
Abstract
Spirituality is an important aspect of humanity. Concerned with deriving meaning from events, and connection with others, it provides a mechanism for some to cope with illness and disability. While spiritual support is recognised as important, little is known about the spiritual needs of those people experiencing dementia. This meta-synthesis considers the experiences of spirituality from the perspective of people living with a diagnosis of dementia. Using a review protocol, key words from a preliminary scoping review were used to direct database searches in November 2013. A total of 667 papers were initially identified. However, following careful quality review assessment a final eight papers were selected. Findings demonstrated the ongoing importance of spirituality to people living with dementia and its importance as a means of finding hope, meaning and linkage with past, present and future. Expression of spirituality through faith practices, contact with faith communities, and the impact of dementia on these, were also highlighted.
Introduction
The term spirituality is derived from Latin and refers to ‘breath of life’ (Brillhart, 2005, p. 31). Spirituality is frequently conceptualised in terms of being at the core of who we are (Eliopoulous, 2014; Frankl, 1963; Narayanasamy, 2010). While no universally agreed definition is available, we believe the description presented by McSherry (2009, cited in McSherry & Smith, 2012), is particularly apt in relation to dementia, as it is not reliant on intellectual capacity, whereas others require cognitive awareness to experience spiritual needs (Weathers, McCarthy, & Coffey, 2015). This description suggests spirituality is: universal, deeply personal and individual; it goes beyond formal notions of ritual or religious practice to encompass the unique capacity of each individual. It is at the core and essence of who we are, that spark which permeates the entire fabric of the person and demands that we are all worthy of dignity and respect. It transcends intellectual capability, elevating the status of all humanity to that of the sacred. (McSherry, 2009, cited in McSherry & Smith, 2012, p. 118)
Methods
Systematic reviews occupy a vital role in the process of making sense of research findings to inform healthcare decisions through the ‘identification, critical appraisal and summary of evidence’ (Handoll & Smith, 2004, p. 227). They are a key contributor to evidence-based healthcare (Khan, Kunz, Kleijnen, & Antes, 2003). Meta-synthesis is a particular systematic review approach to the synthesis of the findings of qualitative research studies with the intent to produce a new or expanded understanding or interpretation of a pre-defined research question (Cooke, Smith, & Booth, 2012; Korhonen, Hakulinen-Viitanen, Jylha, & Holopainen, 2013). According to Korhonen et al. (2013), the synthesis of qualitative research introduces a patient or person-focused standpoint to evidence-based practice.
The term meta-synthesis is used to refer to a number of differing approaches to the synthesis of qualitative research, including thematic synthesis (Hannes & Lockwood, 2011), meta-aggregation (Korhonen et al., 2013; The Joanna Briggs Institute, 2011); and meta-ethnography. This meta-synthesis employed a meta-ethnographic approach, which focuses on generating new knowledge through interpretation to produce theory or explanatory models (Booth, Papaioannou, & Sutton, 2012; Noblit & Hare, 1988). The form of meta-ethnography that was found to be most applicable in the current systematic review was reciprocal translation in which concepts or metaphors across studies are similar or new metaphors can be used to apply to interpretations from a set of studies (Noblit & Hare, 1988; Thorne, Jensen, Kearney, Noblit, & Sandelowski, 2004). A systematic review protocol was devised by the review team to inform the conduct of the review. The components of this protocol were not altered during the systematic review process, so that faithfulness to the aim of the systematic review was ensured.
Aim and objectives
The aim of this systematic review was to establish the experience of spirituality from the perspective of people living with dementia. The specific objectives were:
To review the available empirical evidence relating to the experience of spirituality from the perspective of the person living with dementia. To collect data on the experience of spirituality from the perspective of the person living with dementia. To produce an interpretation of the research phenomenon. To integrate the retrieved data to produce a new higher order interpretation of the experience of spirituality in dementia with which to enhance understanding.
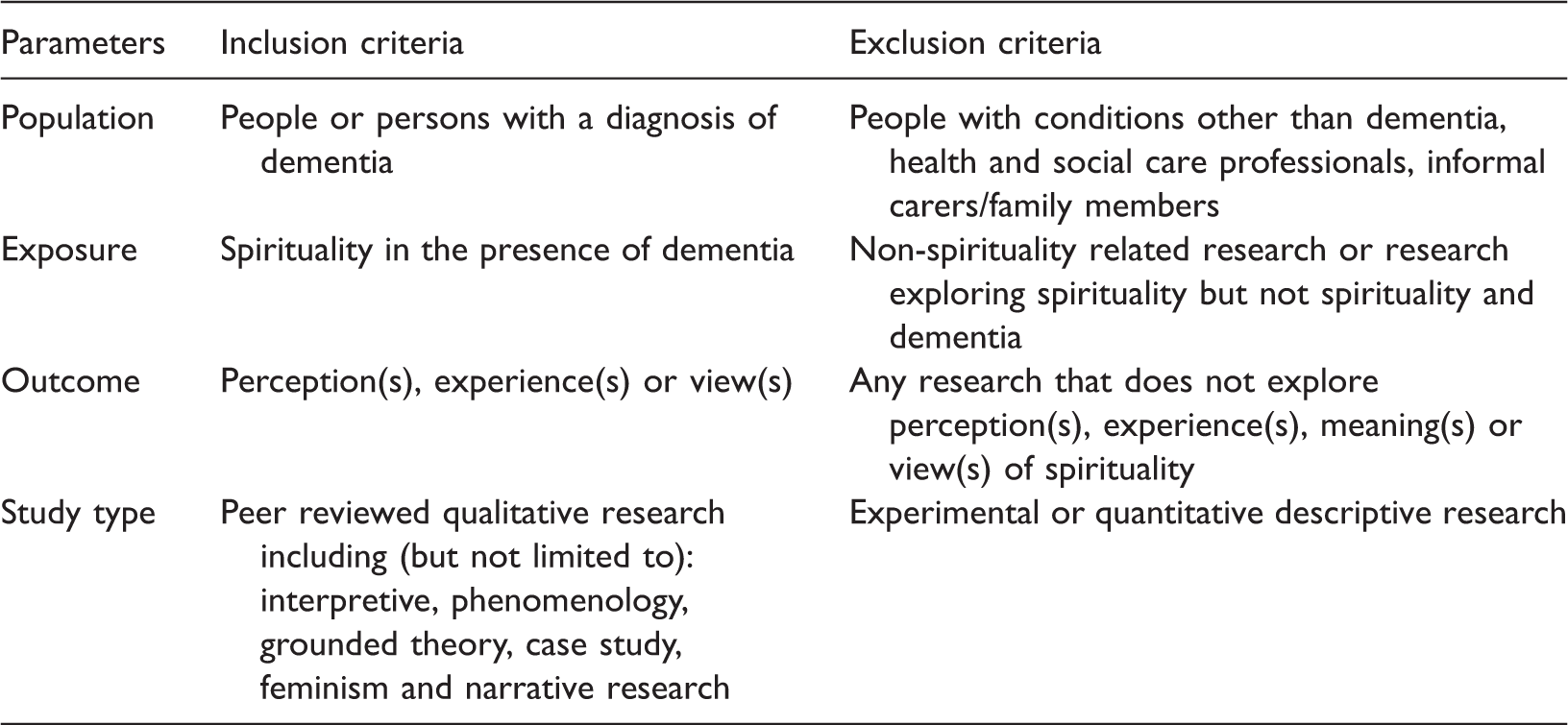
Inclusion and exclusion criteria
Inclusion and exclusion criteria.
Literature search strategy
Search terms used to retrieve relevant literature.
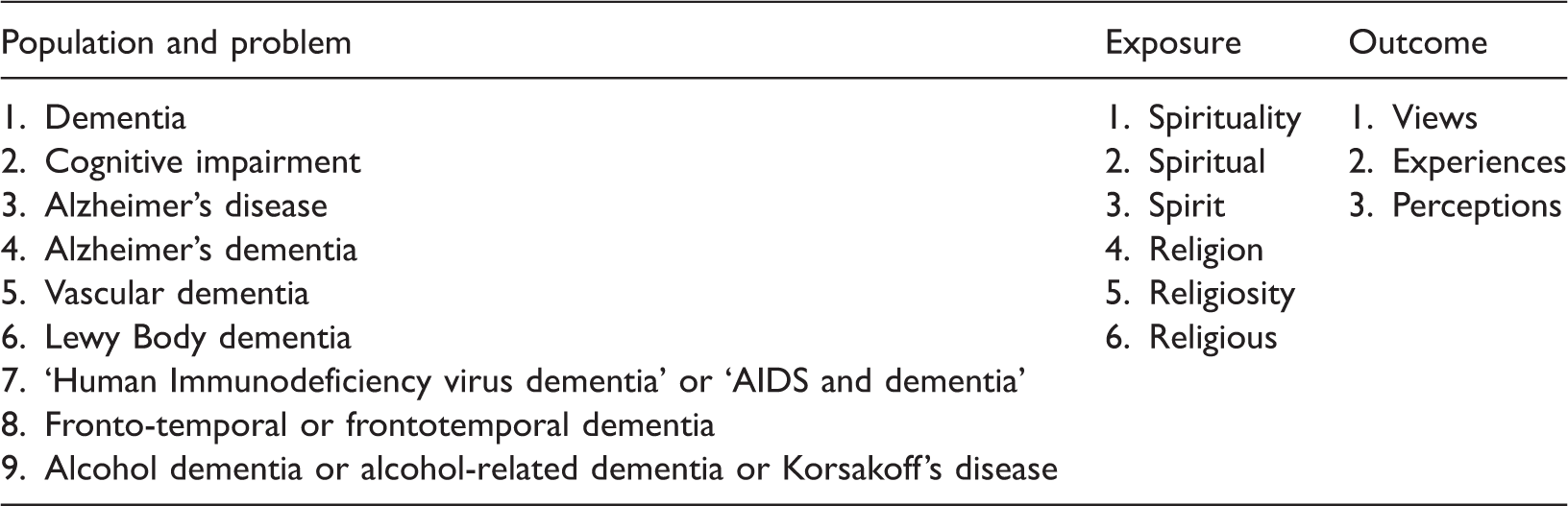
Each set of keywords was firstly combined using the Boolean operator ‘Or’ and then the outcome of each set was combined using ‘AND’. Where appropriate each database was searched using free text searches and a thesaurus or MesH search. No timeframe was applied. The only search limitation used was ‘English language’. In addition, the indexes of the following journals were searched: Dementia The international journal of social research and practice, Journal of Christian Nursing, Journal of Religion and Health, Mental Health, Religion and Health, and the Journal of Holistic Nursing, as were the reference lists of all retrieved studies. Figure 1 provides an overview of the search and selection process.
Flow diagram of the search and selection process.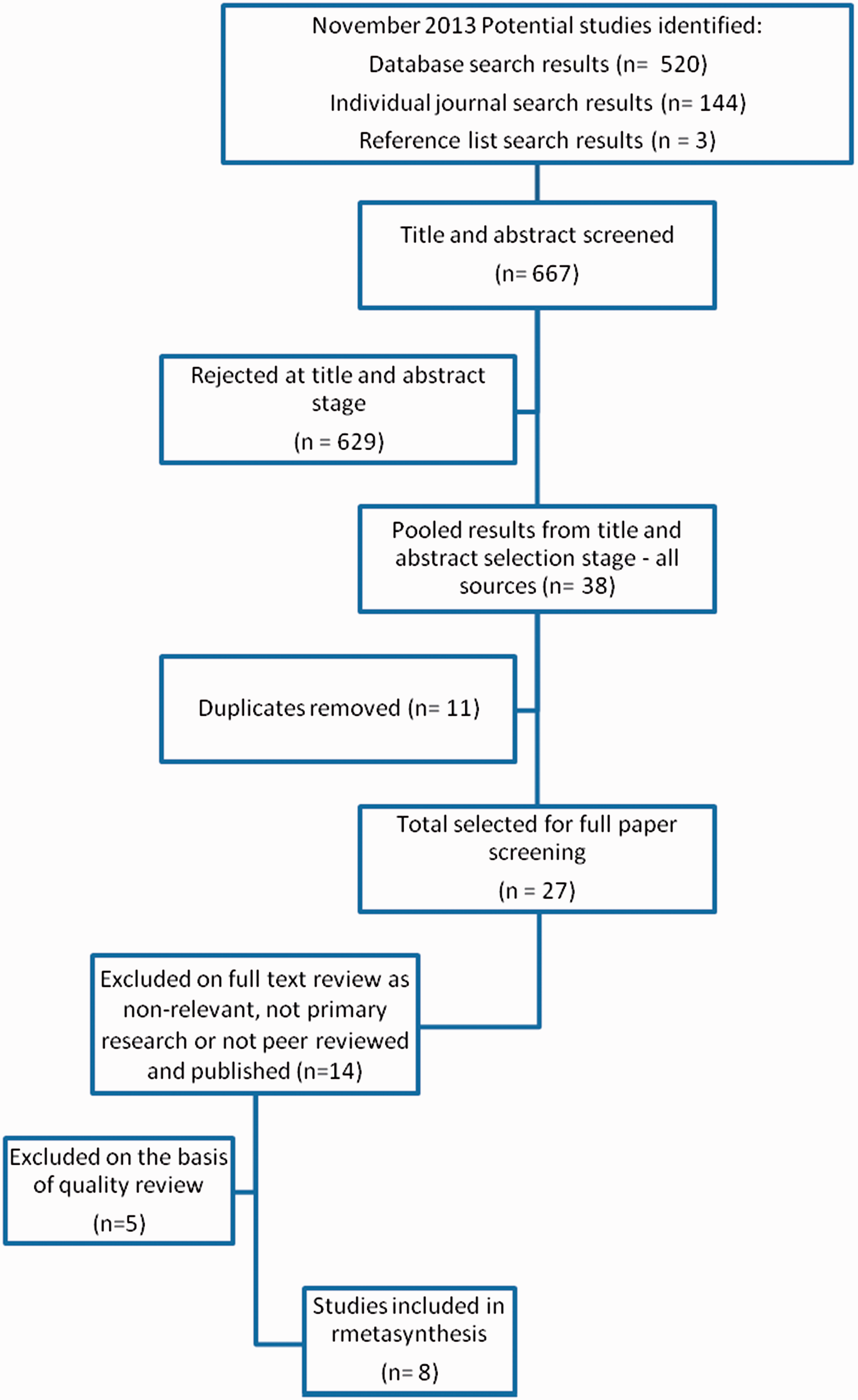
A total of 667 papers were identified. On title and abstract review, 629 papers were excluded on the basis that they did not fit the inclusion criteria for the review. After removing duplicates, the remaining 27 papers were selected for full text review. Fourteen of these papers were further excluded on full reading as they were found not to be primary research or did not relate to the purpose of the systematic review. The final 13 papers were then subjected to a rigorous quality assessment.
Quality assessment
An adapted format of the COREQ 32 item check list was used to facilitate the quality assessment of each of the selected papers. This tool was adapted by Lundgren, Begley, Gross, and Bondas (2012) to include 13 additional items (total 45 items), for example relating to ethical considerations, literature usage and relevance and transferability. The quality assessment of each study was conducted independently by two of the systematic review team who then met to agree each study's inclusion or exclusion. Where questions arose around suitability for inclusion (n = 2), the third member of the systematic review team reviewed the study and a consensus decision was then made.
Data extraction, analysis and synthesis
To ensure consistency, a standard purpose designed data extraction tool was used to extract relevant data from the findings sections of each of the included studies. Firstly each study was read by a member of the systematic review team a number of times to facilitate immersion and to enable the identification of pertinent research findings with which to inform the meta-synthesis. This process enables reviewers to become more cognisant of the participants' worlds and facilitates understanding from their perspectives (Betany-Saltikov, 2012).
Secondly, the extracted data for each included paper was then subjected to content analysis using open coding during which key concepts or interpretive metaphors relevant to the research phenomenon were identified and linked to related text (Booth et al., 2012; Campbell et al., 2003). Once this process was complete, a search for the presence or absence of these concepts or interpretive metaphors was conducted across all eight studies using constant comparison (Tranfield, Denyer, & Smart, 2003). This resulted in an iterative process to synthesise the systematic review findings to produce an expanded holistic interpretation of the experience of spirituality from the perspective of the person with dementia.
Findings
Overview of included studies
Characteristics of included studies.

From the eight studies included, one overarching theme and three sub-themes were identified as constituting the experience of spirituality from the perspective of the person with dementia (Figure 2). All of the themes were found to inter-relate with the others as components of the overall experience. The findings of the meta-synthesis will now be discussed with reference to these themes.
Illustration of themes and sub-themes.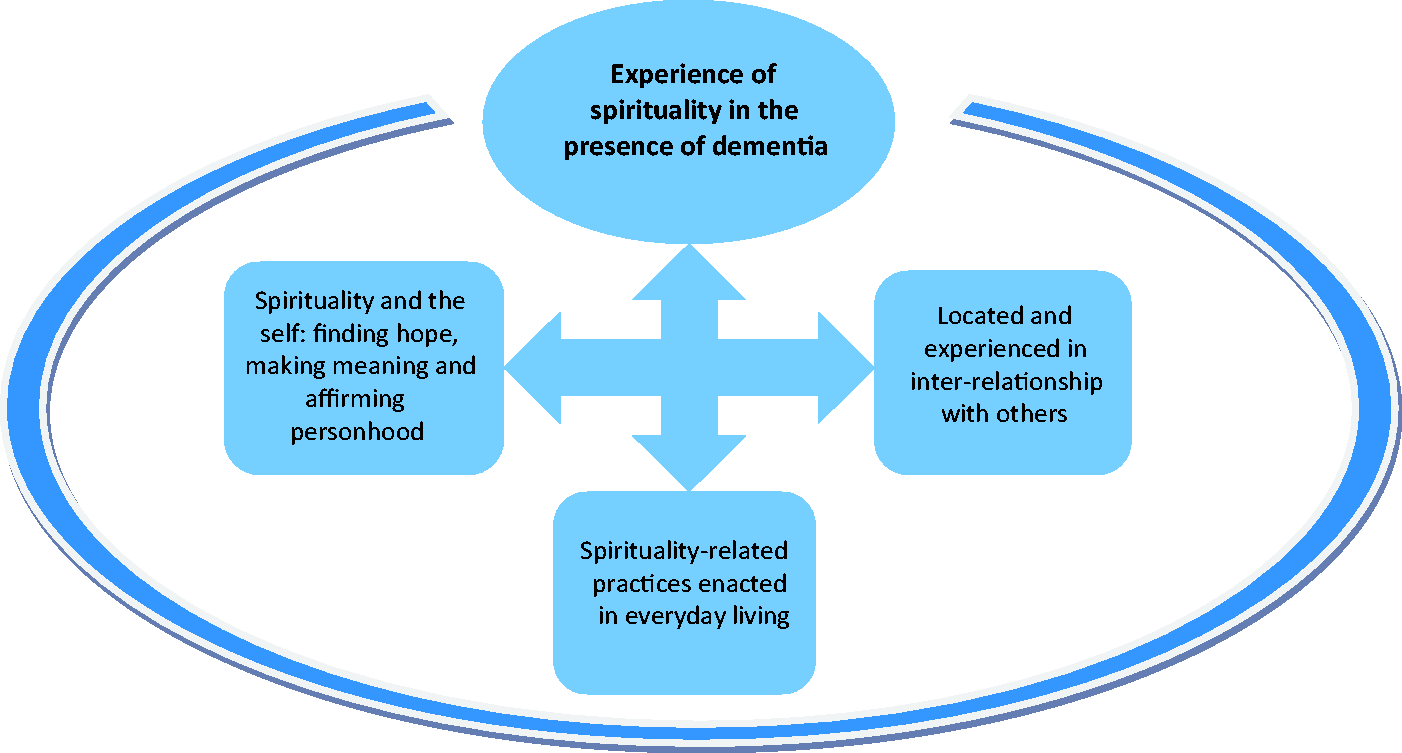
Overarching theme: The experience of spirituality in the presence of dementia
This theme conceptualises the point at which spirituality-related experiences of dementia come together to create an overarching and encompassing sense of spirituality in the lives of people with dementia. Although spirituality as a concept was not explicitly presented in terms of a definition by participants, the importance of spirituality, its nature and its essence in terms of personal meaning to the person, were referred to by participants in all studies (studies 1–8 as listed in Table 3). Data suggested that a sense of the self, and expressions thereof, were indistinguishable from a person's spirituality and findings in some studies (studies 2, 3, 8) suggested that a sense of the spiritual may be heightened in the presence of dementia: … their [people with dementia] experience of spirituality seemed to be woven into the fabric of their life, part of them, and therefore dependable and sure. (study 7, p. 82, lines 11–12) This man later explained that the experience of having AD gave him a heightened spiritual sense. ‘My religion has always been a part of me, and it gets stronger and stronger. It has gotten more intense’. (study 3, p. 59, lines 5–8) …God is there to be a companion through the challenges presented to us in life. (study 2, p. 301 or 2, lines 1–5) The Lord is with me and beside me all the time. (study 8, p. 234, lines 34–35) All the participants described an experience of faith that was a living and active part of their lives. This seemed to contribute to their sense of themselves as a person. (study 7, pp. 81–82, lines 3–4) Christ is my crutch. He is there to lift me up and walk with me. That is a very strong comfort to me. (study 3, p. 590, lines 10–11)
Sub-theme 1: Spirituality and the self – Finding hope, making meaning and affirming personhood
This sub-theme incorporates two subcomponents both of which support the affirmation of the personhood of the person living with dementia. The first of these subcomponents relates to the supportive role and function of spirituality in relation to the provision of hope. Persons with life-limiting illnesses such as dementia need to have hope and to be supported through difficult times. The findings demonstrated that spirituality and its forms of expression are drawn on by people with dementia as active coping mechanisms to this end, particularly by those for whom spirituality was an ongoing part of their life-course (studies 1, 2, 3, 7, 8). Findings suggested that connection with personal spirituality may enable the person living with dementia to foster hope (studies 2, 4, 7), particularly early on in the trajectory of the condition, that in turn may contribute to the preservation of identity. For example whereas dementia is frequently conceptualised as a threat to self and personhood, here in counterbalance spirituality was referred to in terms of the following: that one's religion or spirituality provided solace by inspiring feelings of hope, strength, security, or guidance. (study 2, p. 304, lines 9–11) Furthermore, prayer was comforting and gave hope to these participants. For example one woman shared, ‘I pray every night and I always feel better after I do that. It gives me hope’. (study 3, p. 590, lines 20–23) Trust in God. Some Participants showed their deep trust in God and stated that they put their life in God's hands. Their attitude toward life is to accept what God gives to them, including both the good and the bad in life and not to worry about what they cannot change. (study 1, p. 325, lines 12–15) I figure if the Lord wanted me to have it, that's what's gonna happen. I just don't worry about it. (study 3, p. 590, lines 3–4) It [spirituality] guides a person's view of the world and self, providing structure, purpose, and meaning to everyday activities. (study 3, p. 589, lines 12–13) All the participants described an experience of faith that was a living and active part of their lives. This seemed to contribute to their sense of themselves as a person. (study 7, p. 81, lines 2–4) I’ve come to the conclusion that everything has a purpose; the Good Lord knows the best for you. Maybe this was to slow me down to enjoy life and to enjoy my family and to enjoy what's out there. And right now, I can say that I’m a better person for it. (Stuckey et al., 2002, p. 203) (study 2, p. 302, lines 14–20) …Two people communicated the way in which their faith had been consistent through the spiritual activity of their lives, and that it continued into the present. (study 7, p. 81, lines 8–10) Some individuals may find a new or renewed interest in seeking out a faith or practice to help them along in this challenging journey …. Six respondents spoke of ways in which Alzheimer's had influenced their spiritual behaviour or actions. For one Jewish man, this meant a reawakening of his interest in spiritual matters. (study 2, p. 309, lines 12–20)
Sub-theme: Spirituality located and experienced in inter-relationships with others
The experience of spirituality in dementia was found to relate to the way in which it was enmeshed within relationships with others (studies 1–8). Two forms of such relationships were evident, that with a transcendental being (reported in the overarching theme previously) and that with other people (explored here). As such, spirituality while having an intra-personal dimension was equally shown to be socially constructed within the spaces and places between and among others: I'm a spiritual person who lives it and reflects in what you do … [Spiritual care is] to help everybody I can … and teach and talk to and love (Larry person with dementia). (study 5, p. 405, lines 11–13) All of the participants spoke of ways in which their connections with others helped them to express their spirituality or to feel connected spiritually. (study 7, p. 89, lines 40–41) Eight participants continue to serve in a church role such as deacon, choir member of usher … These activities fulfill their needs to be useful and give them a sense of accomplishment …. ‘When [people at church] they got questions, they call on me for support’. (study 3, p. 591, lines 24–27) … Alma seemed to be communicating a sense in which she felt less of a person in the social world. (study 7, p. 83–84, line 42.1) As my journey into Alzheimer's progresses, my walk with the Lord grows more precious. I am frightened that the day will come when I no longer will be able to think of God's everlasting promises. Then I will have to rely on my dear friends in Christ to keep me close to our Lord …. (study 2, p. 308, lines 30–38) My daughter is my salvation … She is my strength …. I know the Lord is involved, and I think he sent her here. She moved there to be with me. That is sacred. (study 8, p. 235, lines 33–38)
Sub-theme: Spirituality-related practices enacted in everyday living
The final sub-theme illuminates the way in which the embodied experience of spirituality for persons with dementia was referred to in terms of being enacted in the context of everyday living. While related to, this differs to spirituality being experienced in inter-relation with others as it relates to personal spirituality practices and beliefs that generally continued to be integrated into daily life (studies 1–8): All the participants described an experience of faith that was a living and active part of their lives. (study 7, p. 81, lines 2) Reading, reciting, or hearing certain Bible verses was reassuring and comforting for all participants. (study 3, p. 590, lines 27–28 and p. 591, lines 1–3) To the extent that singing religious hymns was related to the practice of worship, several participants reported private and corporate involvement in this activity. One narrative reflected the meaningfulness of this practice for dealing with memory loss. (study 8, p. 240, lines 17–20) For some individuals, the idea of being spiritual but not religious is a matter of finding personal fulfilment in aspects of human life with which they connect at an intangible, emotional level that is both satisfying and meaningful. The worlds of art and music, the wonders of nature, holiday celebrations and the bonds of social relationships are examples of other expressions of spirituality that eclectically draw meaning – such as peace, wonder, joy, or love – from many different sources. (study 6, p. 68, lines 42–43 and p. 68, lines 1–5). Observations of the participants' homes revealed symbols of their relationships or religious artifacts such as crucifixes, crosses, angels, framed pictures with Bible Scriptures, and church hymnals. (study 3, p. 590, lines 12–14) Well, I don't get to go to church, I don't. I'd have to ask them [children] to take me to church …. I miss that … . (study 1, p. 327, lines 26–28) A Catholic man found that his religious practice was being dramatically altered by the effects of Alzheimer's disease. He wrote: I no longer remember prayers I once recited automatically. The prayers frequently get mixed up with each other …. As for the sacrament of penance or confession it too requires memory. (study 2, p. 307, lines 33–40) Persons with early-stage dementia experience cognitive changes that limit their independent religious activities. Therefore, their religious practice becomes more private than public. A personal relationship with God, mostly through prayer, seems to be very important to them. (study 1, p. 326, lines 13–16)
Discussion
Good dementia care embraces a respect for the person's ‘life story’. Such an approach to care takes cognisance of the life history of the person and how s/he has lived life up until now (Caspari et al., 2014). Furthermore, it facilitates meaningful engagement between carers and the person living with dementia (Caspari et al., 2014). It is important while caring for people with dementia and getting to know the person, their family and the emerging life story, that a sense of the person's underlying spiritual and religious beliefs are determined (Caspari et al., 2014). It is often perceived, due to the secular nature of society, that people are less religious or spiritual now than in previous generations (Paley, 2008). Indeed some carers may have discomfort with addressing this element of people's lives, and it is often a low priority in care settings (Powers & Watson, 2011). However, the spiritual is widely accepted as another component of the holistic person. It is also understood that spirituality and religion may become more important for people as they age (Atchley, 2003), and that contemplation of life's meaning and purpose is increasingly common during the aging process and towards the end of life (MacKinlay, 2012).
One important element emerging from this study is the coming together of what is known about the phenomenon which results in new understanding of the experience of spirituality for those with dementia. For many, spirituality took on a personal meaning that was closely intertwined with their sense of the self. Indeed there was evidence that spiritual behaviours and spiritual needs may be heightened in the presence of dementia. It is important, however, when seeking to address these needs in practice, that this is done on an individual needs led basis and not based on assumptions (McSherry, 2006). Personal needs vary, and for some clients, spiritual and religious beliefs may not be important (Molzahn et al., 2012), therefore a blanket approach to providing spiritual support to groups of people should be avoided. Those with dementia are particularly vulnerable as they may not be able to express their preferences in advanced dementia, so close liaison with family members (Powers & Watson, 2011), and careful recording of life histories will make their needs more accessible. At the same time, it must not be assumed simply because there is cognitive decline that there are no spiritual and religious needs present (Powers & Watson, 2011).
Religion, religiosity, transcendence or a connection/relationship with a transcendental being or God were sources of strength emerging from this review. Related beliefs assisted people to accept their diagnosis and live more easily with dementia. Religious rituals have been identified as comforting for people (MacKinlay, 2012; Timmins, Kelly, Threadgold, O'Sullivan, & Flanagan, 2015) and staff have noted that saying of prayers, singing hymns and use of quiet sacred space can reduce distress in those living with dementia (Ødbehr, Kvigne, Hauge, & Danbolt, 2014). Again linked care approaches need to be individualised, but staff ought not to be discouraged from supporting clients' particular religious needs where appropriate. Professional carers may lack knowledge and awareness in this regard, and therefore, it is important to use available resources to assist with this. The Royal College of Nursing (RCN, 2015), for example provides a useful resource and a guide to assessing clients' spiritual needs in practice (RCN, 2011). Chaplaincy services are also very useful support services as they are specifically prepared to directly assess and address clients' spiritual needs (Fitchett & Nolan, 2015). Within the literature it is recognised that the spiritual care of a person with dementia can be overlooked particularly when the person can no longer ask for such support. It is important therefore to raise awareness of the continuation of spiritual needs despite cognitive decline, and the potential benefit of addressing those needs. It is also important to remember the importance of religious rituals at the end of life, particularly as dementia is a life limiting condition (Peacock, Duggleby, & Koop, 2014). This is furthermore important as the facilitation of spiritual and/or religious rituals around death can also be incredibly supportive for families (Newell & Carey, 2008; Nuzum, Meaney, & O'Donoghue, 2014).
The finding that spirituality is enmeshed in inter-relationships with others is consistent with the work of Nagai-Jacobsen and Burkhardt (1989) who identified one of the characteristics of spirituality as a sense of harmonius interconnection with others as well as self and an ultimate other. These writers also understand spirituality as a factor which serves to integrate the human person, and that the experience of spirituality for the person living with dementia contributes to the upholding of personhood. Of particular importance in this review was the finding that a person's engagement with their own spirituality was further shown to enable confirmation of oneself and a recognition and confirmation of the person by others, and a means to aim for, if not attain, transcendence. Seeking to assess clients spiritual needs and providing support for these (RCN, 2011, 2015), including sacred space (MacKinlay, 2012), may enable people living with dementia to maintain and develop their relationship with the transcendent. Supporting and nurturing relationships with family is also important, as is the acknowledgment, within the understanding of the person's life story, of the importance of these people in their lives. Wheeler's (2010, p. 19) interviews with 36 staff caring for older people with dementia for example found that nurses felt that it was important to engage with clients completing their tasks and nursing care. It was helpful if this involved ‘reminiscence’ and ‘involving family and keeping family on board’. These actions built relationships and opened communication. Engagement and building of relationships between both client and family and client and staff are also essential components of person-centred (Brooker & Latham, 2015) and relationship-centred (Brown-Wilson, 2013) care. It is observed that clients may become dehumanised and objectified in healthcare settings, whereby tasks are the main focus rather than the person (Clarke, 2013). Seeking to engage with the spiritual, that is what the client finds meaningful in life, serves to restore personhood (Clarke, 2013), and certainly from this review, and as advocated by Duggleby et al. (2012), helps renew a sense of hope.
People with dementia considered their spirituality as part of their everyday living. This finding demonstrates the value and importance of spiritual practices and beliefs in the daily life of those living with the condition and supports the growing concern about the need to address clients' spiritual needs (Cullen, 2016). Only by understanding what gives life meaning, and what those individual spiritual needs are, can effective support be provided to each person (RCN, 2015). At the same time, it is important to remember that spiritual support needs to be individualized. As such assumptions must not be made that all people living with dementia will require spiritual support. Rather this will be dependent on their life story and particular preferences, much of which can be determined from an accurate life history assessment and from speaking with friends and family. However at the same time, the review findings certainly indicate that this is an important facet of life for many living with dementia. Facilities that are often incorporated into nursing home and other such care settings, such as sacred space, religious rituals and chaplaincy support (MacKinlay, 2012), ought to be encouraged and developed to support the needs of the community. Where clients are not from the majority religious faith, and have expressed religious needs, referrals may be made by the staff or chaplains to community religious groups (Health Service Executive, 2011; Swift, 2015) so that clients may receive support in this way. In the studies reviewed, many participants felt disappointed that their advancing dementia was experienced in a way that meant that they were challenged to, or could no longer, participate in local community religious occasions and events. For these people, the findings suggest that establishing a parallel situation in residential care, could be very important in re-establishing meaning and connection, and providing support and hope with a challenging diagnosis and the related impacts on a person's life journey. Overall, it is important to: … acknowledge the spiritual dimension of a person and support spiritual expression and growth. Spirituality no longer merely denotes religious affiliation, it synthesizes a persons's contemplative experience. Illness, a life crisis, or even the recognition that our days on earth are limited may cause a person to contemplate [their] spirituality. (Meiner, 2010, p. 25)
Limitations
Only studies written in the English language were included in this review due to a lack of access to translation services. In addition, the writers while attempting to capture all related literature acknowledge the difficulty in ensuring an exhaustive literature search when conducting, a meta-synthesis – e.g. variety of research approaches and the underlying focus of the primary research itself. Therefore, the possibility exists that other relevant studies and studies in languages other than English may exist.
Conclusion
This meta-systhesis explored the experiences of spirituality from the perspective of the person living with dementia that have been reported in peer reviewed published literature. Our intent was to create a synthesised interpretation from the existing evidence base so as to advance understanding of the phenomenon. Overall the studies included indicated that people with dementia experience a deep understanding of spirituality, often enhanced by their re-remembrance of early life experiences. Faith, belief and rituals over the life-course were shown to sustain the person through the challenges they encounter in living with dementia. The potential benefits of faith rituals have been identified in other studies (Timmins et al., 2015). Embracing spirituality, which is unique to each person, creates the potential for individuals, adapting to and living with the life changing events that accompany a diagnosis of dementia. As such, spirituality was shown as a means, to cope with and ascribe meaning to these events. Spirituality may be also be experienced through connection with others, and the importance placed on this, whether it be family or faith community, serves to energise at least some people with dementia who reported that living with their diagnosis was made easier by having a belief and faith. Increasingly, in this secular age it is common to overlook the potential spiritual needs of clients receiving healthcare (Radford, 2008). The findings of this systematic review affirm the importance of not neglecting the importance of spirituality and spiritual needs of those living with dementia. They further confirm the need for spiritual competence for health and social care practitioners involved in dementia care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.