
Abstract
There is a paucity of information on the perceptions of community pharmacists about the nature and effectiveness of pharmaceutical care services they provide to people living with dementia in care homes. This paper explores pharmacists’ perceptions of the nature and effectiveness of pharmacy services provided, and their experiences when providing these services. Community pharmacists delivering services to care homes with dementia in Thurrock, Essex and in Medway, Kent, England were invited to participate in the study involving face-to-face interviews. Analysis of semi-structured interviews with 15 community pharmacists revealed that the main pharmaceutical service provided by the pharmacists was prescription processing, normally involving the clinical review and supply of medication into monitored dosage systems (dosette boxes) and delivery to the homes. This was coupled with advice to care homes on the appropriate storage and administration of drugs and appliances supplied, which was in line with the NHS Community Pharmacy Contractual Framework Enhanced Service for care homes. A majority of the community pharmacists interviewed acknowledged that the services they were currently commissioned to provide did not meet the pharmaceutical care needs of dementia patients in care homes, including the monitoring of the appropriateness, safety and effectiveness of drug therapy.
Introduction
Dementia is a broad term used to describe a range of progressive, degenerative, terminal organic diseases characterised by continuous deterioration in cognitive function (Malek & Greene, 2014). Though not a normal part of ageing, dementia constitutes one of the major causes of disability in later life, and its prevalence doubles with every five-year increment of age after 65 (World Health Organisation / Alzheimer’s Disease International (WHO/ADI), 2012). This poses great challenges for health care systems worldwide, due to the ageing global population. In 2009, it was projected that by 2050, there will be over two billion people aged over 60 (United Nations, 2009). In 2016, it was estimated that over 47 million people worldwide were living with dementia, set to rise to 131.5 million by 2050 (Alzheimer’s Disease International, 2016).
The commonest cause of dementia is Alzheimer’s disease (AD) (60%) followed by vascular dementia (VaD, 15–20%), dementia with Lewy bodies (DLB, 15%), other rarer causes and occasionally reversible conditions (5%) (O’Brien & Burns, 2010). In the UK, there are over 850,000 people living with dementia, a figure set to rise to over one million by 2025 (Prince et al., 2014).
Dementia is acknowledged as one of the strongest determinants of entry into residential care in people aged over 65 (Alzheimer’s Society, 2007). Up to 69% of care home residents are living with dementia (Prince et al., 2014) due to their limited ability to self-care, or to their symptoms worsening to a point where they can no longer be cared for in the community (Corbett, Nunez, & Thomas, 2013).
Pharmaceutical care: A role for community pharmacists
Pharmaceutical care is the responsible provision of drug therapy for the purpose of achieving definite outcomes that improve a patient’s quality of life, and a systematic approach or a philosophy of practice that involves the practitioner seeking to ensure that a person receives the correct medicine, in a safe, effective dose, at the right time (Hepler, 1990).
People living with dementia are often prescribed medication to manage the symptoms of the disease, to control the behavioural and psychological symptoms of dementia, or to manage frequently co-morbid conditions such as depression or epilepsy (Jordan et al., 2015). Healthcare professionals including pharmacists have a responsibility to ensure that the extent to which dementia compromises quality of life in sufferers is limited, and that their medication and other co-morbid conditions do not impact negatively on their overall functioning. Approximately a third of patients over the age of 65 in developed countries are prescribed five or more medicines a day (Qato et al., 2008) and incidentally, the majority of people living with dementia fall within this age group. The consequences of poly prescribing, especially in the older adult population with co-morbidities such as dementia, are functional and cognitive impairment, which can worsen health outcomes (Hilmer & Gnjidic, 2008).
Community pharmacists are amongst the most easily accessible healthcare professionals in primary care. They are highly visible and frequently form long-standing relationships with their patients (Chang, Patel, & Schulz, 2015), so play an essential role in the overall health and wellbeing of the community in which they operate. People living with dementia both in the community and in care homes can benefit from the expertise of community pharmacists, who are trained to understand how medicines affect cognitive function.
Pharmacists can conduct clinical medication reviews, to ascertain whether medication prescribed to people living with dementia are helping them, causing any harm, or if indeed are still required (Blenkinsopp, Bond, & Raynor, 2012). The medication review process has been formalised by pharmacists in all settings of care (Blenkinsopp et al., 2012), and has different levels comprising: Level 1 (prescription review) which involves a technical review of a list of the patient’s medication, level 2 (treatment review) which is a review of medicines with the patients full notes, and level 3 (clinical medication review) which is a face-to-face meeting with a patient to review their medication and condition (‘Clinical Medication Review: A practice guide’, 2013). As people with dementia may not always be relied on for their own history (Maidment et al., 2016), conducting level 3 medication reviews with them may prove challenging so their clinical records would be the main source of information. Pharmacists can also monitor patients for disease progression and other medication related issues such as adherence.
Care home services from community pharmacies are listed under ‘enhanced services’, within the community pharmacy contract. In England, NHS England is the national commissioner for the NHS community pharmacy services to care homes, and commissions pharmacies to provide 'advice and support to the residents and staff within the care home, over and above an essential dispensing service, to ensure proper and effective ordering of drugs and appliances, their clinical and cost effectiveness, storage, supply and administration, and proper record keeping' (Pharmaceutical Services Negotiating Committee (PNSC), 2005). However, clinical commissioning groups are also free to develop their own local services in response to identified local needs (PSNC, 2017).
A Pharmacy Integration Fund (PhIF), launched in 2015 was included in the new funding arrangements for community pharmacy in England (Community Pharmacy 2016/17 and beyond: the final package, 2016). One of the priorities of the PhIF is to deploy pharmacists and pharmacy services to primary care settings including GP practices and care homes.
In October 2016, NHS England (NHS Commissioning Pharmacy Integration Fund, 2016) confirmed that from April 2017 the PhIF will fund the deployment of pharmacy professionals in care homes, including development of the workforce through educational grants. This is a welcome development for care home residents, particularly those with chronic, progressive diseases such as dementia.
Deployment of clinical pharmacists in care homes can greatly improve disease management in residents (Royal Pharmaceutical Society (RPS), 2016), but currently, this is a relatively small workforce and the service is not consistently offered in all care homes. There is an overwhelming need for a bespoke model of pharmaceutical care for dementia patients, responsive to local patients' needs and contributing to the achievement of defined public health goals.
This study broadly explores pharmacists' knowledge and understanding of the pharmaceutical care needs of people with dementia living in care homes and their opinion of the effectiveness of current pharmaceutical services provision.
Methods
Aims and objectives
Aim
To explore the perceptions of participant pharmacists about the pharmaceutical care needs of people living with dementia in care homes and establish the nature of pharmaceutical care services provided to these residents.
Objectives
To investigate pharmacists’ awareness of pharmaceutical care needs of people living with dementia in care homes.
To explore the nature of services provided by pharmacists and their opinions on their knowledge and ability to provide these pharmaceutical services.
Study design
A qualitative study design using face-to-face semi-structured format was employed to explore the views and perceptions of pharmacists who provide services to care homes that have people living with dementia. A qualitative methodology was chosen to support in – depth exploration of issues from the perspective of the research participants, and it followed the Consolidated Criteria for Reporting Qualitative studies (COREQ) guidelines (Tong, Sainsbury, & Craig, 2007). Ethical approval was obtained from the Cross-Schools Research Ethics Committee (C-REC) at the University of Sussex.
Participant recruitment
Community pharmacists were invited to participate in two ways: first, a purposive sample of all 17 care homes in the Thurrock area that have dementia patients or a mixture of dementia and non-dementia patients were identified by searching the website, www.carehome.co.uk (Care Homes Residential Homes UK Guide, 2015). The researcher contacted the homes identified to ascertain the main provider for their pharmaceutical services. Pharmacists working in pharmacies identified by the care homes were contacted by the researcher and invited to participate in the study. Their contact details were obtained from the Find Pharmacy services – NHS Choices website (2015). A written letter of invitation including detailed information about the study was sent to the pharmacists identified. This was followed up by a phone call after five working days to ascertain the willingness of the pharmacist to participate. Ten pharmacists consented to participate.
A similar approach was used to identify pharmacists providing services to care homes in the Kent area, and eight pharmacists were approached, with six consenting to participate in the study. More participants were recruited from the Kent area, a different locality, to validate original findings from Thurrock and follow an iterative process.
The recruitment process was conducted by BN.
Data collection
Semi-structured interviews were carried out face-to-face with each consenting community pharmacist and comprised a combination of open and closed questions (see Appendix 1 for interview schedule).
The interviews followed a standard format and at the start, each pharmacist was thanked and asked to confirm that they are happy to participate in the study; permission will also be sought to record the interview using an audio recorder.
Face-to-face interviews allowed the interviewer (BN) to probe fully for responses and clarify inconsistencies and ambiguities more easily. The disadvantage in this approach lies in the fact that interviews can be expensive, time consuming and there is potential for interviewer bias to be introduced (Bowling, 2009).
Participants who consented were interviewed face-to-face at a time of their convenience at their place of work. The length of each interview varied between 10 and 30 minutes.
Inclusion criteria
For both the Thurrock and Kent localities, pharmacists contacted were eligible to participate if they provided services to care homes catering for dementia patients, or have a mixed clientele which included patients with dementia.
Data analysis
Following each interview, audio-tapes were reviewed for familiarisation with the data obtained.
Interview tapes were transcribed verbatim and content analysis carried out using a thematic framework approach for sorting, categorisation and interpretation of recorded interviews (Bowling, 2009).
The thematic framework included:
Analysis for emerging themes, Coding of emerging themes, Rearranging the data according to identified themes, Mapping and interpretation.
Transcripts were independently reviewed by BA, who met with BN for mapping, interpretation and comparison of findings to ensure consistency.
Findings
To ensure anonymity, pharmacists interviewed in Thurrock were designated P1 to P10 and those interviewed in Kent were designated K1 to K5.
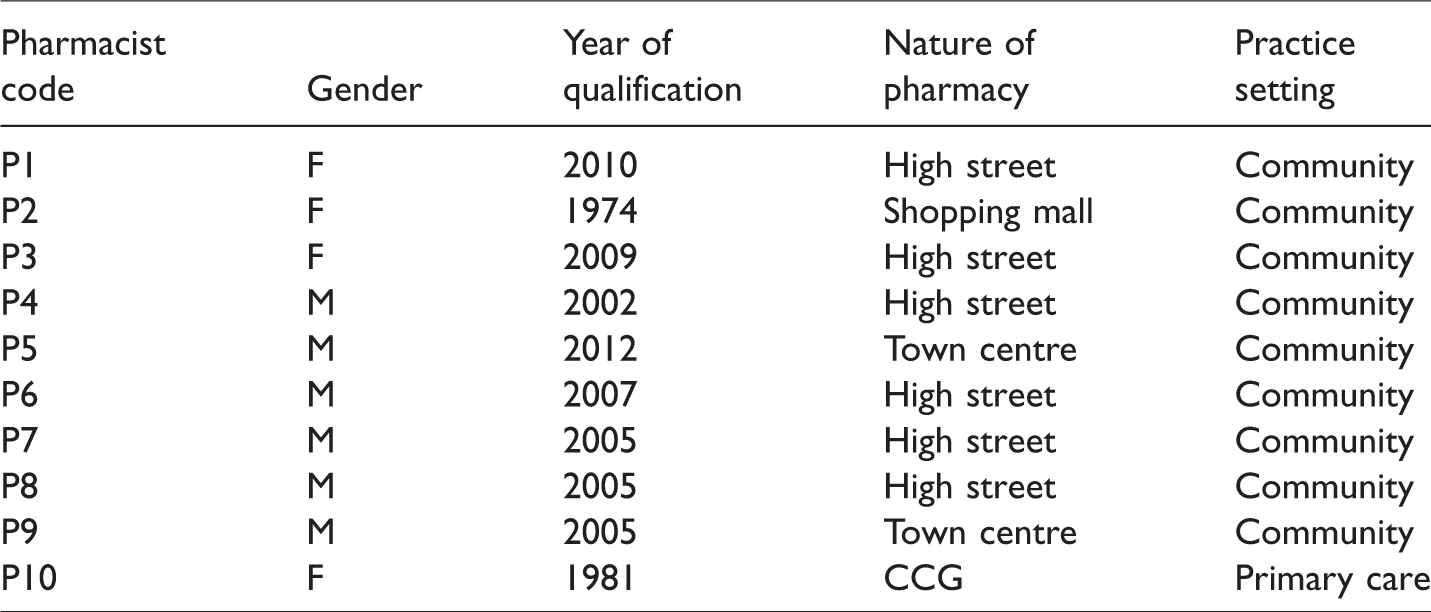
In Thurrock, 10 pharmacists participated in the study, six male and four female pharmacists who have been qualified in the UK between three years and 40 years. Nine pharmacists supplied services to care homes with dementia patients and the 10th was a practice support pharmacist reviewing medication in care homes (Table 1).
Demographics of pharmacists interviewed in Thurrock.
In the Kent arm of the study, six pharmacists consented to participate but one, (K2), subsequently dropped out, stating that she did not deal with people living with dementia and did not work with care homes, and had consented to participate in the study without fully understanding what it was about.
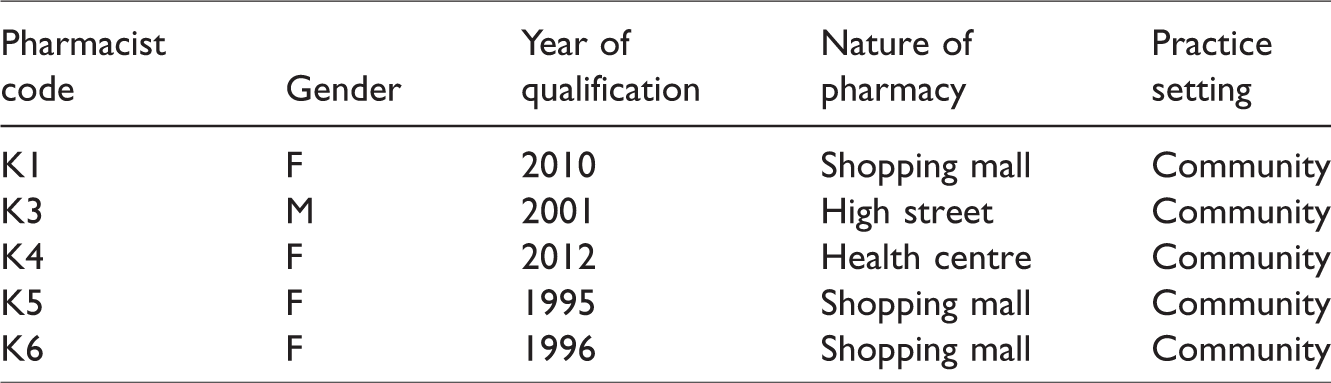
One male and four female pharmacists who have been qualified in the UK between three years and 20 years participated in the study. All were community pharmacists working in a high street, health centre or shopping mall setting (Table 2).
Demographics of pharmacists interviewed in Kent.
A focused analysis of the interview transcripts was performed by exploring the responses provided with consistencies and variances being highlighted. Data saturation (no new information forthcoming) was achieved by the 10th interview in Thurrock and sixth in Kent, and this fact was verified by both BN and BA.
BN reviewed emergent themes for patterns and connections within and between the categories, deriving four main overarching themes, which were verified by BA. These were: medication supply, medication reviews, care home staff training and adequacy of services provided.
Medication supply
The main pharmaceutical service provided by pharmacists in both locations involved the dispensing of medication in monitored dosage systems (dosette boxes) with subsequent delivery to the care home. ‘… we only blister their medication, that’s the only service that we provide, then once a year, we’ll go and do a “care home visit”’ (P3). ‘… we provide nomads (dosette boxes) … we prepare the medication and then deliver to them’ (K3) ‘… we monitor their medication. Where there are changes, we check with the doctors … we basically deal with their prescriptions, medications and deliveries’ (P5). ‘… checking medication to be delivered monthly, as well as intra-medication they may request between their monthly instalments’ (K5) ‘I think it is quite difficult for the pharmacist to input beyond making sure the medication is in the dosette … it is quite difficult for the community pharmacist to do anything other than maybe enable the person to have things they can easily open’ (P10) ‘Apart from the usual repeat dispensing and obviously getting their monthly medications for them, we also offer pharmacist advice visits, where we go there and just look into standards, regulations and standards on how to manage medication in care homes’ (K1) ‘I go like once a month to ensure that they’re taking their medication on time, and then if they have any issues or any problems, then they can discuss with me’ (K3) ‘… sometimes when they have minor ailments, we are able to provide them with things like paracetamol and medicines for constipation, just the little things that will take their doctors’ time …’ (K4)
Medication reviews
Medication review is defined as a critical examination of a patient’s medication with a view to reducing medication-related problems, optimising impact of medicines and reducing waste (Taskforce on Medicines Partnership and the National Collaborative Medicines Management Services Programme, 2002). Clinical medication reviews by pharmacists, which can be performed at a number of levels, have been shown to reduce medicines-related problems and pharmaceutical waste, as well as improve health outcomes (Krska, 2001).
Amongst the Thurrock study participants, only one pharmacist conducted medication reviews in care homes. Other participants did not provide this service because it was not commissioned by their local clinical commissioning group (CCG). ‘We don’t get paid for it, so we don’t do it’ (P2). ‘They do have a team of people who are employed by the CCG to go out and do a lot of medicines optimisation. So where I could do anti-psychotics audits, they’re normally done for me …’ (P2). ‘We haven’t offered any because of the simple reason that I don’t think the PCT will allow it’ (P7). ‘… I do like, medicine use reviews there, to see whether there are any compliance issues or any problems; then we go from there. It’s for the GP then.’ (K3). ‘If they were on antipsychotic medication, there’s this separate set of protocols to look through to make sure that it’s being used properly. For dementia medication, it would be like any other: checking dose, side effects, history, interactions with what else they are taking, that they’re being administered correctly, just as you would in any normal medicine use review’ (K5)
Care home staff training
Only half of the participants interviewed in the Thurrock area provided training to help improve the skills of care home staff such as ordering, storage, administration, disposal and record keeping of medicines (P1, P2, P3, P4, and P7) ‘… Basically we train on administrations, importance of MAR sheets, how to read medication labels and what a prescription looks like and what the controlled drug is …’ (P7). ‘We’re not trained in that … we don’t do any kind of training with care homes’ (P6). ‘So anytime we sign up, we draw a contract with the care home and before we start issuing medication to them, she goes there to train all the staff, just for them to understand our policy’ (K1). ‘There is a lead in the care home unit who, if a request is put in for some training or some advice, they would go and do that, and also there is an internet site for care home staff to access on different aspects of care home procedure and illnesses and I believe dementia is one of them’ (K5)
Pharmacist K4 didn’t have it in her remit, while K6 was not personally involved in training and was unsure of what her establishment offered their care homes in terms of training.
Adequacy of services provided to care homes
All participants were asked to comment on whether the pharmaceutical services they provided to care homes were sufficient to meet the needs of the residents.
A majority of the community pharmacists interviewed in Thurrock acknowledged that the services they currently provided did not fully meet the pharmaceutical care needs of patients in the care homes, including dementia patients: Elaborating on this, P1 said ‘they need specific tailored care, than just general healthcare from the nursing assistants and general care from the GP surgery, or rather a more specific tailored dementia friendly health service would be helpful: specific training for dementia carers to understand their problems and be able to support them’ ‘I don’t think we have time for our patients to sit down and talk about their needs’ ‘we get paid to dispense the medication, that’s really all we get paid to do’,
P6 said ‘personally, I would love to see more involvement of pharmacists in dementia care. That’s really the future, I think, just like American pharmacists are doing’.
In contrast, three participants stated that the services they supplied were sufficient and in line with their contractual obligation. ‘We are not specifically trained to provide services for dementia patients, but we do provide services within the framework that we have, which is the supply them, and what happens beyond supply is beyond our control’ (P1). ‘When you’re working in the pharmacy, you’re working on your own. So it’s very hard to leave’ (P4).
Interestingly, those who said they were providing an adequate service focused solely on medication supply and responding to queries: “… they are satisfied with the service because we do deliver to them on time …” (K3). ‘Yeah, well, we deliver to them when they need it, so, yeah, definitely. It’s sufficient for their needs’ (K4). ‘I think so, yes … we’re also chasing them on medication they haven’t ordered, that the homes may have forgotten or have overlooked …’ (K6).
However, an extension in the role of the community pharmacist was supported by K1, who expressed a view that more could be done: ‘I think there is a lot we can do … medicine reconciliation and also a lot of audits … I don’t think we are doing enough. More involvement, pharmacists being involved more in their care can really help’ (K1).
Discussion
Whilst all participants in this study considered supply of medication to be the main service they provided to care homes, a few undertook medication reviews and some trained care home staff as part of their pharmaceutical service.
Dispensing (supply) and repeat dispensing of medicines is an essential service offered by all pharmacy contractors in England, Scotland and Wales (PSNC, 2017). The supply role historically established the image of community pharmacy as a profession in which dispensing and sales of medication dominates (Varnish, 1998). This has led to the perception of pharmacists as the least visible professionals within the primary care network when compared to roles played by doctors, dentists, midwives, optometrists and nurses (Hassell, Seston, Schafheutle, Wagner, & Eden, 2011).
In England, the population of people aged 65 and over is projected to increase by 51% by 2030, and that of over 85s by 101% (Office for National Statistics, 2011). The implication of this is increased levels of long-term conditions and reliance on medication to ensure independence and a good quality of life. Pharmacists in expanded roles would work more closely as part of multidisciplinary healthcare teams to support patients with long-term conditions, and reduce the burden on emergency care services by providing patient-focused care which would help keep the old and frail out of hospital (Sharpe, 2013).
Consequently, over the last three decades, steps have been taken by pharmacy professional bodies and the Department of Health (DOH) in the UK to expand the role played by pharmacists (DOH, 2003). This led to the incorporation of advanced and enhanced services into the community pharmacy contractual framework (PSNC, 2005). Pharmacists now offer services such as smoking cessation, weight management, appliance use reviews and New Medicine Service (NMS) amongst a myriad of other advanced and enhanced services, to patients/service users in the community.
However, as a result of the involvement of pharmacists with these pharmacy-based commissioned services which require their presence on the premises, there are limits to their capacity to provide more than an enhanced supply role to care homes in general, and people living with dementia in particular.
While the previous service specification for community pharmacy services to care homes does not cover medication reviews, it has been suggested that community pharmacists can ‘build a compelling case to improve medicine management’ in care homes by doing just that (Lau, 2014).
Alternatively, employing specialist pharmacists to offer a clinical service to care homes, reviewing medication and improving disease monitoring can lead to better management of dementia and other chronic health conditions, with the added benefit of reducing wastage and saving thousands of pounds in medication costs (Andalo, 2014). For people living with dementia in care homes, this service has been shown to lead to a reduction in the level of antipsychotics prescribed (Child, Clarke, Fox, & Maidment, 2012; Prentice & Wright, 2014).
This model has been proven to be beneficial to vulnerable residents of care homes especially in reducing inappropriate prescribing (Furniss et al., 2000), and recommendations have been made for every care home to have a designated pharmacist for this purpose (Barber et al., 2009; NICE Guideline ‘Managing medicines in care homes’, 2014; RPS, 2014; RPS Scotland, 2012; Webber, 2015). However, there is currently no obligation for local CCGs to commission such services.
Community pharmacists are accessible, and already provide an efficient supply service to care homes. They are well placed to provide an enhanced medicine management service to care homes which do not have a specialist pharmacist working in that capacity. Community pharmacists can provide patient advocacy and support, integrating with other members of the healthcare team to ensure continuity of care (Crump et al., 2011). Medication management for people living with dementia is known to be sub-optimal (Deeks, Cooper, Draper, Kurrle, & Gibson, 2015). This makes the argument for the establishment of an on-going systematic approach to pharmaceutical care in dementia quite compelling. The DOH (2014) document entitled ‘Dementia Revealed: What Primary Care Needs to Know’ recognises that ‘systematic follow-up of patients with dementia whether on drug treatment or not presents a logistical challenge for general practice’ and advocates that patients have simple care plans which include treatment and review plans. Community pharmacists who regularly interact with people with dementia and/or their carers are an underutilised resource that could be trained to provide the much needed systematic follow up.
In welcoming the announcement of a £42 million-pound PhIF by NHS England in October, 2016 (NHS Commissioning Pharmacy Integration Fund, 2016), the Chief Pharmaceutical Officer for England, Dr Keith Ridge, acknowledged that community pharmacy will have to change the way it works. He asserted that there will be a shift from the old-fashioned view of the pharmacist as dispensers, with integration into a greater NHS role in helping patients.
According to proposals in the new Community Pharmacy Contractual Framework for 2016–2018, the PhIF will support community pharmacy as it develops new clinical pharmacy services. Part of these will be the deployment of pharmacists into care home settings from April 2017. This is in line with recommendations by the RPS (2014), that pharmacists should be responsible for medicines and their use in care homes, and that every care home should be assigned to a community pharmacist and GP practice to ensure co-ordinated care of a consistently high standard.
Whilst implementation of these recommendations would greatly improve medication management for people living with dementia in care homes, there are significant barriers to community pharmacists delivering such a role. These barriers include the limited resources available to support pharmacists (Maidment et al., 2016), variability in outcomes from pharmacy-led interventions, and the fact that community pharmacists are usually unable to access patients’ clinical records (Richmond et al., 2010). The increasing work load of community pharmacists (Gidman, 2011), potential lack of adequate knowledge and skills in the field of dementia, lack of access to patient care records and inadequate communication with prescribers (Maidment et al., 2016) have all been suggested as possible reasons why an optimal pharmaceutical care service is not currently provided by pharmacists to care homes in England.
In this study, only three participants said they offered any form of training to care home staff, lack of time being cited as the reason this service was not provided. Residents in care homes are amongst the most vulnerable people in our society relying almost entirely on care home staff for their needs, and considering that many are on more than seven different medications for complex medical conditions, the margin for medication error can be high (Centre for Policy on Aging (CPA), 2012). Staff awareness has been identified as key in avoiding medication errors in care homes, and a programme of initial and refresher training in areas such as the importance of timings between medication doses, correct inhaler technique, monitoring of adherence should be established (CPA, 2012). Local community pharmacists are best placed to deliver such training and indeed some do. Staff in care homes can also face challenges in communicating with people with dementia, and pharmacists can play an important role in educating staff, addressing their questions especially with relations to medication and side effects, or directing them to additional resources where necessary (Chang et al., 2015). In this study, the community pharmacists interviewed, delivered services to care homes ranging from one care home in the case of one participant to over 70 care homes in the case of another. However, though the Care Quality Commission (CQC) report, ‘Cracks in the Pathway’ (2014), described many aspects of poor care for people living with dementia in care homes, ranging from issues with assessment of care needs to planning and delivery of care, roles for community pharmacists were not considered.
This study has identified the current nature of services provided by community pharmacists to people living with dementia and other morbidities in care homes; it has also identified areas where pharmacists’ roles can be expanded for example, in the training of care home staff and in the provision of medication reviews in care homes.
Study limitations
This was a small qualitative study, and as such, the findings are not generalizable to the wider community.
The interviews were conducted in community pharmacy consultations rooms but there were constant interruptions as participants often had to stop recording to deal with queries and conduct clinical checks of prescriptions within the pharmacy. This could have disrupted their thought processes and contributed to less than comprehensive answers.
Additionally, though data were obtained from face-to-face interviews from participant pharmacists with varying lengths of experience, there is still a possibility that they may have given socially desirable responses to some of the questions posed.
Conclusion
Analysis of semi-structured interviews with 15 pharmacists revealed that the pharmaceutical care provision by community pharmacists to dementia patients in care homes consisted mainly of medication supplies, in accordance with the contractual framework agreed between the local authorities and the community pharmacy contractors. Dealing with barriers such as time pressure, poor communication with other members of the healthcare profession and training on pharmaceutical care needs of people living with dementia, may lead to a more person-centred care from pharmacists.
However, the precise pharmaceutical care needs of people living with dementia in care homes still need to be clearly defined. This is necessary to develop a comprehensive service framework that underpins a cognitive, transformative and well-defined pharmaceutical service to be delivered by pharmacists providing pharmaceutical care to these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.