
Abstract
The goal of this study was to estimate the rate of the progression of mild cognitive impairment to dementia and identify the potential risk factors in German specialist practices from 2005 to 2015. This study included 4633 patients aged 40 years and over from 203 neuropsychiatric practices, who were initially diagnosed with mild cognitive impairment between 2005 and 2013. The primary outcome was diagnosis of all-cause dementia recorded in the database until the end of the five-year follow-up period. Cox regression models were used to examine mild cognitive impairment progression to dementia when adjusted for confounders (age, sex, and health-insurance type). The mean age was 68.9 years and 46.6% were men. After the five-year follow-up period, 38.1% of women and 30.4% of men had been diagnosed with dementia (p < 0.001). The share of subjects with dementia increased with age, rising from 6.6% in the age group of ≤ 60 years to 64.7% in the age group of > 80 years (p < 0.001). Men were at a lower risk of being diagnosed with dementia than women (hazard ratio = 0.86). Patients in the age groups 61–70, 71–80, and > 80 years also had a higher risk of developing this psychiatric disorder, with hazard ratios ranging from 3.50 to 11.71. Finally, mild cognitive impairment was less likely to progress to dementia in people with private health-insurance coverage than in people with public health-insurance coverage (hazard ratio = 0.69). Around one in three patients developed dementia in the five years following mild cognitive impairment diagnosis. Sex, age, and type of health insurance were associated with this risk.
Introduction
In Germany, mild cognitive impairment (MCI) is a concept that has mainly been applied in the context of research (Kaduszkiewicz et al., 2014; Luck et al., 2007). The International Classification of Diseases (ICD-10), which must be used as the diagnostic manual in German practices, has conceptualized MCI as a general form of cognitive condition rather than a preclinical stage of dementia. This latter concept has recently been added to the fifth version of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013).
Several European studies have suggested that the prevalence of missed or delayed diagnoses of dementia is potentially high in primary care (Eichler, Thyrian, Teipel, & Hoffmann, 2015; Vernooij-Dassen et al., 2005). In view of these findings, general practitioners are aware of the importance of systematically detecting dementia, and there is both a need and a desire to implement methods to detect the condition in routine care (Bohlken, Peiseler, & Kohlmann, 2015; Stoppe, Haak, Knoblauch, & Maeck, 2007; Thyrian et al., 2016). Dementia detection in ambulatory medical care is of particular importance in Germany since high rates of attendance for ambulatory medical care have been recorded among the elderly population (van den Bussche et al., 2016). Surprisingly, little data are available concerning the share of MCI detection in such practices (van den Dungen et al., 2015). Recent investigations based on pharmacoepidemiological databases have shown very low rates in Germany (Bohlken et al., 2015), underlining the fact that practitioners are familiar with neuropsychological evaluations (Thyrian & Hoffmann, 2012), but such evaluations are seldom performed in primary care (Schulz, Bohlken, Hering, & Bätzing-Feigenbaum, 2014). While self-referrals to dementia specialists such as neurologists or psychiatrists are possible, patients are most often referred to these specialists by their general practitioners (GPs; Eisele et al., 2010). Interestingly, it has been discovered that numerous factors (e.g., comorbid disorders, cognitive functions, or age) are associated with this progression rate to a significant extent (Amieva et al., 2004; Kaduszkiewicz et al., 2014; Palmer, Bäckman, Winblad, & Fratiglioni, 2008; Roberts et al., 2014).
The goal of the present study was to estimate the rate of the progression of MCI to dementia and identify the potential risk factors in the routine setting of German specialist practices from 2005 to 2015.
Methods
Database
The Disease Analyzer database (IMS HEALTH) compiles drug prescriptions, diagnoses, basic medical, and demographic data obtained directly and in an anonymous format from computer systems used in the practices of resident physicians (Becher, Kostev, & Schröder-Bernhardi, 2009). Diagnoses (ICD-10), prescriptions (Anatomical Therapeutic Chemical (ATC) Classification System), and the quality of reported data have been monitored by IMS based on a number of criteria (e.g., completeness of documentation, linkage between diagnoses, and prescriptions).
In Germany, the sampling methods used for the selection of physicians’ practices were appropriate to obtain a representative database of general and neuropsychiatrist practices (Becher et al., 2009). Prescription statistics for several drugs were very similar to data available from pharmaceutical prescription reports (Becher et al., 2009). The age groups for the given diagnoses in Disease Analyzer also agreed well with those in the corresponding disease registries (Becher et al., 2009). Finally, this database has already been used in several studies focusing on dementia and other psychiatric disorders (Bohlken, Jacob, Schaum, Rapp, & Kostev, 2015; Bohlken, Weber, Rapp, & Kostev, 2015; Booker, Bohlken, Rapp, & Kostev, 2016; Booker, Jacob, Rapp, Bohlken, & Kostev, 2016).
Study population
This study included patients aged 40 years and over from 203 neuropsychiatric (NP) practices who were initially diagnosed with MCI between 2005 and 2013 (index date). The follow-up period lasted up to five years and finished in December 2015. Exclusion criteria were dementia diagnosis, Parkinson’s disease diagnosis, or antidementive prescriptions prior to the index date (Figure 1). After these criteria had been applied, 4633 patients were included in the analysis.
Flow chart for selection of patients with MCI to be included in the study. MCI: mild cognitive impairment.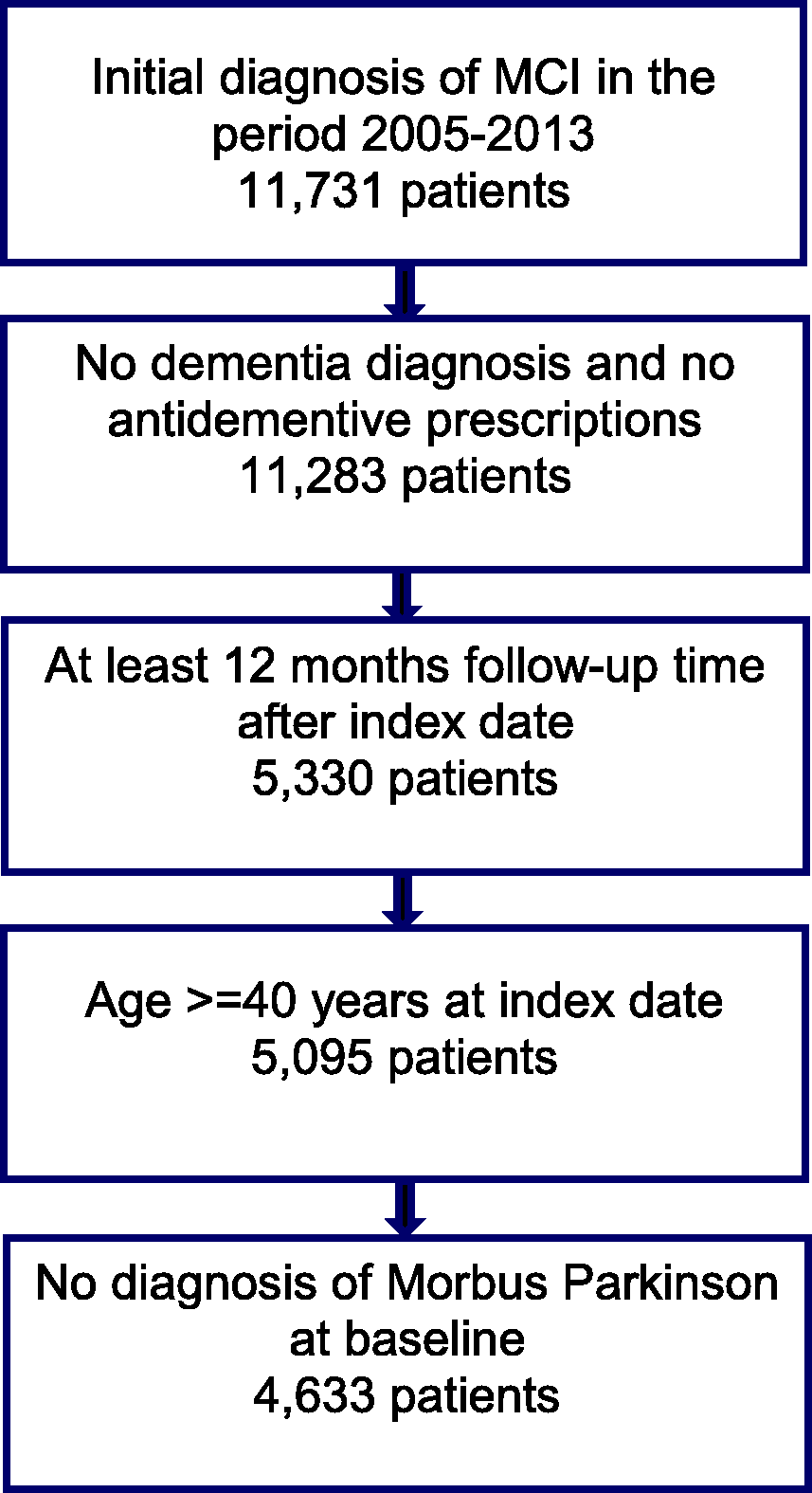
Study outcome
The primary outcome was diagnosis of all-cause dementia recorded in the database between the index date and the end of the follow-up period. The assessment of dementia diagnoses was based on ICD codes for vascular dementia (F01), unspecified dementia (F03), or Alzheimer’s disease (G30).
Independent variables
Demographic data included age, sex, and health-insurance type (private or statutory). Depression (F32 and F33) and stroke (I63, I64, and G45), which are potentially associated with MCI progression to dementia, were also determined.
Statistical analysis
Descriptive analyses were obtained for all demographic and clinical variables and mean ± SDs were calculated for normally distributed variables. Kaplan–Meier curves were used to analyze the proportion of patients with dementia over time. Finally, multivariate Cox regression models were used to examine MCI progression to dementia when adjusted for confounders (age, sex, and health-insurance type). Values of p < 0.05 were considered statistically significant. Analyses were carried out using SAS version 9.3.
Results
Characteristics of MCI patients in German neuropsychiatrist practices.
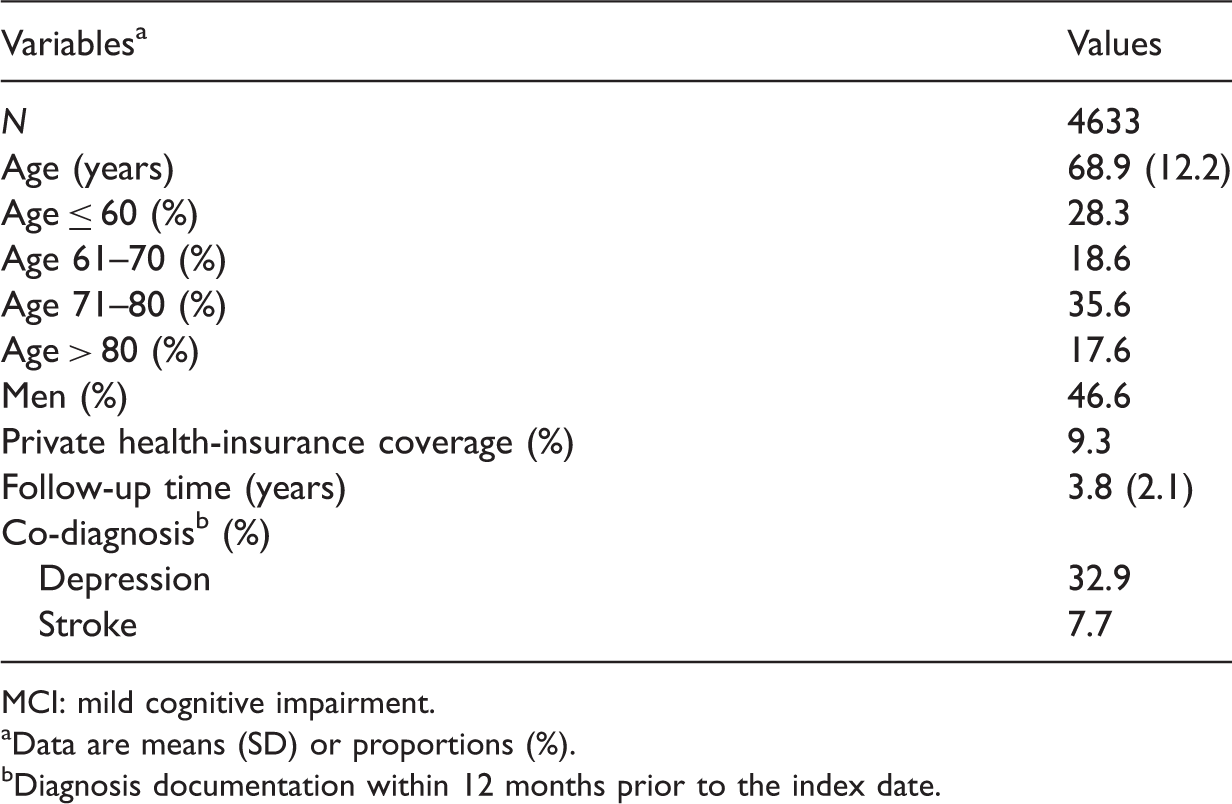
MCI: mild cognitive impairment.
Data are means (SD) or proportions (%).
Diagnosis documentation within 12 months prior to the index date.

Kaplan–Meier curves for time to dementia diagnosis in MCI patients by sex. MCI: mild cognitive impairment.
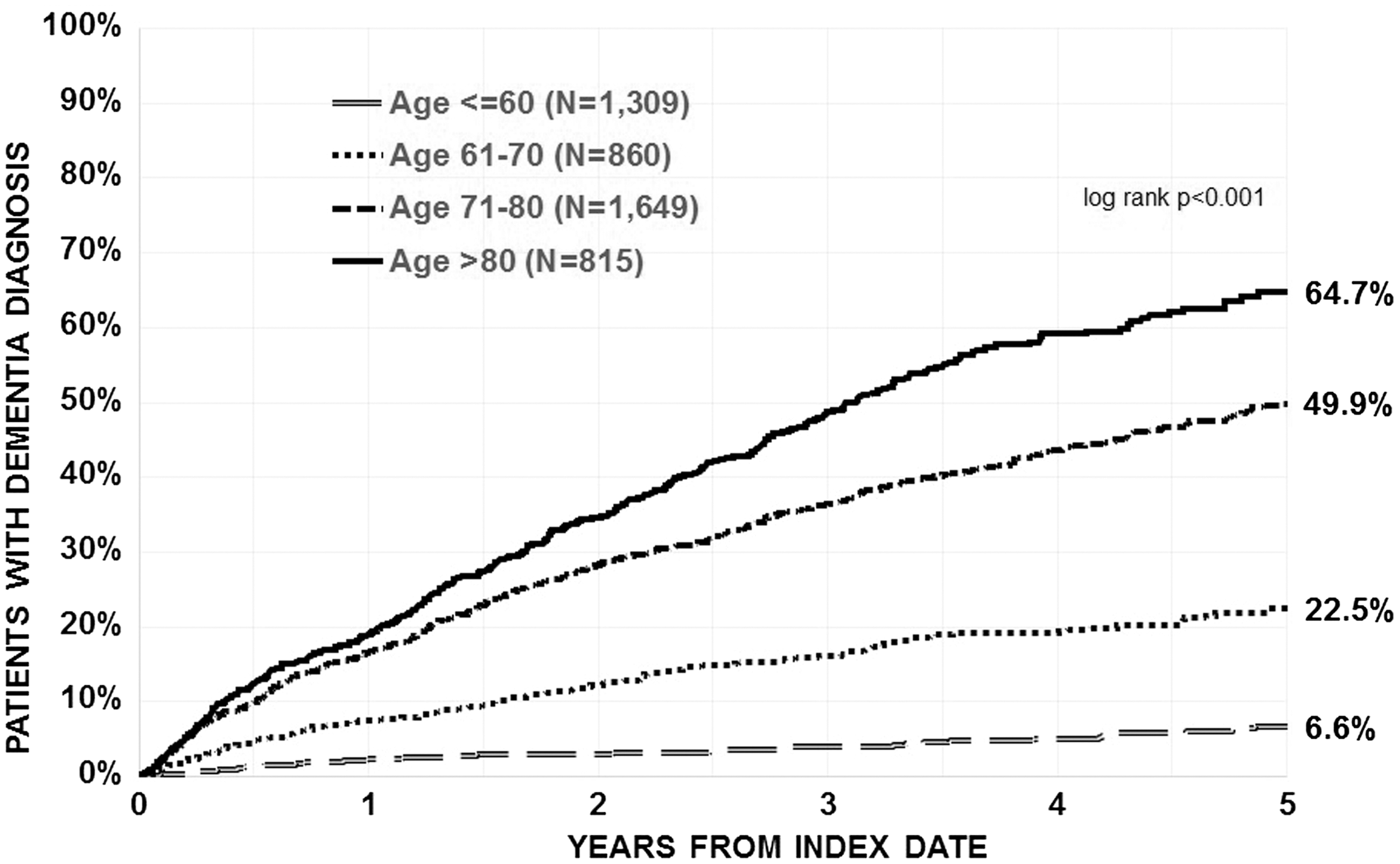
Kaplan–Meier curves for time to dementia diagnosis in MCI patients by age. MCI: mild cognitive impairment.
Multivariate Cox regression model for dementia diagnosis in MCI patients (stepwise selection).

CI: confidence interval; MCI: mild cognitive impairment.
Only variables with significant effect are included in the table.
Discussion
The present retrospective study found that more than one-third of the individuals treated in German NP practices developed dementia in the five years following MCI diagnosis. The share of patients diagnosed with dementia was higher in women than in men. Furthermore, this share also increased with age. The multivariate Cox regression model showed that women, older people, and patients with public health-insurance coverage were at a higher risk of dementia diagnosis than men, younger people, and people with private health-insurance coverage.
The prevalence of MCI in the elderly people has been studied by several authors in Germany. Busse, Bischkopf, Riedel-Heller, and Angermeyer (2003) discovered in a population-based study that MCI prevalence ranged between 1% and 15%. Individuals diagnosed with MCI progressed to dementia at a rate of 10%–55% over a 2.6-year period, depending on the subclassifications of the psychiatric disorder (Busse et al., 2003). Later, Luck et al. (2007) corroborated these findings when they found in general practices that between 15% and 25% of elderly people were affected by MCI depending on the definition of the condition. Interestingly, MCI was positively related to age, apoE ɛ4 allele, vascular diseases (notably stroke and peripheral arterial obstructive disease), and symptoms of depression (Luck et al., 2007). While previous studies had failed to clarify the impact of age and sex on MCI occurrence in full (Panza et al., 2005), these new data brought new evidence to light that supported the theory that these factors were associated with this disorder to a significant extent and highlighted the importance of intensive management for older women in particular. Although all of these analyses found similar rates of MCI in the elderly people (Artero, Petersen, Touchon, & Ritchie, 2006; Busse et al., 2003; Luck et al., 2007; Ritchie, Artero, & Touchon, 2001), it is important to bear in mind that the real prevalence of this chronic condition may have been underestimated. As a matter of fact, it is possible that patients with severe mental disorders may simply stay at home or live in nursing homes, and are therefore not seen by GPs (Lawrence & Kisely, 2010). Moreover, in the case of the study by Luck et al., 22.9% of the invited individuals could not be contacted by investigators and 26.8% refused to participate.
In their review, Eschweiler, Leyhe, Klöppel, and Hüll (2010) underlined the fact that MCI, which is a preclinical form of Alzheimer’s disease, may last as long as five years until the onset of dementia. Thus, intensive detection of dementia in elderly people affected by MCI is possible and highly recommended by health professionals (Ambigga et al., 2011), particularly in ambulatory medical care, where a substantial share of the German population over the age of 60 years is monitored (van den Bussche et al., 2016). The main goal of such detection for GPs and neuropsychiatrists is to distinguish between people with progressive forms of the disease and those with remittent and stable courses. In the first case, the aim of the follow-up is to delay the onset of dementia and to diagnose the mental disorder as soon as possible. In the latter case, the aim is to focus on the daily management of MCI symptoms.
In 2014, a study conducted on older individuals with MCI who were interviewed over a period of three years found that around 22% of them had progressed to dementia (Kaduszkiewicz et al., 2014). By contrast, 41.5% of the population displayed remission of symptoms with normal cognitive function, 21.3% had a fluctuating course, and 14.8% showed stable symptoms (Kaduszkiewicz et al., 2014). In line with the literature, the authors also found that age, depression, and impairment in more than one cognitive domain were positively associated with the risk of developing dementia (Kaduszkiewicz et al., 2014). Interestingly, the result of a test based on the ability to learn new material and reproduce it 10 minutes later was found to be the best tool for distinguishing between baseline patients with constant MCI and patients with progressive MCI (Kaduszkiewicz et al., 2014). This study corroborated the findings of a previous American analysis in which almost 29% of the individuals with MCI included were diagnosed with dementia over the median follow-up period of 5.1 years and in which the risk of progression to dementia was found to be 23 times higher in MCI cases than in controls (Roberts et al., 2014). In line with these two works, the current study showed that the share of dementia was high in MCI patients five years after diagnosis, and that sex and age were risk factors for MCI progression to dementia. Moreover, it was underlined that people with public health-insurance coverage had a higher risk of progression to dementia than people with private health-insurance coverage. This last result clearly highlighted the importance of personalized follow-up on MCI patients with low incomes in Germany. In addition to higher incomes, most people with private health insurance also have a higher level of education. Tifratene, Robert, Metelkina, Pradier, and Dartigues (2015) showed for a public sample that a higher level of education is a protective factor.
In general, retrospective primary-care database analyses are limited by the degree of completeness of the data on which they are based. The major limitation was related to the medical diagnoses performed by the neuropsychiatrists, since these could not be documented fully. Data on socioeconomic status and lifestyle-related risk factors were also unavailable. Moreover, psychiatrists do not document cardiovascular or endocrine diagnoses like diabetes or hypertension, which can also be risk factors for dementia. Finally, additional detailed data on MCI and dementia diagnoses were lacking, so that in the diagnosed patients, no information was available regarding the extent to which the diagnoses were made, for example, whether they were made solely on a clinical basis or by means of additional validated questionnaires.
The strengths of this work are the number of patients, the various types of dementia included in the analysis, and the fact that it is the first study to use routine data from practices, which is also used for insurance companies.
Around one in three patients developed dementia in the five years following MCI diagnosis. Age, sex, and type of health insurance were the risk factors for MCI progression to dementia. Further studies are needed to gain a better understanding of the impact of potential comorbid diagnoses on this progression.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.