
Abstract
Depression, agitation, and wandering are common behaviors associated with dementia and frequently observed among nursing home residents. Even with pharmacological treatment, behaviors often persist, hindering quality of life for elders, their family, and paid caregivers. This study examined the use of music therapy for treatment of these symptoms among 132 people with moderate to severe dementia in nursing homes. Participants were evaluated for depressive symptoms, agitation, and wandering to determine their predominate behavior. There were two assessments, two weeks apart, prior to intervention, followed by a two-week intervention, and two follow-up assessments, also two weeks apart. A repeated measures ANOVA determined that after two weeks of music therapy, symptoms of depression and agitation were significantly reduced; there was no change for wandering. Multivariate analyses confirmed a relationship between music therapy and change in neuropsychiatric symptoms associated with dementia. Results suggest widespread use of music therapy in long-term care settings may be effective in reducing symptoms of depression and agitation.
Introduction
Globally, there are 35.6 million people living with dementia (Prince et al., 2013). The prevalence of dementia is rapidly increasing and there are concerns that, without treatments that delay the onset or progression, the occurrence of dementia will reach approximately 65.7 million worldwide by 2030 and 115.4 million by 2050 (Prince et al., 2013). As people age, the risk of having Alzheimer's disease or related dementias increases. One in nine people aged 65 and above have dementia, and about a third of elders above the age of 85 have dementia (Hebert, Weuve, Scherr, & Evans, 2013). People with dementia comprised 39.6% of residential care community residents in 2012 (Harris-Kojetin, Sengupta, Park-Lee, & Valverde, 2013).
The prevalence of neuropsychiatric symptoms in dementia has been estimated to be between 80 and 90% and more than 80% of these symptoms persist for at least 18 months (Steinberg et al., 2004). Neuropsychiatric symptoms such as depression, agitation, and wandering often co-exist in people with dementia with prevalence rates varying from 25 to 80% (Lyketsos et al., 2000). For nursing homes, helping residents who have these symptoms is an ongoing challenge.
Depression in dementia is a collection of symptoms distinguished by the deterioration of the ability to regulate mood and occurs in 15–20% of nursing home residents (Stewart, 2013). Agitation occurs in about 20% of nursing home residents (Morley, 2011) and is one of the most difficult symptoms to manage (Faull, Carter, & Daniels, 2005). Many nursing home residents with dementia exhibit symptoms of wandering, which may lead to adverse outcomes including falls, accidents, injuries, and other potentially fatal results (Beattie, Song, & LaGore, 2005). Appropriately managing these neuropsychiatric symptoms is essential to reduce distress for people with dementia and their paid and family caregivers (Ballard & Fossey, 2007).
Treatment for the symptoms of dementia includes pharmacological and nonpharmacological interventions. There are nonnegligible risks of side effects of antipsychotic medication for behavioral and psychiatric symptoms related to dementia, including dizziness and fatigue that can result in injuries (Blackburn & Bradshaw, 2014).
Music therapy as a nonpharmacological treatment
Nonpharmacological interventions, such as music therapy, that are person centered may be the most effective psychological approach to long-term improvement in neuropsychiatric symptoms reduction (Sjogren, Lindkvist, Sandman, Zingmark, & Edvardsson, 2013). These interventions can provide a low cost alternative to medication to reduce behavioral disturbances (Raglio, Filippi, Bellandi, & Stramba-Badiale, 2014).
Several meta-analyses and literature reviews have concluded that nonpharmacological treatments, including music therapy, have been effective with behavioral and psychological symptoms of dementia (Beard, 2012; Patel, Perera, Pendleton, Richman, & Majumdar, 2014; Ueda, Suzukamo, Sato, & Izumi, 2013). Music therapy is not a curative measure for dementia but has been shown to decrease symptoms; multiple meta-analyses have determined that music therapy is a safe, humane intervention, with effects on measures of behavior that are similar to those of regularly prescribed psychiatric interventions (Koger & Brotons, 2000; Opie, Rosewarne, & O'Connor, 1999; Sherrat, Thornton, & Hatton, 2004). In a literature review, Patel et al. (2014) included several rigorous studies that demonstrated the effectiveness of music therapy in reducing behavioral and psychological symptoms of dementia. Another review of the literature that evaluated six studies that suggested music therapy was a promising nonpharmacological intervention and concluded that music therapy has the potential to reduce anxiety, agitation, and depression at a low cost (Blackburn & Bradshaw, 2014). In a systematic review and meta-analysis, Ueda et al. (2013) concluded that music therapy had small but statistically significant effects on depression and moderate effects on anxiety.
Music therapy has been growing in popularity as a means to alleviate common symptoms associated with dementia (Guetin et al., 2013). A study that compared music therapy with education or entertainment found that the music therapy group experienced fewer delusions, less agitation, anxiety, apathy, irritability, motor restlessness, and fewer night-time disturbances (Raglio et al., 2008). Individual music therapy for nursing home residents with dementia has been shown to decrease agitation and aid in prevention of psychotropic medication use (Ridder, Stige, Qvale, & Gold, 2013). Involvement in music-based programs for nursing home residents with dementia can offer social opportunities, and engaging in various types of music activities such as movement, rhythm-based programs, and singing may all lead to lessening of agitated and depressive symptoms. Music may be the only activity in which nursing home residents can experience social interaction (Hanser & Clair, 1995).
Music therapy and depression in dementia
It is important for people with dementia to be provided with a creative outlet for expression, especially during times of distress, dysfunction, and deflated mood that often occurs due to the diagnosis. For people with dementia, music therapy leads to feelings of positive self-esteem, increases feelings of competence and independence, and diminishes feelings of social isolation (Sixsmith & Gibson, 2007). In several randomized controlled trials, depression was significantly reduced in the group that received music therapy (Albornoz, 2011; Chu et al., 2014). In 2000, Ashida used music therapy techniques such as reminiscence with familiar songs for people diagnosed with dementia who had symptoms of depression and found, in a pre–post test analysis, that after five sessions of small group music therapy, symptoms of depression were significantly reduced.
Music therapy and agitation
Similar to findings regarding depression, studies have shown that music therapy can decrease symptoms of agitation (Narme et al., 2014; Sung & Chang, 2005). Music therapy may provide a safe and active environment that meets the social and emotional needs expressed by people with dementia who demonstrate agitated behaviors (Ledger & Baker, 2007). Sung, Chang, Lee, & Lee (2006) presented results indicating that the number of agitated behaviors was significantly reduced after music therapy. Through both quantitative and mixed methods studies, researchers observed a short-term reduction in agitation after the use of music therapy (Brotons & Marti, 2003; Ridder et al., 2013; Svansdottir & Snaedal, 2006). Ledger and Baker (2007) evaluated the long-term effects of music therapy on agitation and concluded that while music therapy reduced agitation for short periods of time, there were no significant differences in the frequency, range, and severity of agitation between the control and treatment groups over the long term.
Music therapy and wandering
The effect of music therapy on wandering in people with dementia has been studied with varying outcomes. In a randomized controlled trial, Raglio et al. (2008) discovered that after eight weeks of music therapy, the experimental group demonstrated fewer symptoms of wandering and other behavioral and psychiatric symptoms of dementia. Groene (1993) found that participants wandered significantly less in music therapy groups when compared to reading groups. On the other hand, Raglio et al. (2008) reported that the control group experienced less wandering in comparison to the experimental group that received a music therapy intervention.
Despite the numerous studies that have suggested music therapy's efficacy in decreasing neuropsychiatric symptoms in dementia, few have provided adequate descriptions of methods or analysis (Vink, Birks, Bruinsma, & Scholten, 2004). Other previous reports have not sufficiently described the intervention, did not use validated outcome measures, or provided insufficient descriptions of the process by which music therapy aided in changing behaviors (Beard, 2012; de Medeiros & Basting, 2014).
Conceptual framework
The conceptual framework for this study is the need-driven, dementia-compromised behavior model NBD, which is based on clinical observations that troublesome behaviors expressed by individuals with dementia indicate an unmet need (Penrod et al., 2007; Song & Algase, 2008). Researchers and practitioners can view these behaviors as a way to “aid them in identifying persons at greatest risk (for disruptive behaviors and try to fulfill those needs) with highest likelihood of precipitating these behaviors” (Algase et al., 1996, p. 10). Once these individuals and their needs are identified, researchers can test the effects of interventions in addressing the need-driven dementia-compromised behaviors (Algase et al., 1996).
The model posits that behaviors derive from the interaction of risk factors including cognitive and physical deficits and the physical and social environment (Kolanowski et al., 2011). The model suggests that the caregiver should try to understand the identity of the person with dementia, and the way in which his or her current cognitive status may interfere with their ability to interact with others (Penrod et al., 2007), an important step for the therapeutic process.
Clinical experience suggests that music therapists have been successful using this approach through activities that take into account the nursing home resident's background and/or historical patterns of behavior. Nursing home residents who were provided with therapy that connected with their backgrounds and focused on historical patterns of behavior had higher levels of engagement, decreased negative behaviors, and improved effect in comparison to residents whose social and personal histories were unnoted (Penrod et al., 2007). The need-driven dementia-compromised behavior model suggests providing individuals with activities appropriate to their cognitive and physical abilities and their personal interests (Kolanowski et al., 2011).
In this report, we provide a detailed description of a music therapy intervention for nursing home residents with dementia, including the specific methods used to alleviate several of the most troublesome behavioral symptoms of dementia. This study was designed to answer the research question: Will participation in small group music therapy reduce the level of depressive symptomatology, agitation, and wandering behaviors with sustained effects for two weeks posttreatment among skilled nursing home residents with moderate to severe dementia? In addition, we sought to examine whether changes in depressive symptoms, agitation, and wandering behaviors were related to age, gender, dose of intervention (as measured by music therapy attendance), or level of impairment.
Method
Setting and design
This study used an exploratory design, in which each individual was his own control, to evaluate the effectiveness of music therapy on depressive symptoms, agitation, and wandering. Modeled after previous studies by Buettner and Fitzsimmons (2014) who used this design to measure changes in agitation in people with dementia, this study compared the effects of two weeks of usual care with a two-week music therapy intervention and a two-week period after music therapy ended to determine immediate and lingering effects of the intervention. To protect the validity of the study, the tester did not take part in the intervention nor was there any prior relationship with the participants.
The research protocol was as follows:
Screen and recruit of participants. Obtain signed consent from participants' legal representatives. Gain assent from participants. Perform baseline assessment to determine dominant behavior. Two weeks of treatment as usual. Repeat assessment of dominant behavior performed at baseline. Music therapy intervention for two weeks. Repeat assessment of dominant behavior. Two weeks no intervention. Repeat assessment to measure sustainability of effect of intervention.
In order to be eligible, participants had to exhibit at least one of the three problem behaviors. Screening for consented residents was accomplished by the project director using Reisberg's Functional Assessment Screening Test (FAST) (Auer & Reisberg, 1997). Only participants who scored a five or higher on the FAST, indicating dementia severity of moderate or greater, were considered eligible for inclusion in this study.
Sample
Convenience sampling was used for study recruitment and participation (N = 132). The New York University School of Medicine Institutional Review Board approved the protocol for this study. Residents were recruited by the study investigators from three nursing homes: Menorah Center for Rehabilitation and Nursing Care, the former Shorefront Center for Rehabilitation and Nursing Care, and the former Metropolitan Jewish Geriatric Center, all located in Brooklyn, New York, and owned by Metropolitan Jewish Health System (MJHS), a not-for-profit health system.
Demographic characteristics of the sample (n = 132).

Mean age = 89.6, range = 59–101.
Instrumentation
The Cornell Scale for Depression (CSD) is a 19-item assessment tool that is designed to measure severity of depressive symptoms (Kurlowicz, Evans, Strumpf, & Maislin, 2002). Several studies confirm that the scale has a high level of concurrent validity compared with similar measures of depression in older adults with dementia (Amuk, Karadag, Oguzhanoglu, & Oguzhanoglu, 2003; Barca, Engedal, & Selbaek, 2010; Williams & Marsh, 2009) and has been found to be reliable with nursing home residents (Barca et al., 2010).
The Algase Wandering Scale (AWS) is a 28-item questionnaire that assesses five dimensions of wandering with moderately strong interreliability (Algase, Beattie, Bogue, & Yao, 2001). Validity of the questionnaire is supported by its ability to distinguish between wandering and nonwandering behaviors (Algase et al., 2001).
The Cohen Mansfield Agitation Inventory (CMAI) has been used in studies in long-term care facilities. The assessment tool was evaluated with nursing home residents (n = 105); test/retest reliability was moderate to good, but interrater reliability varied (Zuidema et al., 2011).
The FAST has been found to be a reliable brief rating scale to evaluate severity of functional abilities and activities of daily living throughout the stages of Alzheimer's disease (Na et al., 2010). In 2010, Na et al. found statistically significant correlations between Clinical Dementia Rating-Sum of Boxes, the Global Deterioration Scale, the Mini-Mental Status Examination, the Barthel Activities of Daily Living, and the FAST determining that the FAST is a reliable and valid assessment technique to be used with people in varying stages of dementia. A systematic review that included 23 articles and 6109 participants aged 65–87 concluded that the FAST has a history of reliability and validity in assessment of stages of dementia (Olde et al., 2011).
Characteristics of participants
Participants served as their own controls. They were tested at baseline using three instruments: CSD, CMAI, and AWS. At baseline, the range for CSD scores was 1–21, for CMAI 34–128, and AWS 32–74. Following baseline assessments, each individual's scores were compared across behaviors. Since many individuals exhibited multiple symptoms of depression, agitation, and wandering, they were selected for a specific group based on relative severity. To determine this, CSD, CMAI, and AWS scores were entered into Excel where they were converted into percentages of the total number of symptoms that were based on each scale. For each additional data point, we collected scores only for each individual's identified dominant behavior. Participants whose scores indicated an absence of depressive symptoms, agitation, and wandering were not included in this study. At baseline, we found a strong positive correlation between number of agitation and depressive symptoms, r (130) = .429, p < .001 and a weaker positive relationship between wandering and depressive symptoms, r (130) = .260, p = .003. The relationship between agitation and wandering was not statistically significant, r (130) = .111, p = .204. The participants were assigned to one of three study groups: depressive symptoms, agitation, or wandering, based on the highest score obtained.
A total of 330 nursing home residents were screened for this study: of these, 180 were ineligible because of mental health diagnoses, health status, or research staff's inability to gain informed consent from legal representative. Of the 150 participants who initially began this project, four were discharged prior to the study, four passed away before the study began, two were unable to continue due to health issues, one was transferred to another facility, and seven others did not present with neuropsychiatric symptoms at baseline assessment. One hundred and thirty two (88.7%) completed the study. The majority of the participants were female (n = 112, 84.8%), which reflects the MJHS nursing home population as a whole. The sample was elderly (mean = 86.9 years, SD = 7.29), with the youngest aged 58 years and nine months and the oldest 101 years and three months. Upon project initiation, all participants scored within the moderate to moderately severe dementia range according to FAST; score results (mean = 5.63, SD = 1.09). The most common target behavior among participants was symptoms of depression (n = 71, 53.8%), followed by wandering (n = 33, 25.0%), and then agitation (n = 28, 21.2%).
Intervention
A therapeutic program utilizing preferred music therapy for participants with mid-stage dementia was developed for this study. The sessions were held three times a week for two weeks, a total of six sessions, in a private lounge in the nursing home.
Music selection
Sample of music selected for individual and group therapy.
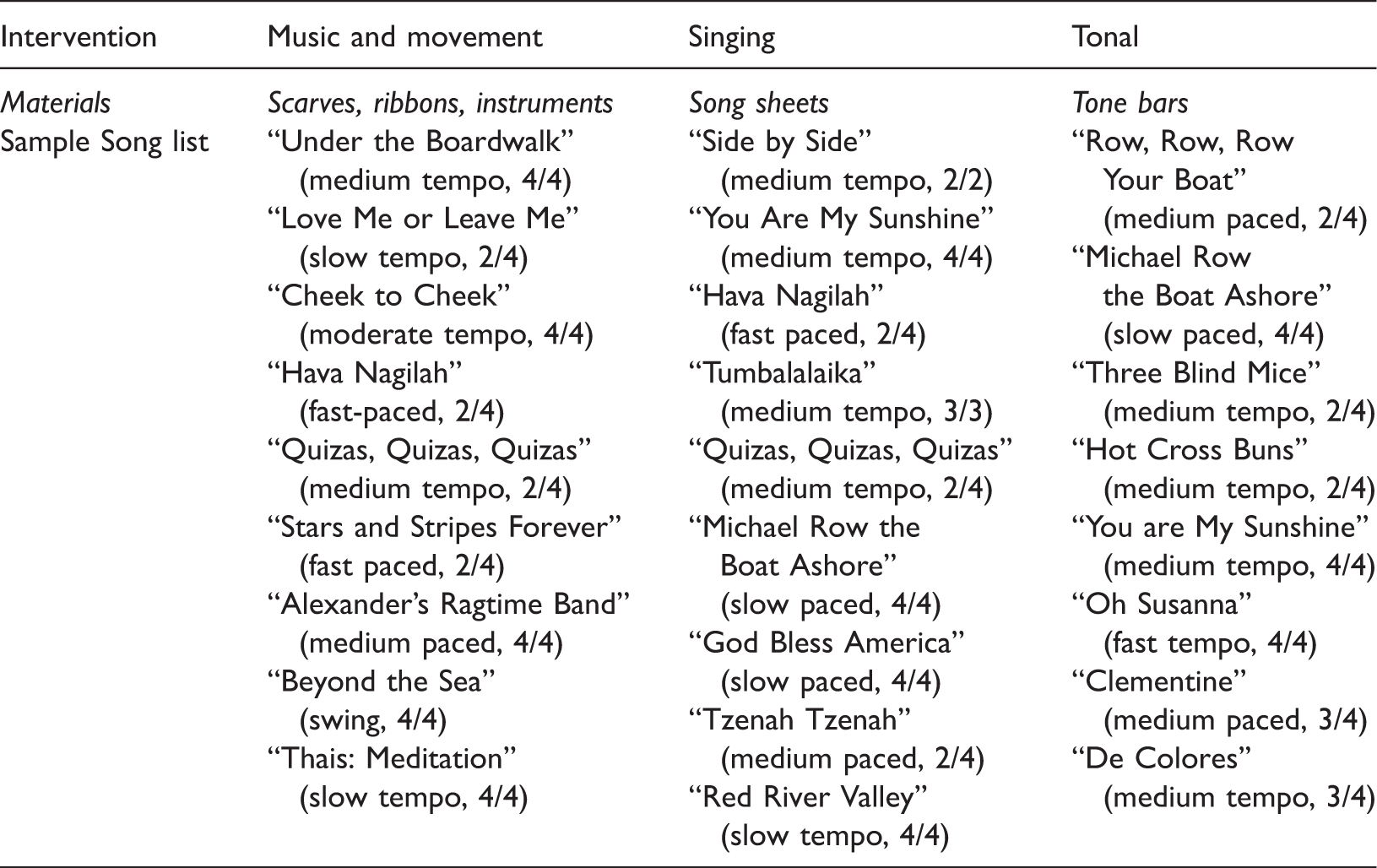
Materials
The music therapist utilized a Martin 6-string acoustic guitar, Yamaha keyboard, several types of rhythm instruments, colorful scarves, Remo djembe drums, ocean drums, and sheet music. For music and movement therapeutic sessions, rhythm instruments such as hand bells, Basic beat egg shakers, tambourines, scarves, and ribbons were used. Tonal sessions involved selected instruments: Sonor contra and contra bass tone bars—C & G, and Basic beat tone bars.
Structure of therapy
Music therapy was conducted in groups for almost all individuals (n = 129, 97.7%), The groups consisted of between four and six participants, each of whom exhibited at least one of the symptoms—depression, agitation, or wandering, and lasted from 15 min to 1 h depending on the participant's tolerance level. Participants were free to leave at any time. Support was provided if assistance was required to relocate to residents' preferred area. Consideration was given to participants' schedules and did not interfere with meals, appointments, recreational activities, or other types of therapy. Three participants who were unable to attend group sessions were provided individual music therapy. For one participant, a hearing device contributed to problematic issues with crowd noise. The two others requested individual sessions, stating a preference not to socialize with others in a group setting. They were historical loners.
The content of the music therapy sessions was based on target behaviors of the members of each group. The residents with depressive symptoms, agitation, and wandering were placed in the same small music therapy group. Since groups were made up of only an average of 4–6 residents, music therapists were able to address targeted behaviors of each individual member. The goals for the residents with depressive symptoms were to increase socialization and develop relationships between the therapists and peers to decrease isolation and improve mood. For individuals who exhibited agitation and wandering symptoms, the therapists sought to both focus their attention on the here and now and remove any distress. The music therapists used receptive therapy techniques to relax individuals who were agitated or restless, reflect on memories related to familiar songs, and aid in improving the mood of the participants who exhibited depressive symptoms (Maratos, Gold, Wang, & Crawford, 2008). The therapists attempted to reduce the needs expressed by agitated and wandering behaviors through singing, rhythm, and movement therapeutic activities with the goal of stimulating a body/mind response that may occur through memory associated with a familiar song an individual finds soothing (Craig, 2014; Gerdner, 2012). Recurring themes that arose included grief, loss of a loved one, and coping with an illness. The sessions included improvisation and entrainment, a procedure in which the therapist provides rhythmical synchronization for the group in order to shift states of agitation or mood. Sessions integrated: music and movement, singing, and tonal activities. The intervention was structured as follows:
Music was selected prior to all group sessions based on assessment of musical preferences of individuals in the group; Introduction (Musical Greeting); Therapeutic Music and Movement, Singing or Tonal Activity; Music and movement: With the assistance of music played on guitar or keyboard, participants engaged in movements beginning with a slow pace followed by medium paced to fast to a return to slow while utilizing scarves, body, or rhythm instruments. Tempo of music reflected engagement in movements. Singing: Therapist prepared song list prior to meeting with participants. Lyrics to songs were distributed to participants as needed. Therapist engaged residents in playing instruments and singing songs and talked with participants about the music addressing individual needs such as mood or agitation. Ask questions such as (a) “What does the music make you think of?”; (b) “Does this music seem familiar to you?”; (c) “What kind of music is this?” Tonal: The tone bars used are handheld instruments that are played by striking with a mallet. The colored tone bars used for these groups ranged from middle C to an octave higher. Therapist demonstrated use of tone bars prior to introducing song selected for singing along with playing tone bars for each group. Discussion of music presented; reminiscence of memories ignited (occurs throughout therapeutic intervention); Short reflection of therapeutic experience (Participants asked: “Did you enjoy the music therapy?”).
Analysis
Repeated measures ANOVAs with post hoc tests for depressive symptoms, agitation, and wandering.
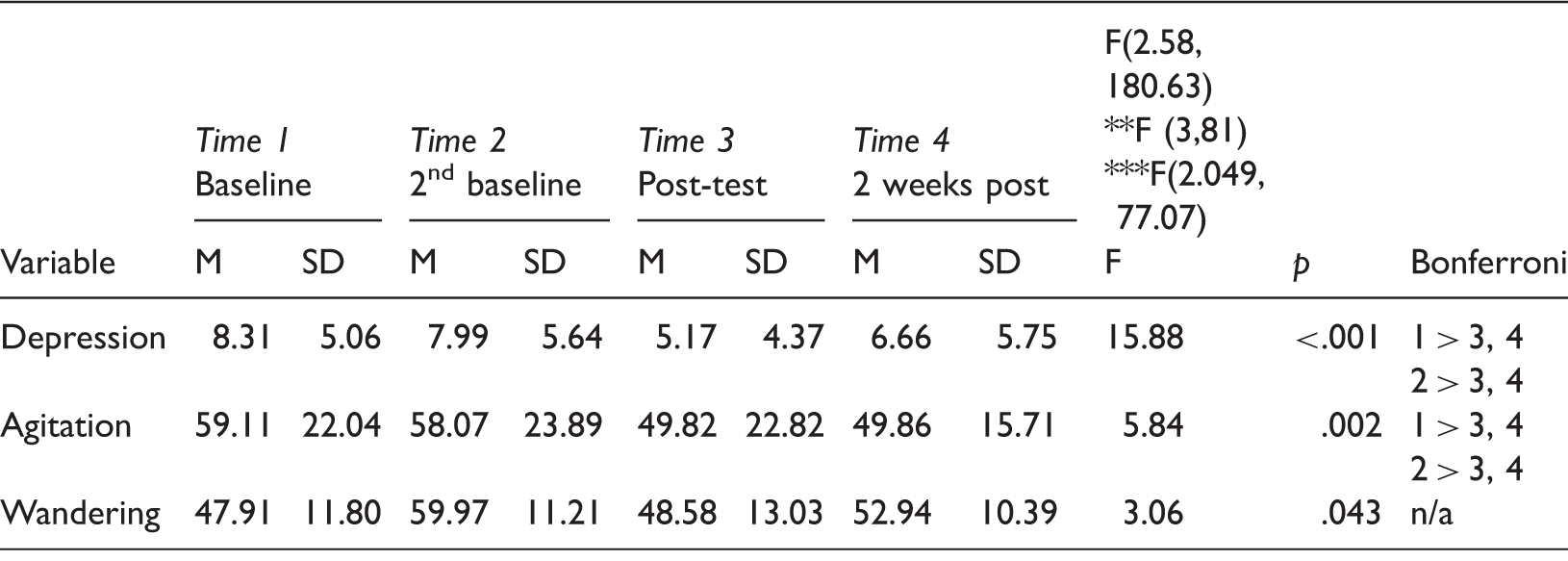
Note: Bonferroni correction used to indicate which time periods were statistically significantly different.
**F value for agitation, ***F value for wandering.
There are risk factors that may contribute to changes in depressive symptoms and agitation (Cooke, Moyle, Shum, Harrison, & Murfield, 2010; Heun & Hein, 2005) other than the addition of a music therapy intervention. In order to examine the potential influence of these risk factors on outcome, a series of multiple regression analyses were performed with the CSD, CMAI, and AWS postintervention scores as the dependent variables and the CSD, CMAI, and AWS baseline scores, age, gender, dose as documented by attendance, and severity of impairment measured using FAST scores as the independent variables. Gender was coded as female=0, male=1, and severity of dementia was coded as moderate (FAST 5) = 0 and moderately severe (Fast 6) = 1.
Results
The results for each analysis are specific to the targeted symptom. Outcomes are presented in sections to reflect separate analyses for depressive symptoms, agitation, and wandering behaviors.
Changes in symptoms of depression
A repeated measures ANOVA determined that mean depression scores differed significantly between time points. Mauchly's test of sphericity indicated that the assumption had been violated, x2 (5) = 17.06, p = .004; therefore, a Greenhouse–Geiser correction determined the results, F (2.58, 180.63) = 15.88, p < .001. Post hoc tests using the Bonferroni adjustment revealed that depressive symptoms decreased slightly from first to second baseline (8.31 ± 5.06 versus 7.99 ± 5.64), which was not statistically significant (p > .05). However, depressive symptoms reduced to 5.17 ± 4.37 following the music therapy intervention, which was statistically significant (p < .001) and increased slightly, but not significantly two weeks following the intervention (6.66 ± 5.75, p = 0.05). This increase remained significantly lower than baseline scores (p = .006). These results suggest that participation in two weeks of music therapy significantly reduces symptoms of depression and maintains these changes for at least two weeks posttreatment (Table 3, Figure 1).
Graph displaying progression of Depression Scale (CSD) scores from baseline to immediately to two weeks after music therapy. (Figures are graphical representation of study data. Created using IBM SPSS 21.)
Changes in symptoms of agitation
As with the depressive symptoms analysis, we used repeated measures ANOVA to investigate differences between time points. The assumption of sphericity was met as assessed by Mauchly's test of sphericity, x2 (5) = 3.86, p = .570. The Mauchly's test of sphericity showed that mean agitation scores differed significantly between time frames F (3, 81) = 5.84, p = .002. The Bonferroni adjustment for multiple comparisons determined that there were no significant differences in scores between first and second baseline (59.11 ± 22.04 versus 58.07 ± 23.89, respectively). Similar to the depressive symptoms, agitation was reduced significantly immediately following music therapy (49.82 ± 22.82), p < .05. We measured agitation scores two weeks after the conclusion of the intervention and found that the scores had not changed much (49.86 ± 15.71, p > .05) but were still significantly lower than at baseline (59.11 ± 22.04, p = .018) suggesting that the two-week intervention had immediate and lingering effects on agitation (Table 3, Figure 2).
Graph displaying progression of Agitation Scale (CMAI) scores from baseline to two weeks after music therapy.
Changes in symptoms of wandering
For wandering, Mauchly's test of sphericity indicated that the assumption had been violated, x2 (5) = 11.24, p = .047. The Greenhouse–Geisser was used to correct the repeated measures ANOVA. The test with correction found that mean wandering scores did significantly differ between first to second baseline, baseline to posttest, and posttest to two weeks following the intervention F (2.049, 77.07) = 3.06, p = .043 with wandering increasing significantly over the entire time period. However, the Bonferroni post hoc test determined that the differences between successive time periods were not statistically significant (47.91 ± 11.80 versus 50.97 ± 11.21 versus 48.58 ± 13.03 versus 52.94 ± 10.39). From first baseline (47.91 ± 11.80) to second baseline the wandering scores increased (50.97 ± 11.21) though not significantly, p = .672. The scores decreased from second baseline (50.97 ± 11.21) to posttreatment (48.58 ± 13.03), p = .624. Overall, the music therapy intervention was not effective in lessening symptoms of wandering for this group, p < .05 (Table 3, Figure 3).
Graph displaying progression of Wandering Scale (AWS) scores from baseline to two weeks after music therapy.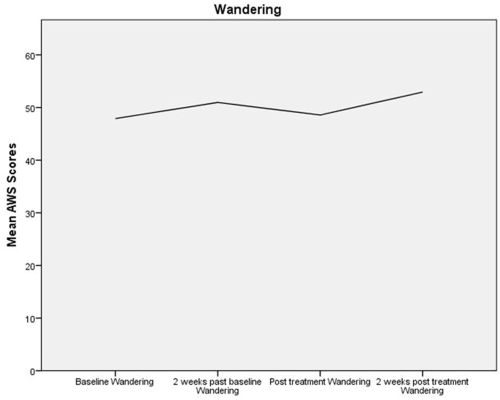
Multivariate analyses: Symptoms of depression, agitation, and wandering
Each multiple regression model incorporated age, gender, level of impairment, dose, and baseline CSD scores. For depressive symptoms, the adjusted R 2 was .333, F (5, 65) = 6.49, p < .001. The standardized coefficients β were: depressive symptoms score β = .374 (p < .001), age β = −.035 (p = .538), gender β = −1.287 (p = .319), dose β = −1.081 (p = .047), and level of impairment: β = 1.238 (p = .344). As demonstrated in Table 4, participants who engaged in music therapy were found to have lower depressive symptoms, after controlling for gender, age, dose, and level of impairment (Table 4). Dose, the number of times Dose, the number of times participants received music therapy, significantly predicted posttreatment depressive symptoms, p = .047.
Multiple regression of symptoms of depression, agitation, and wandering scores with risk factors among 132 nursing home residents with dementia immediately following a music therapy intervention.

Note: *p < .05.
Like symptoms of depression and agitation, a multiple regression analysis was performed for wandering. The adjusted R2 was .629, F (5, 27) = 9.148, p < .001. The standardized coefficients β were: wandering score .833 (p < .001), age −.020 (p = .946), gender 4.50 (p = .296), dose .037 (p = .970), and level and impairment 1.056 (p = .913). Gender, age, dose, and level of impairment did not contribute to the change in wandering (Table 4).
In summary, from the results of both the multiple regression analyses and the repeated measures analysis of variance, we can conclude that the music therapy intervention significantly reduced symptoms related to depression and agitation. The multiple regression analysis indicated that the only other factor to influence depressive symptoms was dose; the number of times music therapy was provided significantly influenced depressive symptoms.
Discussion
The use of music therapy for neuropsychiatric symptoms of dementia has been widely studied in observational trials for decades. As a nonpharmacological treatment it is recommended as an intervention to reduce behavioral symptoms (Patel et al., 2014; Ueda et al., 2013), though there is little research that documents the procedures undertaken for the intervention and many music therapy researchers use the one-size-fits-all method for interventions prescribed (Beard, 2012). In the current study, we examined the use of therapeutic singing, music and movement, and a tonal protocol specifically created for individuals with moderate to severe dementia in long-term care settings. Our findings revealed that when compared to usual care, our music therapy intervention reduced symptoms of depression and agitation but not wandering behaviors. Our results suggested that the music therapy interventions had effects on symptoms of depression and agitation, over and above any medication effects. We believe this evidence has important implications for music therapy practitioners' and long-term care professionals' consideration of music therapy as a nonpharmacological treatment.
The music therapy interventions, e.g. singing, tonal, and music and movement sessions, were constructed by the research music therapists to be sensory stimulating and involve the participant's musical preferences. Previous studies imply that playing music that is preferred for someone with dementia decreases agitation as measured by the CMAI (Hicks-Moore, 2005; Ridder et al., 2013; Sung & Chang, 2005; Sung, Chang, & Abbey, 2006). The therapeutic activities in this study were designed especially for nursing home residents with moderate to late stage dementia for individual or small groups as advised in previous studies (Aldridge, 1994; Heyn, 2003). The results of this study reinforced recommendations from Gfeller and Hanson's (1995) randomized controlled trial that using rhythm-based and physical music programs significantly affect behaviors that are impacted by dementia. Participants were asked to perform gentle movements while listening and/or singing to a live version of their preferred music. The results of our study indicate that participation in an intervention that involves music and movement, singing, and tonal programs can decrease the occurrence of neuropsychiatric symptoms considered by staff and family as negative behaviors.
The music therapy intervention provided an opportunity for self-expression through verbal and nonverbal modes using music and movement, singing, and tonal therapeutic activities. The positive effects may have occurred both because of the music therapists' focus on individual music preferences and from the provision of physically and cognitively stimulating activities, a recommendation of the NDB (Kolanowski et al., 2011). The need of the participants may have been met by the music therapists' acknowledgement of each individual's background and historical pattern by singing familiar songs and reminiscing about family relations, employment, or childhood memories, but any short-term benefits of the intervention occurred without sustained effects, leading to individuals reverting to usual wandering patterns.
Depressive symptoms
Our study suggests that only two weeks of music therapy intervention are necessary to effectively reduce symptoms of depression both immediately after and at least two weeks. This is consistent with a randomized controlled trial by Chu et al. (2014) that demonstrated that music therapy decreased depression, although one month following the intervention, improvements began to dwindle. Our findings also corroborate those of a study by Erkkila et al. (2011) that determined in a randomized controlled trial that participants with depression symptoms who received music therapy in comparison to those who received standard care showed greater improvement.
For the participants who exhibited symptoms of depression, dose was an important factor in predicting positive outcomes. Our aim was for each person to attend six sessions within the two-week time frame. The average attendance was five sessions with varying lengths and types of sessions that were provided depending on the needs of the residents. From our analyses, it is clear that the more music therapy offered, the better the short-term and long-term outcomes for people with moderate dementia with depressive symptoms.
Agitation and wandering
Gerdner (2012) describes agitation as inappropriate verbal and motor activity that occurs without explanation. In this study, we hypothesized that agitation and wandering (unexplained motor activity) would both be lowered in our study participants following music therapy. Our participants often exhibited behaviors including resisting care, incomprehensible verbalizations, hitting, screaming, etc. that may be nonverbal expressions of discomfort. These behaviors can be distracting to other residents and may interfere with quality of life. Our study demonstrated the positive effects of providing an opportunity for participants who exhibit agitated behaviors to experience a relief in discomfort through therapeutic programs such as singing using their preferred music. These results corroborate the findings of several other studies that found that music therapy was effective in reducing agitation in people with dementia (Hicks-Moore, 2005; Ridder et al., 2013; Sung & Chang, 2005; Sung et al., 2006). From our observations, the results positively affected not only the participant as evidenced by fewer symptoms but may have impacted other nursing home residents living in close quarters.
Our results signal that music therapy is an effective treatment for agitation in people with dementia and that these improvements can be sustained for at least two weeks following the music therapy intervention. This is in concert with Livingston and colleagues' (2014) review of three randomized controlled trials that found short-term reductions in agitation immediately following music therapy.
For wandering, there was no greater change with music therapy than there was from first to second baseline when participants were receiving treatment as usual. It is possible that we found no effect on wandering at least in part due to the inability of staff to recognize the need represented by wandering behaviors. In many nursing home settings, wandering is not perceived as a tolerable behavior due to the consistency of staff monitoring and safety concerns, but for people with dementia the act may be purposeful, an expression of a need-driven behavior.
The NDB model states that in order to provide appropriate treatment for cognitively impaired individuals, the need must be understood (Algase et al., 1996). Some researchers believe that wandering may be goal directed with intent. Wandering behavior may be caused by emotional and/or physiological problems, which are often not apparent to caregivers (Cipriani, Lucetti, Nuti, & Datti, 2014; Coltharp, Richie, & Kaas, 1996). In this study, the music therapy researchers noticed increased attention to task, observable instances of pleasure, and decreased motor activity. This suggests that some of the wandering behavior caused by irritation, depression, or anxiety (Yokoi, Aoyama, Ishida, & Okamura, 2012) may have been addressed during the music therapy sessions, despite the lack of overall significant effect. Cipriani et al. (2014) suggest that wanderers should be provided with a safe and pleasant environment that allows them to wander. Further, the use of nonpharmacological interventions such as music therapy is a practical and morally acceptable intervention to aid wanderers (Cipriani et al., 2014).
Limitations
One possible limitation of this study is the internal validity of the test results. At each data point the assessments were completed with assistance from the certified nursing assistants assigned to the residents. While it is possible that the certified nursing assistants rated the symptoms of depression, agitation, and wandering as less of a problem at the follow-up assessments due to knowledge of the residents' participation in the study, it is unlikely that this occurred since the work shifts varied and many of them had no knowledge of the purpose of the study. The study was not a randomized controlled trial but rather relied on a pre–post design. This did not allow us to fully account for changes over time unrelated to the effects of the intervention, although the multiple baseline measures provided some assurance that the music therapy was responsible for the observed results.
Future research should be performed across a wider distribution of socioeconomic status and racial groups. While this study generated an adequate sample size (n = 132), the design required focusing on one targeted behavior, requiring the sample to be divided into three groups. Relatively few participants had agitation or wandering as the predominant targeted behavior. Future work should make an effort to increase sample sizes to assess the efficacy of music therapy in reducing agitation and wandering.
Conclusion
Research has informed us that neuropsychiatric symptoms such as depression, agitation, and wandering may cooccur up to four times more often in people with dementia than those without (Lyketos et al., 2000). At baseline, many of our study participants were experiencing depressive symptoms simultaneously with agitation or wandering behaviors. One strength of our study is that through recruitment of a large sample we were able to create groups with specific types of behavioral symptoms and tailor the music therapy to alleviate the symptoms exhibited. At the time they entered the study, the majority of the participants were taking antidepressant and psychoactive medications, but many still exhibited signs of distress related to depression, agitation, and wandering. Since Herrman and Gauthier (2008) and others have suggested to address neuropsychiatric symptoms with nonpharmacological therapies, our outcomes should encourage practitioners to consider music therapy as a priority, but if medications are ultimately deemed necessary, may also complement pharmacological treatment of depressive symptoms and agitation for nursing home residents diagnosed with dementia.
From our perspective, the outcome measures neglected to present the full value of the music therapy. We also believe that all participants received life-enriching experiences during the music therapy sessions. It is important not to neglect factors such as pleasure that may be equally important but more difficult to measure (de Medeiros & Basting, 2014). Future studies should be designed to elucidate the mechanisms through which music therapy achieves success in reducing neuropsychiatric symptoms and evaluate other benefits such as improved quality of life.
Footnotes
Acknowledgements
The authors thank Suzanne Fitzsimmons, NP, University of North Carolina at Greensboro, for her guidance and clinical oversight. They also thank Jay Gormley and Audrey Waters from MJHS planning, research and public relations departments for their invaluable support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the New York State Department of Health with continued assistance from the MJHS Foundation.