
Abstract
A caregiver’s attachment history with their parents may affect the thoughts, feelings, and behavior they now have as they care for a parent with dementia. Participants were 77 daughters of a parent with dementia. The nature of participant conscious episodic memories of their parental figures and unconscious procedural knowledge of caregiving processes (secure base script knowledge) were identified as two aspects of the caregiver’s relationship history that may impact their involvement in care, relationship conflict, critical attitudes, and strain. Our findings indicated that the nature of episodic memories of the caregiver relationship history with parental figures were significantly associated with stress and criticism of their parent. Greater unconscious procedural knowledge of the secure base script was associated with caregiver report of less conflict and less involvement in the caregiving tasks. Potential clinical implications of this pattern are also discussed.
Delivering care for persons with dementia (PWD) is extraordinarily challenging and involves managing a range of behavioral problems, including agitation, confusion, sleep difficulties, and wandering. Most often care is provided by family members or friends and these individuals experience tremendous stress and burden in their role. Indeed, the challenges inherent in navigating both the concrete tasks of providing care and the associated emotional strains of managing problematic behavior are faced by 15.2 million individuals in the United States who look after PWD (Alzheimer’s Association, 2012). Internationally, the prevalence of dementia is also rising. As of 2010, there were approximately 35.6 million PWD worldwide (Prince et al., 2013). These numbers are expected to nearly double every 20 years. In 2010, the associated worldwide costs of dementia was US $604 billion and, particularly for low- and middle-income countries, the costs associated with informal caregiving accounts for the majority of total costs (Wimo et al., 2013). Contributing to those costs are the impact of the strain associated with caregiving, which potentially puts the caregivers themselves at risk for multiple negative health outcomes, including depression, high blood pressure, and heart problems (Holland et al., 2011). In a meta-analysis of 84 studies, significant differences between caregivers of PWD and controls were found in depression, stress, self-efficacy, and subjective well-being (Pinquart & Sorensen, 2003).
Among unpaid caregiving networks, adult children caring for their parents is a common pattern, with daughters in particular frequently taking on this responsibility (Legault & Ducharme, 2009; Steele, Phibbs, & Woods, 2004). In addition, caring for a parent with dementia can be a particularly complicated and challenging role. A growing body of evidence further suggests that the experience of caregiving varies by kinship. Among daughters, for example, caregiver guilt was found to moderate the relationship between frequency of leisure activity and depression but not in sons, wives, or husbands (Romero-Moreno et al., 2014). Additionally, daughters did not show the expected relationship between stressors, stress, and depression in contrast to wives (Simpson & Carter, 2013). These findings suggest that the psychological experience of distress, among daughters in particular, may be impacted to a greater extent by internal factors above and beyond concrete external variables such leisure time or the nature of stressors.
Daughters of PWD bring their unique and sometimes troubled relationship histories into the caregiving context, which may impact the caregiving experience. Although some daughters describe close, loving relationships with their parent, which may serve as the foundation for their commitment to caregiving, other daughters describe histories of neglect, conflict, and, sometimes, physical, emotional, or sexual abuse. The nature of the relationship history can shape the way that daughters feel and act toward the individuals for whom they care. These observations are consistent with literature suggesting that a history of childhood abuse or neglect, for example, may be a risk factor for later elder maltreatment (Reay & Browne, 2001).
One framework for understanding the impact of early relationship history on later relational patterns is attachment theory. Developed by John Bowlby and Mary Ainsworth, attachment theory draws from various theoretical frameworks to form a cohesive system to explain styles of emotional bonding, or attachment styles, based on the nature of early emotional connections with parental figures (Ainsworth, Blehar, Waters, & Wall, 1978; Bowlby, 1969). Research has indicated an individual’s “attachment history” with primary caregivers impacts the manner in which an individual later provides care across a variety of contexts. For instance, an individual’s early attachment experiences with parents have been shown to shape the patterns of caretaking adopted with that individual’s own children (Belsky, 1997; Sroufe, 2005). Further, a strong empirical connection has been made between the nature of the care received from parents and interpersonal patterns in adulthood with romantic partners and peers (Roisman, Collins, Sroufe, & Egeland, 2005; Zayas, Mischel, Shoda, & Aber, 2011). Given the longstanding and deeply involved relationships that occur between parent and child, this effect may be amplified when relationship roles are reversed and daughters take on the role of caretakers for their parents. In particular, research indicates that stronger attachment bonds have been associated with less caregiver burden and stress as well as higher levels of care (Carpenter, 2001; Cicirelli, 1993).
There are a variety of ways in which a daughter’s experience with parental figures, both positive and negative, can impact subsequent interpersonal functioning cross a range of contexts and different relationship roles. Crittenden (1997, 2006) described the ways that one’s attachment quality, via different memory systems, is used to produce predictions about the ways that self and other will relate in various future contexts. This model proposes that these memory systems exist with varying levels of conscious awareness, verbal representation, and affective association. Of particular relevance to our work are two memory systems: (a) episodic memory and (b) procedural memory/knowledge. Episodic memory consists of conscious mental representations of events that contain sequentially organized images, affects, and cognitions. This memory system is hypothesized to trigger affective, cognitive, and behavioral responses when individuals come in contact with circumstances that evoke those memories. For daughters providing care to an older parent with dementia, episodic memories of the ways that a parent treated her as a child can impact the nature of the interpretations and attributions that the daughter makes for her parent’s dementia-related behaviors and the affective responses associated with those behaviors. In contrast, procedural memory represents largely unconscious sensory-motor models that guide behavior through learned sequences. This memory system likely developed out of observing and interacting with parental figures over time in ways that formed the foundation for unconscious expectations, beliefs, and emotional and behavioral reactions in relationships. Individuals come to develop “narratives” or “storylines” for how they believe relationships should or ought to “work.” For instance, one such narrative has come to be known in the attachment literature as the “secure-base script.” This unconscious narrative exists in a person’s mind as an algorithm for how he/she would navigate a situation when caregiving is required. The secure base script consists of (a) an individual successfully recognizing or detecting the need to provide care or assistance, (b) effectively offering and providing that assistance (e.g. offering comfort or helping to manage overwhelming affect), and (c) helping to return the individual being cared for to an emotionally calm place or initiate a new constructive interaction with the individual (Waters & Waters, 2006). The degree of procedural knowledge that an individual has of the secure-base script has been found to predict patterns of interaction in relationships, physiological reactions to distress of individuals being cared for, and the tendency to seek assistance (Creasey, 2002; Groh & Roisman, 2009; Riggs, Jacobovitz, & Hazen, 2002; Vaughn et al., 2007; Webster & Hackett, 2007). In the context of caregiving, these unconscious procedural “scripts” may come to influence the nature of how individuals caring for parents with dementia interact with that parent.
In this study, we attempted to test the hypothesis that unconscious procedural knowledge of the secure base script and the quality of episodic memories of past relationship experiences will have different effects on daughters’ thoughts, feelings, and behavior. Episodic memories of daughters’ relationship with their parents help daughters to create meaning and understand their current relationships in the broader context of their relationship history. These memories often define the meaning of what is happening in the interpersonal interactions around providing care and impact what daughters think and feel. For example, for a daughter whose parent had always been extremely kind and gentle, agitation may be understood more clearly as a product of the parent’s underlying dementia and thus lead to feelings of caring. In contrast, for daughters whose parents have been violent or aggressive throughout their lives, dementia-related agitation may be attributed to a motivation to intimidate or control leading to feelings of anger or stress.
Additionally, unconscious procedural knowledge of the secure base script may contribute to defining the range of potential behavioral responses accessible to the daughter at any given moment. For a daughter who has never experienced a caring, empathic response from a parent, it is unlikely that the individual will have in their repertoire the complex emotional and behavioral skills needed to provide care to others when required. The current study explored the relationship between daughters’ conscious recollections of their relationship history (episodic memory) as well as unconscious knowledge of the secure base script (procedural knowledge) on daughters’ critical thoughts, stress, involvement, and relationship conflict. We hypothesized that:
Procedural memory will be more strongly associated with aspects of the enactment of care—Unconscious procedural knowledge of the secure base script as measured by the Secure Base Script Assessment (SBSA) will be more strongly related to caregiving behaviors such as frequency of involvement and degree of relationship conflict as measured by the Level of Expressed Emotion Scale (LEES) than conscious episodic recollections of parental relationships as measured by the Parental Bonding Instrument (PBI). Episodic memory will be more strongly associated with how daughters make sense of the dementia their parent is experiencing—Episodic memory of parental relationship history as measured by the PBI will be more strongly related to caregiver strain as measured by the Gilleard Strain Scale (GSS) and critical attitudes/thoughts as measured in a Five Minute Speech Sample (FMSS), than unconscious procedural knowledge of the secure base script as measured by the SBSA.
Method
Study design
The analyses of this cross-sectional study were driven by our interest in examining how functioning and experience differed according to daughters’ episodic memory and procedural knowledge. The specific facets of caregiving functioning that were examined pertained to caregiver burden and involvement, as well as critical attitudes on the part of the daughter and perceived relationship quality in the caregiving dyad. Two covariates were chosen, PWD cognitive status and aggressive behavior, to control for the possibility that caregiver functioning could be better accounted for by highly relevant variables other than attachment quality.
Participant characteristics
Participants in this study were 77 daughters of parents with dementia. Participants were not remunerated for their participation. Trained research staff obtained informed consent, and all protocols were approved by the IRB at the University of North Carolina at Chapel Hill (UNC-CH). The majority of the sample (71%) was faculty, students, or other employees of UNC-CH who were recruited via an e-mail advertisement about the study. The remainder (20%) were former participants in the Alzheimer’s Association’s Dementia Care Study (Zimmerman et al., 2005), referrals from previous participants (7%), and individuals who responded to flyers placed in nursing facilities, senior centers, and memory disorders clinics (2%). The majority of daughters self-reported that they were White (91%), highly educated (70% with a college degree or graduate degree), and had a household income greater than $50,000 (69%).
The PWD were the mothers (84%) or fathers (16%). The majority (62%) lived in an institutional setting (i.e. assisted living, nursing facility, or special care unit); 22% were living on their own in the community; 9% were living with the daughter.
Sampling procedures and measures
Daughters were mailed a battery of self-administered questionnaires that they completed and then returned to the investigators. A trained research assistant then contacted each participant for a one-hour telephone interview about caregiving experiences and attitudes. The Adult Child/Aging Parent SBSA and the FMSS were administered during the telephone interview to assess daughter implicit knowledge of the secure base script and critical attitudes, respectively.
Measures of attachment
PBI
The PBI is a 25-item self-report scale that asks participants for their memories of their relationship with their mother during the first 16 years of childhood to evaluate attachment quality based on conscious episodic memory (Manassis, Owens, Adam, West, & Sheldon-Keller, 1999). Each item is rated on a Likert-type scale from 0 to 4 and scores are summed for overall and subscale scores. The PBI has been demonstrated to have strong test–retest reliability over a 10-year time span (Wilhelm & Parker, 1990). The PBI is a commonly used measure of adult attachment and has been significantly correlated with relevant outcomes in previous studies (Paley, Shapiro, & Worrall-Davies, 2000). The measure demonstrated strong internal consistency in our sample (α = .99)
SBSA
The SBSA is a measure of unconscious procedural knowledge of the caregiver’s assess to a secure base script. It is based on the Attachment Script Assessment validated for parents and couples (Waters & Waters, 2006). Additional details about the development and psychometrics of this measure are discussed in Chen et al. (2013). The measure is administered by providing participants with word prompts and asking them to tell an imaginary first person narrative describing an interaction with their parent. Daughters’ responses were tape recorded, transcribed, and later scored by two trained independent coders using a seven point scale reflecting the extent to which the story reflected a secure base narrative (Waters & Rodriques-Doolabh, 2004). Secure base script scores for the three passages were averaged to yield a single composite score and higher scores indicate greater procedural knowledge of the secure base script.
Measures of caregiver functioning
LEES—Caregiver version
The LEES is a self-report questionnaire of caregiver conflict consisting of 60 true/false items that assesses the caregivers self-reported behavior along four dimensions: (a) intrusiveness (e.g. I am always interfering), (b) tendency to respond to the PWD in ways that exacerbate the PWD’s distress (e.g. I make matters worse when things aren’t going well), (c) express negative attitudes about the illness to the PWD (e.g. I often accuse him/her of making things up when he/she isn’t feeling well), and (d) have a low tolerance for disturbed behaviors or high expectations of the patient (e.g. I am realistic about what he/she can or cannot do). Higher scores on the LEES indicate greater relationship conflict as characterized by intrusiveness, overly emotional responses, expression of negative attitudes, and intolerance. The LEES has been shown to be reliable and internally consistent (Cole & Kazarian, 1988). Cronbach’s alpha for our sample was 0.70.
FMSS
The FMSS was used to measure critical attitudes in daughters, who are asked to talk about their feelings toward their family member for approximately five minutes (Gottschalk & Gleser, 1969; Magana et al., 1986). The audiotaped monologue is scored on nine facets with the current analyses focused on whether the individual is rated as high or low on criticism. Scores for the subscales of interest are based on the number of critical statements that are expressed.
GSS
The GSS is a 13-item self-report measure of caregiver strain that asks respondents to rate the degree to which they experience feelings such as embarrassment, frustration, danger, concern about finances and anxiety (Gilleard, 1984). Each item is rated on a 3-point Likert-type scale and the sum of all items is used to create an overall scale score.
Caregiver Involvement Scale (CIS)
The CIS assesses for the level of daughters’ involvement and consists of eight items that ask respondents to report the frequency of their involvement in a variety of typical tasks that caregivers of either community residing or institutionalized older adults perform, including assistance with daily care, visitation, and monitoring finances (Zimmerman, Sloane, & Ory, 2001). The sum of each of the items is used to estimate the overall degree of family caregiver involvement. Previous research indicated that the CIS was significantly correlated with caregiver burden and current attachment behaviors toward a PWD (Chen, 2006).
Covariate measures
Minimum Data Set Cognition Scale (MDS-COGS)
The MDS-COGS is a measure of cognitive status administered by trained research staff and completed by a family caregiver. The MDS-COGS has been demonstrated to be capable of measuring impairment ranging from no impairment to very severe cognitive impairment across care settings. The MDS-COGS contains eight items designed to assess memory, orientation, and decision-making and has been found to be a valid measure of cognitive status (Hartmaier, Sloane, Guess, & Koch, 1994). It has demonstrated good sensitivity and specificity for correctly discriminating cognitively impaired from cognitively intact subjects as defined by the Mini Mental Status Examination. Sensitivity and specificity were above 0.90 and kappa coefficients of agreement were above 0.80 (Hartmaier et al., 1994).
Cohen-Mansfield Agitation Inventory (CMAI—shortened version)
The CMAI measures the frequency of episodes of aggressive behavior and is commonly used to assess agitation among individuals with dementia (Cohen-Mansfield & Billig, 1986). The present study used a 16-item short-form of the CMAI, which assessed a wide range of symptoms including physical and verbal aggression (e.g. hitting or screaming), activity disturbances (e.g. wandering or restlessness), and verbal and physical behaviors that deviate from social norms such as sexual disinhibition, irrelevant verbalizations, and hoarding. Higher scores indicate greater frequency and severity of behavioral problems. Studies have shown good psychometric properties for this instrument (Cohen-Mansfield, 1995).
Analytic approach
SAS version 9.3 was used to analyze the data. To answer the primary question of interest of whether the pattern of results differed depending on the attachment measure, we first conducted correlational analyses to confirm that the associations between the attachment measures and caregiver functioning were consistent with the hypotheses. Next, two sets of linear regression analyses were constructed: the four aspects of caregiver functioning and two covariates were separately regressed on attachment quality based on procedural knowledge of the secure base script (SBSA) and attachment quality based on episodic memory (PBI). By entering covariates into the simultaneous regressions, we were able to evaluate the direct effects of aggressiveness and cognitive status, which were believed to have the potential to explain significant variance in caregiver functioning. The final result was a total of eight regression models, with all variables entered simultaneously. Caregiver involvement was transformed using a natural log function given its non-normal distribution (positively skewed). Because of the relatively small sample size (N = 77), regression analyses were carried out separately for each of the attachment measures, and we did not adjust for repeated comparisons, thus increasing the likelihood of Type I error.
Results
Intercorrelations between caregiving outcomes.

GSS: Gilleard Strain Scale; FMSS: Five Minute Speech Sample; LEES: Level of Expressed Emotion Scale.
p < 0.05, **p < 0.01, ****p < 0.0001.
Intercorrelations between attachment and caregiver outcomes.

Intercorrelation between attachment measures = −0.06 (not significant).
GSS: Gilleard Strain Scale; FMSS: Five Minute Speech Sample; LEES: Level of Expressed Emotion Scale; PBI: Parental Bonding Instrument; SBSA: Secure Base Script Assessment.
p < 0.05, **p < 0.01, ***p < 0.001.
Simultaneous multiple regression analyses predicting change in facets of the caregiver experience from episodic memories of parental figures and implicit script knowledge.
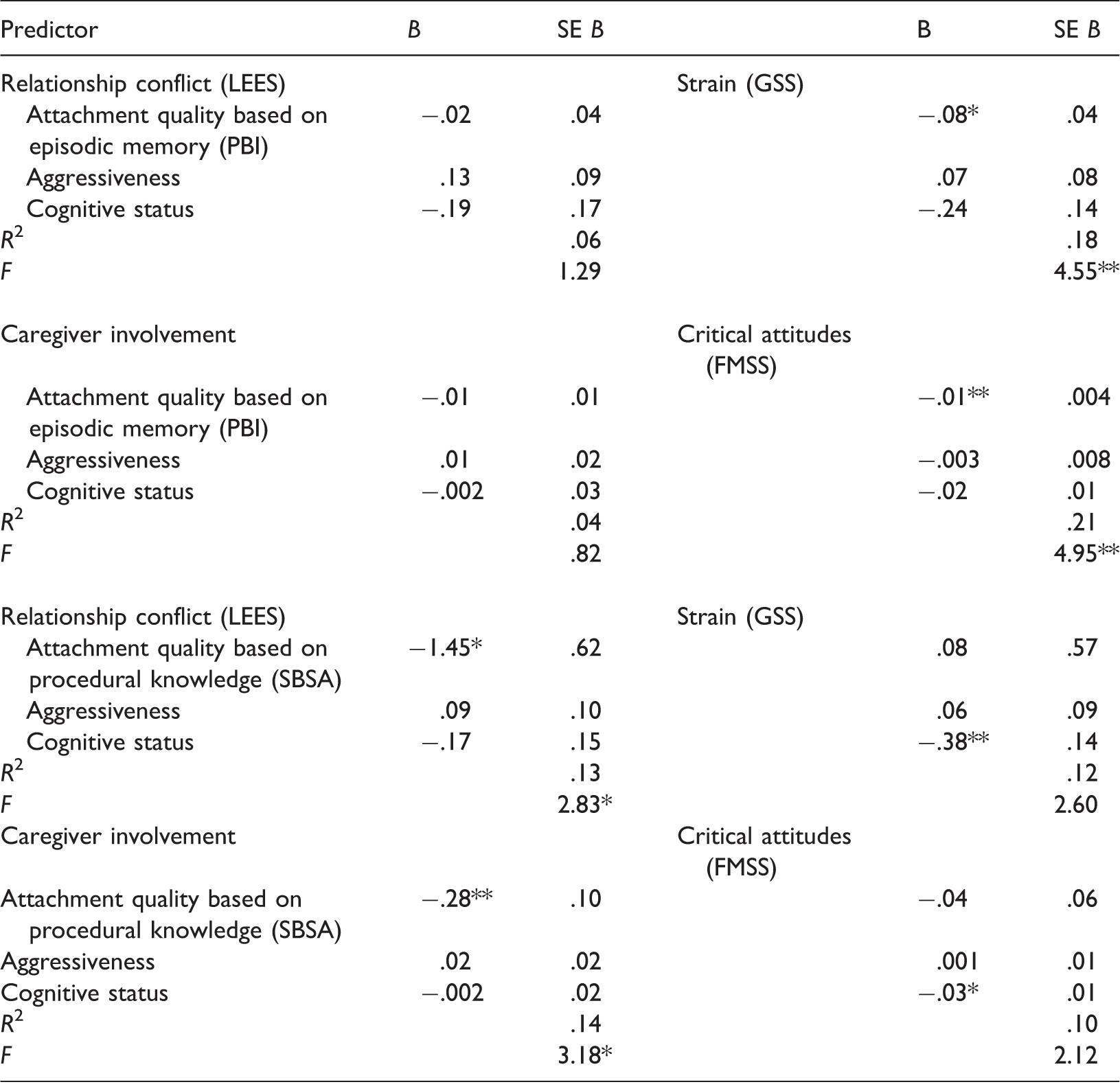
GSS: Gilleard Strain Scale; FMSS: Five Minute Speech Sample; LEES: Level of Expressed Emotion Scale; PBI: Parental Bonding Instrument; SBSA: Secure Base Script Assessment.
p < 0.05, **p < 0.01, ***p < 0.001.
In the analysis of critical attitudes as predicted by the attachment variables, only attachment quality based on episodic memory (PBI) was a significant predictor of critical attitudes, B = −.01, t(57) = −2.78, p = .007, such that explicit memories of more positive attachment experiences were associated with less critical attitudes toward one’s parent. In the analysis of caregiver strain, again only attachment quality based on episodic memory (PBI) were found to be a significant predictor of burden, B = −.08, t(64) = −2.24, p = .03, such that daughters’ episodic memories of more positive attachment experiences were associated with less caregiver experience of strain.
Intercorrelations between procedural knowledge and aspects of relationship conflict (LEES).

LEES: Level of Expressed Emotion Scale; SBSA: Secure Base Script Assessment.
p < 0.05.
Discussion
This study attempted to better understand the different effects that daughters’ attachment quality can have on their thoughts, feelings, and behavior as caregivers of a parent with dementia. Specifically, we examined the relationship between episodic memories of parental figures and procedural knowledge of the secure base script. Furthermore, we differentiated the aspects of the caregiving relationship pertaining to episodic memories of parental figures versus unconscious procedural knowledge of the secure base script.
Our findings suggest that there is no significant relationship between daughters who report more positive explicit recollections of early parental relationships and unconscious procedural knowledge of the secure base script. Thus, a daughter could have positive conscious memories of parental figures and low levels of unconscious procedural knowledge of the secure base script. Another daughter may show the opposite pattern where they report less positive conscious memories of parental figures but high levels of unconscious procedural knowledge of the secure base script. This is consistent with attachment theory, which hypothesizes that the degree of positivity reported in conscious recollections of an individual’s history with their parent is not necessarily related to the unconscious processes that drive interpersonal functioning (Hesse, 1999). For example, some individuals who are characterized as having “dismissing” patterns of attachment have been found to restrict their awareness of negative feelings, limit recall of upsetting relationship related memories, and present descriptions of their relationship histories that are vague and not based on actual memories and yet show patterns of physiological arousal around interpersonal issues such as separation and rejection that they verbally deny as being significant (Dozier & Kobak, 1992). Other attachment patterns are characterized by idealized and “overly positive” memories of parents that reflect a lack of nuance and complexity in how these patients understand relationships and can translate into difficulties navigating the real relationships in the person’s life (Hesse, 1999). In fact, studies that have compared measures based on self-reported attachment style with interview-based assessments designed to assess unconscious aspects of attachment have also concluded that these measures may capture different constructs (Crowell, Treboux, & Waters, 1999).
As hypothesized, the conscious recollections of a daughter’s history with the parental figure that they are now caring for was significantly associated with the daughter’s felt experience of being strained by their responsibilities as a caregiver as well as a tendency to hold more critical attitudes toward the parent they were caring for. However, conscious recollection of daughters’ relationship history with parental figures did not significantly predict caregiver behavioral patterns either in terms of self-reported conflict or degree of caregiver involvement. In contrast, while unconscious procedural knowledge of the secure base script was not significantly associated with daughters’ experience of strain or critical attitudes toward their parent, it did significantly predict certain aspects of caregiver behavior. Specifically, daughters who had greater unconscious procedural knowledge of the secure base script reported less conflicted relationship patterns and less of a tendency to be intrusive in their care toward their parent. Examples of items on this measure included, “I leave him/her feeling overwhelmed” and “I am always interfering.” This tendency may partly explain the initially counterintuitive finding that greater unconscious procedural knowledge of the secure base script was associated with less caregiver involvement. This finding contrasts with other attachment research, which has reported that a secure attachment style among adult children has been found to relate to a greater likelihood that they will protect and care for elderly parents (Karantzas, Evans, & Foddy, 2010). For example, secure attachment has been associated with caregivers who maintain community-based care for older parents, rather than placing them into nursing home facilities (Markiewicz, Reis, & Gold, 1997). Additionally, insecure attachment styles characterized by anxiety about the availability of care or avoidance of dependency/a tendency to be emotionally distant are associated with greater caregiver stress and burnout and increased behavioral symptoms in the individual with dementia (Cooper, Owens, Katona, & Livingston, 2008; Crispi, Schiaffino, & Berman, 1997; Kokkonen, Cheston, Dallos, & Smart, 2014; Perren, Schmid, Herrmann, & Wettstein, 2007). One might hypothesize from these findings that greater procedural knowledge of the secure base script would lead to higher levels of caregiver involvement. We propose, however, that caregiver involvement is not a monolithic construct. Involvement can represent necessary aspects of care required to keep a PWD healthy and independent, but as reflected in our findings, involvement may also represent intrusiveness where a PWD feels disrespected, controlled, or burdened by overly anxious caregivers. Thus, future research may explore the variety of ways that involvement may manifest and its impact on caregivers and PWD’s.
Although our findings suggest a clear difference in the variables that each of these aspects of daughter attachment quality relate to, the reality is likely much more complex. Attachment research has reported that attachment style based on patient self-report of episodic memory of their relationship history has been correlated with various aspects of behavior in romantic relationships (Davila & Bradbury, 2001; Dewall et al., 2011). Similarly, unconscious aspects of attachment have been shown to relate to cognition and affect (Dykas, Woodhouse, Ehrlich, & Cassidy, 2012; Groh & Roisman, 2009). Thus, the results from the present analyses may demonstrate a cleaner differentiation of impact than what might be expected if the methods were repeated many times in multiple samples. However, our findings suggest ways in which different aspects of daughter attachment quality have a greater or lesser impact on different aspects of a caregiver’s experience and relationship. It is perhaps not unexpected that there may be overlap in the ability for these aspects of attachment to predict thoughts, feelings, and behavior as these aspects of the caregiving relationships are themselves interrelated. The theoretical framework underlying cognitive behavioral approaches to treatment emphasizes the relationship between thoughts, feelings, and behavior (Muran, 1991). Thus, we recognize that it may be overly simplistic to suggest that episodic memories of parental figures only impact thoughts and feelings and that unconscious procedural knowledge of the secure base script only impacts behavior. The attachment literature has presented a complex picture of the various ways that attachment styles may be evoked and the impact various styles have on coping. For example, avoidant attachment style was surprisingly unrelated to problems in coping with loss, specifically bereavement (Field & Sundin, 2001). Coping with dementia can be conceptualized as a form of “ambiguous loss,” which may suggest that attachment styles typically associated with adjustment difficulties may operate in unexpected ways in this context (Boss, 2009). However, our data offer an intriguing pattern of findings that these conscious and unconscious aspects of attachment quality differentially impact styles of caregiving. Additional research may help to better understand these differences.
Limitations and clinical implications
A number of limitations exist for our study. The homogeneity of the sample may limit the generalizability of the findings, and additional work will need to be done to determine whether similar patterns exist in populations with lower levels of education, socioeconomic status, or different racial and ethnic backgrounds. Additionally, the current study includes only daughters serving as caregiver. Future studies should investigate whether the relationships between the variables studied may vary based on caregiver gender or kinship. Although the size and distribution of our sample did not allow for additional analyses of the impact of care setting on the relationships explored in this study, we looked at these processes across settings because prior research had indicated that caregivers of PWD in institutional settings continue to experience similar levels of burden and maintain involvement as caregivers (Bowman, Mukherjee, & Fortinsky, 1998; Garity, 2006; Stull, Cosbey, Bowman, & McNutt, 1997; Zarit & Whitlatch, 1993). However, it is unclear how the associations studied might be different across settings. There is evidence to suggest that the care setting may impact the relationship between stressors and strain experienced by caregivers (Bowman et al., 1998). Thus, had our sample consisted primarily of daughters caring for a parent in the home, the relationships found in our study may have been stronger because of, for example, more frequent opportunities to evoke the attachment system. Future research in this area could address this limitation in the present study by focusing efforts on studying only those caregiving dyads living in this same setting.
One final limitation of the current study concerns the uncertain direction of causality given the cross sectional nature of the data. Although it is possible that stress associated with caregiving might affect a daughter’s unconscious procedural knowledge or conscious recollection of past experiences with their parent, we believe this is unlikely. Attachment research has supported the hypothesis that these patterns develop early in life and remain relatively stable throughout life. Accordingly, we understand the data to represent a sequence in which caregiving demands trigger the attachment system, which thus initiates longstanding patterns of relating and feeling toward PWD. However, although we know of no empirical findings demonstrating the stability of these variables in the context of dementia caregiving, there are findings to suggest that negative life events, like trauma, may impact some attachment variables (Waters, Merrick, Treboux, Crowell, & Albersheim, 2000). Therefore, longitudinal studies of the stability of episodic memories of parental figures and unconscious procedural knowledge of the secure base script over the course of dementia caregiving may elucidate the direction of these relationships.
Despite its limitations, we believe our study has implications for clinical practice with daughters who serve as caregivers. Our findings suggest that understanding the nature of a daughter’s relationship history may shed light on different needs for support. Some daughters whose conscious awareness of early strained relationships bias them toward misinterpreting their parent’s behavior may benefit from psychoeducation about the nature of the dementia and efforts to challenge unrealistic ideas about their parent’s control over symptoms. A number of caregiver interventions have a significant psychoeducational component designed specifically to provide caregivers with greater education about the nature and impact of dementia (Nichols, Martindale-Adams, Burns, Graney & Zuber, 2011). For some daughters, redefining expectations and challenging assumptions about the meaning of their parent’s behavior may be the critical agent for decreasing caregiver distress. These daughters may also report higher levels of subjective stress and thus may benefit from mindfulness based stress reduction approaches to managing the burden associated with caregiving responsibilities.
In contrast, other daughters may struggle with a lack of procedural knowledge of how to effectively provide care and interact in ways that do not exacerbate their parent’s anxiety or distress. Some approaches that are specifically informed by attachment theory are designed to help individuals develop more effective ways of interacting and providing care (Marvin, Cooper, Hoffman, & Powell, 2002). Others offer strategies to help caregivers manage and navigate the different symptoms faced by individuals with dementia (Belle et al., 2006; Nichols et al., 2011). Psychodynamic approaches to psychotherapy that are designed to increase a person’s capacity to reflect on their own and other’s experience may also help to shift the unconscious relationship scripts that drive some problematic relationship patterns (Bateman & Fonagy, 2004). There are some indications that certain approaches to psychotherapy may shift attachment patterns and may be a mechanism through which “earned-security” is achieved (Fonagy & Bateman, 2006; Levy et al., 2006). Overall, we believe that an understanding of attachment theory and specifically the impact of early experiences with parental figures on caregiver thoughts, feelings, and behavior may enhance our efforts to support and assist daughters who serve as caregivers in navigating the challenges they face.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Career Development Award from VA Health Services Research and Development (Grant CDA-2-10-023), grant 1T32 AG00272-01 A1 from the University of North Carolina Institute on Aging, and Sigma Xi Scientific Research Society Grant in Aid of Research (Cory K. Chen, Principal Investigator).