
Abstract
Dementia caregiving is thought to have a negative impact on health and wellbeing. This critical review of qualitative literature explored the lived experience of familial dementia caregivers from an occupational therapy perspective. The method was informed by systematic review and qualitative research methodologies and was structured within the occupational dimensions framework of doing–being–becoming–belonging. A comprehensive search of major databases was undertaken which identified 484 studies on the topic; 14 met the inclusion criteria and were included in the review. Ten themes emerged within the doing-being-becoming-belonging framework from the analysis of the studies. The occupational participation of caregivers is conveyed within the ‘doing’ domain. Ways in which caregiving impacts upon opportunities for self-nurture are presented within the ‘being’ domain. The ‘becoming’ domain elucidates ways in which caregivers redefine themselves, their values and their priorities through their caregiving role. The ‘belonging’ domain depicts ways in which caregivers’ connections with their care recipient and others are shaped over time. Practice implications for health and social care practitioners who work with familial dementia caregivers are presented in light of the findings.
Introduction
The majority of people diagnosed with dementia live in the community, with many becoming increasingly reliant upon the support of family members to enable them to sustain community living as their condition progresses (Ablitt, Jones, & Muers, 2009). It is estimated that there could be up to 670,000 informal dementia caregivers in the United Kingdom (Alzheimer’s Society, 2014), and family members are seen as a crucial form of this support (Department of Health (DH), 2009). The process of taking on a caregiving role is often experienced as an unexpected and unplanned role transition. Although for some people it can be a rewarding experience (Yap et al., 2010), providing support to a family member with dementia, frequently over a number of years, is recognised as being demanding and stressful and may have negative repercussions upon a caregiver’s health and wellbeing (Chung, 1997; Ory, Hoffman, Yee, Tennstedt, & Schultz, 1999).
The occupational therapy profession recognises that significant links between health, wellbeing and engagement in everyday activities, or occupations, exist, suggesting that occupational engagement and occupational balance influence a person’s health and wellbeing (Doble & Caron Santha, 2008; Law, Steinwender, & Leclair, 1998; Wilcock et al., 1998). Wilcock (1998) contends that achieving a dynamic balance between ‘doing’, ‘being’ and ‘becoming’ supports health and wellbeing. She encouraged occupational therapists to broaden their view of occupation from a focus on the visible, or doing, actions of people to consider it as a synthesis of doing, being and becoming. Rebeiro, Day, Semeniuk, O’Brien, and Wilson (2001) built on this premise and suggested that human beings also possess ‘belonging’ needs, relating to their connection with others.
Due to their understanding of the ways in which occupational engagement influences wellbeing, it has been identified that occupational therapists have a role in supporting familial dementia caregivers through enabling adjustment to changes in their routines and roles (College of Occupational Therapists (COT), 2010). Researchers have explored relationships between occupational engagement and wellbeing in dementia caregiving, identifying that it necessitates significant adjustments and adaptations to a caregiver’s roles, routines and support systems (Chung, 1997). This may result in decreased participation in meaningful occupations, threats to wellbeing and loss of occupational balance (Hwang, Rivas, Fremming, Rivas, & Crane, 2009). Systematic reviews of multi-disciplinary literature within an occupational therapy framework have additionally demonstrated that the notions of perceived responsibility and occupational adaptation are key factors in determining the wellbeing of caregivers (Thinnes & Padilla, 2011; Yong & Price, 2014).
The purpose of this thematic review was to analyse the findings from multi-disciplinary qualitative research studies on familial dementia caregiving within the framework of doing, being, becoming and belonging described above, in order to increase awareness of the impact of caregiving upon a person’s occupational experience and to identify factors which support adaptation and foster wellbeing. The question for the review was “What is the lived occupational experience of caregiving for family members caring for a relative with dementia in a community setting?”
Methodology
A thematic systematic literature review of published primary qualitative research was undertaken to answer the research question. A focus on qualitative research was deemed appropriate because it fits with the intention to understand the lived experience (Silverman, 2013) of dementia caregivers.
Search strategy
Inclusion and exclusion criteria.
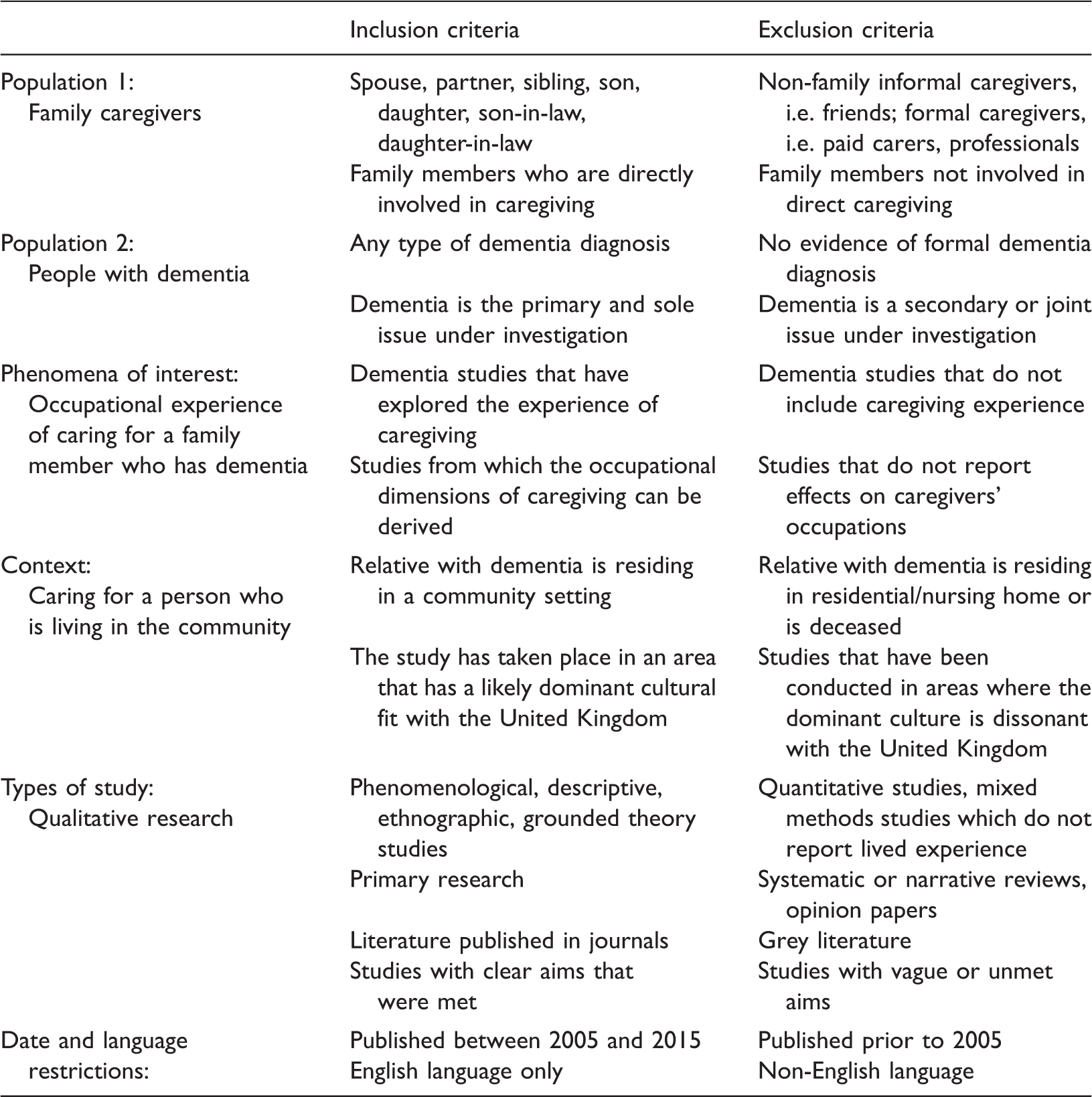
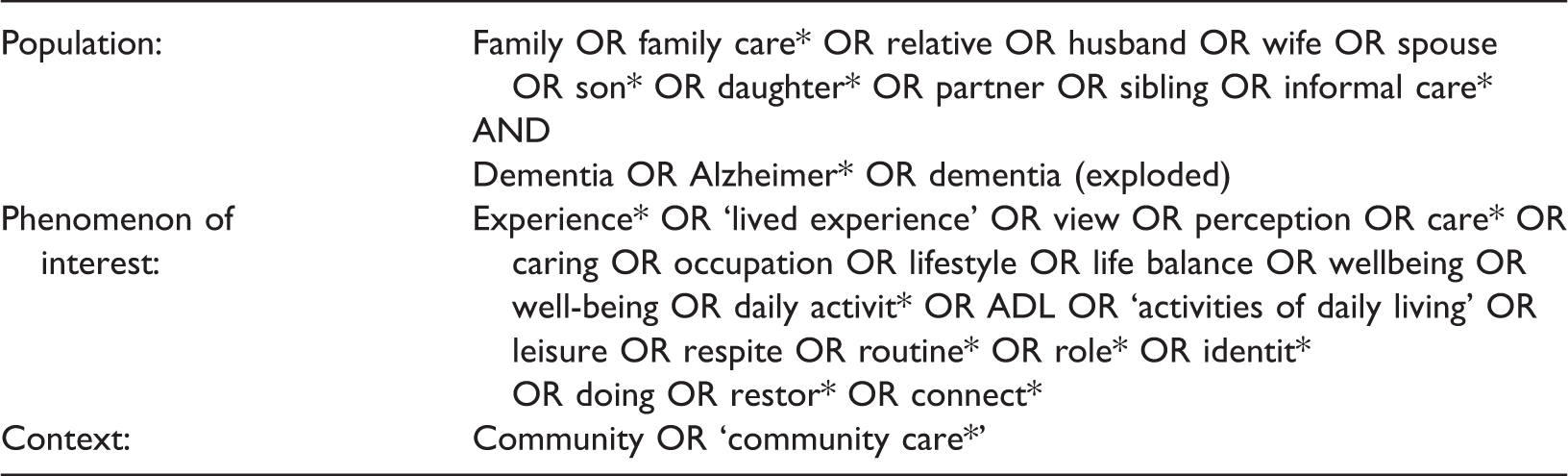
Key search terms.
Data extraction and analysis
A data extraction template was developed in order to support the thematic nature of the review. Thematic reviews use a conceptual framework to provide a lens through which to explore the literature (Yong & Price, 2014) and within the present review, the conceptual framework of occupation as a dynamic synthesis of doing–being–becoming–belonging (Wilcock, 1998; and also Rebeiro et al., 2001) was chosen to frame the analysis. The benefits of using this framework are twofold: providing a novel approach to exploring the occupational experience of dementia caregivers, and establishing whether this is a credible framework for this purpose (Noyes & Lewin, 2011). Key texts relating to the doing–being–becoming–belonging framework were reviewed in order to capture definitions, concepts and experience descriptors. These served to structure the analysis of the included literature.
In order to synthesise findings across the qualitative studies the Gewurtz, Stergiou-Kita, Shaw, Kirsh, and Rappolt (2008) approach of first order concepts, second order categories and third order interpretations was adopted. First-order concepts were formed through initial extraction and coding of data for each of the studies according to the domains of doing–being–becoming–belonging. Data from each domain were then amalgamated so that synthesis across the studies could commence. Emerging themes were annotated onto the text of the extracted data providing visual confirmation that all of the data had been systematically coded, representing second order categorisation. The themes that emerged from the data within each domain were interpreted from an occupational therapy perspective, representing third-order interpretation of the key concepts that were evident, and forming the findings of this review.
Search outcomes
The search outcomes are outlined in Figure 1 using a PRISMA flow-diagram (Moher, Liberati, Tetzlaff, Altman, & the PRISMA group, 2009).
PRISMA flow diagram of search outcomes.
Critical appraisal
A total of 14 papers were included in the review. Each of these was critically appraised by the first author under the supervision of the second author. The Letts et al.’s (2007a) critical review form for qualitative studies was used for this purpose. To enhance reliability, two independent reviews of one of the included papers were completed. Broad consensus was achieved between all parties during this exercise, engendering confidence in the trustworthiness of the appraisal.
Strengths and limitations were evident in varying degrees across the studies. Common strengths included adherence to ethical principles and provision of evidence regarding the rigour and trustworthiness of the research process (Hek & Moule, 2006). Limitations included poor justification for sample size, with only three studies reporting that data saturation was achieved. Several studies also failed to provide enough information about the sample characteristics to enable understanding of the ‘whole picture’ (Letts et al., 2007b). For example, information regarding the stage of dementia of the care recipient, and the length of time or the nature of caregiving (such as whether the respondent was the primary caregiver) was lacking in some studies. This information would have aided clarity about the credibility of the participants.
Study characteristics
Included studies: origin, design, sample characteristics, main findings and limitations.

All of the studies were cross-sectional in design, and the majority (9) adopted a phenomenological or hermeneutic phenomenological approach. Aside from a diary study conducted by Valimaki, Vehvilainen-Julkunen, Pietila, and Koivisto (2012), the studies used interviewing as the primary data collection method. Geographically, four originated in the United Kingdom or Southern Ireland, three from Scandinavia, two from Canada and five from the United States of America. The ethnicity of the participants was not always explicit, limiting understanding of the cultural context of the research (Joanna Briggs Institute, 2011). Purposive sampling was used in most of the studies, with sample sizes ranging from 2 to 83 (mean = 18). The majority of respondents were spousal caregivers (83%). As such, the findings and discussion within this review relate predominantly to the experiences of spousal caregivers.
Findings
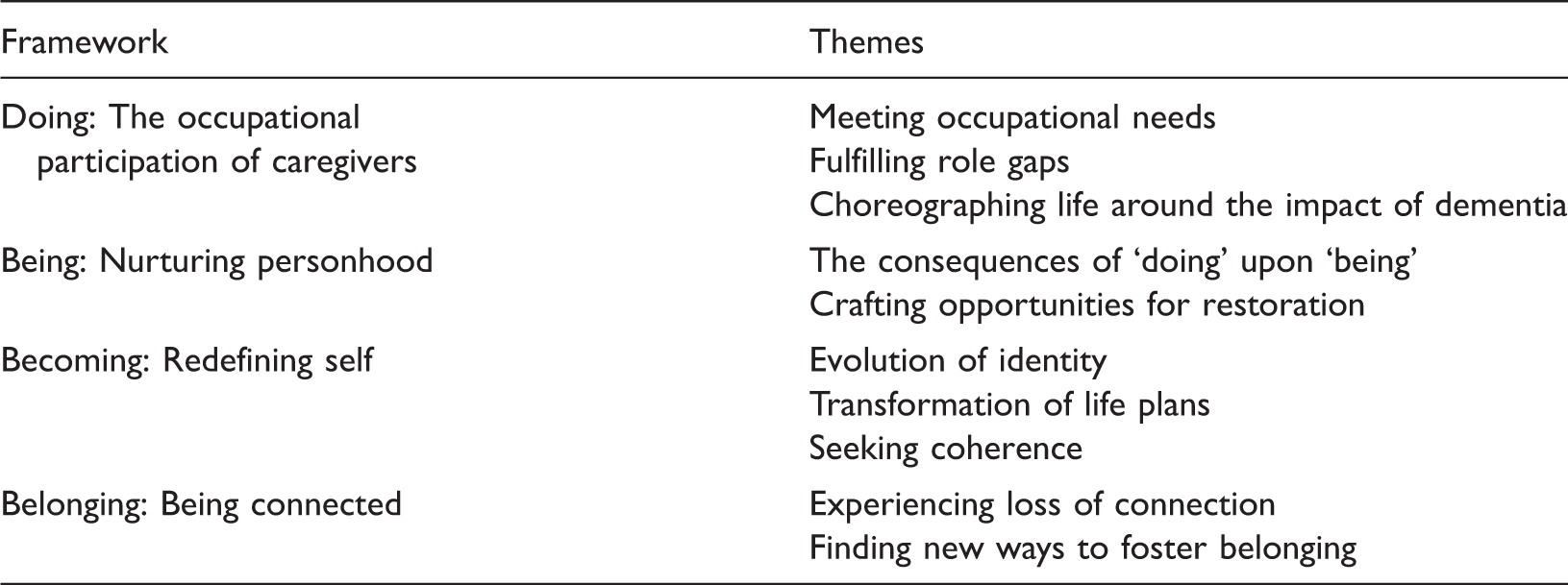
Themes within the doing–being–becoming–belonging framework.
Doing: The occupational participation of caregivers
The notion of ‘doing’, for occupational therapists, is a core construct. It is identified as being synonymous with occupation (Wilcock, 1998) and occupational performance (Doble & Caron Santha, 2008), and is considered to be the visible dimension of human occupation (Watson & Fourie, 2004).
Given the widespread conceptualisation of dementia caregivers being busy and ‘pulled’ in multiple directions, it is perhaps unsurprising that experiences regarding the act and implications of ‘doing’ are well represented in the literature. Three themes emerged: meeting occupational needs, fulfilling role gaps, and choreographing life around the impact of dementia.
Meeting occupational needs
Even before diagnosis, family members take increasing responsibility for providing support, initiating activities and preserving normality for their loved one (Ducharme, Kergoat, Antoine, Pasquier, & Coulombe, 2013; O’Shaughnessy, Lee, & Lintern, 2010; Valimaki et al., 2012), frequently bearing this duty alone (Massimo, Evans, & Benner, 2013). Meeting needs is an evolving and increasingly consuming experience, with caregivers finding themselves on a ‘continuous shift of duty’ (Valimaki et al., 2012), providing care or supervision to maintain their loved one’s safety (Persson & Zingmark, 2006; Quinn, Clare, Pearce, & van Dijhuizen, 2008; Walters, Oyebode, & Riley, 2010) as their condition progresses.
Caregivers go through a process of learning strategies to manage the changing abilities of their loved one (Massimo et al., 2013). It is evident that many make deliberate choices about how to deliver their support out of consideration for the care recipient, maintaining their involvement in such a way as to compensate for their needs whilst also supporting their unique personhood (O’Shaughnessy et al., 2010; Persson & Zingmark, 2006; Quinn et al., 2008; Valimaki et al., 2012). This may necessitate learning new skills that cross traditional gender boundaries, such as a husband applying make-up on his wife in order to maintain her appearance (Calasanti & Bowen, 2006).
As caregivers learn and implement successful strategies and approaches, they may experience validation, pride and satisfaction in their role (Calasanti & Bowen, 2006). In this regard, enabling their loved one to maintain their sense of personhood supports the wellbeing of both the care recipient and the caregiver (Persson & Zingmark, 2006).
Fulfilling role gaps
This theme was particularly evident in the accounts from spousal caregivers, as they took responsibility for the tasks that were previously performed by their partner with dementia in addition to their other obligations (Calasanti & Bowen, 2006; Ducharme et al., 2013; Hayes, Boylstein, & Zimmerman, 2009; Persson & Zingmark, 2006; Quinn et al., 2008; Valimaki et al., 2012). These multiple roles led to caregivers describing themselves as feeling ‘overwhelmed’ (O’Shaughnessy et al., 2010; Persson & Zingmark, 2006).
The experience of fulfilling role gaps may differ according to gender. Caregiving wives may find it more difficult to take on their husband’s roles than the act of providing care to their impaired spouse. This could be because they view providing care as a more natural extension of their existing role (Calasanti & Bowen, 2006; Furlong & Wuest, 2008). Caregiving husbands equally describe the process of adopting responsibility for roles previously fulfilled by their impaired wives as being challenging, especially when they take over tasks that are essential, such as food preparation. This potentially adds to the husband’s stress whilst he adapts to this new role. However, caregiver husbands display greater willingness to accept help with fulfilling these tasks (Calasanti & Bowen, 2006).
Choreographing life around the impact of dementia
Caregivers make major adjustments to their previous roles and routines as they increasingly choreograph their lives around the impact of dementia (Furlong & Wuest, 2008; Kjallman-Alm, Norbergh, & Hellzen, 2013; Walters et al., 2010). They experience erosion of opportunities to attend to their own occupations and many feel that their lifestyle and freedom become restricted as they become increasingly tied to the home (Persson & Zingmark, 2006; Quinn et al., 2008; Valimaki et al., 2012).
Caregiving may also impact on finances and lifestyle. This was particularly highlighted in studies conducted with people of working age, either spousal caregivers for people with young onset dementia (Flynn & Mulcahy, 2013), or adult children caring for a parent with dementia (Kjallman-Alm et al., 2013), who may have had to relinquish their paid occupation. Some struggle to meet financial obligations such as mortgages or childcare as a result of lost income or lack of statutory support.
Being: Nurturing personhood
In order to sustain their ability to fulfil this demanding role, caregivers need to address the loss of occupational balance that accompanies caregiving. Nurturing, sustaining and restorative occupations are essential in this regard. These elements represent Wilcock’s (1998) ‘being’ domain.
Occupational experiences relating to the concept of ‘being’ were present in the reviewed literature, but were minimally reported within the vast majority of the studies. Exceptions to this are the studies by Furlong and Wuest (2008), Persson and Zingmark (2006), and Watts and Teitelman (2005). Two themes emerged: the consequences of ‘doing’ upon ‘being’, and crafting opportunities for restoration.
The consequences of ‘doing’ upon ‘being’
Due to the impact of managing multiple demands on their time, caregivers find it difficult to carve out the space and energy to engage in self-nourishing activities (Hayes et al., 2009; Kjallman-Alm et al., 2013; O’Shaughnessy et al., 2010; Walters et al., 2010). They frequently relinquish interests that they previously valued, and which may have served as a source of pleasure (Quinn et al., 2008). In this sense, the demands of ‘doing’ subvert the opportunity to ‘be’. This loss of freedom is expressed through emotive language, including feeling ‘confined’ or ‘imprisoned’ (Valimaki et al., 2012; Walters et al., 2010), and being alone is viewed as a luxury (Ducharme et al., 2013; Quinn et al., 2008).
When caregivers are afforded the opportunity to have breaks, they frequently do not use these to engage in restorative activities, instead fitting as many other ‘doing’ tasks into their time away from direct caregiving as they can. Watts and Teitelman (2005) describe this phenomenon as ‘playing beating the clock’ (p. 285).
Tension exists for caregivers between meeting their own needs and the needs of the person they support, and often the welfare of the care recipient prevails (Furlong & Wuest, 2008; O’Shaughnessy et al., 2010). According to Wilcock (1998), a person’s wellbeing is dependent upon achieving a balance between ‘doing’ and ‘being’. It can be seen from these findings that caregivers are at significant risk of erosion of their wellbeing due to the loss of opportunity to engage in restorative occupations. Furlong and Wuest (2008) identify that the turning point which precipitates creation of a counter-balance commonly occurs when caregivers experience a negative change in their own health.
When a caregiver recognises the importance of creating a counter-balance, they become prepared to live with the potential negative consequences of taking a break. This includes willingness to take the risk of confrontation (Furlong & Wuest, 2008) and possible neediness of the care recipient upon their return (Watts & Teitelman, 2005). In this sense, they display readiness to make adjustments which enable them to nurture their sense of ‘being’.
Crafting opportunities for restoration
Caregivers identify a variety of strategies which they adopt in order to facilitate engagement in restorative occupations. One such strategy reported by Furlong and Wuest (2008), Persson and Zingmark (2006), and Watts and Teitelman (2005) is to engage in restorative activities alongside the care recipient. This may necessitate adjustment of the activity so that it provides a jointly positive experience, or mutual engagement in activities which require little cognitive demand, such as watching birds. Caregivers describe that engaging in such activities engenders joy, dignity and togetherness (Persson & Zingmark, 2006). This echoes with Hammell’s (2004) conceptualisation of ‘being’ as savouring the moment alongside special people, and represents a time of shared connection when the presence of dementia does not dominate (O’Shaughnessy et al., 2010).
Whilst engaging in joint activities may afford caregiver’s opportunities to nourish their ‘being’ needs, Furlong and Wuest (2008) and Persson and Zingmark (2006) identify the importance of creating opportunities for personal nourishment away from caregiving responsibilities. This generally requires organisation and planning ahead (Flynn & Mulcahy, 2013; Furlong & Wuest, 2008). However, Watts and Teitelman (2005) point to the benefit of being ready to take advantage of unscheduled opportunities as they arise, and this readiness may support opportunities for ad-hoc engagement in restorative occupations. Interestingly, for caregivers who are in employment, the workplace is identified as a space that affords respite from caregiving (Persson & Zingmark, 2006), indicating that occupations do not need to be overtly ‘relaxing’ to be nurturing.
The effects of meeting ‘being’ needs are predominantly positive in nature. Caregivers identify that they feel physically and mentally revitalised (Watts & Teitelman, 2005), enabling them to regain or maintain balance (Shim, Barroso, Gilliss, & Davis, 2013), and able to face the next challenge that they meet (Watts & Teitelman, 2005). These outcomes provide evidence that it is both possible and necessary to carve out opportunities for ‘being’, and doing so not only provides personal nourishment but also enables caregivers to sustain this role.
Becoming: Redefining self
Through becoming a caregiver, people experience a transformation from their former selves. They redefine their values and rethink their priorities (Hammell, 2009) in light of their new role. This evolution of occupational identity forms the notion of ‘becoming’ (Doble & Caron Santha, 2008). Embedded within this dimension is the process of change over time (Hammell, 2004) and a person’s sense of their future (Lyons, Orozovic, Davis, & Newman, 2002; Wilcock, 1998).
The experiences of caregivers relating to the dimension of becoming are well represented throughout the literature reviewed, and three themes emerged: evolution of identity, transformation of life plans and seeking coherence.
Evolution of identity
Caregivers perceive a significant change in their personal identity. Many express that their former identity has been subsumed by that of ‘caregiver’ (O’Shaughnessy et al., 2010), with some experiencing difficulty in accepting this label, feeling as if it has been imposed upon them rather than adopted out of choice (Massimo et al., 2013).
A caregiver’s relational identity towards their loved one also becomes reconfigured. Spousal wives, in particular, identify that they experience a change in their identity from ‘wife’ to ‘mother’ (Ducharme et al., 2013). Some wives express that this identity change precipitates feelings of resentment towards their husband, especially if he continues to display sexual libido whilst being unable to fulfil his role as a husband in other aspects (Hayes et al., 2009; Valimaki et al., 2012). Younger spousal caregivers may experience a strong sense of lifespan displacement, feeling that they have been pulled prematurely into ‘old age’ (Ducharme et al., 2013; O’Shaughnessy et al., 2010), whilst adult child caregivers find themselves acting as a parent to their own parent (Kjallman-Alm et al., 2013).
Caregivers may perceive a change in the fundamental identity of their loved one, viewing them as being a different person since the onset of dementia, whereas others continue to perceive them as being essentially the same person albeit with changes, signifying diversity of experience. Walters et al. (2010) provide useful insight into the impact of these differing perceptions, finding that caregivers who sought continuity were more able to manage change. This resonates with Hammell’s (2009) conceptualisation of continuity lying within the domain of ‘becoming’, and fostering wellbeing.
Transformation of life plans
The process of becoming a caregiver represents an unexpected life transition. According to Blair (2000) transitions such as these necessitate adjustment and adaptation, and the experiences of caregivers resonate with this concept as they reframe their life plans according to the demands of dementia. Plans for retirement, mid-life projects or employment are adjusted (Ducharme et al., 2013; Persson & Zingmark, 2006), and caregivers find themselves radically reinterpreting their expectations for the future (Massimo et al., 2013).
One of the manifestations of the ‘becoming’ domain is that occupations from the past are envisioned as continuing in the future (Hammell, 2009). There is little evidence of this in the experiences of dementia caregivers, who predominantly anticipate that life will become more difficult due to the foreseeable decline in their loved one (Valimaki et al., 2012). As such, many avoid thinking too much about the future, choosing instead to focus on the present. The future is generally perceived as being bleak (Flynn & Mulcahy, 2013) or depressing (Quinn et al., 2008) and uncertain (Ducharme et al., 2013), engendering hopelessness (Quinn et al., 2008).
However, some caregivers are able to achieve hope through deliberately choosing to focus on satisfactory elements of their lives and anticipating that they will grow accustomed to the changes that dementia creates; although these hopes are sometimes unrealistic, such as recovery from dementia (Valimaki et al., 2012).
Seeking coherence
Embedded within the notion of ‘becoming’ is the process of finding meaning in a situation (Lyons et al., 2002). It is evident that as some caregivers grow into their role they are able to make adjustments which foster meaning. These caregivers recognise that they are learning strategies which enable them to proactively manage challenges through problem-solving and learning through their experiences (Calasanti & Bowen, 2006; O’Shaughnessy et al., 2010; Shim et al., 2013; Valimaki et al., 2012; Walters et al., 2010). They display shared traits, demonstrating acceptance of their situation and recognition that they have a choice to make about how to approach their caregiving role, overtly choosing a positive attitude and determining to be happy about good moments when they occur (O’Shaughnessy et al., 2010; Quinn et al., 2008; Shim et al., 2013; Valimaki et al., 2012; Watts & Teitelman, 2005). Characteristics of altruism, trust, hope, love, compassion and empathy are evident, along with self-awareness and willingness to seek support (Shim et al., 2013). Some identify that they have a spiritual faith (Shim et al., 2013; Watts & Teitelman, 2005) and that the act of caregiving brings them emotionally closer to their loved one (Hayes et al., 2009; Valimaki et al., 2012).
Others, however, lack a sense of control over their circumstances and have difficulty in resolving life disruptions. These caregivers feel that they are living a life that they are not prepared for and over which they have little control (Ducharme et al., 2013; O’Shaughnessy et al., 2010). They may become resentful (Walters et al., 2010) and focus on the unfairness of their situation (Valimaki et al., 2012). A caregiver’s values, interests, health and emotional bonds affect their perceptions and influence how successfully they are able to resolve the disruptions that arise from ‘becoming’ a caregiver (Persson & Zingmark, 2006).
Doble and Caron Santha (2008) propose a number of factors which they believe underpin wellbeing, two of which are particularly pertinent to these findings, agency: exerting influence and choice about valued aspects of life, and coherence: engagement in occupations which confirm who a person is and wants to become. It can be seen that caregivers who make a positive choice about their role and find meaning within it display greater wellbeing than those who lack agency and coherence.
Belonging: Being connected
Individuals exist in connected relationships with others. Social interaction and mutual support are elements that underpin the occupational dimension of ‘belonging’ (Hammell, 2004, 2009). This dimension is well represented in the included literature and two main themes emerged: experiencing loss of connection and finding new ways to foster belonging.
Experiencing loss of connection
Many caregivers experience an increasing loss of meaningful connection and sense of alienation from their loved one as their condition progresses (Massimo et al., 2013; O’Shaughnessy et al., 2010). Loss of conversation, shared understanding and intellectual exchange are mentioned frequently in the included studies (Ducharme et al., 2013; Kjallman-Alm et al., 2013; O’Shaughnessy et al., 2010; Persson & Zingmark, 2006; Quinn et al., 2008; Walters et al., 2010). When caregivers experience a lack of confirmation regarding their actions they may feel burdened by having to make decisions alone (Persson & Zingmark, 2006; Quinn et al., 2008).
Additionally, caregivers frequently experience loss of reciprocity from their loved one (Quinn et al., 2008), a factor which is especially pertinent for spousal caregivers who may no longer feel ‘looked after’ themselves (Flynn & Mulcahy, 2013; Furlong & Wuest, 2008; Kjallman-Alm et al., 2013; Persson & Zingmark, 2006). This may leave them feeling unworthy of attending to their own needs, especially if they historically received external validation from their spouse (Hayes et al., 2009). The context of a person’s relationship history is important in shaping the degree to which such a loss of reciprocity impacts on the caregiver, being felt more keenly by those who have led a co-dependent life previously (Walters et al., 2010). In the midst of experiencing increasing separateness, occasions of support and comfort received from the person with dementia are especially valued (Shim et al., 2013).
Despite the erosion of meaningful reciprocal connection that caregivers experience, it is evident that many display strong motivation towards continuing to nurture their sense of belonging and togetherness. Some identify love as a motivating factor and continue to express their feelings even if these are not reciprocated (Hayes et al., 2009). Additionally, spouses, particularly husbands (Shim et al., 2013), and adult children (Kjallman-Alm et al., 2013) identify that caregiving provides them with the opportunity to reciprocate the love and care that they previously received from their loved one. Similarly, catching glimpses of the person their loved one used to be enables caregivers to feel reconnected (Furlong & Wuest, 2008). Moments of connection, however fleeting, are powerful motivators and support the caregiver to value the time they spend with their loved one. In this regard, interplay between the domains of ‘doing’, ‘being’, ‘becoming’ and ‘belonging’ can be seen.
Finding new ways to foster belonging
Due to the loss of companionship and affirmation that they experience, many caregivers will seek different ways in which they can foster their sense of belonging. Although caregivers are most likely to find relational support through their existing networks, they frequently report that their social circle diminishes as they find out who their supportive friends are (Flynn & Mulcahy, 2013; Hayes et al., 2009; Persson & Zingmark, 2006). Reducing the isolation that caregivers feel through engaging in reciprocal interactions with others can bring comfort (Quinn et al., 2008). Being understood and knowing that someone cares (Persson & Zingmark, 2006) may provide external validation that has been lost from the care recipient. Through attending a support group, some caregivers find acceptance, understanding and emotional support (O’Shaughnessy et al., 2010; Quinn et al., 2008). Whilst support groups may not appeal to every caregiver, they evidently engender validation and foster belonging for some.
Caregivers frequently need practical support to be in place for their care recipient in order to be able to access opportunities for gaining relational support (Furlong & Wuest, 2008), especially as their loved one’s condition progresses. However, many struggle to access or implement this for a variety of reasons relating to availability and acceptability. Some experience a lack of formal support through statutory organisations, and they express frustration about this (Flynn & Mulcahy, 2013). Others have found that even when such support is offered, it is not flexible enough to meet their needs (Ducharme et al., 2013). Additionally, some have difficulty in asking for support because they are not used to being dependent upon others (Shim et al., 2013), necessitating a behavioural shift for these caregivers (Furlong & Wuest, 2008).
Once support has been offered or requested, caregivers may also have difficulty in accepting it. Watts and Teitelman (2005) identified that caregivers need to trust in another person’s ability to provide care as well as they can, and to perceive that the offer of support is genuine. Additionally, when they fear a negative reaction from the care recipient towards the substitute caregiver, or when the care recipient exhibits distress at their being out of sight, caregivers may resist accepting support. Although both instrumental and relational supports are important factors in enabling caregivers to foster ways of ‘belonging’, the process is not necessarily straightforward.
Discussion and conclusions
The purpose of this thematic review was to understand the lived experience of familial dementia caregivers from an occupational therapy perspective, through extracting data from multi-disciplinary qualitative literature within the conceptual framework of doing, being, becoming and belonging. The findings have demonstrated that taking on this role leads to dramatic changes for caregivers, who not only find that their lives are increasingly arranged around the needs of their loved one, but commonly find themselves also having to master unfamiliar tasks as they take responsibility for those previously fulfilled by the care recipient (Calasanti & Bowen, 2006; Hayes et al., 2009; Persson & Zingmark, 2006; Quinn et al., 2008; Valimaki et al., 2012). Whilst the act of caregiving is evidently a valued occupation (Kielhofner, 2008), with caregivers demonstrating strong conviction that what they are doing is important, managing these multiple demands may lead to erosion of their health and wellbeing as they lose opportunities to engage in personally restorative occupations. In many ways, they are ‘over-occupied’ (Wilcock, 1998) and risk finding themselves in a state of occupational imbalance (Townsend & Wilcock, 2004) as the demands of ‘doing’ usurp opportunities for ‘being’. The occupation of caregiving not only affects the way in which caregivers structure their time and priorities, but also transforms their identity in relation to their loved one with dementia and to wider society. Caregivers’ support systems inevitably change as their loved one’s ability to provide reciprocal support is eroded by the impact of dementia. They may find themselves feeling isolated and marginalised, especially if they perceive that they are left to cope alone (Furlong & Wuest, 2008; Hayes et al., 2009; O’Shaughnessy et al., 2010; Persson & Zingmark, 2006).
Whilst it is evident that these issues are salient across caregivers, there appears to be a juxtaposition of experience whereby some are able to adapt to their new role, finding purpose, meaning and personal growth through their caregiving experience (Shim et al., 2013), whereas others find themselves in a state of dysfunction (Whiteford, 2000). The findings of this review therefore support those of Yong and Price (2014), in that successful adaptation is a significant factor in determining wellbeing for dementia caregivers.
The notion of adaptation is well recognised within the occupational therapy profession (Kielhofner, 2008; Turpin & Iwama, 2011), and is thought to be linked to periods of transition (Collins, 2014). Dementia caregivers are essentially living in a perpetual state of transition as they manage the continually changing needs of their loved ones, and therefore the adaptation process is significant. This review has demonstrated that the experience of caregiving is shaped by a range of internal and external influences, and has elucidated aspects of lived experience relating to identity, competence and the caregiver’s environment which the authors consider to be significant in shaping the degree to which adaptation is successfully achieved. These factors are of importance to health and social care professionals who are working with dementia caregivers in a number of ways.
Clinical implications
Caregivers demonstrate high levels of motivation but providing care is a physically and emotionally demanding role. With relation to meeting their ‘doing’ needs, the findings suggest that successful occupational adaptation is underpinned by perseverance, support and recognition of development in their ability to meet their loved one’s needs. Establishing what factors enable growth and role mastery, and exploring how caregivers can retain a breadth of occupational participation that remains in congruence with their values may aid adaptation. Adopting a coaching approach could be beneficial in this regard.
The occupation of ‘caregiver’ is so dominant that it takes precedence over caregivers’ wider needs, potentially impacting negatively on their health and wellbeing. Successful occupational adaptation occurs when caregivers are able to address threats to imbalance in their lives. If they succeed in creating opportunities to nurture their ‘being’ needs, it enables them to continue ‘doing’ this valued occupation. Supporting caregivers’ readiness to make these adjustments may aid effective adaptation.
Relatives of people with dementia are on a difficult journey of learning how to ‘become’ a caregiver. Their perceptions of choice and control within this are important. Those who identify that they have chosen to take on this role are more likely to experience coherence with their identity. Promoting agency in caregivers through establishing which aspects of their life bring meaning and satisfaction, and supporting them to exert influence within their lives may facilitate successful adaptation.
Having a sense of belonging seems to be particularly pertinent for spousal caregivers due to the loss of connection and reciprocity they experience. Adaptation could be promoted through engagement in mutual activities which enhance connection, thereby nurturing both ‘being’ and ‘belonging’ within the care provider–care recipient relationship. Establishing how caregivers connect with others and supporting them to implement strategies to foster these relationships may also engender adaptation.
Strengths and limitations of the review
A theoretical conceptualisation of occupation as a synthesis of doing–being–becoming–belonging (Wilcock, 1998; and also Rebeiro et al., 2001) was used to guide analysis of the literature included in this thematic critical review. This framework provided a novel approach to exploring and framing the experiences of dementia caregivers, and strengthens appreciation that the occupational experience of caregivers extends beyond the visible manifestation of ‘doing’. Whilst using a theoretical framework to guide data extraction has been highlighted as being a beneficial way to maintain focus on findings which are relevant to the research question (Noyes & Lewin, 2011), consideration was given as to whether taking such an approach resulted in manipulation of the data in order to ‘make the shoe fit’ (Lyons et al., 2002). To address this, the first author evaluated whether any data relating to occupational experience did not fit within these categories and concluded that there was sufficient scope within the existing framework to capture breadth of experience fully, lending credence to the rigour of this theoretical framework.
The findings of this review should be interpreted in light of the characteristics of the studies included. The studies were identified as a result of the inclusion and exclusion criteria, and the assumptions and restrictions that guided the development of these may have led to bias in the findings. For example, relevant articles could have been lost through date, language and publication restrictions, with the findings representing a predominantly female, spousal, Western, cross-sectional view of dementia caregivers. Consideration of the transferability of the findings should be borne in mind in light of this. Future systematic reviews which include a wider demographic could elucidate possible cultural differences in the caregiving experience. Nevertheless, this review has shed light onto the lived experience of dementia caregivers and has identified factors which support role adaptation and foster wellbeing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.