
Abstract
A diagnosis of mild cognitive impairment is associated with an increase in anxiety and depression and a decrease in psychological well-being. Despite this, individuals with mild cognitive impairment may not receive the appropriate support needed to manage the emotional and practical elements of their diagnosis. A psychosocial group intervention based on the ‘Recovery Model’ was developed in order to meet these needs. Outcome data from a trial of this group intervention indicated it was successful in meeting its aims.
Background
Although the specifics of the term are contested (Peters & Katz, 2015), a label of mild cognitive impairment is typically given when an individual presents with degree of cognitive impairment that is abnormal, given their age and education level. This impairment represents a decline in previous level of cognitive functioning, though less significant than would receive a diagnosis of dementia. However, those with mild cognitive impairment have an elevated risk of developing dementia in the future, with an estimated annual conversion rate of 10–15% (Petersen et al., 2009).
Within the United Kingdom, official guidelines (National Institute for Health and Care Excellence, 2006) recommend those with mild cognitive impairment are monitored by memory assessment services. Whilst the individual would be recalled to the service 12 months after the initial diagnosis, traditionally little has been provided to help them manage the emotional and practical impact.
Recent research suggests that those with mild cognitive impairment are at an increased risk of anxiety and depression (Orgeta, Qazi, Spector, & Orrell, 2015) and decreased psychological well-being (Gates, Valenzuela, Sachdev, & Singh, 2014). This is perhaps unsurprising, given the impact of cognitive impairment on daily functioning and the degree of uncertainty associated with the diagnosis. Furthermore, previous qualitative research has indicated that a diagnosis of mild cognitive impairment can be troubling for individuals, leaving them feeling unequipped to deal with their current impairment or future prospects (Frank et al., 2006; Lingler et al., 2006).
Within the Birmingham Solihull Mental Health National Health Service Foundation Trust, individuals diagnosed with mild cognitive impairment were referred from memory assessment and community mental health services to the Older People’s Intervention Pathway. The Older People’s Intervention Pathway provides tailored interventions for older adults within the community who experience both functional and organic mental health difficulties. These include a number of psychosocial interventions for individuals with dementia. Two previous dementia intervention groups – the ‘Self-Management Programme’ (Martin, Turner, Wallace, & Bradbury, 2013) and ‘Memory Management’ (Molly Burnham, private communication 2014), were combined and adapted to create a new mild cognitive impairment group intervention.
Method
Design
The study was an A-B design – outcome measures were taken at a baseline, at the beginning of the group intervention, and again following the completion of the group intervention. A total of 16 individuals attended across three complete group intervention programmes. Individuals were referred to the service from older adult Community Mental Health Teams and a local Memory Assessment Service. They were then screened by a facilitator to ascertain suitability regarding the group intervention. Participants were assessed as suitable on the following criteria:
They had received a diagnosis of mild cognitive disorder within the last year. Within the National Health Service Trust, diagnoses are made with reference to the International Statistical Classification of Diseases and Related Health Problems (ICD-10; World Health Organization, 1992), with ‘mild cognitive disorder’ representing an alternate label for ‘mild cognitive impairment’. They expressed interest and motivation in engaging with the group intervention. They were physically able to attend the group at a central location. Their cognitive impairment and/or any sensory deficits were not so severe as to prevent them from following the pace of the group or retaining the information discussed (although hand-outs were produced to aid retention of discussed material).
Demographics
Four individuals attended the first group, five attended the second and seven attended the third. Ages of group participants ranged from 56 to 87 years old, with an average age of 74.2. Nine participants were female, seven were male. All groups took place in an outpatient setting.
Procedure
Each group was staffed by two experienced facilitators. The outpatient service has been running as a group therapy service for eight years and each staff member has received training in group therapy skills as well as specific training in the challenges of mild cognitive impairment. Each facilitator was supervised by a clinical psychologist.
The intervention consisted of eight, two-hour, weekly sessions. The overall aims of the group were to provide:
Social and emotional support, normalisation and validation, in a setting where all individuals could share and benefit from each other’s experiences. This was measured by the Warwick Edinburgh Mental Well Being Scale (outcome measure references available on request from the author). Practical support and the provision of tips, strategies and aids to help manage the impact of cognitive impairment within daily functioning. This was measured by the Goal Attainment Scale. Promotion of well-being and the continuation of meaningful and enjoyable activities despite the impact of cognitive impairment. This was again measured by the Warwick Edinburgh Mental Well Being Scale.
The individual sessions were designed to discuss the nature of mild cognitive impairment and the experience of the same, memory strategies, the impact of mood on memory and steps to manage the same including the impact on social relationships. There was a session dedicated to enduring personhood and this was maintained as a focus throughout the group with an emphasis on setting goals and celebrating weekly achievements. The philosophy behind the group was drawn from the Recovery Model (Roberts & Wolfson, 2006), which seeks to promote the person behind the diagnosis and focuses on how they can remain in touch with their identity and continue living a meaningful and valued life despite the challenges. Please contact the author for copies of the protocol.
Outcome measures
Pre- and post-outcome measures were taken in sessions two and eight of the intervention. Session two was chosen because evidence has suggested that measures used at Session 1 will capture the uncertainty of starting a new intervention and risk overwhelming the older person with paperwork, thus threatening clinical engagement (Stone, 2013). The Warwick Edinburgh Mental Well-Being Scale was used as a measure of group members’ levels of well-being. The Warwick Edinburgh Mental Well-Being Scale consists of 14 positively-worded statements relating to different aspects of well-being, for example – ‘I’ve been feeling useful’, ‘I’ve been feeling optimistic about the future’, ‘I’ve been feeling close to other people’. Participants were asked to indicate the degree to which they felt each statement described their experience over the last two weeks. Responses for each statement are given using a five-point Likert scale, with potential answers being:
None of the time (a score of 1) Rarely (a score of 2) Some of the time (a score of 3) Often (a score of 4) All of the time (a score of 5).
Possible scores range from 14 to 70, with higher scores indicating greater levels of well-being. Population norms have been obtained within England (Health & Social Care Information Centre, 2012) and Scotland, (Davidson, Sewel, Tse, & O’Connor, 2009) indicating mean scores of 51.6 (standard deviation [SD] = 8.7) and 50.7 (SD = 8.8) respectively.
The Goal Attainment Scale was used to ascertain individual’s goals regarding attendance of the intervention and whether they were successful in meeting these. Goals set by the participants tended to focus around developing a greater understanding of mild cognitive impairment, dealing better with the practical difficulties of mild cognitive impairment (e.g. learning memory strategies) and/or dealing better with the emotional impact of mild cognitive impairment (e.g. increasing levels of confidence). At the end of the group, participants were asked whether they felt they had met their goals. Their responses were indicated using a five-point Likert scale, with potential answers being:
I met the goal much better than expected I met the goal a little better than expected I partially met the goal I didn’t meet the goal and am at the same level as before I didn’t meet the goal and am worse than before.
Finally, a ‘Family and Friends Test’ was used at the end of the group (Session 8) to indicate how likely group members would be in recommending the intervention to family members or friends, supposing they were also diagnosed with mild cognitive impairment/disorder and could potentially benefit. They were also asked to provide their reasons for their recommendations (or lack thereof). This information is routinely collected in National Health Service practice since April, 2013 (National Health Service England, n.d.). This information can be highly skewed and is included as an indication of the value that participants placed on inclusion in the group. A score of 8 out of 10 or higher would indicate a positive score. A score below 8 would indicate that the person was dissatisfied with the service.
Results
Despite the small sample, the Warwick Edinburgh Mental Well-Being Scale data met criteria for parametric statistics and were analysed by Microsoft Excel using a dependent t-test. This analysis indicated that group members’ levels of well-being were higher at the end of the intervention (M = 57.16, SD = 8.87) than the beginning (M = 48.01, SD = 7.77). This increase in well-being was statistically significant, t(15) = 4.89, p > 0.01, two-tailed (Figure 1).
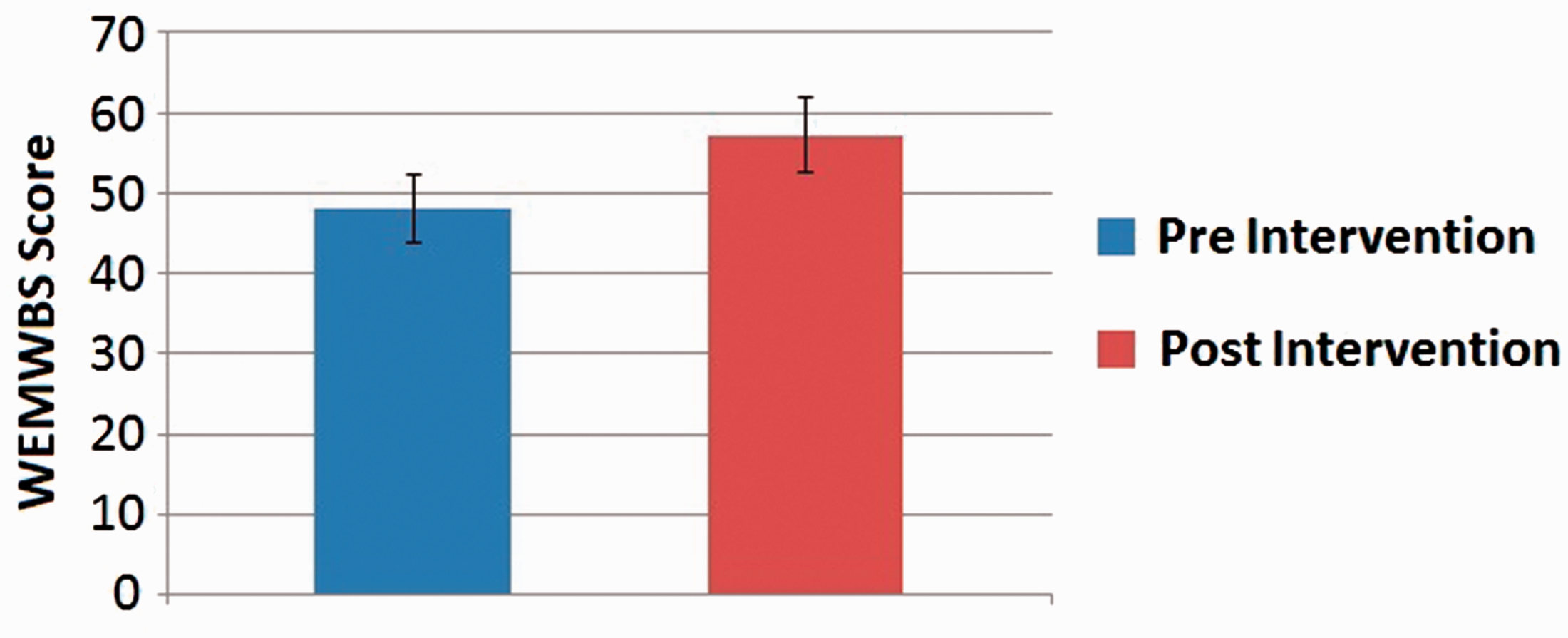
A comparison of group members' mean scores on the Warwick-Edinburgh Mental Well-being Scale (WEMWBS) before and after the group intervention. Error bars represent 95% confidence intervals.
The Goal Attainment Scale data were not normally distributed, given the small sample size and the grouping of data. It indicated that 15/16 group members rated themselves as meeting their goals ‘much better than expected’, with the final group member having met their goal ‘better than expected’ (Figure 2).
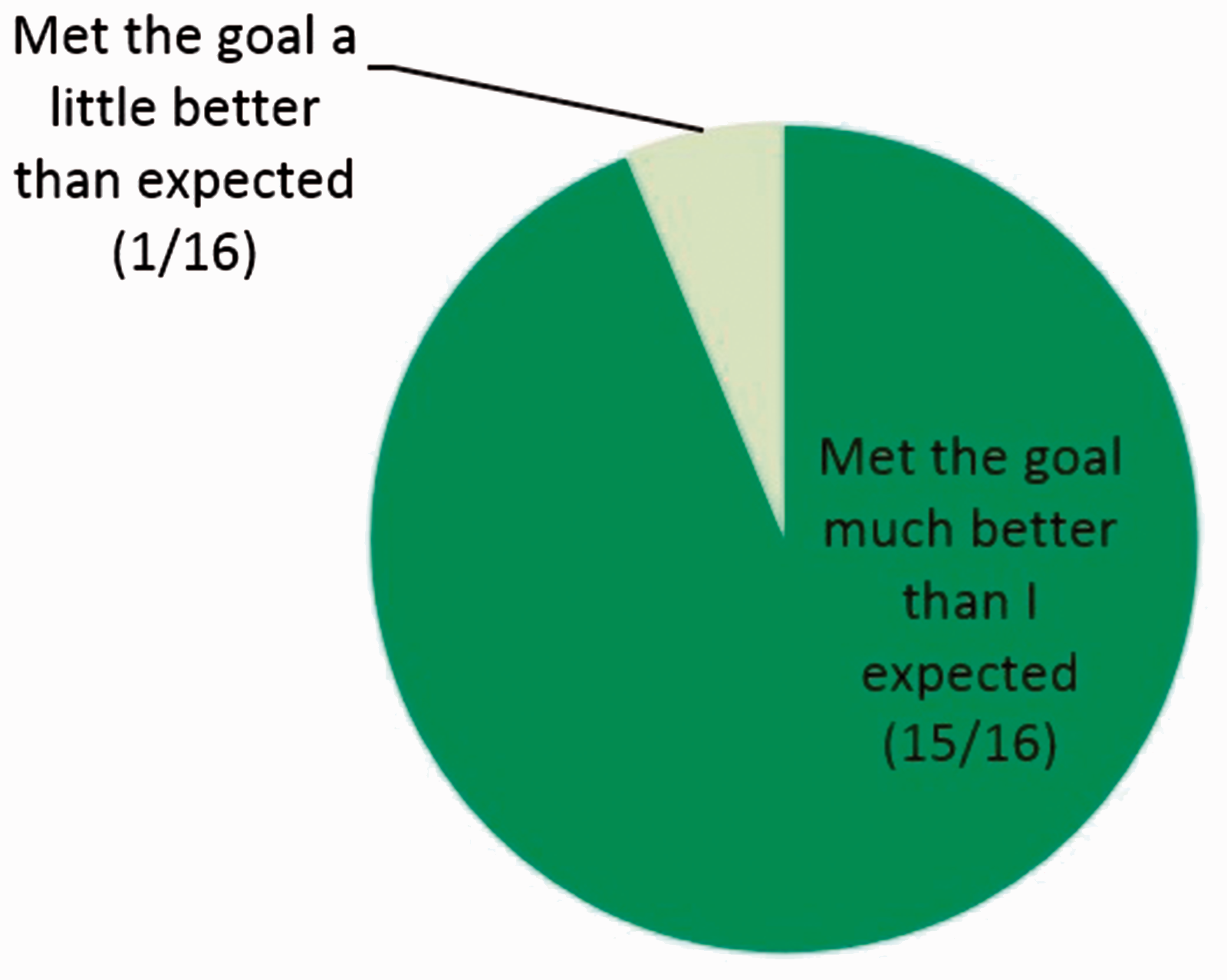
Group members' responses on the Goal Attainment Scale outcome measure.
Data from the Family and Friends test indicated that all participants would be likely to recommend the group intervention, with 14/16 individuals giving the highest possible recommendation (Figure 3).
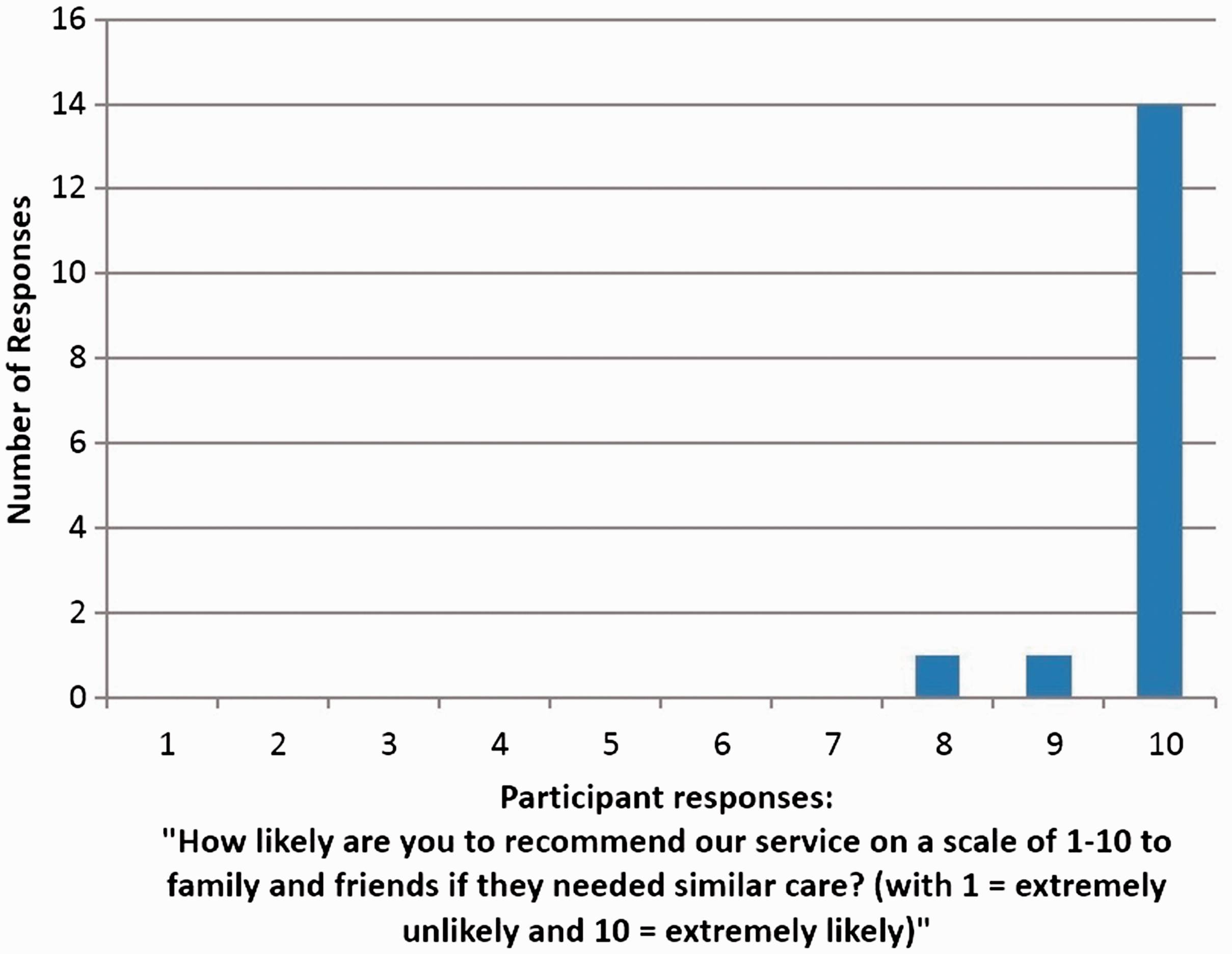
Group members’ responses on the Family and Friends outcome measure.
Discussion
Although only based on a small sample of 16 individuals, the outcomes from this group intervention indicate that it has been successful in improving the emotional well-being of participants and meeting the practical goals set by the individuals who took part after being diagnosed with mild cognitive impairment. Of particular note is the significant increase in well-being associated with attendance of the group intervention. The Warwick Edinburgh Mental Well-Being Scale scores for the group prior to the intervention were in the low average range for the age group (Mean for England is expected at 51.6, SD = 8.7), we hypothesise this indicates the emotional impact of the diagnosis as previously reported (Orgeta et al., 2015) and the experience of managing the symptoms of mild cognitive impairment. This is significantly alleviated with a group intervention that normalises this experience and educates individuals to maintain their mental health. The emphasis and philosophy behind these ideas is the Recovery Model, which encourages participants to maintain their sense of personhood and continue living according to personal commitments and values despite their diagnosis. There has been some debate about whether the Recovery Model, traditionally in the UK applied to those with functional mental health difficulties, might benefit those experiencing dementia (Hill, Roberts, Wildgoose, Perkins, & Hahn, 2010) and the way in which this is a natural progression from the person-centred care model. However, the outcome of this group intervention suggests that adopting this approach can be beneficial for those diagnosed with mild cognitive impairment.
These results can be compared with other psychosocial interventions commonly used in dementia. For example, cognitive stimulation therapy has been found to improve confidence, interaction and quality of life for individuals with dementia (Woods, Aguirre, Spector, & Orrell, 2012) and as such is a nationally recommended intervention within the United Kingdom (National Institute for Health and Care Excellence, 2006).
We recognise that the current study featured low number of participants (16 in total) and so widespread generalisations cannot be made regarding the impact of psychosocial interventions for individuals with mild cognitive impairment. Furthermore, the current study has not been able to control for the contact that is provided by the group.
Follow-up investigations would be valuable, to ascertain whether the gains experienced in the group are maintained and if there were other long-term benefits; for example, to see whether those who went on to develop dementia were better able to manage their mental health and daily functioning as a result of the support received within the mild cognitive impairment intervention. Whilst further exploration would be required, the current study should be considered a pilot with promising results, which encourages consideration of the emotional impact of a diagnosis of mild cognitive impairment and the way in which health workers can alleviate the difficulty.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.