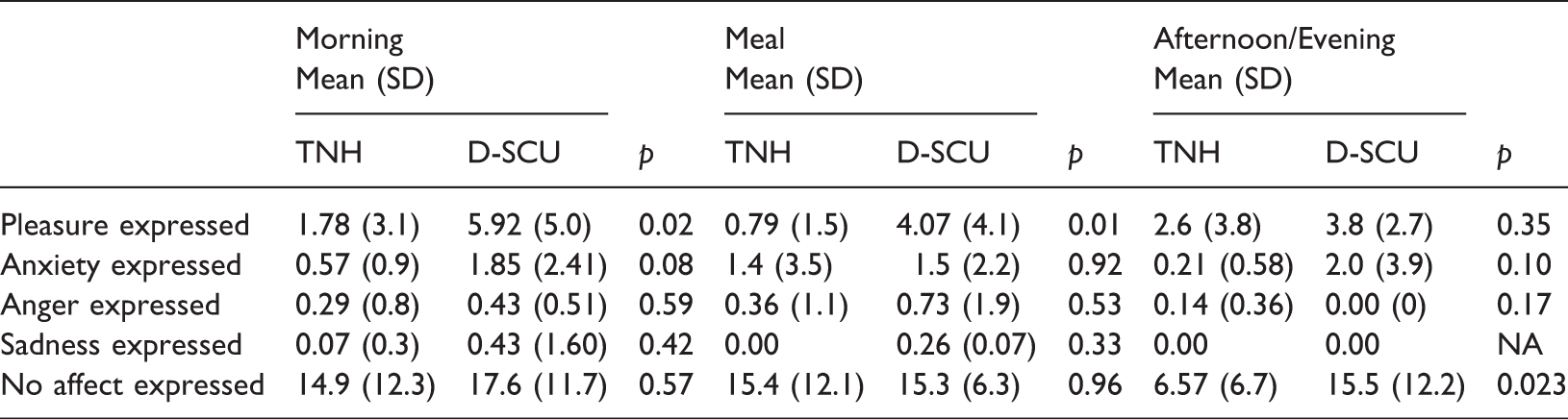
Quality of interaction
Comparison of affect expressed during interactions by traditional nursing home (TNH) and dementia special care unit (D-SCU) residents during morning, meals, and afternoon observations (N = 29).
Discussion
In this study, we observed 1704 interactions over the course of 143 h among 29 residents with cognitive impairment residing in both a D-SCU and a TNH. Overall, the majority of resident interactions were verbal and initiated by staff. Interactions were social in context, and occurred in public areas, such as the common room with a large screen TV. The average interaction was brief lasting less than 1 min and did not change the resident’s affect. While the short duration of interactions can be viewed negatively as ‘small talk’, recent studies have found that brief interactions “promote personhood” among NH residents (Edvardsson, Varrailhon, & Edvardsson, 2014). Promoting personhood is a fundamental aspect of person centered care and functions to recognize the NH resident as a valuable person (Edvardsson et al., 2014).
The finding that NH residents spend a relatively small proportion of their time (10–16%) interacting with other people is concerning because we were observing during the optimal times for interactions. Similar findings have been reported (Burgio et al., 2001; Van Haitsma, Lawton, Kleban, Klapper, & Corn, 1997) indicating the continued struggle facilities face to provide for structured interactions that could develop into friendships. De Medeiros, Saunders, Doyle, Mosby, and Van Haitsma (2011) found that friendships among persons with dementia are possible and that staff can create friendship barriers. Friendships are an essential part of the human experience and can lead to fewer behavioral and psychological problems of dementia, such as agitation (Cohen-Mansfield & Marx, 1993; Cohen-Mansfield, Dakheel-Ali, Jensen, Marx, & Thein, 2012). There are likely individual preferences related to the amount of social interaction each person requires. Future research is needed to identify both individual and group level targets of optimal amounts of social interactions that are a necessary component to developing friendships.
The finding that 93% of interactions were verbal is concerning, especially for residents who are not able to engage in verbal communication. This is a risk factor for social isolation and additional efforts need to be made by staff to interact with residents who are not able to verbally communicate. We hypothesized that having more interactions would lead to fewer behavioral and mood disturbances and/or less depression. However, we did not find any differences between the groups. This may be due to lack of variability as depression scores were low across both groups when compared to a median prevalence of 29% in US NH residents (Seitz, Purandare, & Conn, 2010). The remainder of our discussion focuses on group comparisons to assess our specific research questions.
The common room with a large screen TV is ubiquitous in most NHs and is where we observed the majority of interactions. In our field notes, we identified these locations as areas where staff could keep an eye on residents while they performed their duties. It was also the largest open space allowing for large group activities to take place. One difference between the groups was that residents in the D-SCU had more interactions in the dining area, not during meals, as compared to the TNH residents. We attribute much of this difference to the physical design of the two dining rooms. The D-SCU dining room was part of a large open area while the TNH dining room was down a short hall from the common room, separated by a glass wall, and locked in between meal times. Incorporating environmental design conversations with attention to creating spaces for residents to interact is needed and supported by the theory of person-environment fit (Lawton & Nahemow, 1973).
D-SCU residents left the facility more often than TNH residents. This is likely due to having more mobility and greater continence. However, is leaving the facility a more normal activity that allows residents to feel more socially integrated? Both groups had approximately the same number of visits, but D-SCU residents had more unique visitors than the TNH residents. In other words, the same two people may visit a TNH resident twice a week, while five different visitors would visit a D-SCU resident once a week. This finding may be due to the higher cognitive function among D-SCU residents as well as the more open floor plan of the D-SCU, which is more conducive to visits from groups of people.
Only one significant difference was found between groups in terms of the quantity of interactions. D-SCU residents were observed having more interactions in the afternoons as compared to TNH residents. This finding may be due to the D-SCU activities program, where we observed staff encouraging individuals not to nap in the afternoon, but to attend structured activities. We observed a different tactic in the TNH where staff assisted residents either to the common area with large screen TV or their individual rooms. There were statistically significant differences among D-SCU residents and TNH residents with regard to interactions with staff. D-SCU residents were statistically significantly more likely to have interactions with staff at all times of the day than TNH residents. In addition, these interactions were more likely to be initiated by D-SCU staff.
While nursing personnel staffing ratios were the similar across both units, activities staffing was not. There was a lower staff/resident ratio of recreation staff in the D-SCU. In addition, the D-SCU had a DCC and we did not observe a similar level staff member in the TNH. The DCC was an extra set of eyes and ears who set the tone for the universal worker philosophy in the D-SCU by pitching in to help with serving food and assisting residents when needed. We were informed that all D-SCU staff were expected to help a resident, regardless of their official position. For example, the activities personnel served meals and often sat to eat with residents. Separate dining room staff served meals in the TNH and none of the staff ate with residents. This may have led to our finding of D-SCU residents expressing more positive affect (pleasure) during meals. Activities staff serving lunch and eating with residents have an existing relationship and comfort interacting with persons with dementia. Our field notes indicate that not all staff eating with residents engaged them in conversation. In particular, housekeeping staff typically did not engage in conversations with residents. This observation points to potential staff training opportunities, including housekeeping personnel, to learn how to engage and communicate with persons with dementia.
Studies have shown that it is possible for direct care workers in NHs to engage in a resident preferred activity one-to-one, two to three times per week for 10 min with each session leading to increases in resident positive affect (Van Haitsma et al., 2015). Other studies have found that individualized activity interventions reduce behavioral symptoms and increase positive affect leading to greater engagement in activities (Kolanowski, Van Haitsma, Meeks, & Litaker, 2014). Finally, the NursingHome Toolkit Promoting Positive Behavioral Health was created by a national interdisciplinary team of researchers and clinicians who compiled evidenced-based resources using a person-centered philosophy of care (Kolanowski & Van Haitsma, 2013). This toolkit is a vetted starting point for NH providers who seek a comprehensive repository of initiatives designed to promote the delivery of high quality person-centered dementia care.
Limitations
We recognize that it is not ethically possible to randomize individuals to a D-SCU or a TNH. Therefore, we attempted to compare two groups that were similar based upon diagnosis and behavior characteristics. While the two groups were similar on many aspects (e.g. age, education, number of health conditions, and length of stay) they were significantly different on important clinical characteristics (e.g. function (ADLs), cognition (BIMS). While this was partially expected due to the selection criteria for living in this D-SCU, we recognize that having a more functionally and cognitively impaired comparison group is likely to have affected our results. Future studies using larger samples can consider these characteristics as important covariates or matching criteria. In addition, one week into our data collection a respiratory virus broke out in the TNH and residents were quarantined to their rooms. This had two effects on the study. First, 30% of consented TNH participants passed away before completing the study. Second, the quarantine prevented us from completing contemporaneous observations in both settings as we had planned. We were forced to change our protocol to complete observations in the D-SCU first and then move into the THN once the quarantine was lifted. Third, this was a small, homogeneous sample and our sample size limited our ability to detect statistically significant effects (we had 57% power and the standard is 80%). Replication of this study in additional special care units and longitudinal studies to tease out selection effects versus causation are needed. Finally, we were seeking objective means for measuring social integration and did not include subjective measures from the perspective of the resident or family. Future studies integrating the voice of the older adult regarding their preferences for social connections and integration are necessary.
Conclusions
In conclusion, levels of social integration among NH residents with dementia have not received as much attention as clinical indicators in part because it is a difficult concept to measure. This exploratory study sought to measure social integration through the location, type, context, quantity, and quality of interactions. Findings show that interactions are brief, verbal, and social in nature. Overall, a small percentage of resident’s time is spent interacting with others. When comparing interactions among D-SCU residents and a similar group of TNH residents, D-SCU residents experienced more interactions with staff members, but not interactions of longer duration. D-SCU residents also expressed more pleasure and anxiety than residents in the TNH. Future studies are needed to determine if D-SCU residents experience greater social integration leading to better quality of life outcomes.
Footnotes
Acknowledgements
The authors wish to thank the older adults who participated in this study as well as the employees from the facility who provided guidance throughout the study period.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Justine S. Sefcik was supported by the National Institutes of Health, National Institute of Nursing Research (T32NR009356; Individualized Care for at Risk Older Adults; Principle Investigator, Dr. Mary Naylor).