
Abstract
This scoping review is an extended version of a narrative review of couple-centred interventions in dementia shared in part A and the previous publication in this edition. The rationale for expanding study A emerged through the fact that most dyadic interventions have samples consisting of a majority of couples. The exclusion of interventions with samples of mixed relationships in part A therefore contributed to a narrow picture of joint dyadic interventions for couples in which one partner has a dementia. The aim of this second review is to explore the ‘what’ (types of interventions) and the ‘why’ (objectives and outcome measures) of dyadic interventions in which sample consists of a majority of couples/spouses and in which people with dementia and caregivers jointly participate.
Method
A five-step framework for scoping reviews guided the procedure. Searches were performed in Academic Search Premier, CINAHL, PsycINFO, PubMed, Scopus, and Web of Science.
Results
Twenty-one studies with various types of psychosocial interventions were included. The main outcome measure for people with dementia was related to cognitive function, respectively caregiver burden and depression for caregivers.
Conclusions
The findings of this extended review of joint dyadic interventions in dementia are in line with the findings of part A regarding the negative approach of outcomes, lack of a genuine dyadic approach, lack of tailored support, neglect of interpersonal issues and the overlook of the views of people with dementia. This review also recognises that measures of caregiver burden, as well as relationship quality should be considered in samples of mixed relationships due to the different significance of burden and relationship quality for a spouse as opposed to an adult child or friend.
Introduction
This scoping review is an extended version of our first study ‘A review of couple-centred interventions in dementia: Exploring the what and why part A (the previous publication in this edition)’, which was a narrative review of interventions aimed at couples where one partner has a diagnosis of dementia. The inclusion criteria of the first review required that people with dementia were living at home, that people with dementia and caregivers had partner relationships (spouses) and that they participated jointly throughout the intervention. The narrative review resulted in six studies and was considered to be too focused to enable a comprehensive view of joint dyadic interventions for couples with dementia to emerge. Nevertheless, the majority of the samples in joint dyadic interventions for people with dementia living at home consisted of couples/spouses (Moon & Adams, 2012; Smits et al., 2007; Van’t Leven et al., 2014). In this extended follow-up review, we will broaden our scope by extending the inclusion criteria to include joint dyadic interventions in which the majority of the participants consist of people with dementia and caregivers in a partner relationship. In this review, the spouse/partner of the person with dementia will be referred to as the care partner, whilst caregiver represents any kind of informal caregiver, including care partners.
Background
It is estimated that over 47 million people worldwide are living with dementia, by including all people affected by dementia, such as family and friends, the population would be significantly multiplied. The majority of people with dementia live in ordinary housing; in high-income countries the figure is estimated to be nearly two-thirds (Alzheimer’s Disease International, 2013). Most people with dementia wish to live at home with their family for as long as possible, having the opportunity to age in place enables feelings of attachment and preserved identity, roles, independence and relationships (Gould & Basta, 2013; Wiles, Leibing, Guberman, Reeve, & Allen, 2012).
Dementia is the leading condition for dependency in everyday living and the person therefore needs support of varying levels, which increases as the condition progresses (Alzheimer’s Disease International, 2013). Most people with dementia in ordinary housing live together with their partner who will often become an informal caregiver (Merrick, Camic, & O’Shaughnessy, 2016). It is estimated that 85% of couples where one partner has a dementia require some form of support to be able to continue to live together in their own home (Alzheimer's Disease International, 2009).
Support provided for couples living with dementia is often fragmented and unresponsive to need (Alzheimer’s Disease International, 2016), as reflected by most research that focuses either on the person with dementia or the care partner (Clare et al., 2012; Gilhooly et al., 2016; Hellström, Nolan, & Lundh, 2007). Moreover, support is often of a practical nature, e.g. cleaning, cooking, shopping, respite care, and/or psychosocial support mainly directed to the caregivers (Alzheimer’s Disease International, 2016; Gilhooly et al., 2016). This type of support is important; however, there is, at present, a lack of relationship-based support aimed at couples living with dementia.
The couple’s relationship is often challenged (Evans & Lee, 2014; Hellström et al., 2007; Robinson, Clare, & Evans, 2005) due to the constant change in roles and adaptive demands (Berg & Upchurch, 2007; O'Shaughnessy, Lee, & Lintern, 2010). Indeed, the experiences of spouses living with dementia are often described in terms of multiple losses, such as loss of identity as a couple, loss of shared decision-making, and loss of meeting life's challenges together. The willingness to care may also be reduced when the caregiving spouse experiences high levels of relationship loss (Davis, Gilliss, Deshefy-Longhi, Chestnutt, & Molloy, 2011). On the one hand, low relationship quality not only impact on couples wellbeing, but it also predicts need for nursing home admission (Joseph, Fang, Kathleen, & Jean, 2009; Spruytte, Van Audenhove, & Lammertyn, 2001). On the other hand, several authors point out that even though dementia has a significant impact on the relationship, a sense of connection love, warmth, closeness and affection may be intact (Ablitt, Jones, & Muers, 2009; Hellström et al., 2007; Wadham, Simpson, Rust, & Murray, 2016).
Supporting a couples’ relationship, therefore, has been highlighted to be of importance and has the potential to reduce the negative impact of dementia (Ablitt et al., 2009; Hellström, Nolan, & Lundh, 2005; Hellström et al., 2007; Keady, 1999; McGovern, 2011). Furthermore, supporting couples in utilising the strengths and positive resources of their relationship could help couples to focus on what they do have and what they can do, rather than focus on what they do not have and cannot do (Review Part A). Bearing in mind the importance of relational support for couples with dementia, in this follow-up review we wanted to explore the types and objectives of interventions aimed at this population.
Aim
The aim of this scoping review is to explore the ‘what’ and the ‘why’ of joint dyadic interventions in which the majority of participants are couples/spouses.
Scoping review questions
What types of interventions have been conducted for couples living with dementia? (What?) What were the objectives and outcome measures of the interventions? (Why?)
Methods
Study design
The main purpose of a scoping review is to map research from existing literature, which can lead to identification of knowledge gaps and recommendations for future research (Arksey & O’Malley, 2005; Davis, Drey, & Gould, 2009). Scoping reviews does not seek to assess the quality of studies (Arksey & O'Malley, 2005), nor the effectiveness of the interventions (Levac, Colquhoun, & O'Brien, 2010). Rather, scoping reviews contributes with a ‘what and why’ perspectives and new perspectives of current research. This review is intended to provide a summary of ‘what’ interventions that have been conducted, and ‘why’ in terms of their theory of impact which we assume to be mirrored by the objectives and outcomes. We also intend to identify knowledge gaps and to provide recommendations for future research. A five-step framework for scoping reviews guided the procedure. The five steps include: identifying the research question, identifying relevant studies, study selection, charting the data, and collating, summarising and reporting the results (Arksey & O’Malley, 2005).
Search terms
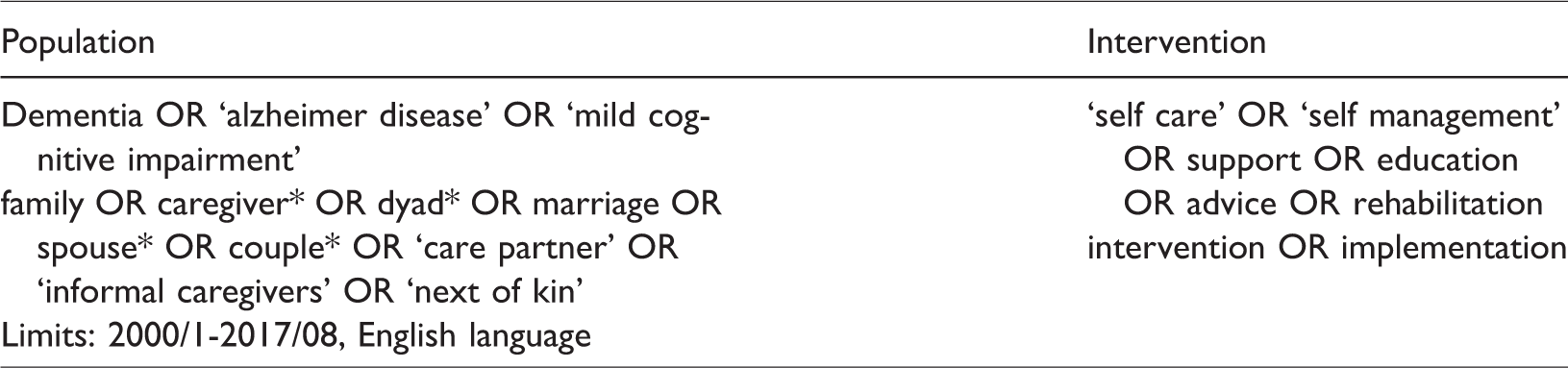
Dementia was defined broadly and included all types of dementia diagnosis and mild cognitive impairment (MCI). The support strategy of interventions was also defined broadly to include various types of interventions, from self-care and self-management to support, advice, education and rehabilitation. Search terms and limits are displayed in Table 1.
Search terms and limits.
Search strategy
A Boolean string was established with truncated search terms and adapted to the specific databases in which the searches were performed. We searched Academic Search Premier, CINAHL, PsycINFO, PubMed, Scopus, and Web of Science for articles published from January 2000 to August 2017 and limited to English language (Table 1). Inclusion criteria required: Person with Dementia or person with MCI who was living in ordinary housing and was participating in the intervention together with a caregiver. Dyads should not be separated during the intervention and the majority of participants should have partner relationships (spouses). Exclusion criteria were review articles, study protocols (design articles) and care programmes (care management). Inclusion and exclusion criteria are presented in Table 2.
Inclusion and exclusion criteria.

PwD: person with dementia; MCI: mild cognitive impairment; CG: caregiver.
Selection of studies
Searches generated in total, 5711 references. The EndnoteX7 software tool was used to organise references and remove duplicates. When abstracts were lacking information of the sample, and if people with dementia and caregivers jointly participated in the intervention, full text scanning of the articles was required. Out of the 5711 references, 667 articles where scanned in full text. Out of these, a high number of articles were excluded (647) due to that many appeared to have separate support for the person with dementia and the caregiver. The review process resulted in 20 articles. We also searched the reference lists of the 20 articles, which generated one additional article. See article selection flowchart in Figure 1.

PRISMA flow diagram.
The summary table
A summary table of key categories was constructed (Table 3). Data for extraction was identified through multiple readings of the articles. Both authors read, collated and analysed the data for consistency. The category source was chosen to gain an overall view of authors, country and year of publication. Information was extracted from articles and presented in the category. The categories design and type of intervention, sample and implemented (where, by whom) were chosen for representing the ‘what’. Design was labelled consistently, although different terms occurred in the articles. Sample and implemented (where, by whom), were extracted when available and presented in the categories. The categories objectives/goals and outcome measures were chosen for identifying the ‘why’. In this review, objectives/goals relate to the theory of impact on participants, and were therefore defined broadly and included formulations as goals, objectives and hypotheses that could be identified in the articles. If objectives or goals for participants were not stated specifically, we identified sections where hypotheses or theories of impact for people with dementia and caregivers were formulated. Studies included a broad range of outcome measures. Outcome measures were extracted from articles and listed under the person to whom they referred, i.e. outcomes listed under the person with dementia included indirect outcome measures from caregiver views (see Table 3). In order to provide a summarised overall view of outcomes, we grouped the outcomes with related content, and for people with dementia and caregivers, respectively. Outcomes are listed in relation to whom the measures refer to, i.e. outcomes listed under people with dementia also include indirect outcome measures from caregiver views (Table 4). See online appendix for grouping procedure.
Interventions for people with dementia and caregivers.

PwD: person with dementia; CG: caregiver; RCT: randomised controlled trial.
Overview of outcomes for people with dementia and caregivers.
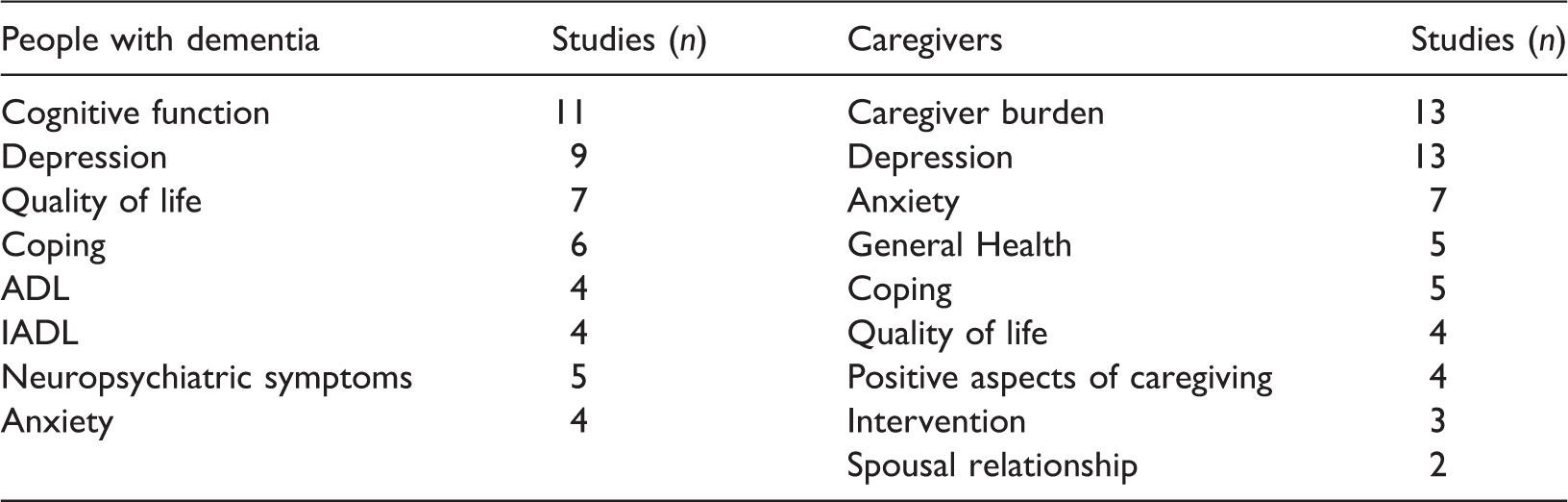
ADL: activities of daily living; IADL: instrumental activities of daily living.
Results
‘What’
Twenty-one studies were included in this review. The majority of the studies were conducted in the USA (n = 11), followed by the UK (n = 4), Australia (n = 2), Sweden (n = 1), the Netherlands (n = 1), Spain (n = 1) and Ireland (n = 1). The year of publication ranged from 2000 to 2017. Approximately two-thirds of the interventions were randomised controlled trials and one-third had a single group design. Fifteen studies had interventions delivered for the dyad individually and six studies involved group interventions (Camic et al., 2013; Osman et al., 2016; Roberts & Silverio, 2009; Schmitter-Edgecombe & Dyck, 2014; Schmitter-Edgecombe et al., 2008; Woods et al., 2012). Analysis revealed various types of psychosocial interventions, counselling, music therapy, cognitive (-stimulation/-rehabilitation/-behavioural therapy), exercise, skills training, goal attainment, psychoeducation and reminiscence (Table 3).
Sample sizes varied between four dyads (Schmitter-Edgecombe et al., 2008) and 488 dyads (Woods et al., 2012). Approximately one-third of interventions had samples consisting of only couples (Auclair et al., 2009; Baker et al., 2012; Neely et al., 2009; Quayhagen & Quayhagen, 2001; Quayhagen et al., 2000; Schmitter-Edgecombe et al., 2008) which were the included studies in our narrative review , and two-thirds had samples of dyads with mixed relationships. People with dementia had diagnoses of mild to moderate dementia or MCI. Occurring diagnoses were: Alzheimer's disease (AD), vascular dementia, MCI, very mild dementia (VMD) and amnestic mild cognitive impairment (AMCI) (Table 3). Gender was not provided in two studies (Auclair et al., 2009; Camic et al., 2013), and only gender of people with dementia was provided in Stanley et al. (2013). Gender distribution based on 18 articles revealed that the majority of people with dementia were male (about 60%) and the majority of caregivers female (about 70%).
Interventions were delivered in the dyads’ home, community settings/sites or clinics. Twelve of the interventions were home-based or primarily home-based. Four of the studies did not provide the location where the intervention was implemented (Auclair et al., 2009; Martin-Cook et al., 2005; Schmitter-Edgecombe & Dyck, 2014; Schmitter-Edgecombe et al., 2008). Caregivers, clinicians, article authors, nurses, facilitators, volunteers, social workers, doctoral students, graduate students, and music or exercise professionals implemented the interventions. One study, O’Sullivan et al. (2015), did not provide information on who implemented the intervention.
‘Why’
Objectives/goals for participants could be identified in all articles except one by Quayhagen and Quayhagen (2001). The objectives were various but most commonly related to wellbeing and cognitive function (Table 3). Two studies had only qualitative outcomes (Auclair et al., 2009; Osman et al., 2016). Some of the quantitative studies included one or two qualitative outcomes, most commonly related to the experience of the intervention (Baker et al., 2012; Camic et al., 2013; Hanser et al., 2011; O’Sullivan et al., 2015; Quayhagen et al., 2000; Stanley et al., 2013). The overview of outcomes showed that the most frequently used outcome measure for people with dementia was related to cognitive function, which occurred in 11 studies, followed by outcomes of depression in nine studies and outcomes of quality of life in seven studies. The most frequently used outcome measures for caregivers were related to caregiver burden and depression, which occurred in 13 studies each, followed by outcomes related to anxiety, which occurred in seven studies (Table 4).
Discussion
The purpose of this scoping review was to explore the ‘what and why’ of interventions in which couples living with dementia jointly participated without being separated during the intervention. We hypothesised that interventions delivered joint, would be the optimal condition to identify interventions that focuses on relationships and which targets both the person with dementia and the caregiver.
The What and Why
Twenty-one studies were included in this review. Mapping of the ‘What’ showed a wide range of psychosocial interventions, which were most commonly conducted within the discipline of psychology. Most interventions were dependent on the delivery of professionals and required dyads to travel to community sites or clinics. No intervention was referred to as self-management although some interventions had components that could be viewed as self-management, i.e. when the caregiver was implementing the intervention after receiving instructions from professionals (Baker et al., 2012; Hanser et al., 2011), or where interventions included homework . Exploring the ‘Why’ showed a wide range of objectives/goals for participants; predominant were the objectives within the cognitive domain for people with dementia and in the psychological domain for caregivers, reflected by the outcome measures that were mainly related to cognitive function for people with dementia, and to caregiver burden and depression for caregivers.
Identified areas of challenge within dyadic interventions
The reviewed joint dyadic interventions promoted opportunities for interaction and shared activity either for the individual dyad or through group sessions, supporting the importance of social interaction and social inclusion. However, we identified several challenging areas that limited interventions to be delivered with a dyadic approach and which also limited possibilities for tailored support. We will highlight these areas below.
The neglect of interpersonal issues
According to Martire, Schulz, Helgeson, Small, and Saghafi (2010), dyadic interventions differ widely regarding involvement of interpersonal issues, which is also shown in this review. Neglect of interpersonal, and ‘real world’ impact, occurs when caregiver–care recipient relationships are being viewed as homogenous (Purkis & Ceci, 2015) which has a tendency to occur when relationship factors are disregarded. More than two-thirds of the studies in this review had samples of mixed relationships, a factor leading to high risk of neglect of the different significance of outcomes such as burden, strain, losses and quality of relationship for a spouse as opposed to an adult child or friend. Reasons for embracing a less dyadic approach in dyadic interventions may be due to the desire to apply findings to a broader population, and the conduction of group interventions which have benefits in regard to financial resources but disadvantages in addressing interpersonal issues (Martire et al., 2010). The lack of relational understanding has been highlighted in previous reviews of dyadic interventions (Moon & Adams, 2012; Van’t Leven et al., 2014) as well as the importance of differentiating between caregiver subgroups (Braun et al., 2009; Smits et al., 2007). A clearer relational understanding and taking into account the nature of the relationship could enhance interventions in dementia (Merrick et al., 2016) thus leading to that outcome measures such as burden, strain and relationship quality can be interpreted in the right context.
Need for relationship sustaining care
Sustaining relationships, especially close emotional relationships (Smebye & Kirkevold, 2013), is a crucial factor for the person with dementia to be able to maintain sense of personhood (Hellström et al., 2005; Phinney, 2002; Smebye & Kirkevold, 2013). Caring within families should be viewed from an holistic, historical and systemic perspective as each relationship has a specific dynamic with different strengths and weaknesses that affect the relationship (Morhardt & Spira, 2013). Unfortunately, the findings of this review suggest that most interventions failed in regard to an holistic approach. Dyadic interventions, in which a holistic approach is applied, should have increased potential to support close relationships, thus contributing to sustained sense of personhood, and for partners’ also sustained sense of couplehood.
Lack of tailored support
Two previous reviews of dyadic interventions (Moon & Adams, 2012; Van't Leven et al., 2014), which included studies with joint and separate sessions for people with dementia and caregivers, showed promising effects on both members of the dyad’s well-being. However, both reviews highlighted the need for a couplehood approach and for tailored support. The lack of tailored support in dementia care was also highlighted in our previous review of couple-centred interventions (Review, Part A). In order to tailor support and determining appropriate outcomes, the nature of the relationship must become considered more important, as well as the target of the intervention must be adapted to the specific needs of the dyad. The latter was also discussed in our previous review (Review, Part A) with regard to the assumptions of that relationships in dementia are assumed to be burdensome. The majority of the outcomes in this review are illness-specific, symptom-oriented and are focusing on negative aspects of dementia. Arguably, such an approach is not beneficial for all dyads and does not match the needs of all dyads. We believe, therefore, in line with Van't Leven (2014), that a structured needs assessment of both the person with dementia and the caregiver prior to the intervention would enhance stronger and more realistic effects. Additionally, an illness-specific and symptom-oriented approach may even impact on the dyads views of their situation when presented to a battery of outcomes related to negative aspects of dementia.
Overlooking the views of people with dementia
Exclusion of the person with dementia’s views was a recurring feature in this review; nearly one-third of the interventions based all their outcome measures on caregiver views only (Baker et al., 2012; Hanser et al., 2011; Judge et al., 2013; Martin-Cook et al., 2005; Neely et al., 2009; Prick et al., 2015). These studies clearly overlooked the views of people with dementia, but this might be a too simplistic conclusion to draw when interventions had different targets and different objectives. Judge et al. (2013), for example, with only outcome measures for caregivers, makes it clear that they focus on caregivers with a battery of outcome measures related to burden. However, it has to be questioned whether or not caregiver burden can be viewed in isolation from relationship dynamics and the nature of the relationship. A similar issue arises in the one study focusing exclusively on people with dementia, which involves goal setting and goal achievement in regard to personal, relevant goals (O’Sullivan et al., 2015). Even though the goal setting was primarily related to memory function, e.g. everyday life, habits, routines and personal goals, there is a reciprocal impact on a relationship and vice versa, not least when it comes to couples living in the same household. The remaining studies can thus be considered to focus on dyads, but they still lack a dyadic approach (i.e. overlooking relationship factors, failing to report on dyadic data and/or failing to include the views of people with dementia in dyadic data), with the exception of the two studies with qualitative outcomes (Auclair et al., 2009; Osman et al., 2016). However, not asking for people with dementia’s views is always difficult to justify, despite the severity of dementia (Clare, 2017; Dementia Alliance International, 2016). In this review, in which studies focus on mild to moderate dementia, it should be even harder to justify this phenomenon. Overlooking the views of people with dementia is not the only way to produce a fragmented picture of dyad’s dynamics; a fragmented picture might also occur when outcomes are proxy-measured.
Lack of easy-accessible support
The studies in this review were dependent on the delivery of professionals and/or required dyads to travel to community sites or clinics. Given that the number of couples living with dementia will increase in the coming years, support should not only be dependent on resources in the care sector. In recent years, there has been an increasing interest in cost-effective interventions for people with dementia and informal caregivers such as self-management interventions (Quinn et al., 2016). Self-management for people with dementia, however, could be considered controversial due to a common (mis) conception that people with dementia are unable to learn new skills (Martin, Turner, Wallace, & Bradbury, 2013; Mountain, 2006) and that they should not be given too much responsibility over their situation (Ibrahim et al., 2017). However, in order to apply self-management for people with dementia, the target should focus on managing everyday life rather than managing the condition (Martin et al., 2013). A dyadic format of self-management could be appropriate in order for the person with dementia to be supported by a family member, as well as to apply the importance of relationship sustaining care, and in order to provide increased accessibility.
Some limitations need to be addressed in this review. A scoping review aims to provide an overall view of the research area and may therefore fail to include all relevant literature. We excluded care programmes and care management as they often involve multi-component interventions not described in detail, which leads to difficulties in reproducing the content of the intervention and in determination of joint participation. Some of the reviewed interventions did not explicitly state their objectives/goals, in those we identified sections in which some theory of impact for participants could be identified and might therefore not be the primary objective of the intervention. Outcome measures of the interventions were broad and difficult to compare among the studies. In order to summarise and obtain an overall view of the outcomes, the outcomes with related content were grouped and labelled. The significance of outcomes may be interpreted in different ways, and may therefore be considered when interpreting the findings. Another limit to this study was the exclusion of studies that not reported the proportion of couples/spouses in their sample (see for example Orrell et al., 2017). Considering that most participants in dyadic interventions are couples/spouses, some studies may have been overlooked. Additionally, our inclusion criteria of purely joint interventions excluded interventions with separate sessions for the members of the dyad. For example, in the study of Charlesworth et al. (2016), in which the majority of participants were couples/spouses, they combined joint and separate sessions and was therefore excluded. In this scoping review, we were interested in interventions where the couple participated together throughout the intervention and does not mean to insinuate that combinations of joint – and separate – sessions are always lacking a dyadic and/or relationship-focused approach.
Conclusions
This scoping review indicates that many dyadic interventions which include couples in which one partner has a dementia are lacking a relational understanding. The joint design of the reviewed articles thus promoted opportunities for interaction and shared activity either for the individual dyad or through group sessions, supporting the importance of social interaction and social inclusion. The majority of interventions in this review did not take into account relationship factors and the nature of the relationship, which reduced the opportunities for tailored support and outcome measures. Even when dyadic interventions have the primary objective of reducing caregiver burden or neuropsychiatric symptoms in people with dementia, we dare to say that there always are relationship factors present, and that the voice of people with dementia should be obvious in the context of dyadic joint interventions.
Implications for future research
The findings of this review indicated a lack of relational understanding in dyadic interventions. We suggest that future research should involve a needs assessment tool and a screening of the quality of the relationship prior to the intervention, which aims to give guidance on which path to choose; improving or sustaining relationships (or abilities). We also suggest that support for people with dementia and caregivers should be complemented by easy accessible support such as self-management that focuses on everyday wellbeing rather than on the condition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The support of the Economic and Social Research Council (ESRC) and National Institute for Health Research (NIHR) is greatfully acknowledged. This work forms part of work programme 6 of the ESRC/NIHR Neighbourhoods and Dementia mixed methods study [![]() ]
]
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.