
Abstract
Since anxiety in patients with dementia is a complex, understudied phenomenon, this paper presents clinicians’ experiences of anxiety in this population. Semi-structured interviews were conducted with seven clinicians experienced with dementia in elderly patients (65 years and above), and then evaluated via qualitative content analysis. Analysis revealed three main categories: A reaction to loss and worries, symptoms of anxiety and depression interfere with each other, and anxiety in dementia—a multidisciplinary task. Anxiety in this population is perhaps best understood as a reaction to loss and worries, and existential in nature by the participants. Care interventions can reduce or prevent anxiety symptoms in this population. However, when anxiety co-exists with depression it might be difficult to attenuate these symptoms through care measures alone. To better identify and treat the condition, valid dementia-specific anxiety-screening instruments are necessary.
Introduction
Anxiety is frequently found in patients with dementia. Studies report that the prevalence varies from 8% to 71% for anxiety symptoms measured with different screening tools, and 5% to 21% for anxiety disorder (Seignourel, Kunik, Snow, Wilson, & Stanley, 2008). Anxiety co-occurring with dementia is associated with decreased function in activities of daily living (Teri et al., 1999), increased dependency (Orrell & Bebbington, 1996), an increased number of behavior problems (Gibbons et al., 2002; Ownby, Harwood, Barker, & Duara, 2000), a greater risk for nursing home placement (Gibbons et al., 2002), and an additional burden on the patients and caregivers (Cooper, Balamurali, & Livingston, 2007). Clearly, anxiety reduces dementia patients’ quality of life (Orrell & Bebbington, 1996; Selwood, Thorgrimsen, & Orrell, 2005). It is, therefore, critically important that anxiety in patients with dementia is thoroughly identified, assessed, managed, and treated.
Despite the high prevalence and negative impact of anxiety in dementia, anxiety symptoms in patients with dementia are often overlooked by caregivers and health care personnel (Seignourel et al., 2008). The reasons for this could be many: First, the symptoms of dementia and anxiety may overlap. Anxiety symptoms such as restlessness, being easily fatigued, and difficulty in concentrating can occur in patients with dementia without being an expression of anxiety (Seignourel et al., 2008). It might also be difficult to distinguish between symptoms of anxiety and other behavioral and psychological symptoms of dementia (BPSD) such as irritability, aggression, wandering, and sleep disturbance (McClive-Reed & Gellis, 2010). Therefore, anxiety symptoms are often considered a part of dementia itself. Porter et al. (2003) suggested that anxiety symptoms could be a nonspecific result of severe dementia, but this is still unknown (Starkstein, Jorge, Petracca, & Robinson, 2007).
Second, it might be difficult to distinguish between symptoms of anxiety and other mental illnesses. The relationship between depression and anxiety is the most common (Bergh & Selbæk, 2012; Bierman, Comijs, Jonker, & Beekman, 2007; Hynninen, Breitve, Rongve, Aarsland, & Nordhus, 2012). Between 68% and 75% of individuals with dementia and anxiety disorder also meet the criteria for a Major Depressive Disorder (MDD) (Seignourel et al., 2008).
Third, there is a lack of consensus about how to define anxiety in dementia. Currently, the diagnostic criteria for Generalized Anxiety Disorder (GAD) is the same for patients with and without dementia (Seignourel et al., 2008). Starkstein et al. (2007) suggested revised criteria for diagnosing anxiety in patients with dementia, recommending excessive anxiety or worry as the key criterion with the presence of at least three of the following symptoms: restlessness, irritability, muscle tension, excessive fears, and respiratory symptoms.
Fourth, memory- and language impairments in patients with dementia hamper expression of their experiences, and therefore, complicate the assessment process. Health care personnel working with this group of patients have a key role in addressing anxiety in patients with dementia. Their knowledge and experiences are therefore of great importance.
Although a considerable amount of research has been published on the experiences of patients with dementia and their caregivers (Steeman, Casterlé, Dierckx, Godderis, & Grypdonck, 2006), anxiety is rarely a topic. One exception is a study by Qazi, Spector, and Orrell (2010), who investigated the causes and management of anxiety in dementia from the perspective of users, caregivers, and staff.
As a part of a PhD study, one of the original aims of our study was to investigate the phenomenon of anxiety from the perspectives of patients with dementia and their caregivers. To develop an interview guide for the original study, we carried out qualitative interviews with seven clinicians experienced in assessing and diagnosing anxiety and other mental illnesses in patients with mild to severe dementia. The purpose of interviewing the clinicians was to understand how clinicians identify anxiety and differentiate symptoms of anxiety and depression among patients with dementia based on their clinical experiences. Due to lengthiness of the proposed study, qualitative interviews with patients with dementia and their caregivers could not be performed as originally planned. However, the information from clinicians’ interviews was found to be of interest for a publication.
Aim
The revised aim of this article was, therefore, to describe clinicians’ experiences of anxiety in patients with dementia. The specific research questions were:
• What is the clinicians’ perception of the nature of anxiety in patients with dementia? • How do clinicians identify anxiety in patients with dementia? • How do clinicians differentiate anxiety from depression in patients with dementia?
Methods
Design and participants
The study is grounded in a qualitative, descriptive, and cross-sectional design. Semi-structured individual interviews with open-ended questions in line with Kvale and Brinkmann (2009) were conducted with seven clinicians experienced in assessing and diagnosing dementia and other mental illnesses in elderly patients (≥65 years), irrespective of the diagnostic criteria they used. This purposeful sample consisted of two specialist psychologists, two geriatric psychiatrists, and one psychiatric nurse working in outpatient clinic and in-patient care in the unit of old age psychiatry of a hospital, as well as two consultant physicians working in nursing homes. This group of clinicians included five women and two men, and the mean age was 50 years (40 to 71 years). The participants’ clinical experience with elderly patients with mental illness ranged from 7 to 40 years.
In this article, the phrase ‘patients with dementia’ refers to persons with any type and stage of dementia, 65 years and above, receiving medical care either from community health services or specialist health care, and residing either in their homes or nursing homes.
Data collection
Interview guide.
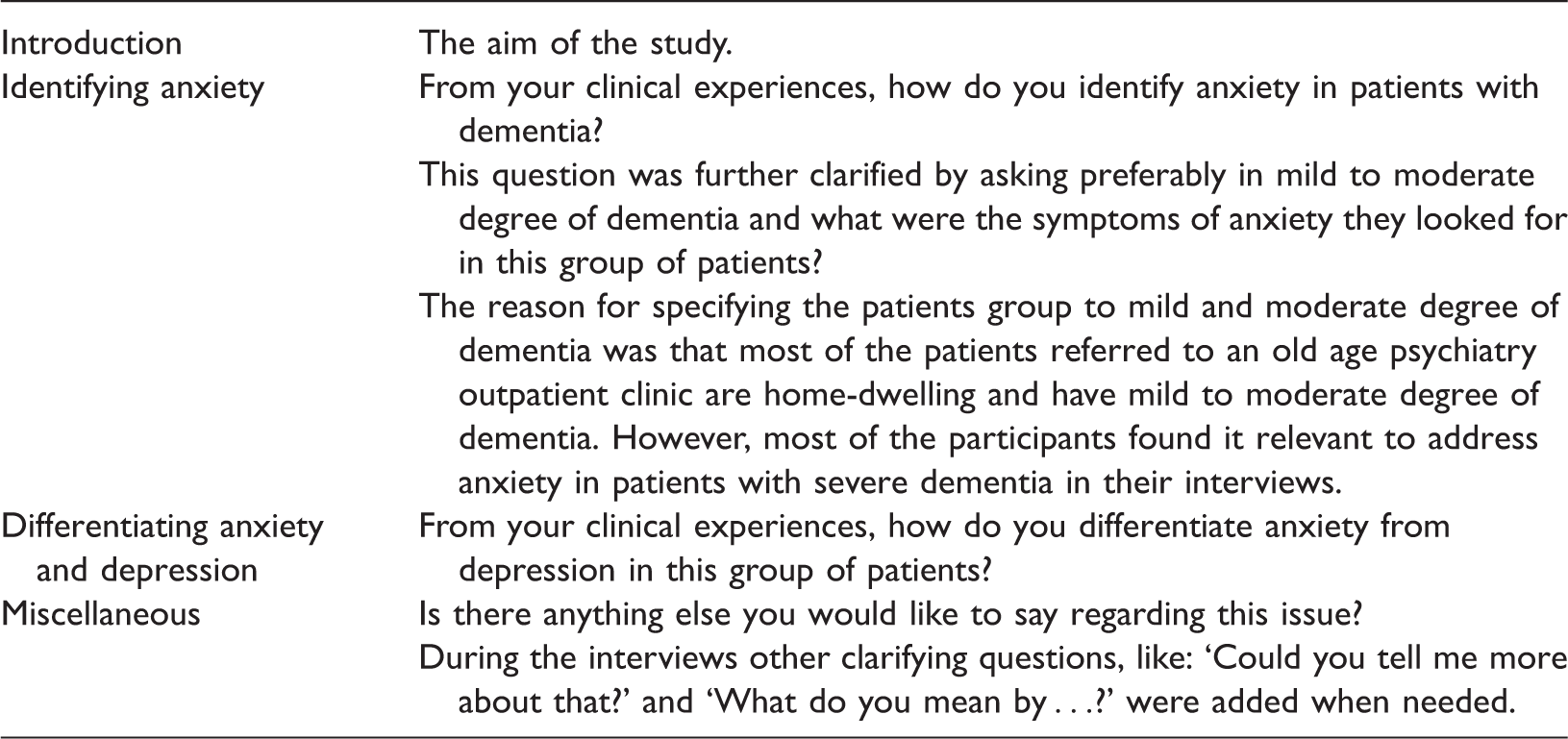
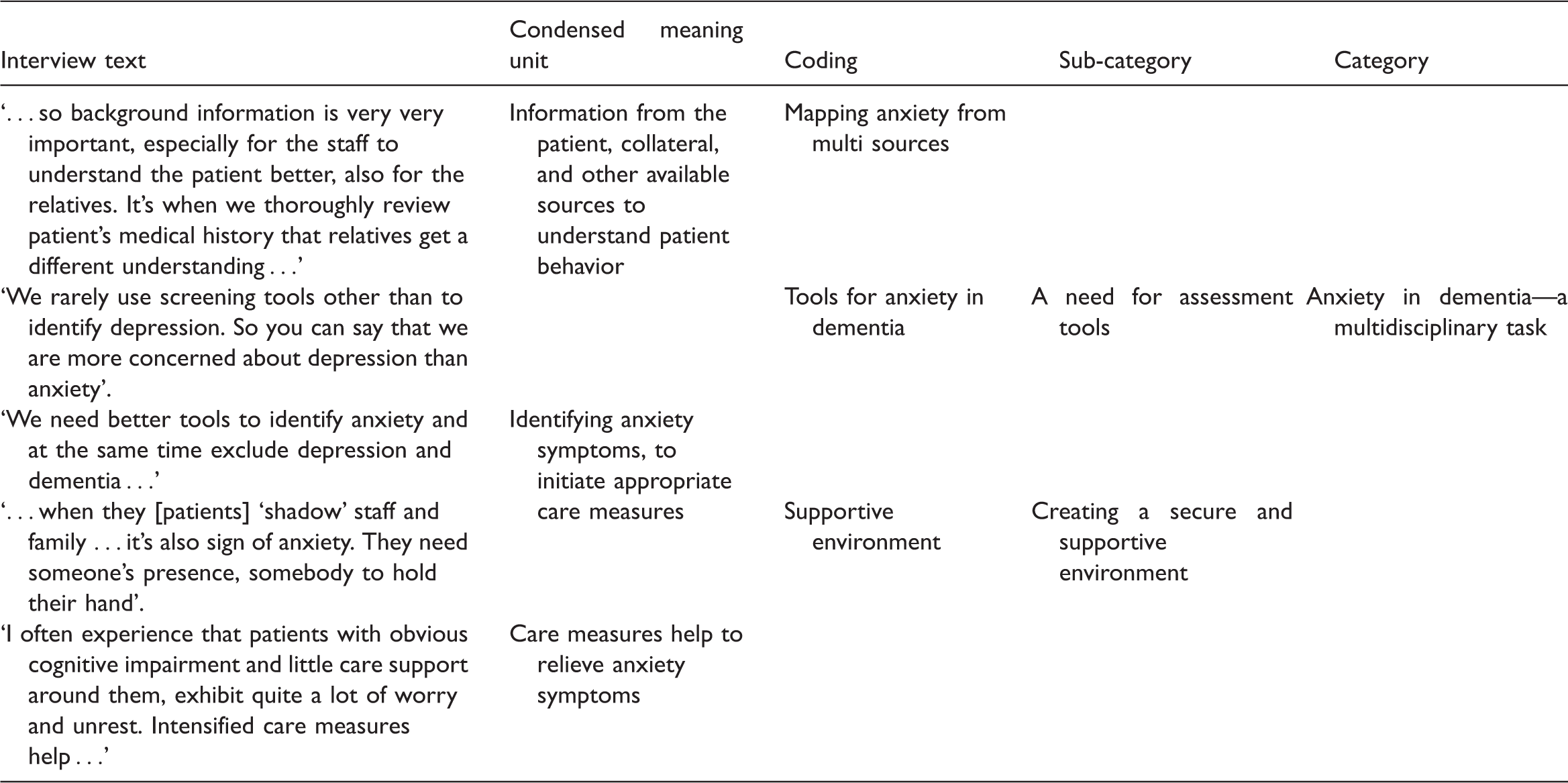
Illustration of analytical process.
Ethical issues and approval
The study was approved by the Regional Committee for Medical and Health Research Ethics (REK) in South-Eastern Norway (record nr. 2012/1958). Oral and written information about the study was provided to acquire informed consent from the participants. The transcribed interviews were de-identified. Once the article is accepted, the audio files will be destroyed.
Data analysis
Transcribed interviews were analyzed in line with qualitative content analysis inspired by Graneheim and Lundman (2004). Qualitative content analysis can be conducted on different levels of abstraction, and the content of a text can either be manifest or latent. The material in this study was analyzed on a manifest level and present what is directly expressed in the text, providing a description of the visible and tangible components of the material (Elo & Kyngäs, 2008; Graneheim & Lundman, 2004). The analysis was conducted by ARG in cooperation with SE, and took place in six stages. The first stage of the analysis, the preparation phase, started when listening to the audio files and transcribing the interviews. Each transcribed interview was identified as a unit of analysis, and was read several times to uncover the self-understanding of the text and provide a sense of the whole. Second, the texts were divided into meaning units. Third, the meaning units were identified and condensed into a description close to the text. Fourth, the condensed meaning units were extracted and labeled with codes. Fifth, various codes were compared based on similarities and differences, and independently grouped into sub-categories by ARG and SE. Sixth, sub-categories were grouped together and abstracted as categories. An example of this analytical process is shown in Table 2.
Results
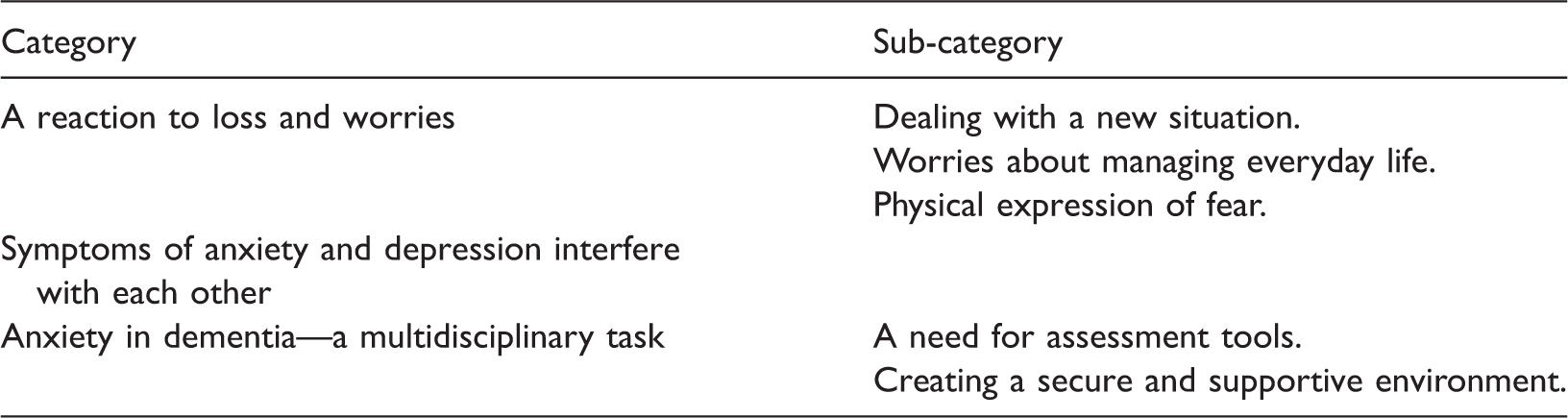
Overview of categories and sub-categories from content analysis of clinicians’ experiences of anxiety in patients with dementia.
A reaction to loss and worries
To outline the nature of anxiety in dementia, the clinicians described symptoms and possible causes of anxiety from both a biomedical and a psychosocial angle. Clinicians shared several examples that provided the context in which anxiety in patients with dementia occurs and described the complexities of revealing anxiety symptoms in this group. Three sub-categories emerged: Dealing with a new situation, worries about managing everyday life, and physical expression of fear.
Dealing with a new situation
Due to the development of dementia, most of the patients experience several losses related to everyday life, including the loss of perspective in their life, the loss of control over their situation, and a loss of meaning. The life-world becomes incomprehensible and complex when experiencing cognitive impairment and patients feel insecure, worried, concerned, and restless. One of the participants expressed: One phenomenon, which I recognize from many occasions with patients with dementia, is that the patient insists to go home … to go to the other house, although the patient has been living in the same house for the last 40 years. One can just wonder what he or she means to go home? I think, they mean to go to their childhood home. They feel insecure, that’s what it represents when they say they will go home. Patients with dementia, I think, often have that existential anxiety. There is a transition in life (…) [as a result of dementia] that creates an existential crisis and I think then the anxiety comes. They [patients] lose the meaning and overview of their own situation (pause) and what we see during the home visits … they turn, I would say, ‘up-side down’ their houses in an attempt to create a sort of order in their lives. I've had patients whose relatives been rang up many times while doing grocery, even though the patient was well informed that he/she will be in the grocery store and gone for an hour (…). Family members feel totally locked in such situations. I think it has to do with the existential anxiety because the patient loses overview and feels insecure.
Worries about managing everyday life
One of the participants stated that the first observed symptom of dementia is very often related to anxiety. Several participants described restlessness and worry as two of the main symptoms of anxiety in dementia: ‘The world becomes incomprehensible, the person loses track, and anxiety symptoms appear in the form of restlessness and worry’.
In mild dementia, symptoms like feeling insecure, being less social, refusing to go to the doctor for check-ups, and reducing activities of daily living were described as common expressions of anxiety. One example offered was of a woman who began making simpler dinners than she formerly made, while another told of a man who was suddenly insecure about driving a car. Anxiety symptoms in relation to mild dementia can be expressed in small daily activities. One of the clinicians stated: Anxiety in dementia, I suppose, is, sort of, more global and primitive. I mean, it’s not that a patient is afraid of, like you say, of a particular thing or a kind of phobia, no … It’s more that the patient is anxious about how to manage day-to-day activities. The patient is frightened of being revealed.
Physical expression of fear
The symptoms expressed in the moderate stage of dementia might become more intense in severe dementia. The participants described additional symptoms such as persistent shouting, complaining of vague bodily pain, palpitations, and tremors (without support of medical history).
According to the participants, physical symptoms such as palpitations, sweating, blushing, and nausea are often seen as side-effects of medications in elderly patients with dementia. From their point of view, it is important to recognize and acknowledge these symptoms as a possible expression of anxiety. The physical symptoms of anxiety are often confirmed by the patient’s caregiver, as one participant noted: When the patient no longer has control over the body as before, does not understand what will happen or may not understand what we say, we often observe the symptoms of anxiety in the form of protest. The patient resists, stiffens the body and hardens the eyes, can get hectic tanned face [redness], and can beat or cling to something or someone.
Symptoms of anxiety and depression interfere with each other
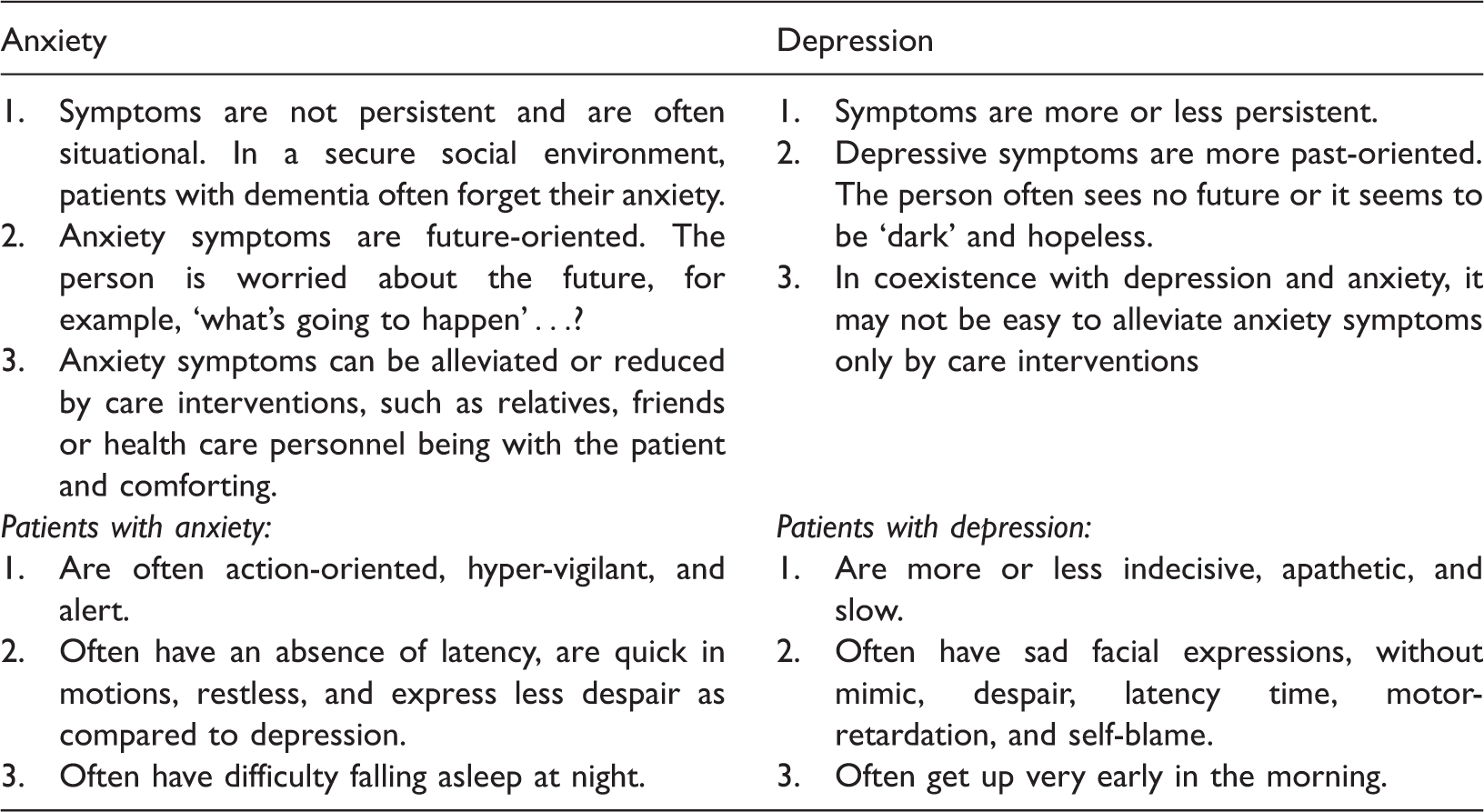
The main differences between symptoms of anxiety and depression in patients with dementia.
Anxiety in dementia—A multidisciplinary task
The challenge of managing anxiety symptoms in elderly patients with dementia was seen as a central aspect of care by the clinician and included two main perspectives: a need for assessment tools and creating a secure and supportive environment.
A need for assessment tools
Clinicians stated that anxiety was seldom the main reason for referral to the old age psychiatry outpatient clinic. Changes in the elderly persons’ behavior and assessment of their cognitive status were two of the main reasons for referrals. Clinicians admitted that they often considered anxiety symptoms to be part of other mental illnesses, and not a disorder of their own.
The participants found it difficult to identify anxiety in patients with dementia because of the changes in memory and language. However, through a systematic assessment of patient’s medical and psychological history, and with the support of assessment tools, it is possible to identify anxiety in patients with dementia. The process was described as a multidisciplinary task, and clinicians emphasized the importance of using appropriate tools for identifying anxiety in this target group. The participants claimed that the assessment tools for anxiety available for this target group had several weaknesses. One of the participants noted, ‘In my opinion, it would have been easier to identify anxiety in patients with dementia if we have had good assessment tool … and, there is a need to have so’.
Creating a secure and supportive environment
The clinicians reported that anxiety symptoms in patients with dementia could be prevented or relieved through different interventions. Most common are interventions conducted by the nursing staff, such as creating a secure social environment and framework for the patients and giving adequate support to their families. Other important aspects include the support offered in activities of daily living, being together with the patient, and making the patient feeling secure or comforting the patient. (…) this existential anxiety more or less, is always there. The caregivers provide a secure and supportive framework. The feeling of security ceases as soon as the caregiver is not there. Then I think, it is very important to build security and supportive measures that provide an overview, understanding and create meaning to the patient. If you inform the patient in a calm and pleasant voice, use simple words what you are going to do, wait for few minutes until the patient has understood. You do things slowly, not in a hurry then it is fine. But … if you don’t have sufficient time, forget to inform the patient or do not take into account, and everything goes fast with harsh movements, … [during morning care], then the patient grabs hold of you or something else in approach (…). You can observe by the patient’s body language (…) the patient opposes instead of being cooperative.
Discussion
As far as we know, this is the first study describing clinicians’ experiences of the complex phenomenon of anxiety in patients with dementia. The participants in our study described anxiety in dementia as a global phenomenon, which was understood as existential in nature. The concept of ‘anxiety’ was described by Soren Kierkegaard as a central aspect of the existential challenges of human life (Grøn, 2008). Due to the progression of dementia, cognitive impairment interferes with the activities of daily living. A patient with dementia loses perspective of day-to-day life and often experiences this new situation as incomprehensible, complex, and unpredictable, which may lead to feelings of insecurity, restlessness, and fear of abandonment. The transition from being an independent individual to being dependent or losing autonomy may trigger an existential crisis in patients with dementia. Thorne (1963) proposed that existential anxiety is the response when the process of existence is perceived as threatening. Situations that inhibit or frustrate ‘full-existence’ generate or release anxiety (Thorne, 1963). Qazi et al. (2010) found that the main cause of anxiety in patients with dementia was related to loss of skills, leading to increased dependence on others, the experience of loss of self-esteem, and negative thoughts. As noted by the participants, the patients’ awareness of the diagnosis or that something is going wrong may threaten the person’s sense of existence, which eventually leads the person to begin searching for the meaning of life. Paul Tillich’s theory of existential anxiety emphasizes meaninglessness as an absolute concern and refers to loss of the significance of life or one’s existence (Weems, Costa, Dehon, & Berman, 2004). Studies have shown that structural, neurochemical, and endocrinal changes in the brain might cause anxiety in patients with dementia (Beaudreau & O'Hara, 2008; Blazer, 2003). Some studies have addressed the existential issues from the perspectives of the caregiver (Høgsnes, Melin-Johansson, Norbergh, & Danielson, 2014; Levine et al., 1984; Piiparinen & Whitlatch, 2011), but the existential aspects have been poorly investigated from the perspectives of patients with dementia themselves.
In our study, symptoms of general anxiety like aggression, irritability, concentration problems, restlessness, feeling of despair, inner turmoil, social isolation, and sleep disturbances were described as overlapping symptoms of anxiety and depression in patients with dementia. Schoevers, Deeg, Van Tilburg, and Beekman (2005) found that depression and anxiety are comorbid, but form distinct constructs in cognitively intact elderly persons. To date, it still remains unclear whether anxiety and depression form distinct constructs in patients with dementia (Seignourel et al., 2008). One of the main difficulties in differentiating between these two comorbidities might be the diagnostic criteria itself, as GAD and MDD share four symptoms: psychomotor agitation or restlessness; being easily fatigued; difficulty concentrating; and sleep disturbances (American Psychiatric Association, 2013). A unique condition experienced by elderly individuals is ‘depression-like’ syndrome which is predominated by physical symptoms and withdrawal (Bryant, 2010; Newmann, Engel, & Jensen, 1991). According to the experiences of our participants, delusions about one’s own body can represent both anxiety and depression in elderly patients, but absence of the other core symptoms of depression (e.g., depressed mood or loss of interest and significant changes in body weight) (Criterion (A) 1-3 of MDD; Diagnostic and Statistical Manual of Mental Disorders-5) (American Psychiatric Association, 2013) may represent symptoms of severe anxiety.
It is important to distinguish anxiety from depression and dementia because of the increased risk of delayed remission and early relapse (Neville & Teri, 2011). As stated by the participants, observing patient behavior and body language may allow clinicians to differentiate between symptoms of anxiety and depression in patients with dementia. Calleo and Stanley (2008) suggested three key components to differentiating between anxiety and depression: (1) understanding the sequence of symptoms, i.e. which came first, anxiety or depression; (2) identifying the severity of the depression or anxiety; and (3) determining which symptom is more prominent in the clinical presentation: fear or sadness. A multidisciplinary comprehensive assessment is therefore necessary to identify anxiety symptoms in this target group. Clinicians noted that the screening tools for identifying anxiety should be used alongside the screening tools for depression because of their high co-existence, and clinicians should have training in using these assessment tools. Instruments designed specifically to assess anxiety in patients with dementia are currently not available in Norway.
Although anxiety could be a normal reaction to the situations that patients with dementia experience, information and awareness is also important for health care personnel. As described by the clinicians, anxiety symptoms in elderly patients with dementia can be reduced or eliminated through different care measures such as creating a socially secure environment for the patient, establishing a trustworthy relationship, and providing support in day-to-day activities. Neville and Teri (2011) found that anxiety in elderly persons with dementia is strongly associated with the skill of the staff. Educating the staff and health care personnel to identify the signs and symptoms of anxiety and strengthening staff skills in managing these symptoms is critically important (Neville & Teri, 2011).
Our participants reported that anxiety symptoms in coexistence with depression can be difficult to alleviate solely through care measures, a finding which has been supported by others (Schoevers et al., 2005). Their study demonstrated that co-occurrence of anxiety and depression represents more severe and chronic psychopathology than either anxiety or depression alone in elderly persons (Schoevers et al., 2005). Our participants emphasized that severe anxiety symptoms may be relieved by anti-depressants. Treatment of anxiety and depressive symptoms should be an essential part of the management and non-pharmacological interventions should be the first step in the management of anxiety in patients with dementia (Orgeta, Qazi, Spector, & Orrell, 2015).
Methodological considerations
Lincoln and Guba (2000) developed guidelines for the evaluation of qualitative studies, emphasizing five areas of importance: credibility, dependability, confirmability, transferability and authenticity (Lincoln & Guba, 2000; Polit & Beck, 2012).
To ensure credibility, dependability, confirmability, and authenticity, we have attempted to describe the process in an open and reflexive manner, presenting each stage of the research in detail. The informants were recruited due to their clinical experience and represent an authentic sample, presenting rich descriptions. Interviewing is an unfolding process during which the interviewer acquires new insight into the studied phenomenon. This new insight influences the subsequent follow-up questions throughout the interview process (Graneheim & Lundman, 2004).
Kvale and Brinkmann (2009) claimed that in order to become open, the researcher must seek to put the judgment about the factual ‘in brackets’. The interviews were conducted by ARG, who is also a psychiatric nurse with several years of experience within the field of mental health in elderly. Her clinical experience, the literature of previous research, and the analysis of the former interviews all informed her pre-understanding. In data collection and analysis, the pre-understanding of the researcher was made explicit. She attempted to be sensitive, with an open attitude during the interviews and in the analysis process. The data collection and process of analysis were also discussed with the co-authors.
The study included a small number of participants from the southern part of Norway. The group was limited in terms of representativeness, but diverse in relation to profession, work place, gender, and length of experience. Transferability of the findings to other cultures and contexts must be handled carefully. We propose that the issues identified in our study generate new knowledge about the nature and experiences of anxiety in dementia that may guide further research.
Conclusion
Our findings suggest that anxiety in patients with dementia was understood as a reaction to loss and worries, and could be seen as existential in nature. With skilled observations of patient behavior and multidisciplinary assessments, it might be possible for clinicians to identify anxiety symptoms in patients with dementia. The participants stated that care interventions could be a way of preventing or reducing anxiety symptoms in this target group. However, when anxiety co-exists with depression, it might be difficult to attenuate anxiety symptoms by care measures alone. This is important knowledge for the health care personnel managing the anxiety of patients with dementia. There is a need for validated dementia-specific anxiety screening instruments for better identification and treatment of this morbidity. The controversies in the literature and the lack of knowledge in this particular area suggest a need to gain more in-depth knowledge of the complex phenomenon of anxiety in patients with dementia. We hope that the findings of this paper are seen as a contribution to a debate rather than an endeavor to find consensus.
Footnotes
Authors’ contribution
Alka R Goyal collected the data and was principally responsible for the analysis, though the process was continuously discussed with Siren Eriksen and Knut Engedal. All authors contributed to the drafting of the manuscript and the final critical revisions.
Acknowledgements
The authors would like to thank the participants for sharing their valuable clinical experiences. Thanks to Dr Oskar H Sommer for his idea of interviewing the clinicians about the topic.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Norwegian National Advisory Unit on Ageing and Health, Vestfold Hospital Trust, Norway [reference number 495000].