
Abstract
Objective
Develop and test a stigma awareness and education curriculum targeted to non-medical staff of a local Alzheimer’s Association chapter.
Methods
The curriculum, developed in collaboration with leadership and educational staff from the Cleveland Chapter of the Alzheimer’s Association, included a definition, types, and domains of stigma; effects of stigma on individuals with dementia and their families; stigma evaluation studies; tips to address the topic of dementia-related stigma with individuals and families. Lastly, an interactive discussion of real-life scenarios facilitated stigma recognition and management.
Results
Most staff felt the training improved their ability to identify Alzheimer’s disease stigma, made them more comfortable talking about stigma, and would change the way they interacted with people and families impacted by Alzheimer’s disease.
Conclusions
This brief, practical educational curriculum has potential to improve awareness of dementia stigma in Alzheimer’s Association staff. Research is needed to expand stigma awareness in individuals and groups with varying levels of dementia knowledge.
Introduction
The projected increase in both absolute numbers and relative proportion of people with Alzheimer’s disease (AD) and other dementias brings to the forefront the challenges that can be expected for individuals and families living with these conditions (National Institute on Aging, 2011). In the United States, the Alzheimer’s Association is the leading voluntary health organization in Alzheimer’s care, support, and research and provides an array of support and services including education, support groups and access to on-line communities (“Alzheimer's Association, http://www.alz.org/).
Stigmatizing attitudes towards individuals with AD and other dementias are common and are a potential barrier to care and support, which can impact help-seeking and community inclusion (Blay & Toledo Pisa Peluso, 2010; Burgener et al., 2015). A recent systematic review of dementia-related stigma research conducted by our group of investigators suggests that broadly implemented evidence-based stigma reduction approaches are not available to communities generally, and research on how best to address dementia-related stigma has been limited (Herrmann et al., 2017). Our systematic review also found that even those with extensive experience with dementia, such as health care professionals, can at times inadvertently exacerbate stigma and that attitudes about dementia from formal or informal care providers can impact people with dementia and their families. (Brannelly, 2011; Cahill et al., 2008; Gove, Downs, Vernooij-Dassen, & Small, 2016; Lahjibi-Paulet et al., 2012; Piver et al., 2013; Vernooij-Dassen et al., 2005; Werner & Giveon, 2008).
Given that reducing dementia stigma potentially leads to more support and a higher quality of life for people with dementia and their families, it is critical that practical approaches that are amenable to broad scale-up be developed and tested. This brief article describes an educational pilot program conducted at the request of a local chapter of the U.S. Alzheimer’s Association. The educational program was a quality improvement project intended to raise stigma awareness and help Alzheimer’s Association staff address stigma in their interactions with people with dementia and their families and care providers. The local institutional review board (IRB) determined that the project did not qualify as human subject research according to U.S. Federal regulations, specifically in being an educational and training curriculum under 45 CFR46 or 21 CFR 56. Findings are intended to inform the development of a stigma education approach that can be formally tested and potentially delivered to members of the community with experience with AD and other dementias.
Methods
This program was funded by an educational grant from the local chapter of the Alzheimer’s Association. The stigma awareness and education curriculum was developed by university researchers with expertise in health behavior, aging/dementia, health communication, and in collaboration with leadership and educational staff from the Cleveland Chapter of the Alzheimer’s Association. The curriculum was informed by findings from a systematic review of research on dementia-related stigma from the last decade, with a particular focus on interventions intended to assess and reduce dementia-related stigma (Herrmann et al., 2017). Program evaluation on the topics of AD knowledge, attitudes, and stigma was either adapted from standardized instruments identified in the review or were standard Likert-type questions intended to evaluate staff satisfaction with the program.
Stigma awareness and education curriculum
The curriculum consisted of four main components, delivered over 2.5 hours. Part 1 included a brief introduction, orientation, and overview of the training purpose (15 minutes). Part 2 was a 30-minute presentation of dementia stigma based on findings from the systematic review of dementia-related stigma. Key points of this presentation included the definition of stigma, discussion of types and domains of stigma, effects of stigma on people and families dealing with dementia, and a review of existing interventions that featured an experimental dementia-stigma assessment. Part 3, delivered by the study health communication expert (LH) provided practical tips and advice on how one might address the topic of dementia-related stigma with individuals and families. Figure 1 illustrates some of these topics. Part 4 featured a series of sample scenarios, derived from the behavioral health expert’s (MS) experience working with patients and families dealing with dementia. The example scenarios were followed by an interactive discussion of stigma recognition and management, as well as how consumer-oriented organizations like the Alzheimer’s Association might provide resources and materials aimed at reducing stigma and its impact. Figure 2 illustrates one of the curriculum scenarios followed by discussion questions.
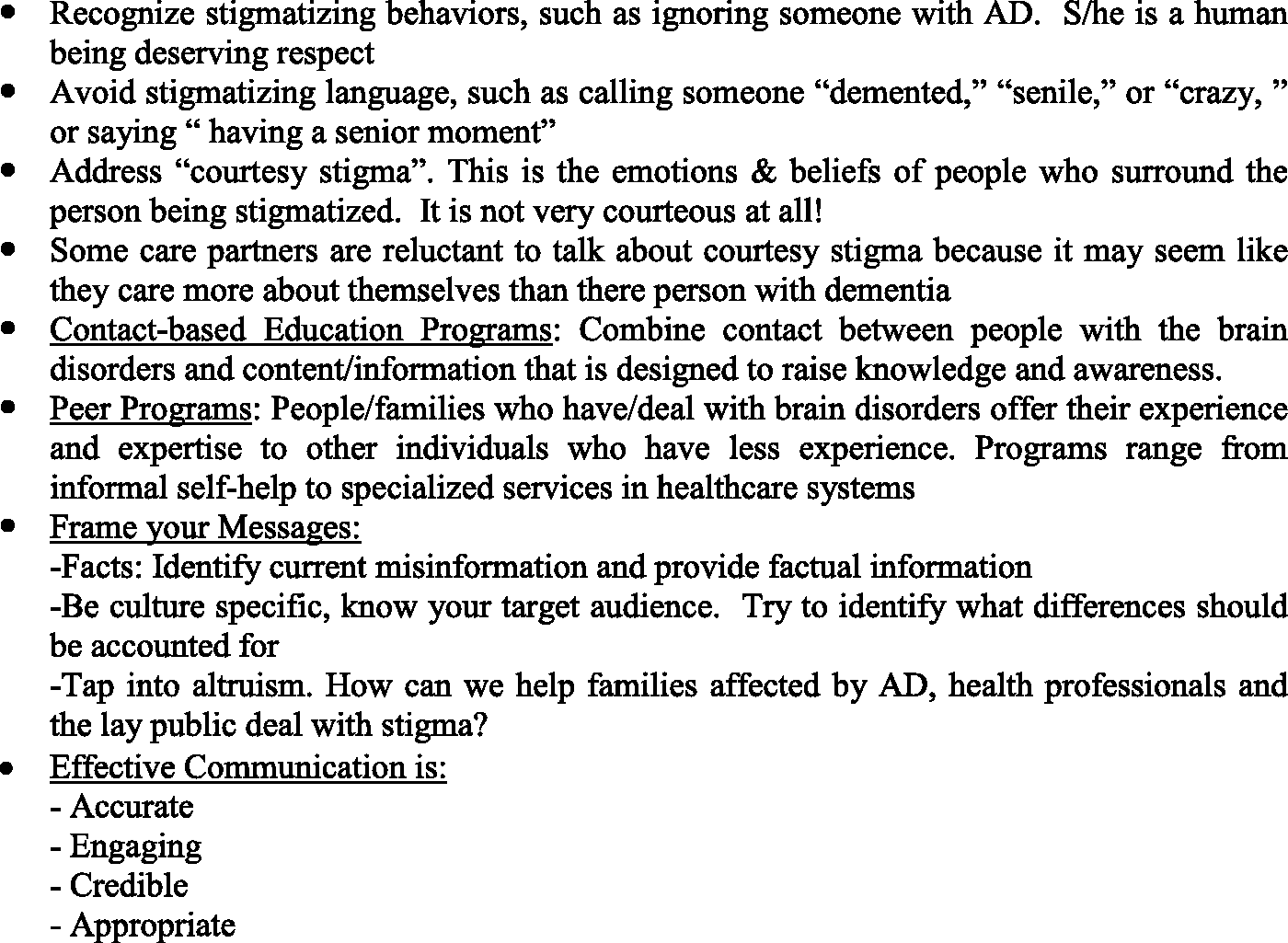
Health communication approaches to address dementia-related stigma.

Case-based scenario: The reluctant card player.
Assessments
A brief battery of assessments was conducted by the educational delivery staff prior to and immediately after participation in the educational program. All program evaluation was conducted anonymously, and there was no attempt to link any survey responses to a given individual. Demographic evaluation and an assessment of AD knowledge were administered prior to the curriculum delivery. Assessments on dementia stigma that staff expected people with dementia to encounter were conducted pre- and post-program. After completion of the curriculum, staff were assessed on their perceptions of how the program might impact their own future behavior and/or practices.
AD knowledge
AD knowledge was assessed at baseline with the validated self-reported 30-item Alzheimer’s Disease Knowledge Questionnaire (ADKQ), developed by Carpenter and colleagues (Carpenter, Balsis, Otilingam, Hanson, & Gatz, 2009). Internal consistency (coefficient alpha 0.71) is adequate, as is test–retest reliability (coefficient 0.81). Scores range from 0 to 100% with higher scores indicating greater knowledge of AD.
Dementia stigma
Program attendees completed a modified version of the self-reported lay public portion of the Family Stigma in Alzheimer's Disease Scale (FS-ADS), developed by Werner and colleagues (Werner, Goldstein, & Heinik, 2011). Validated in a sample of 185 adult children of adults with AD, the FS-ADS has demonstrated acceptable internal reliability with coefficient alphas of 0.66–0.97 in 8 of 9 factors (Werner et al., 2011). In the original scale and in this training exercise, participants rated items on a 5-point Likert-type scale (1= Not at all; 3 = somewhat; 5 = very great extent). Higher scores for negative items indicate more stigma. We administered three of the FS-ADS stigma domains including: (1) 12 items assessing the degree of structural discrimination participants expected individuals with dementia to encounter (for example, unhelpful clinicians and lack of community services); (2) 18 items assessing expectations regarding emotions (antipathy, pity and supportiveness) directed at the person with dementia; and (3) 6 items that evaluated the social distance or avoidance the person with dementia might be expected to encounter.
Stigma awareness, comfort in talking about stigma, and perceived impact on interacting with people with dementia and family members
Four post-program questions on the topics of stigma awareness and impact on interacting with individuals and families were evaluated on a five-point Likert-scale (1 = very likely, 3= neutral, 5= very unlikely). Higher scores indicate lower awareness and less change in behaviors or practice. Write-in post-program comments were also assessed.
Data analysis
We conducted descriptive analysis of demographic, knowledge, and practice variables. Pre-post scores compared item group means and standard deviation. Similar to a dementia stigma study by Johnson and colleagues (Johnson, Harkins, Cary, Sankar, & Karlawish, 2015), we categorized stigma items measuring emotional reactions into three subscales: antipathy (e.g. disgust; repulsion; fear), supportiveness (e.g. concern; compassion; willingness to help), and pity (e.g. sympathy; sadness; pity) on the basis of a principal components analysis. For antipathy items, higher scores indicate more antipathy. For supportiveness items, higher scores indicate more support. For pity items, higher scores indicate more pity. All social behavior questions were focused on negative behaviors, with higher scores indicating worse/more stigmatizing behaviors. Structural factors were categorized as negative/discriminatory (forcing treatment, mocking individuals with dementia) or supportive (available community services, professionals who help caregivers, etc.). Higher scores on discrimination indicate more discrimination or access problems, while higher scores on support indicate more support. Means were calculated for each stigma sub-scale by summing totals and dividing by the number of items in each domain.
Results
Overall sample description
Table 1 shows demographic characteristics of the 21 staff who participated in the training program. The sample was predominantly female, white, and well-educated. While the group had extensive personal experience with AD, none were currently caregivers of a person with AD. Consistent with their extensive familiarity with AD and dementia, scores on the ADKQ (only conducted pre-program) were relatively high, with a mean of 88.25% (SD 12.68%) with a range from 43% to 100%.
Demographic description of Alzheimer’s Association chapter staff participating in a stigma awareness and education curriculum.
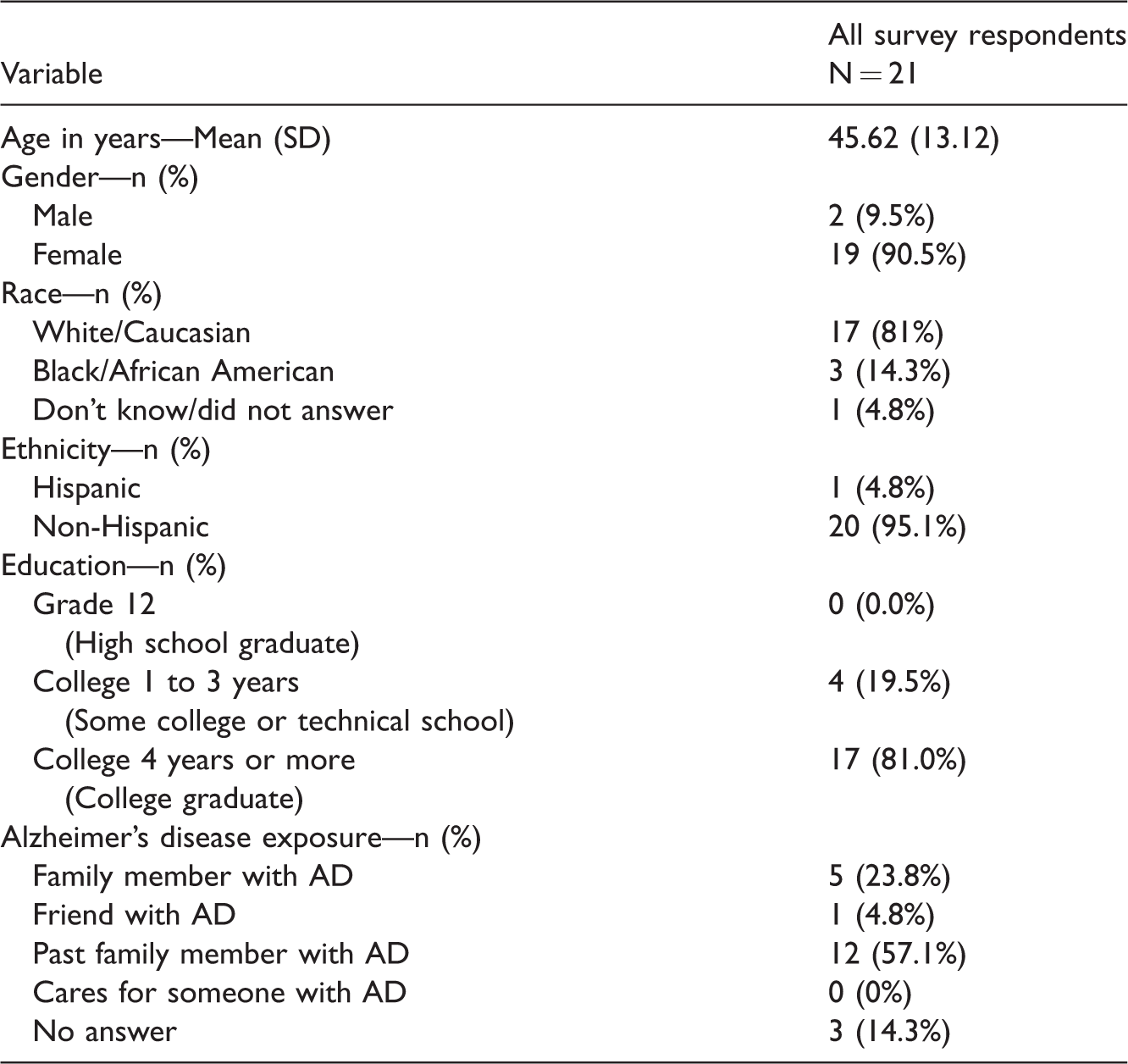
AD: Alzheimer’s disease.
Stigma
Table 2 shows mean scores on the FS-ADS with respect to emotional reactions (FS-ADS 1), social reactions (FS-ADS 2), and structural discrimination (FS-ADS 3). The majority of sub-scale means did not change when comparing pre/post scores, except for the support item, which showed a decrease after the training, indicating stronger belief that individuals with AD have limited support from others.
Pre- and post-program group means on portions of the Family Stigma in Alzheimer's disease Scale (FS-ADS).

aAll FS-ADS sub-scales are presented as mean scores with possible range for each item being 1 (not at all) to 5 (all the time). Higher scores indicate more stigma/discrimination/negative attitudes except for the supportiveness sub-scale where higher scores indicate more support.
bSupportiveness sub-scale items were reverse-scored to yield a total emotional reaction wherein higher scores indicate more stigma/discrimination and less support.
Post-program perceived effects on comfort with discussion about stigma and plans to change behaviors
Table 3 shows proportion of participant responses regarding comfort with stigma identification, perceived impact of this program on comfort with talking about stigma, and likelihood of interacting with people with AD and their families differently because of the program. Notably, the majority of program participants (90–96%) felt that the experience helped them better identify AD stigma, eased their comfort talking about sigma, and would change the way they interacted with people and families impacted by AD.
Perceived impact on stigma identification and likelihood of change in behaviors.
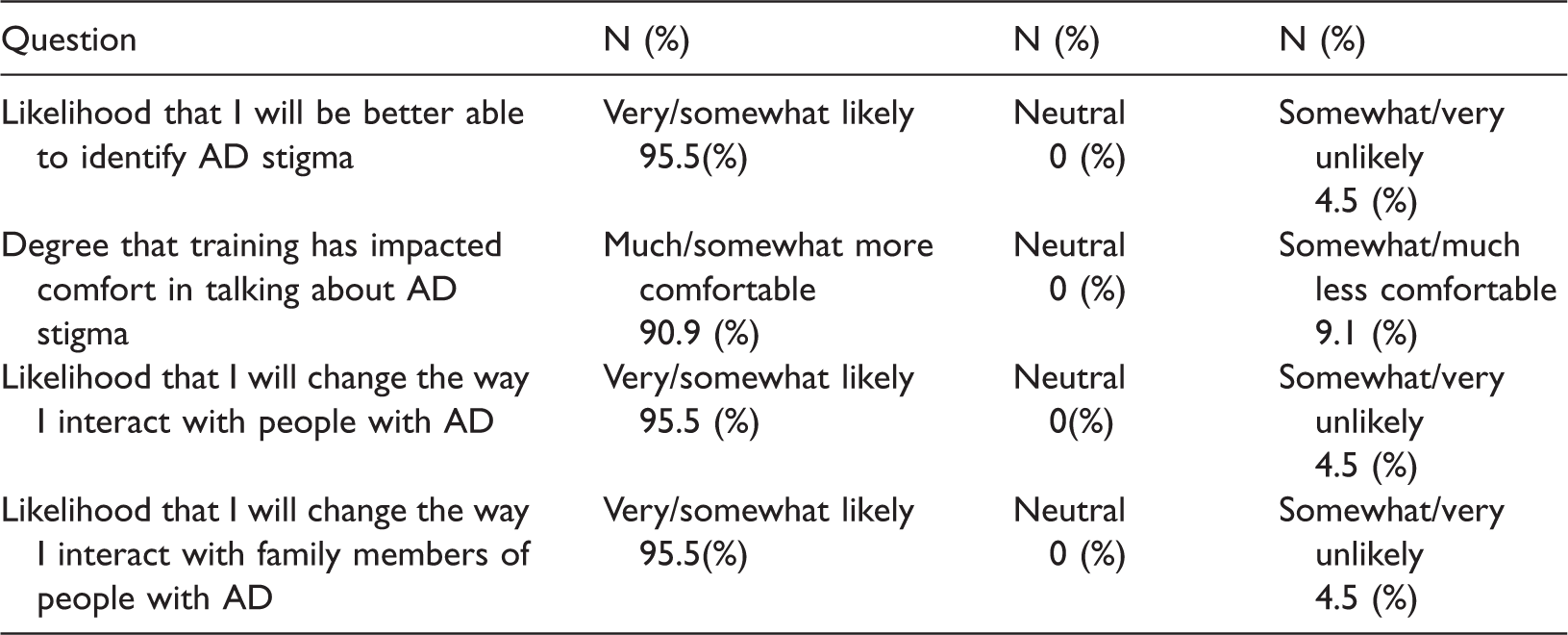
AD: Alzheimer’s disease.
Discussion
This educational curriculum appeared successful in its intended goal of raising dementia stigma awareness and increasing advocacy staff’s confidence in interacting with patients and families around the issue of AD stigma. The majority of Alzheimer’s Association staff felt the training helped them to better identify AD stigma, made them more comfortable in talking about sigma, and would change the way they interacted with people and families impacted by AD. Because this was a program evaluation of a pilot educational curriculum as opposed to a rigorous prospective research project, observations must be tempered by the methodological limitations, including a sample large enough to conduct formal hypothesis testing. Additionally, findings cannot be generalized to individuals or groups who have less experience or familiarity with AD and dementia.
As expected, in a group of individuals with extensive experience with AD and dementia, base rates of AD-related knowledge were high. The average percentage of knowledge questions answered correctly (88%) was higher than reported for samples that included students (67.3%), the lay public (68%), and older adults (80%) (Carpenter et al., 2009; Johnson et al., 2015). Because the training was targeted to a group of individuals with substantial experience with dementia, it did not include extensive review of AD and dementia. In the future, if this program were to be administered to groups with less knowledge of AD, adding more discussion of factual information on dementia and supports available in the community may be beneficial.
Based on pre-post assessment of a standardized stigma scale, no significant change in awareness or identification of structural or social exclusion aspects of stigma after the training curriculum was observed. Findings on the emotional reaction elements of stigma suggested that participants were more likely to endorse the presence of limited support to people with AD because of stigma. It is possible that the training helped improve awareness of the varied and sometimes subtle presentations of stigma that can impede support and help-seeking in families and communities. However, when we combined the emotional response items (antipathy, pity, and supportiveness), we did not see an overall mean change after the training. It is possible that a relatively brief training curriculum may have limited impact on standardized measures of stigma awareness in individuals who already have high knowledge and experience with AD.
There are several points worth noting with respect to future work and implications. The curriculum is relatively brief (2.5 hours) and potentially amenable to broad scale-up given standardized materials. Alzheimer’s Association staff positively endorsed the interactive, case-vignette format that provided a platform for discussing different types of stigma and this may be an ideal way to address “courtesy” or spill-over stigma that families of individuals with AD and dementia may experience. In our pilot work, the curriculum was delivered in a single session, which was practical and efficient; however, this may have limited the amount of information that was digested or appreciated. If the program is to be adapted for use in groups with less AD and dementia familiarity, it may be helpful to deliver the information over multiple meetings for a shorter period of time for each individual session.
Interpretations of our findings have several limitations, most notably a small sample with relative homogeneity with respect to gender, ethnicity, and dementia experience. Participants’ overall high familiarity with AD limits generalizability. In spite of these limitations, it appears the curriculum may help individuals who already have some familiarity with AD and dementia to more specifically address this important topic that impacts the lives of individuals with AD and their families. This practical stigma awareness curriculum has potential to improve recognition of the varied and sometimes subtle presentations of stigma that can impede support and help-seeking in families and communities. Future opportunities for testing and broader-scale up need to be explored in rigorous research designs that allow for formal hypothesis testing. Finally, it will be important to develop and test stigma awareness and reduction approaches that can be used to address AD and dementia stigma in individuals and populations that have limited or no knowledge or familiarity with these conditions.
Data access
Any questions about potential access to the data can be directed to the study lead author.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MS served as consultant for Cognition Group, ProPhase, Bracket, Pfizer, Otsuka, and Sunovion.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: This project was supported by an educational grant from the Cleveland Chapter of the Alzheimer’s Association. MS has received grant support from Otsuka, Alkermes, Janssen, Pfizer, and Merck, royalties from Springer Press, UpToDate, Johns Hopkins University Press and Oxford Press.