
Abstract
The experience of taking care of spouses with young-onset dementia has been identified as unique and merits considerations. However, current knowledge about this area in Chinese spousal caregivers is scarce. A qualitative descriptive study was therefore conducted to explore the experience of spousal caregivers of persons with young-onset dementia in Hong Kong. A total of six spousal caregivers of persons diagnosed with dementia before the age of 65 participated in this study. Three major categories were identified: coming to terms with an unexpected diagnosis; multiple unanticipated and ‘early’ losses and finding positives and meaning. This study has highlighted the influence of sociocultural values on the spousal caregiving experience in young-onset dementia caregiving. The findings also have significant implications for the development of interventions to facilitate the spousal caregivers to accept and sustain their caregiving role.
Introduction
A large number of studies have explored the experience of taking care of persons with late-onset dementia (LOD) (Gilhooly et al., 2016; Sun, 2014). However, much less is known about the experience of caregivers who are caring for persons with young-onset dementia (YOD).
Recently, the increasing number of people suffering from YOD has attracted more attention from researchers, clinicians and policy-makers. Numerous studies have illustrated that persons with YOD presented with more strange behaviours and emotional problems when compared with those with LOD (Smits et al., 2012; Werner, Stein-Shvachman, & Korczyn, 2009). This might be related to the higher prevalence of frontotemporal dementia among the YOD population (Smits et al., 2012; Werner et al., 2009). Studies have shown that the behavioural and emotional problems of persons with YOD have adversely affected the well-being of their caregivers (Spreadbury & Kipps, 2016, 2017; Svanberg, Spector, & Stott, 2011). In addition, misdiagnosis has been frequently reported in YOD because persons with YOD display a broad range of symptoms at the early stage but only with salient cognitive changes (Svanberg et al., 2011; van Vliet et al., 2013). This has contributed to the delay in diagnosis and treatment and subsequently led to an increase in the stress and burden in caregivers (Spreadbury & Kipps, 2016; van Vliet et al., 2013).
Apart from these, most people with YOD are in their 50s (Werner et al., 2009). These people are often working full-time, having dependent children at home and some are the ‘breadwinners’ of their family. The diagnosis of YOD has been suggested as devastating to both the persons with YOD and their families, especially their spouses (Cabote, Bramble, & McCann, 2015; Ducharme, Kergoat, Antoine, Pasquier, & Coulombe, 2013). The gradual loss of cognitive, judgemental and self-care ability of the persons with YOD has forced the spousal caregivers to take up multiple family roles and responsibilities. Furthermore, they are faced with possible loss of employment, financial problems and the lack of preparation to the caregiving role (Roach, Drummond, & Keady, 2016; Ducharme et al., 2013). Recent studies have demonstrated that the caregiving experiences and needs of these spousal caregivers are unique and required specific support (Cabote et al., 2015; Ducharme et al., 2013). Thus, various researchers have pointed out that there is a pressing need to explore more about YOD caregiving in order to develop interventions that can suit the needs of these spousal caregivers (Cabote et al., 2015; Svanberg et al., 2011).
In Hong Kong, people with dementia are encouraged to be taken care of in the community (Tong & Fong, 2014). Due to the influence of traditional Chinese culture which emphasizes on family values, majority of these people are taken care of by their family members (Tu, 1998). Furthermore, Chinese spouses are bounded to the marital philosophy which reinforces that couples have to take care of each other (Tu, 1998). Therefore, spouses have often been identified as the predominant caregivers of persons with dementia (Wang, Shyu, Wang, & Lu, 2017).
It has been illustrated that cultural values play an important role in affecting the caregivers’ perceptions on dementia and caregiving, which in turn affect their coping and adjustment to the caregiving role (Knight & Sayegh, 2009; Sun, 2014). Currently, knowledge about the experiences of caregivers of persons with YOD in Chinese population is scarce, especially from the perspectives of spouses. Studies about the experience of spousal caregivers of persons with YOD are mainly conducted in Western population (Cabote et al., 2015; Ducharme et al., 2013). Developing interventions based on findings from the Western population might not be applicable to the Chinese spousal caregivers. Thus, it is essential to gain more insights into the experience of Chinese spousal caregivers of persons with YOD in order to develop effective and cultural-specific interventions for them.
The aim of this study was therefore to explore the caregiving experience of spousal caregivers of persons with YOD in Hong Kong and provide recommendations for future practice.
Methods
A qualitative descriptive study was conducted in August to December 2016 to explore the caregiving experience of spousal caregivers of persons with YOD in Hong Kong. The qualitative descriptive approach was chosen because it facilitated data collection and data analysis in a naturalistic way (Sandelowski, 2000). This allowed researchers to explore and describe the phenomenon under studied by revealing the individuals’ true stories and with minimal interpretation of researchers (Sandelowski, 2000).
Setting and informants
Permission was obtained to conduct this study in one community centre in Hong Kong. This community centre provided services to persons with dementia and their caregivers, such as caregiver workshops and support groups.
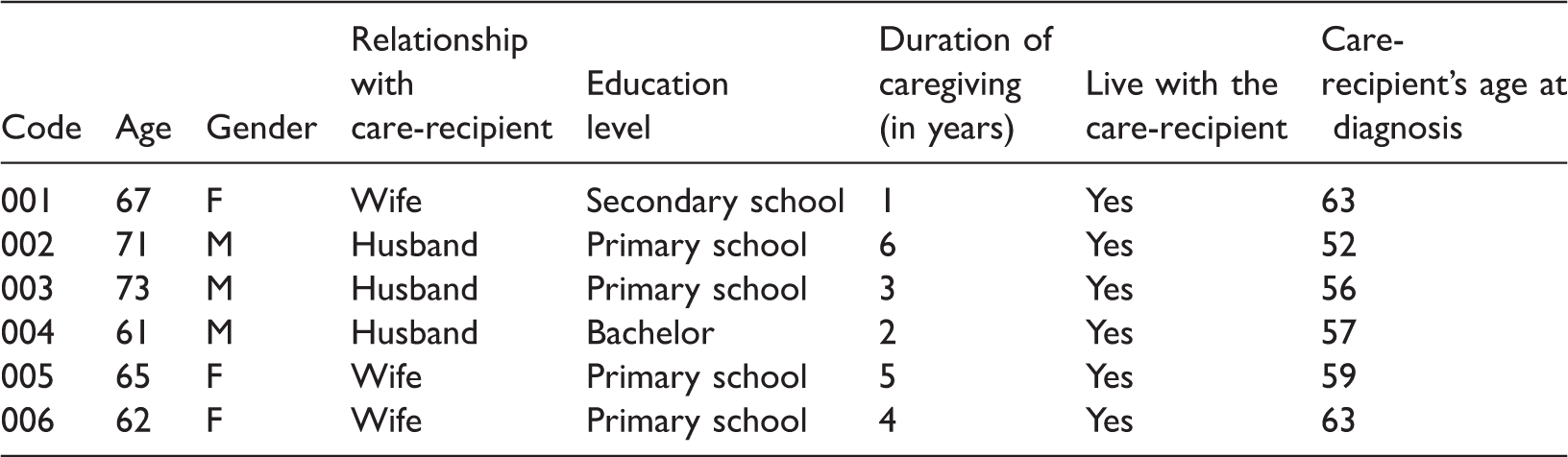
Purposive sampling was employed in this study to identify informants who had experience about the phenomenon under studied and were willing to share the experience (Speziale & Carpenter, 2011). Chinese spousal caregivers of persons diagnosed with dementia younger than 65, identified themselves as the primary caregiver and were responsible for providing most of the day-to-day care to the care-recipients were invited to participate in this study. A total of six informants were recruited. The characteristics of each informant are presented in Table 1.
Characteristics of informants.
Data collection
Prior to recruitment, ethical approval was obtained from the Survey and Behavioural Research Ethics Committee of the Chinese University of Hong Kong. The social worker of the community centre referred potential informants who were interested to participate in the study to the researcher. The researcher then contacted and met the potential participants. The purpose and format of the study with issues about confidentiality, voluntary participation and protection of human rights were explained to the participants. Written consents were obtained from the participants before data collection.
The experiences of taking care of the care-recipients were elicited through face-to-face, in-depth interviews. The interview guide consisted of open-ended questions to elicit rich data about their caregiving experience and the difficulties and satisfactions encountered during their caregiving journey. Questions such as ‘Could you share with me when and how you have taken up the caregiving role for (name of the care-recipient)?’, ‘Have you encountered any difficulties during the caregiving journey? How do you deal with them?’ and ‘Could you find any satisfactions during the caregiving journey? How do these satisfactions influence your caregiving experience?’ were asked to encourage a thorough sharing of the caregiving experience. All interviews were conducted by the same researcher at the private meeting room of the community centre. All interviews were audio taped and lasted between 55 and 128 minutes.
Data analysis
All transcripts were transcribed verbatim and analysed using qualitative content analysis (Graneheim & Lundman, 2004). First, the transcripts were read through several times in order to familiarize with the data. Then, the meaning units, that is, the text about the experience of taking care of spouses with YOD was extracted. The extracted meaning units were further condensed into a description close to the text and labelled as ‘condensed meaning units’ (Graneheim & Lundman, 2004). The condensed meaning units were then abstracted and coded based on their content. Finally, the codes were then grouped into sub-categories and the sub-categories were further grouped into categories by comparing their similarities and differences (Graneheim & Lundman, 2004). The process of analysis was an iterative and ongoing process. The two researchers regularly discussed the issues related to the data analysis process, such as how the codes, sub-categories and categories were generated and the meaning of each code, sub-category and category until an agreement was reached.
Trustworthiness
All interviews were audio taped and transcribed verbatim. The transcripts were checked line by line against the audiotape to ensure that the transcription process was accurate and no personal ideas of the researchers were incorporated into the study (Lincoln & Guba, 1985). Second, two researchers participated in the data analysis process and met regularly to discuss any issues arising from the data analysis process until consensus was reached. This ensured the codes, sub-categories and categories developed were more accurate and objective (Lincoln & Guba, 1985). Third, an audit trail which documented the data collection and data analysis process, the selection of the research topic and the characteristics of the informants and setting was kept. This allowed readers to evaluate if the findings could be applied to another setting (Lincoln & Guba, 1985).
Results
Three categories about the unique caregiving experiences of Chinese spouses of persons with YOD were identified: (a) coming to terms with an unexpected diagnosis, (b) multiple unanticipated and ‘early’ losses and (c) finding positives and meaning.
Coming to terms with an unexpected diagnosis
All caregivers expressed that it was difficult to recognize the care-recipients’ cognitive and behavioural changes because both of the caregivers and the care-recipients were still at work. Some of these caregivers and the care-recipients even had to work on shift. Thus, they had little contact time with the care-recipients to recognize their changes. Indeed, most of the caregivers were usually alerted by the employers of the care-recipients about the care-recipients’ atypical changes. These changes were often described as ‘becoming slower than before’, ‘unable to plan and organize work’ and ‘keep asking the same questions’. Being affected by dementia, the care-recipients were not able to perform efficiently at work and made mistakes frequently. This had prompted the employer to offer leave for the care-recipients or even blame them without considering the possibility of having dementia: His boss found that he was unable to work independently. He always repeated what others had told him. He was unable to complete the tasks. Therefore, his boss called me and blamed, ‘I think he has to rest. He cannot work anymore’. (Caregiver 005)
Two caregivers in this study, however, were told by the care-recipients about the atypical changes rather than being alerted by the care-recipients’ employers. These two care-recipients were both housewives and had no full-time job at the time of dementia onset. They regarded the caregivers as their major support and used to share and discuss everything with the caregivers. Thus, these two care-recipients sought help from the caregivers once they had recognized those atypical changes. Those atypical changes were mainly related to memory problems and were severe enough to affect their daily functioning, such as meal preparation and feeding pets. These unusual changes had prompted caregivers to accompany the care-recipients for medical consultation immediately. However, the caregivers were also uncertain about the care-recipients’ changes at this stage and had never attributed those changes to dementia.
Insufficient knowledge about dementia had been frequently mentioned as the major barrier to early diagnosis by the caregivers in this study. They believed that dementia only affects older people. Caregivers therefore felt unprepared for the diagnosis and were shocked at the time of diagnosis disclosure. They often questioned: ‘I can’t believe that he is demented. He is in his 50s. He is still young. Why him?’. The diagnosis of dementia had brought frustrations, fears and uncertainties to these young spousal caregivers. All caregivers were uncertain about the care-recipients’ disease progression and felt difficult to plan for their future. In addition to these uncertainties, wife caregivers often worried about their financial conditions because the care-recipients had lost their ability to work and were unable to shoulder the financial responsibilities. Rather than worrying about the financial difficulties, husband caregivers, in contrast, were more concerned about their ability to provide day-to-day care to the care-recipients in the long run.
Most caregivers in this study often covered up the care-recipients’ diagnosis and isolated themselves from their social network. These caregivers explained that dementia was a stigmatized disease in Chinese culture. Having a family member with dementia was a kind of ‘loss of face (mianzi)’ (feeling shameful), especially when the family member was so young. They mentioned that dementia was an ‘elderly disease’ and should not be found in people with such a young age unless the care-recipients had done something bad in their past life. They stressed that others would look down on them if they disclosed the care-recipients’ diagnosis. Thus, these caregivers preferred to manage the problems within the family. One wife caregiver expressed: We [my husband and I] felt that we were being stigmatized by others [our friends and neighbours]. For example, one of our neighbours always asked him: ‘Who is she [caregiver]?’ My husband replied: ‘She is my mom.’ Then, he [the neighbour] laughed. I felt embarrassed…It’s a ‘loss of face’ to have a husband with dementia, especially when he is so young. I will not seek help from others because they will look down on me. I felt inferior to others. (Caregiver 006) Sometimes my wife [the care-recipient] told me that she was useless and she wanted to die. I would encourage her and said: ‘Why do you have such an idea? We should treasure every moment in life. Now, I treat you very well. I take care of you every day. You don’t have to worry anything. Just live your life to the fullest.’ (Caregiver 003)
Multiple unanticipated and ‘early’ losses
The diagnosis of dementia had brought multiple unanticipated and ‘early’ losses to the spousal caregivers of persons with YOD who were still young and in a more active life phase. Taking up the caregiving role had forced them to make transition into a new stage of life and face the various losses at a time earlier than they expected.
Most caregivers in this study had a full-time job at the time when the care-recipients were diagnosed with dementia. The sudden changes of the care-recipients had forced them to give up their employment and take up the caregiving role without any preparation. Even though the caregivers worried about their financial conditions as a result of unemployment, they eventually decided to take up the caregiving role. They believed that they should fulfil the marital obligation and should not leave the care-recipients alone to face the disease. Some caregivers therefore sought financial assistance from the government in order to compensate the financial losses due to the unemployment.
The demanding caregiving duties and the time-consuming nature of caregiving had also forced the caregivers to sacrifice themselves to provide constant care for the care-recipients. As a result, they experienced loss of social interactions, loss of time for their own activities and loss of their retirement plans. Caregivers were frustrated about these losses especially when they witnessed their friends who were at the same age but could travel around and enjoy their retirement life.
Another common loss that most caregivers experienced was the unanticipated ‘early’ loss of spousal relationship. The changes of the care-recipients as a result of dementia, such as changes in personality, communication and self-care abilities, had prompted the caregivers to question if the care-recipients were the one they married. Most caregivers were in deep sorrow when they witnessed their loved ones were gradually deteriorating and becoming more distant from them. At first, most caregivers wondered why the care-recipients had become a completely different person and felt hard to accept this change. A husband caregiver shared: She is very emotional now. Whenever I tried to stop her from doing something she wanted, she would shout at me very loudly. I’m sad but I have to tolerate her. I know that I need some time to accept [this change]. (Caregiver 002)
Furthermore, due to the impacts of dementia, the care-recipients’ cognitive and judgmental abilities were progressively deteriorating. They could no longer perform their usual family roles and fulfil their family responsibilities. Thus, caregivers had to take up all the family responsibilities and became the major support of the family. Both husband and wife caregivers considered this as a big challenge and they required time to learn and adapt to their new roles. For the husband caregivers, they used to work outside and provide financial support to the family. Therefore, it was challenging for them to learn new skills related to household matters and take up their wives’ responsibilities such as preparing meals, doing household cleansing and laundry. On the other hand, it was also challenging for wife caregivers to deal with the maintenance and repair at home, which had been previously done by their husbands.
The unexpected diagnosis of dementia had brought various unanticipated and ‘early’ losses to the spousal caregivers of persons with YOD. These losses could reflect how dementia had significantly affected the physical, psychological, social and financial aspects of the spousal caregivers’ life.
Finding positives and meaning
The spousal caregivers of persons with YOD were still young and had many years ahead of them. Most caregivers expressed that dementia and caregiving were the unavoidable sufferings in life. They realized that they were unable to change these situations, but they could change their own attitudes in facing these situations. Most of the caregivers stressed that it would be very painful if they could not cope with the frustrations, sadness and despair as a result of these unanticipated and ‘early’ losses. They therefore believed that they had to accept these losses in order to better adapt to their caregiving role. To facilitate the process of acceptance, most caregivers in this study then sought religious and spiritual support and found positives and meaning in caregiving.
A few caregivers therefore prayed for strength and wisdom for assisting them to go through the difficult caregiving journey, while some caregivers resigned caregiving to their destiny. These caregivers believed that everything was planned in life and they had to accept their destiny. Realizing that life was full of sufferings, these caregivers regarded caregiving as an opportunity to prepare themselves in facing the challenges ahead. These religious and spiritual beliefs had provided the caregivers with peace and motivated them to continue with their caregiving role.
Most caregivers also strove hard to find positives and meaning in caregiving in order to cope with the multiple unanticipated and ‘early’ losses. They reviewed the care-recipients’ condition and appreciated their own efforts in keeping the care-recipients’ condition stabilized or preventing them from deteriorating. This had provided caregivers with a sense of self-worth and encouraged them to continue providing good care to the care-recipients. Some caregivers gained a sense of satisfactions when they were appreciated by their relatives for the excellent care they had provided to the care-recipients. These appreciations had motivated caregivers to sustain their caregiving role because caregivers realized that they were doing something meaningful to the care-recipients. A husband caregiver shared: To me, taking care of my wife is definitely meaningful because I can bring hope to her and build up her confidence to live with dementia…Even my siblings appreciated what I have done to my wife. I’m confident to say that I have made a right decision [take up the caregiving role]. (Caregiver 004)
In order to reestablish the loss of spousal relationship with the care-recipients, some caregivers arranged shared activities with the care-recipients. These activities could simply be going out for a walk, participating in a one-day trip or performing cognitive training exercises together with the care-recipients. Some caregivers also made use of their old photographs to stimulate the care-recipients’ memories and recollect their mutual and joyful memories in life. When looking at the old photographs, the care-recipients were able to describe the events that the photographs had recorded and share their feelings. Through these interactions, caregivers were able to regain a sense of connectedness with the care-recipients and reestablish the loss of spousal relationship. Consequently, they no longer felt that the care-recipients were becoming increasingly distant from them. Instead, they believed that caregiving could be a way to continue their relationship.
Discussion
This study contributes to the current literature by describing the caregiving experience of spousal caregivers of persons with YOD in the Chinese sociocultural context. Similar to the findings reported in Western literature, these Chinese spousal caregivers also felt shocked at the time of diagnosis because of having insufficient knowledge about YOD. They also experienced various unanticipated and ‘early’ losses as a result of caregiving. However, this study has revealed that the caregiving experience of these Chinese spousal caregivers is influenced by their sociocultural values, which might have counterbalanced the negative impacts of caregiving and facilitated these caregivers to accept their caregiving role. Contrary to the Western literature, Chinese spousal caregivers in this study were able to find positives and meaning in caregiving.
It is evident that the spousal caregivers in this study also highlighted their difficulties in recognizing the care-recipients’ changes at the early stage. Even though they recognized the care-recipients’ cognitive and behavioural changes, they seldom related these changes to dementia. Instead, they just normalized the symptoms to work-related stress and tiredness. This might have been influenced by the low prevalence and the low public awareness of YOD in Hong Kong and the general assumption that ‘dementia affects older people’ (Lam et al., 2016). Although issues related to dementia have been much discussed in the local media recently, it has been seldom linked to younger people and the issues specifically related to YOD have not been highlighted. Thus, caregivers might not be aware of and overlooked the care-recipients’ symptoms. Numerous studies have demonstrated that media often overemphasize on the negative aspects of dementia, such as the incurable nature of dementia, the aggressive behaviours of the patients and the devastating impacts on caregivers (Gerritsen, Yolande, & Jessika, 2014; Van Gorp & Vercruysse, 2012). These have created a negative and stigmatized image to dementia and have significantly influenced the public perception of dementia (Gerritsen et al., 2014; Van Gorp & Vercruysse, 2012). Subsequently, caregivers’ interpretation of dementia, their emotional reactions at the time of diagnosis and their adjustment to the caregiving role have found to be affected (Sun, 2014). Thus, it is unsurprising that the caregivers in this study felt shocked, frustrated and were uncertain about their future.
Similar to other studies about Chinese dementia caregiving (Sun, 2014; Woo, 2016), this study also demonstrated that dementia is often associated with fear of ‘loss of face (mianzi)’ because of its stigmatized image in Chinese society. In Chinese culture, ‘loss of face’ does not only mean that the persons with dementia lose their social reputation but also bring embarrassments to their family (Lam et al., 2010). This issue appears more apparent in YOD and can be reflected in this study. Most care-recipients in this study were still young at the time of diagnosis and were the ‘breadwinners’ or the major support of their family. The diagnosis of YOD had not only affected their ability to work and to contribute to their family but also brought embarrassments and shame to their family. Thus, most of the care-recipients considered themselves as ‘useless’ and further isolated themselves from social network. In addition, their caregivers were also reluctant to seek outside support in order to avoid ‘loss of face’. Most caregivers in this study felt embarrassed to tell others about the care-recipients’ diagnosis because dementia was often associated with old age. The feeling of ‘loss of face’ among these spousal caregivers was more intense because the care-recipients were still young. They believed that people around them might misinterpret the care-recipients’ diagnosis because of the low public awareness towards YOD. Thus, these spousal caregivers appeared more sensitive to the public stigma and believed that others would look down on them. In order to ‘protect their face’, they therefore preferred to manage the problems within the family.
Various studies in Western cultures have reported that spousal caregivers of persons with YOD seldom describe positive aspects in caregiving (Cabote et al., 2015; Spreadbury & Kipps, 2017; Svanberg et al., 2011). Contrary to these studies, despite the negative experiences, the spousal caregivers in this study strove hard to sustain their caregiving role by finding positives and meaning in caregiving. One of the explanations to this difference can be related to the different sociocultural values in Chinese and Western cultures.
In Chinese culture, interdependence and obligation are highly valued in marital relationships (Tu, 1998). Couples are bound to marital philosophy which asserts the lifelong commitment to take care of each other. Like most of the studies about Chinese caregiving, caregivers in this study considered taking care of the care-recipients’ as a marital commitment (Miyawaki, 2015). Thus, they took up the caregiving role without considering caregiving could be a choice. Moreover, the belief of fatalism has also influenced how caregivers perceived their caregiving role and coped with the caregiving demands. Chinese people believe that everything is predetermined in life, including marriage and caregiving (Tu, 1998). Individuals are powerless to change the situation. Thus, caregivers in this study simply resigned caregiving to their destiny and accepted their caregiving role.
In addition, Chinese culture values collectivism, while Western culture emphasizes on individualism (Cheng, Lo, & Chio, 2010). In Chinese culture, the group’s goals are always prioritized on top of personal goals. Maintaining harmony and balance is the key to live in a collectivistic culture and to survive (Cheng et al., 2010). In order to maintain harmony and balance, acceptance is deemed to be an important response to difficult situations (Cheng et al., 2010). However, it does not mean that caregivers have to passively accept all difficulties and refrain themselves from pursuing their goals in life. Instead, they are encouraged to recognize the reality is changing and they have to change their own attitudes to face the difficult situations (Cheng et al., 2010). Chinese believes that every difficult experience can be beneficial to individuals because strengths, wisdoms and resilience can be derived from these difficult experiences (Cheng et al., 2010). Furthermore, Chinese culture also encourages individuals to embrace life as a whole, which means that individuals should not only focus on the ‘negatives’ but also the ‘positives’ in life (Cheng et al., 2010). This can be clearly revealed in this study. The spousal caregivers in this study adapted to the caregiving role by recognizing the positives in life and changing their own attitudes to face the situation. For example, they looked at the positive sides of the care-recipients and recollected their mutual and joyful memories. These memories provided caregivers with uplifts and mitigated the negative emotions arose from caregiving. Furthermore, caregivers in this study tended to focus on the meaningful side of caregiving instead of solely focusing on the losses. They felt satisfied and were more motivated to continue the caregiving role once they recognized they were doing something meaningful for the care-recipients. These findings provide significant implications for healthcare professionals in helping the spousal caregivers of persons with YOD to sustain their caregiving role.
Limitations
There are several limitations of this study. First, the sample of this study is small and may not be representative to all spousal caregivers of persons with YOD in Hong Kong. Moreover, the sample was recruited from a community centre which means that these caregivers might be more active and motivated to learn more about the disease and caregiving skills. Therefore, the experience of caregivers who are less active and isolated themselves from the community cannot be reflected in this study. Second, as the sample are all Hong Kong Chinese spousal caregivers, therefore, findings might not be applicable to other cultures. However, this study has opened a promising avenue for comparative study among different cultures. Third, no data about the care-recipients’ cognitive impairment status and the severity of the symptoms was collected. With this information, better understanding of the spousal caregiving experience at various stages could be obtained. Fourth, as the sample are all spousal caregivers who have good relationship with the care-recipients. The findings therefore might not be able to reflect those spousal caregivers who have poor relationship with the care-recipients. Although this study has several limitations, as to our knowledge, this is the first study in Hong Kong which aimed at exploring the caregiving experience of Chinese spousal caregivers of persons with YOD. This study significantly extends the current knowledge by providing important insights into the caregiving experience of Chinese spousal caregivers of persons with YOD.
Implications
Raising the public awareness of YOD is important for early recognition of symptoms, diagnosis and treatment (Spreadbury & Kipps, 2017). It can also reduce the negative and stigmatized image of YOD if appropriate promotion strategies are used (Van Gorp & Vercruysse, 2012). For example, inviting persons with YOD and their caregivers to share their experience through radio and television programmes. Rather than focusing on the negative aspects of YOD, their sharing can emphasize on the positive sides of living with YOD and their effective strategies to cope with YOD. Also, public health talks about YOD and carnivals can also be organized so as to raise the public awareness and cultivate a YOD-friendly living environment. This can prevent the persons with YOD and their caregivers from being stigmatized and isolated from the community.
In addition, empowering spousal caregivers and family members to take care of the persons with YOD is essential. As reported by the caregivers in this study, understanding more about the disease could facilitate them to adapt to their caregiving role. Currently, as most interventions are not tailor-made for these caregivers, interventions such as health education programmes which provide knowledge and caregiving skills specifically related to YOD are urgently needed. Further studies about the needs of these caregivers are warranted so as to better understand their situations and develop interventions specific to their needs.
It has been identified that spousal caregivers of persons with YOD always reported a sense of loss of spousal relationship (Cabote et al., 2015; Ducharme et al., 2013). Various studies have also demonstrated that communication and affection are important in maintaining spousal relationship (Ducharme et al., 2013; Wang, et al., 2017). The loss of communication in persons with YOD has affected their ability to show care and love to their spouses, hence affecting their spousal relationship (Wang, et al., 2017). However, it is important to acknowledge that the spousal caregivers in this study could cope with this loss by reviewing their life and showing old photographs to the care-recipients. This enabled them to reestablish a sense of connectedness and relationship with the care-recipients. Therefore, interventions using dyadic and life review approach might be beneficial to both of the caregivers and the persons with YOD. Through life review, nurses can guide them to think of the positive aspects of each other and their precious memories. At the same time, nurses should not ignore their difficult experiences. Instead, nurses should guide them to recognize their strengths in handling these difficult experiences and utilize their strengths to cope with the current caregiving situation.
In addition, YOD not only affects the persons suffering from it but it also affects every member in the family. Because family members are interdependent, their emotional and behavioural response can influence the well-being of other members in the family (Cabote et al., 2015). Therefore, further studies can focus more on the family experience of taking care of persons with YOD. For example, how the family adjust to live with YOD, the interactions between family members and how these interactions could influence their well-being and their decisions on the care-recipients’ care plan. Such findings can provide important insights for professionals to develop family-centred interventions and utilize the family strengths to assist persons with YOD to live with the disease.
Conclusion
This study has revealed that the spousal caregiving experience of persons with YOD is unique and is shaped by their sociocultural context. Because of having insufficient knowledge about YOD, the spousal caregivers in this study often normalized the care-recipients’ symptoms and believed that dementia would not affect young people. Thus, they usually felt shocked at the time of diagnosis disclosure. Similar to the findings reported in Western literature, caregivers in this study also encountered various unanticipated and ‘early’ losses. However, Chinese cultural values, such as ‘interdependence and marital obligation’, ‘fatalism’ and ‘harmony’ have helped these spousal caregivers to cope with the caregiving demands and accept their caregiving role. Thus, despite encountering multiple unanticipated and ‘early’ losses, these spousal caregivers were able to find positives in caregiving.
Furthermore, it is important to acknowledge that YOD not only affects the person suffering from it but also their family members. The emotional and behavioural response of each family member can influence one another (Cabote et al., 2015). Therefore, considering family as a unit and including all family members in further studies is warranted in order to achieve a comprehensive understanding about the family experience in taking care of persons with YOD. Such findings can provide insights into the development of family-centred interventions to support persons with YOD and their families to live with the disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Professional Development Fund of Association of Hong Kong Nursing Staff.