
Abstract
Alzheimer’s is a syndrome mainly suffered by women and the care they need is also mainly provided by other women. The aim of this paper is to describe the profile of users of professional support services and to find out if some socio-demographic factors are linked with those elections. The study was conducted from January to June 2012 thanks to the cooperation of over 41 Alzheimer’s Associations in Andalusia, in the south of Spain. A person trained by the main researcher (a social worker or a psychologist) completed the questionnaire during an interview with the caregiver. Seven hundred and seventy-eight questionnaires were analysed. Contrary to previous findings, the use of external services is not infrequent. The most commonly used services are Day Care Centres (22.4%) and Cognitive Workshops (19.2%), but Home Assistance Services are the most frequently used either alone or in combination with the other two (27.5%). A higher level of education increases the probability of choosing a nursing home. The two main factors for looking for external support are non-cohabitation and working outside the home. Among caregivers under 40 years old this is the main profile. Using no services or in low and medium intensity in service hours leads to informal caregivers being the main caregivers. The potential labour market for professional caring is reduced by a crowding-out effect. Employment reduces the chance of being a caregiver.
Introduction
Taking care of a dependent person who suffers from Alzheimer’s Disease and Related Disorders (ADRD) is a long-term activity that usually falls on close kin, and mainly on women. Even when the caring activity is provided by professional carers, women mainly dominate the network of caregivers (Toribio-Díaz, Medrano-Martínez, Moltó-Jordá, & Beltrán-Blasco, 2013).
Women have traditionally assumed the role of care providers over different generations in all cultures. They take care of children as mothers, they take care of grandparents when they get old and in many situations, they do it once again with their grandchildren whilst their own children are working. This provision of in-kind services is an important form of economic transfer to the society.
The structure of the family is shrinking and the role of women, especially younger women, is moving towards a more active position in the labour market. This social change has also been more evident with an increased participation of middle-aged women in professional occupations (Casado-Marín, 2006). Nonetheless, the family is still the main agent of care, and the intermediary between the health and social system (H&SS) and the person who needs care (Rubio & Solórzano, 2004), but it is evident that the increasing labour market participation by women will subsequently lead to a less prominent participation of women as the main caregiver in the future (Bauer & Stroka, 2013; Degiuli, 2010).
It is well known (Hussein & Oğlak, 2014; Pohl, 2011) that the population is aging and with this phenomenon the need for long time care (LTC) will grow. This situation adds stress to the H&SS. Holdenrieder (2006) stated for the case of the European Union (EU) that a combination of demographic, social and macroeconomic developments have put EU LTC schemes under severe pressure. The demand of services for LTC for people with ADRD is increasing but the economic crisis that the whole world has suffered has led to a review of the sustainability of the welfare state. Supply from public and private agents will have to cover the increasing demand.
However, despite the above, some papers have shown that there is a low use of H&SS for patients with ADRD even though considerable proportions of caregivers report low levels of life satisfaction and high levels of being overloaded and resentment (Brodaty, Thomson, Thompson, & Fine, 2005; Scalmana et al., 2013). Caregivers of people with ADRD often delay the use of community resources until late into the disease process (Robinson, 2005). In a recent study conducted by Michalowsky et al. (2015), with the German population, they found that formal care services were utilised less (26.3%) than informal care (85.1%).
Being a caregiver has consequences for the people who play that role. When the caregiver is limited in their own social life, they may fail to receive appropriate emotional support and contact from others (Wimo, Winblad, & Grafstrom, 1999). The impact on caregivers in terms of physical and emotional burden (Akpınar, Küçükgüçlü, & Yener, 2011), financial and employment status may be enormous, especially when the patient is still working (Luscombe, Brodaty, & Freeth, 1998; Vogel, Ludwig, & Börsch-Supan, 2012), or when the caregivers are younger and adapt their life to provide care. Many have to quit work, reduce working hours, or take time off because of caregiving (Cox & Pardasani, 2013). Van Vliet, de Vugt, Bakker, Koopmans, and Verhey (2010) conducted a review of seventeen articles to show what the consequences are, particularly in the cases of early onset of ADRD. However, when they compared caregivers of early onset cases as opposed to late onset, the differences were not so relevant, with the obvious exception of those related to the loss of their active roles in society.
All these disrupting consequences in the caregivers lives, and especially if we consider that most of them are women, may lead to conclude that the demand for support services should have experienced an increase in the last decades, but a review of the published papers does not support that idea. Some previous papers have shown that, for women in particular, starting to provide care means reducing their hours of paid employment (Johnson & Lo Sasso, 2006). A recent paper in Spain, Ruiz-Adame, Gonzalez-Camacho, and Mainar (2015), demonstrated that those who care for dementia patients have greater limitations accessing the labour market than the rest of the population. Moreover, those effects seem to continue over time. Moscarola (2010) in a study done in the Netherlands concluded that previous informal care provision slightly reduces the probability of the caregiver working after they stop providing care and vice versa between women.
Using an external service, such a day care service, could be useful to maintain a certain physical and psychological balance (Gaugler, Zarit, Townsend, Parris Stephens, & Greene, 2003). Furthermore, caregivers consider working as to be valuable and desired form of respite (Utz, Lund, Caserta, & Wright, 2012); however, most of the LTC for ADRD is provided at home.
The empirical study has been performed in Andalusia, the region that occupies the south of Spain. It is a geographical area of 87,268 km2, an area higher than many European countries such as Austria, Holland, The Czech Republic, Ireland or Denmark. With a similar extension to Portugal or Hungary. Andalusia has a population of 8,381,213 people, which is higher than the population of Finland, Norway or Ireland. Its population is similar to that of Switzerland or Austria. The general characteristics of this population are very similar to the general profile of the Spanish, and with all the Mediterranean cultures, where the family is the core of care provision in LTC.
The Spanish population still has a very traditional structure among the middle-aged people, and this is the most common profile of caregivers. As we have stated, despite the consequences that being a caregiver involves it seems that there is still a way to go. In this sense, and particularly in the Spanish population, as far as we know, there is a lack of knowledge that we aim to bridge with this study. It is necessary to know how the external service demand between caregivers is and how the caregiver’s profiles affect that demand.
In order to prove the contribution to the literature of our research we have done a review of the published papers in the two main databases, Medline and Scopus, with the following keywords: long-term care, labour market, employment, unemployment, Alzheimer, dementia, use of services. We used booleans operators to combine these keywords and limit the search only to journal articles or reviews within the last five years. If there were less than 20 results, we widened the search to the last 10 years or we even removed the time limitation. We only selected papers in English or in Spanish about the western population of Europe, Australia or America (see supplementary tables A and B).
The aim of this paper is to describe which factors define the demand for the main external services among caregivers of people with ADRD in the south of Spain (Andalusia) and to discover if there is a link between their socio-demographic characteristics and this demand.
After the review, to the best of our knowledge, this is the principal research with empirical data on this issue with the Spanish population. Very few papers were found (only four) when searching these criteria with Spanish population. Some of them are obsolete due to the time they were conducted and sample they used (Casado-Marín, García-Gómez, & López-Nicolás, 2010; Rubio & Solórzano, 2004). And others are performed with a clearly lower sample and in a reduced area (Olazarán Rodríguez, Sastre Paz, & Martín Sánchez, 2012; Toribio-Díaz et al., 2013). In any case, none of these four papers addressed the topic of the aim of our research. Consequently, our paper fills a gap in knowledge with this population.
Methods
The data collection for this study was performed from January to June 2012 thanks to the cooperation of over forty one Alzheimer’s Associations in Andalusia, in the south of Spain. The sampling procedure was selective non-probabilistic sampling.
The draft was submitted to the associations who ethically gave consent to it. After the approval of the board of directors, the associations informed their members and we contacted and interviewed those caregivers who had previously indicated that they would be willing to participate. The participation was entirely voluntary, and caregivers were given the option to withdraw consent at any time.
A person trained by the main researcher (a social worker or a psychologist) completed the questionnaire during a face-to-face interview with the caregiver. Interviews took fifteen–twenty minutes to complete and were conducted at the Alzheimer’s Associations. The main researcher performed a monthly follow-up of the instructions and results with the interviewers.
The people who analysed the data were blind to the origin of it. Incomplete questionnaires and those that had errors were discarded from the analysis. Of the total number of questionnaires some were incomplete for different reasons such as a refusal of the caregiver to continue (“caregivers were given the option to withdraw consent at any time”) or the interview was interrupted and could not be rescheduled, or even because some data about the expenditure of the caregivers or dedication in time that was unclear or unreliable. In those cases researchers opted to discard these questionnaires. Seven hundred and seventy-eight questionnaires were analysed.
In order to obtain a wide and representative sample of informal caregivers, the only requirement for participation was that the caregiver be active at the moment of the interview (a criterion of exclusion was the death of the patient prior to the recruitment of the caregiver). Consequently, nobody was dropped from the study due to their socio-demographic characteristics, experience as a caregiver, or the stage of the syndrome of the patient.
This study is part of a larger one about caregiver’s profiles and the societal cost of providing care. In this paper, we centre on the elections of external services and the consequences of them for caregivers and society. We only focus on those services that reduce the implication of taking care of the caregiver, such as Home Assistance, Cognitive Workshops, Day Care Centres and Nursing Homes.
In this study, Home Assistance is a service characterised by the support at home by a nursing assistant for a period of hours usually dedicated to help in activities of daily living. The amount of hours can vary widely from a few hours per week to a 24-hour/day period. Home Assistance service can be used in combination with Cognitive Workshops or with Day Care Centres. Cognitive Workshops are services focused on cognitive training. These services can include a transportation service or not, and the amount of hours of service can also vary largely depending on the level of severity of the patient. These services are especially designed for people between mild-to-moderate stages, but they can also assist mild-severe stages too. Day Care Centres are similar to the Cognitive Workshops but in this case the period of attention is greater. Patients usually eat at the centre and the level of severity of the people who go to these centres is mild to severe. They can also include transportation services. Nursing Homes are the most time intensive services. Users of Nursing Homes usually live there for 24 hours/day, sometimes it is the election when one member of the couple has ADRD and they opt to live there to ensure appropriate assistance for their partner. They received all kind of services depending on the stage of dementia, but in most cases people with ADRD who opt for these services are in the more severe stages of the syndrome. The variables are defined in Table 1.
Variable definition.

*: Medium studies: high school; **: High or superior studies: University degree
Results
We have done three consecutive statistical analyses. First, a descriptive analysis based on the frequency for the qualitative variables, and the means and standard deviations (SD) for the quantitative variables to describe the general profile. After that, we have applied two logistic models. Firstly, a binomial to find out which of the variables that we have studied have influenced the use or not of external support services. And secondly, we have performed a multinomial to identify the main differences regarding the preferences of the type of external support service. We chose the logistic models because they are suitable for the main objective of the research and allowed us to express the results in terms of probabilities.
A descriptive statistical analysis was done to find out the characteristics of the caregivers and patients. The general profile of a caregiver is that of a woman (76.6%) with a basic or lower level of education (55.9%), who is the daughter of the patient (60.8%), cohabits in the same household (70.3%) and does not work outside the home (66.5%). The patient is also a woman (71.3%), with a severity level mainly between 4 and 7 (mean: 5.43; SD: 1.32) at the Global Deterioration Scale (GDS) of Reisberg et al (1988). This profile is clearly different with the group of younger caregivers (see Tables 2 and 3), which we have defined as those with an age of 40 years old or under. The average age of this group is 34.8 (SD: 4.9). We have chosen this group to compare with the general group because at this average age (in the area where we have collected the data, Andalusia) the proportion of occupied people is higher and the unemployed people is at the lower rate. The profile results attractive to compare with the general of the sample (Ocupados por grupo de edad, sexo y comunidad autónoma. Valores absolutos. INE.; 2016).
Profile of users of different external support services in the general group (percentage for qualitative variables and mean and standard deviation for quantitative variables).
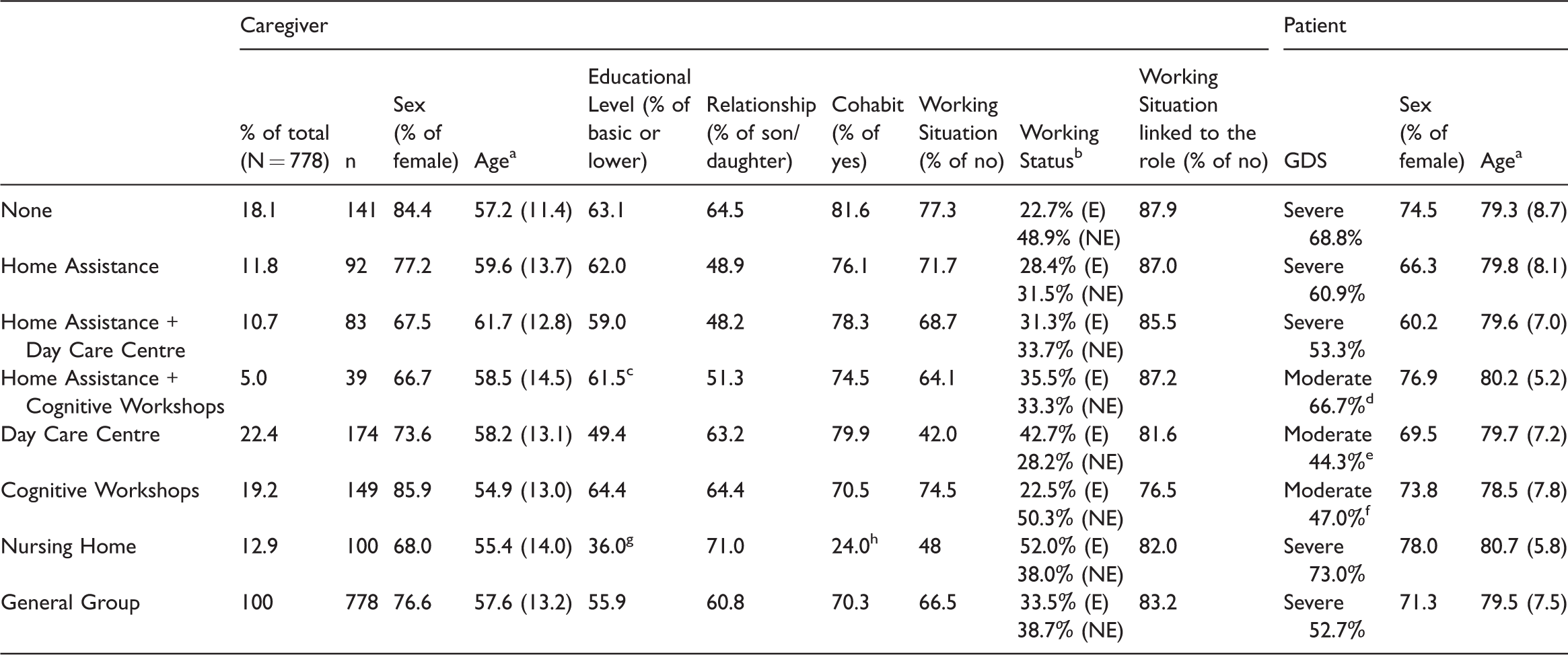
GDS: Global Deterioration Scale.
Mean and standard deviation.
E: Employed; NE: Not Employed (of the remainder 100% are the retired caregivers).
High: 23.1%; Medium: 15.4%.
Severe: 33.3%.
Severe: 43.7%
Severe: 34.2%.
High: 33.0%; Medium: 28.0%; Medium incomplete: 3%.
No: 76.0% (in the case of users of nursing home there are some couples that cohabit).
Profile of users of different external support services when a caregiver is 40 years or under (percentage for qualitative variables and mean and standard deviation for quantitative variables).
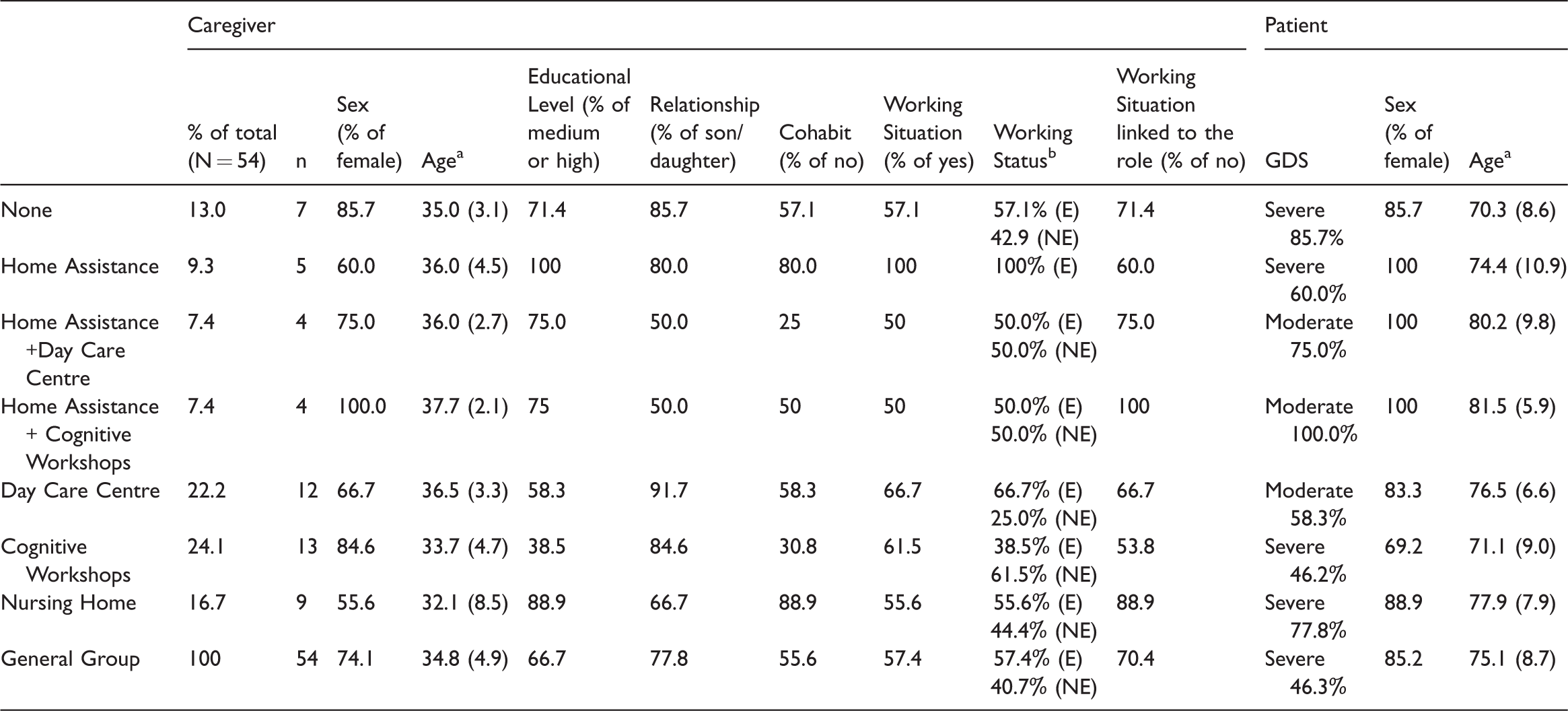
Mean and standard deviation.
E: Employed; NE: Not Employed (of the remainder 100% are the retired caregivers).
The most common external service is shown in Table 2. The mean time of received external services is: (a) for Home Assistant 70.81 hours/month (SD: 113.98). This enormous dispersion shows that there are great differences in the use of this service. Home Assistant is a service that can be received by the person alone, or it can be combined with others such as Day Care Centre or with Cognitive Workshops. (b) For Day Care Centre 176.0 hours/month (SD: 16.01), (c) for Cognitive Workshops 68.89 hours/month (SD: 64.87). In this case the dispersion is related to two factors: (1) Some people use transportation services, that increase in attention time and (2) because Cognitive Workshops are not as homogeneous as other services such as Day Care Centres. People in mild situation of the syndrome usually go to these workshops for just a few hours per week (2 or 3) but in moderate stages they can receive this service in a range between 9 and 25 hours per week. And (d) Nursing Homes are a 24-hour/day service.
In the general group, the most used services are the Day Care Centre (22.4%) and the Cognitive Workshops (19.2%), but the Home Assistance Service is the most commonly used either alone or in combination with the other two (27.5%). The profile of caregivers whose kin are users of Nursing Homes as shown in Tables 2 and 3 is different in Educational Level (higher), Cohabitation (no) and Working Situation (active in higher proportion). For the treatment of the data, the SPSS 23 program was used.
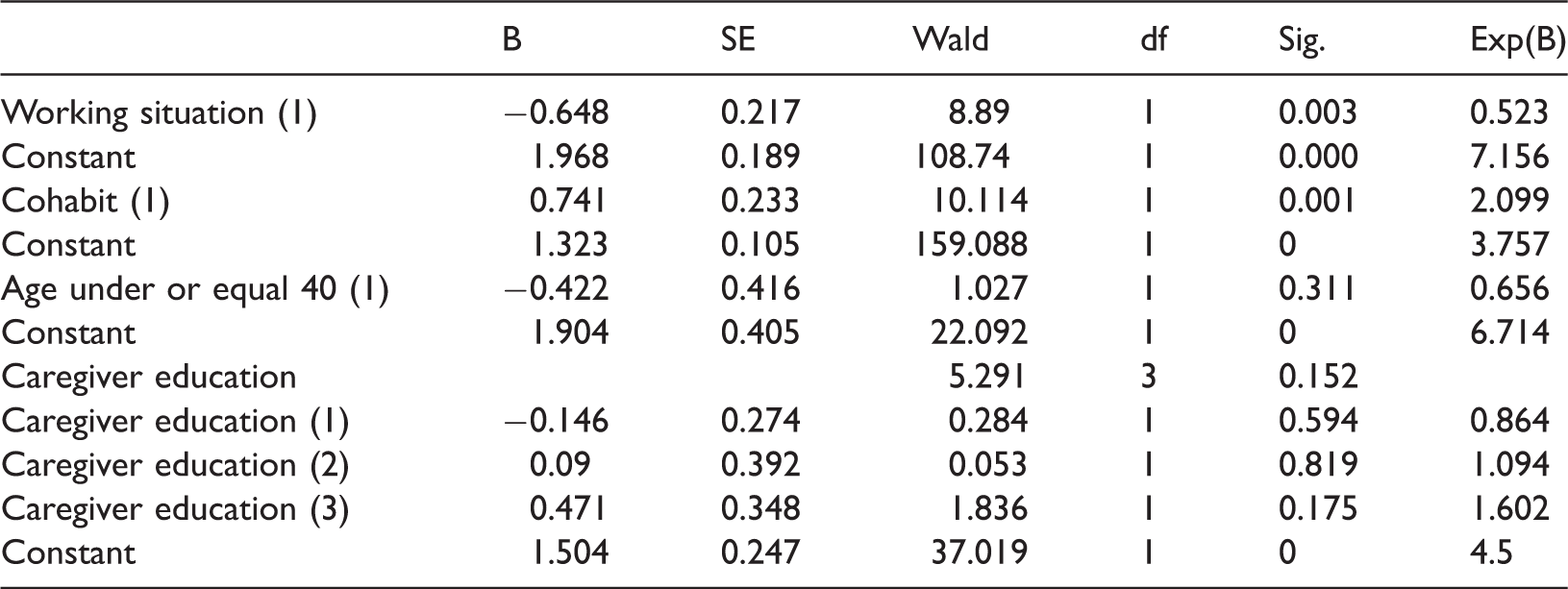
We analysed, using binomials logistics models, to determine if the Use (or not) of External Support Service (the dependent variable (DV)) can be predicted by the following variables: Working Situation (yes or no), Cohabitation of Caregiver and Patient in the same household (yes or no), Age of the Caregiver (under or equal to 40 years old or above) and Caregiver Educational Level (basic or less, medium incomplete, medium and high). See Table 4.
Variables of the equation for the different binomial models.
First of all, we proved the three underlying assumptions in the model: (1) Linearity, (2) The Independence of errors and (3) Non multi-colinearity. The model of logistic regression guarantees the first one. For the second one, we performed the Durbin–Watson test (1.537, between 1 and 3), which this complied with. And the inflate variance factor is under 10 in all cases. The third assumption, non-multi-colinearity, has also been complied with.
For the logistic regression models, the block 0 shows that there is an 81.9% probability of matching the results of the DV, the Use of External Support Services, if we assumed that all people used External Support Services.
For block 1, the statistical efficiency test of ROA shows that there is a significant improvement (P<.050) with the prediction of the probability of occurrence in the categories of the DV for the variables Working Situation (Chi2: 9.59; df: 1; Sig: .002) and Cohabitation (Chi2: 11.23; df: 1; Sig: .001). The values of the R2 of Nagelkerke are .020 and .023, respectively. For the other two variables, Age of the Caregiver, under or equal to 40 or above (Chi2: 1.126; df: 1; Sig: .289) and Caregiver Educational Level (Chi2: 5.73; df: 3; Sig: .125) there is no significant improvement on the predictions of occurrences in the categories of the DV.
As we see in Table 4, the two variables that are significant are if the caregiver cohabits with the patients and if the caregiver is working outside the home. When the caregivers do not cohabit and when they work outside the home, the probability of looking for external services increases. The Wald punctuations for the model show for these two independent variables improve on the prediction of the DV (P<.050).
In addition to the previous analysis, we have analysed what the main differences are with regard to preferences in the Type of External Support Service. These seem to have to do with the Educational Level of the Caregiver, about whether they Cohabit or not, and about if they Work Outside the Home or not (see Tables 2 and 3). A multinomial logistic regression model was performed. The category of the variable Type of External Support Service to compare was None External Service.
The significant results that we have found are that those who have incomplete (B: .954; Exp(B): 2.59; Sig: .045) and completed (B: 1.085; Exp(B): 2.96; Sig: .012) medium studies are more likely to choose a Day Care Centre than None External Service. Those who have basic or lower level of studies (B: .874; Exp(B): 2.39; Sig: .041) and those with completed medium studies (B: 1.288; Exp(B): 3.62; Sig: .009) are more likely to choose a Cognitive Workshop than None External Service. And those who have basic or lower level (B: −1.406; Exp(B): .245; Sig: .000) and incomplete medium studies (B: −1.967; Exp(B): .140; Sig: .005) are less likely to choose a Nursing Home than Non External Service.
The profile of caregivers of 40 years or less, as shown in Table 3, compared with the general group (Table 2) is clearly different. They are still women and the relationship is also of son/daughter in most cases, but the Level of Education is higher (only 22.2% have basic or lower, in the general group is 55.9%), they are in an active Working Situation (23.9% more employed people on average), and they do not Cohabit in the same household in many cases (29.7% do not cohabit in the general group meanwhile in this subgroup it is 55.6% on average). In spite of this, the statistical analysis with the logistic models does not show significant differences. We consider this is an effect of the size of the sample that should be improved in further studies.
Discussion
Most care is provided at home, and caregivers usually prefer when they choose external help to use a low or middle intensity in time service that enables patients to remain in the family household. It means that even when they use a support service they are still the main care providers. In Spain, it is very infrequent to live in Nursing Homes. Among those over 65 years old, 82.8% live in their own homes and even among those over 85 years old the figure remains high, 77.8% (http://www.ine.es/prensa/np965.pdf).
ADRD is a syndrome, mainly suffered by women and the care they need is also mainly provided by other women. The general profile of a caregiver is that of a traditional housewife. In fact, in the vast majority, they are people with a low level of education and who have never worked outside the home. This may explain why they generally consider that their working situation is not affected by the role of a caregiver. There are obviously other moral and cultural factors that must be kept in mind and that determine the taking on of the role. In this regard, some authors (Brodaty et al., 2005; Robinson, 2005; Scalmana et al., 2013) have found that the low use of services is due to caregivers’ perception that they do not need this kind of support, because they have an individual ability to deal with this stressful situations (Mockler, Riordan, & Murphy, 1998) or due to psychological reasons such as a depressed mood (Hancock, Reynolds, Woods, Thornicroft, & Orrell, 2003).
Contrary to previous findings (Brodaty et al., 2005), we have found that the use of external services is more common than we thought. Olazarán Rodríguez et al. (2012) found with a lower sample (N=75) of Spanish population than ours (N=778) that the service most used was Home Assistance and few caregivers used formal social or health services, meanwhile in our sample external services are used by 81.9% (see Tables 1 and 2). In the same sense, Robinson, Buckwalter, and Reed (2013) did similar research in the USA, and they have encountered differences in the profile of kin or age between user and non-user of support services. In our case, the profile is very homogeneous for all groups with the general profile. The exceptions are the people who have a high level of education (14.1%) or completed medium level (20.1%). In those cases, there is a preference for Nursing Homes (see Tables 1 and 2) and they do not cohabit. In the Spanish population, choosing a nursing home seems to be an election conditioned by working circumstances, meanwhile other studies have shown that in other countries it is due to factors such as caregiver’s health and troublesome behaviour (Cohen et al., 1993) or by financing mechanism that facilitates the use of these services (Bishop, 2004).
The support provided by informal caregivers is an economic transfer (Pezzin & Schone, 1999) that reduces the financial impact of attending to this illness (Philp et al., 1995) that is possibly due to the low level of employment between caregivers (Bauer & Stroka, 2013; Michalowsky et al., 2015). In fact, as we have proved, employment reduces the chances of being a caregiver (it increases the use of professional services). Our results agree with previous papers that have stated that women who started providing care reported fewer hours of paid employment (Johnson & Lo Sasso, 2006).
Using no services or low (Home Assistance) and middle (Day Care Centre and Cognitive Workshops) intensive in hours services lead to keeping informal caregivers as the main caregivers. The potential labour market for professional caring is reduced by this crowding-out effect.
As Martindale-Adams, Nichols, Zuber, Burns, and Graney (2015) stated that the caregiver service use is related to caregiver characteristics. Not cohabitating and working outside the home are the two main values that explain the increase of looking for external services. These two values are more present among the younger caregivers (see Tables 2 and 3). These caregivers have a higher level of education, they do not cohabit with the patient, in a higher proportion to the general group, and they are also working. As we have stated previously, in the data analysis, we have not found statistical significance between the comparison of this group and the general sample, but we consider that as a limitation of our study it should be considered in further research.
An increasing number of younger caregivers who work outside the home should reduce this current crowding-out effect in the future, and will probably increase the demand for intensive services such as Nursing Homes. This conclusion is in line with the report published by the WHO, in Global Health and Aging (Suzman & Beard, 2011), where they pointed out that people who live in developed countries seek jobs in cities or other areas, their older relatives back home will have less access to informal family care.
As can be seen in Tables 2 and 3, the general profile of the patients is that of people with moderate-to-severe symptoms in all types of services. We consider that this situation may reflect a tendency between caregivers to delay looking for external support services. Previous papers (Robinson et al., 2013) have underlined the same tendency.
Being a caregiver (Zhu et al., 2015) has physical (lower self-rated health, weakened immune system and increased cardiovascular problems), psychological (higher rates of depression, stress and other psychological problems) and economic consequences, which are sometimes hidden.
The need for personal support for people with dementia is lower in the mild stages, an early diagnosis reduces costs (Kirson et al., 2016; Panegyres, Berry, & Burchell, 2016). As we have seen in our research, people in mild stages need less care. In the first stages of the syndrome the patient is more independent and requires less support resources. It is cheaper to attend to patients at this time. New treatments that could slow down the evolution of the syndrome will also reduce costs and other side effects for caregivers too. Nevertheless, at this point, different stakeholders have different priorities (Bradley et al., 2015). In general, specialists and patients advocates support an early diagnosis. The earlier the intervention starts, the better the results of any treatment, including non-pharmacological, will be. But, on the other hand, the other concerned stakeholders, the payers, are sceptical. They would only promote early diagnosis if it were proved with a robust evidence base that it would lead to improve clinical outcomes. It is necessary to develop more scientific evidence of the clinical effect of early intervention, both pharmacological and non-pharmacological.
We have seen that the current general profile facilitates delaying a long-term institutionalisation (Eloniemi-Sulkava et al., 2009) but it is only possible due to the special circumstance that is changing and it should be bear in mid for policy makers. With the continuous incorporation of women into the labour market and the increase of the mobility of workers, the two main factors that determine the demand for external services should grow, and the demand for professional carers and services will also.
The strengths and limitations of this study are as follows: the main strength is the size and diversity of the sample, and the fact of having empirically studied the preferences of non-professional caregivers in a population such as the Spanish where no other similar study has been done. In general, the profile of caregivers in our research is similar to other previous papers. This allows us to generalize our conclusions, but the main limitation is the source of the sample. People who chose a nursing home as a support resource may be misrepresented in this sample because it is unusual to belong to an Alzheimer’s Associations among those people.
It would also be interesting to explore the profile of younger caregivers and younger patients with a wider sample. Younger caregivers have a clearly different profile with higher cultural level, and they are in the job market in a higher proportion. Younger patients can be in active working situations in greater proportion too, usually develop through all the phases of the syndrome in a shorter period of time, and consequently, their caregivers can have different preferences when they look for external support services that would be interesting to explore.
Footnotes
Ethical approval
Although no specific approval was required for this study, it was considered and approved previously by the direction committee of the associations who participated in the data collection.
Acknowledgements
The authors thank the Alzheimer’s Association of Andalucía, and especially the Santa Elena Alzheimer’s Association (Seville), and their technicians for their invaluable encouragement and effort towards this research. The authors also thank Prof Carmen González-Camacho for her help in the survey design, and Kate Burton for her help with the style and grammar.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Research Group SEJ-393: Public Economy and Globalization of the University of Granada for their support.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.